Johnson’s Behavioral System Model in Nursing Practice
Bonnie Holaday
Nursing is “an external regulatory force that acts to preserve the organization and integration of the patient’s behavior at an optimal level under those conditions in which the behavior constitutes a threat to physical or social health or in which illness is found.” The goal of nursing is to “restore, maintain or attain behavioral integrity, system stability, adjustment and adaptation, efficient and effective functioning of the system.
History and Background
The Johnson Behavioral System Model (JBSM) was conceived and developed by Dorothy Johnson while she was a professor of nursing at the University of California, Los Angeles (UCLA). The process of developing this model began in the late 1950s as she examined the explicit goal of action of patient welfare that was unique to nursing. The task was to clarify nursing’s social mission from the perspective of a theoretically sound view of the client. The conceptual model that resulted was presented at Vanderbilt University in 1968 (Johnson, 1968). Since that time, other noteworthy presentations of the model have been offered (Auger, 1976; Dee, 1990; Derdiarian, 1990, 1993; Grubbs, 1974; Johnson, 1980, 1990). Johnson retired from UCLA in 1978, but she maintained her interest in “systems” through her hobby of shell collecting. She traveled extensively to collect shells and later donated them to a museum in Sanibel, Florida. Johnson died in February 1999. Johnson’s papers, documents, and letters, per her request, are available at the Eskind Biomedical Library Special Collections at Vanderbilt University in Nashville, Tennessee.
The JBSM offers useful guidelines for nursing practice. Used in conjunction with the nursing process, it has provided a useful conceptual map to plan patient care. Poster, Dee, and Randell (1997) provided evidence supporting the efficacyof the JBSM as a tool for evaluating patient outcomes. Auger and Dee (1983) developed the UCLA Neuropsychiatric Institute and Hospital Classification System, based on the JBSM. This system was integrated with the nursing process and is used as a clinical measure of patient progress.
The work of Auger and Dee led to the development of behavioral indices, with each subsystem operationalized in terms of critical adaptive and maladaptive behaviors. The behaviors were ranked into categories according to their assumed level of adaptiveness. Nurse clinicians can rate each behavior for compliance by using an activity rating scale of 1 to 4. This scale provided a basis for allocating nursing resources at the UCLA Neuropsychiatric Institute (Dee & Randell, 1989).
Derdiarian used the JBSM to develop the Derdiarian Behavioral System Model (DBSM) instrument (Derdiarian, 1983, 1988; Derdiarian & Forsythe, 1983). The DBSM’s 22-category interview generated data pertaining to the major changes in the behavioral systems as a result of illness, as well as the positive or negative effects of these changes. Specifically, two types of subjective data were generated. This included the “set”-related variables (the variables that potentially predict or influence the patient’s usual behavior) and the behavior resulting from illness. Overall, research findings suggested that the DBSM instrument improved the focus, comprehensiveness, and quality of nursing assessment, diagnoses, interventions, and evaluation of outcomes of adult patients with cancer, acquired immunodeficiency syndrome (AIDS), and myocardial infarction (Derdiarian, 1983, 1988).
Other studies have also documented the utility of the JBSM for nursing practice. Holaday (1980) used the model to assess health status and to develop nursing interventions for children undergoing surgical procedures. Wang and Palmer (2010) used the model to conduct an analysis of the concept of women’s toileting behavior related to urinary elimination. Dee, van Servellen, and Brecht (1998) found that the JBSM could be used to derive meaningful conclusions about the impact of managed care on nursing care problems, and Coward and Wilkie (2000) demonstrated that the JBSM could be used to plan pain management for cancer patients. Colling, Owen, McCreedy, and colleagues (2003) planned a continence program for the frail elderly; Brinkley, Ricker, and Toumey (2007) used the model to examine esthetic knowing with a hospitalized obese patient; and Tamilarasi and Kanimozhi (2009) developed an intervention to improve the quality of life in breast cancer survivors.
Holaday’s work demonstrated identification of subsystem disorders, validated the notion of behavioral subsystems and their utility and usefulness in nursing practice, broadened the understanding of the role of “set,” and examined the relationship between sustenal imperatives and action (Holaday 1974, 1981, 1982, 1987; Holaday, Turner-Henson, & Swan, 1996). Derdiarian’s research demonstrated the factor-isolating and categorizing potential of the JBSM, validated the notion of behavioral subsystems, and provided empirical descriptions of central concepts in the theory (Derdiarian, 1983, 1988, 1990; Derdiarian & Forsythe, 1983). Meleis (2012) described the body of research related to nursing practice that the JBSM has generated and noted that it provided “significant developments in the conceptualization of the nursing client” (p. 280).
Overview of Johnson’s Behavioral System Model
Johnson’s model for nursing presents a view of the client as a living open system. The client is seen as a collection of behavioral subsystems that interrelate to form a behavioral system. Therefore, the behavior is the system, not the individual. This behavioral system is characterized by repetitive, regular, predictable, and goal-directed behaviors that always strive toward balance (Johnson, 1968).
Johnson (1968) proposed that the nursing client is a behavioral system with behaviors of interest to nursing and is organized into seven subsystems of behavior: achievement, affiliative, aggressive, dependence, eliminative, ingestive, and sexual. Nurses using the model believed that an additional area of behavior needed to be addressed (Auger, 1976; Derdiarian, 1990; Grubbs, 1974; Holaday, 1980). They added an eighth subsystem, restorative. Each subsystem has its own structure and function. Each subsystem comprises a goal based on a universal drive, set, choice, and action. Each of these four factors contributes to the observable activity of a person. Boxes 8-1 and 8-2 provide examples of how one might operationalize the function and structure of each subsystem. Grubbs (1980) provides excellent definitions of the concepts and terms used in the JBSM.
The goal of a subsystem is defined as “the ultimate consequence of behaviors” (Grubbs, 1974, p. 226). The basis for the goal is a universal drive, the existence of which is supported by existing theory or research. The goal of each subsystem is the same for all people when stated in general terms; however, variations among individuals occur and are based on the value placed on the goal and drive strength.
The second structural component is set, which is a tendency to act in a certain way in a given situation. Once they are developed, sets are relatively stable. Set formation is influenced by such societal norms and variables as culture, family, values, perception, and perseverative sets. The preparatory set describes one’s focus in a particular situation. The perseverative set, which implies persistence, refers to the habits one maintains. The flexibility or rigidity of the set varies with each person. Set plays a major role in determining the choices a person makes and actions eventually taken.
Choice refers to the alternate behaviors the person considers in any given situation. A person’s range of options may be broad or narrow. Options are influenced by such variables as age, gender, culture, and socioeconomic status.
The action is the observable behavior of the person. The actual behavior is restricted by the person’s size and abilities. Here the concern is the efficiency and effectiveness of the behavior in goal attainment.
Each of the subsystems also functions in a manner analogous to the physiology of biological systems (e.g., the urological system has both structural and functional components). The goal of the subsystem is a part of the structure. It is not entirely separate from its function.
For the eight subsystems to develop and maintain stability, each must have a constant supply of “functional requirements” or sustenal imperatives (Johnson, 1980, p. 212). The environment must supply the functional requirements or sustenal imperatives of protection from unwanted, disturbing stimuli; nurturancethrough giving input from the environment (e.g., food, caring, conditions that support growth and development); encouragement; and stimulation by experiences, events, and behavior that would “enhance growth and prevent stagnation” (Johnson, 1980, p. 212).
The subsystems maintain behavioral system balance as long as both the internal and the external environments are orderly, organized, and predictable and each of the subsystems’ goals is met. Behavioral system imbalance arises when structure, function, or functional regimen is disturbed. The JBSM differentiates fourdiagnostic classifications to delineate these disturbances: insufficiency, discrepancy, incompatibility, and dominance.
Nursing has the goal of maintaining, restoring, or attaining a balance or stability in the behavioral system or in the system as a whole. Nursing acts as an “external regulatory force” to modify or change the structure or to provide ways in which subsystems fulfill the structure’s functional requirement (Johnson, 1980, p. 214). Interventions directed toward restoring behavioral system balance are directed toward repairing damaged structural units, with the nurse temporarily imposing regulatory and control measures or helping the client develop or enhance his or her supplies of essential functional requirements.
Critical Thinking in Nursing Practice with Johnson’s Model
Making wise choices about nursing care requires the ability to think critically—that is, to analyze the available information, make inferences, draw logical conclusions, and critically evaluate all relevant elements, as well as the possible consequences of each nursing decision. From a constructivist perspective, individuals presented with complex information use their own existing knowledge and previous experience to help them make sense of the material. In particular, they make inferences, elaborate on the information by adding details, and generate relationships between and among the new information and the information already in memory. In short, they think critically about the new and old information (Paul & Elder, 2009). The JBSM provides information in a way that permits problem solving and care planning (Table 8-1).
TABLE 8-1
The Johnson Model and the Nursing Process
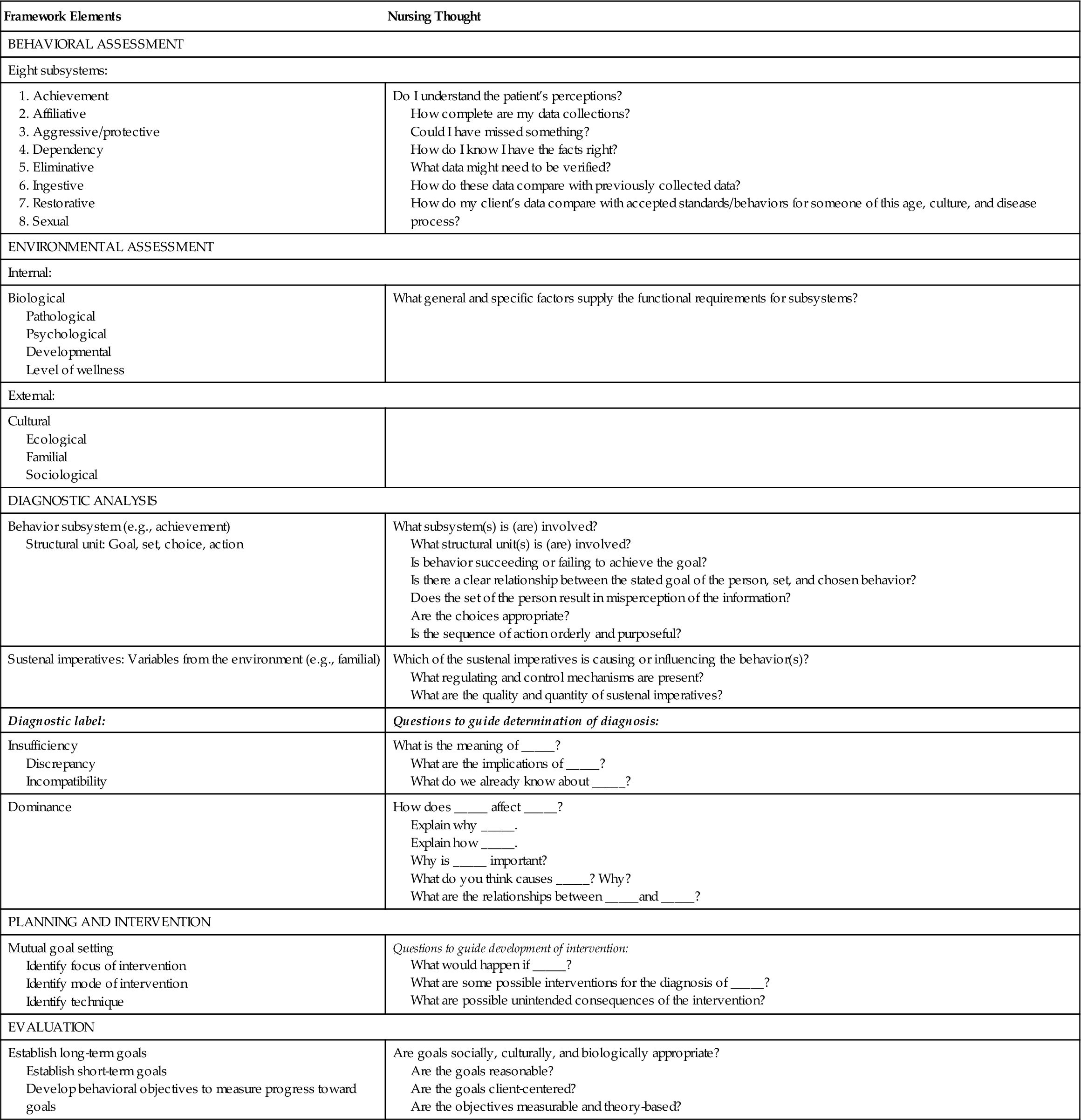
The focus of the process is to obtain knowledge of the client through interviews and observations of the patient and family to evaluate the present behavior in terms of past patterns, to determine the effect of the present illness or perceived health threat and/or hospitalization on behavioral patterns, and to establish the maximum possible level of health toward which an individual can strive. The behavioral systems’ analysis approach provides a comprehensive framework in which various types of data can be organized into a cohesive structure.
The assessment gathers specific knowledge regarding the structure and function of the eight subsystems (behavioral assessment) and those general and specific factors that supply the subsystems’ functional requirements/sustenal imperatives (environmental assessment). Interview questions in both areas need to be theory-based. For example, Piagetian theory can be used to develop questions to assess a child’s ability to express knowledge about illness—eliminative subsystem (Holaday, 1980).
Once the interview has been completed, data analysis (diagnostic analysis; see Table 8-1) is necessary to identify patterns of behavior that are adaptive and functional for the client as well as those that are maladaptive and indicate behavioral systems’ imbalance. One component of the analysis seeks to determine congruency among all structural units. Congruency is expressed as stable, patterned behavior, whereas discrepancy among the components is expressed as unstable and disorganized behavior. The second component examines how the functional requirements/sustenal imperatives influence subsystem behavior. For example, how does family interaction style affect the client’s affiliative subsystem? The latter analysis is critical because it plays an important role in determining how the nurse needs to function as an “external regulator” (Johnson, 1980, p. 214).
The nursing diagnosis is a summary of the results for the analysis and describes the current level of behavioral system function. It serves as a guide for intervention planning by the nursing team. The overall objective of the nursing intervention is to establish regularities in the client’s behavior to meet the goal of each subsystem. The focus on the intervention will be either on a structural part of the subsystem or on the supply of sustenal imperatives/functional requirements.
Identifying goals is essential for evaluating client outcomes and for professional nursing care. To evaluate, the nurse must first predict expected client outcomes. This helps ensure a purposeful, predictable course of client responses. To evaluate effectively, the nurse sets both long-term and short-term goals and behavioral objectives that will indicate progress toward achieving these goals.
Concept mapping is also an effective strategy to combine with use of a nursing theory such as the JBSM (Daley, 1996). A concept map is a graphic or pictorial arrangement of key concepts that address specific subject matter such as behavioral system imbalance. Concept maps are organized with the most important or central concept at the top of or in the center of the paper (Figure 8-1). Related information or issues are to the side or underneath the main topic. There is no right or wrong way to design a concept map. It may be a flowchart or a diagram or even shaped like a heart if the issue were congenital heart disease. The purpose of the concept map is to develop critical thinking skills and problem-solving abilities (All, Huycke, & Fischer, 2003; Ferrario, 2004).

Nursing Care of Debbie with Johnson’s Model
Behavioral Assessment
The relative behavioral assessment data are as follows.
Achievement
Affiliative
Aggressive/Protective
Dependency
Ingestive
Eliminative
Sexual
Restorative
Diagnosis and Intervention
The JBSM provides a perspective for nursing practice by viewing Debbie as a biopsychosocial being represented in a behavioral system. The objective and subjective data indicate a problem in the achievement subsystem, as follows:
Environmental Assessment
The environmental assessment examines the sources of sustenal imperatives (functional requirements) to determine whether they provide the functional requirements needed to maintain behavioral system balance. If these are present (or have been present in sufficient quantity and quality over time), the subsystems and subsequently the entire system operate at the same level of efficiency and effectiveness and are able to maintain overall balance and stability. If they are not present, the nurse will act as an external regulatory force to provide protection, stimulation, or nurturance; change structural units; or impose external regulatory mechanisms. The critical component of the environmental assessment is to identify the factors that cause or influence behavioral system problems.
The environmental assessment identifies several key factors. From a developmental perspective, Debbie is relatively young and thus many of the developmental tasks of young adulthood, such as raising her children and establishing a career and other future plans, could be impaired. The cancer diagnosis raises questions about her physical ability to achieve personal goals, and the pain, fatigue, and anxiety may impair her mental ability to achieve personal goals. During the first 3 months after diagnosis, Debbie needs to address issues related to the diagnosis, including dying, the future, and the meaning life has had (Eiseman & Lalos, 1999). During this same time, Debbie will be presented with a treatment plan and will simultaneously learn to cope with recovery from surgery and the side effects of cancer therapy and to plan for the future. The significance of this initial period cannot be overemphasized as Debbie attempts to regain control over herself and the environment.
Diagnosis and Intervention
In examining Debbie’s perseveratory set, one would note that Debbie’s perception of herself as an independent agent generally capable of accomplishing her tasks and goals has been substantially altered. In terms of the preparatory set, her situational context is also substantially altered. She is most likely uncertain about herchoices. The diagnosis is insufficiency in the achievement subsystem. In terms of intervention, the nurse may protect Debbie from noxious stimuli because she is not presently able to cope with all situations. The nurse can provide nurturance in terms of providing counseling and help with goal setting. Stimulation in terms of teaching new self-care behaviors can also help. The biological disease process is unique for each person, and the psychosocial response to mastering the situation will be equally unique. Thus frequent reassessment and revision of the care plan will be needed.
Most patients faced with a diagnosis of cancer experience a life crisis. Although death is often the first fear, the potential for other stressors exists. Surgery, adjuvant therapy (radiation), the possible spread of malignancy, and an uncertain prognosis are all stressors. Surgery may lead to an altered body image with accompanying feelings of lost femininity. It is reasonable to assume that Debbie is experiencing some sexual concerns, and the sexual subsystem should be thoroughly examined because objective data indicate the potential for behavioral system imbalance.
The objective data identify that Debbie had a radical hysterectomy, which means the vaginal canal has been shortened. Because the trigone of the bladder and the sigmoid colon may be closely associated with the new vaginal apex, sexual intercourse may be uncomfortable. Debbie will receive radiation therapy. Side effects from this therapy may include fatigue, nausea and vomiting, and infection. The subjective data indicate that Debbie’s husband is emotionally distant and sometimes abusive and that Debbie is tearful and worried about the future. The perseveratory set reveals that the current physiological functioning of the sex organs has been disrupted. Past socialization and experience in sex role behaviors may no longer seem applicable to Debbie. Within the context of the present situation (preparatory set), Debbie is most likely unsure where to direct her attention. The selection of a sexual behavior (choice) to meet goals is unclear.
Because the subsystem is not functioning to its fullest capacity, the nurse could diagnose insufficiency. If Debbie takes actions that do not meet the intended goal of the subsystem, a diagnosis of discrepancy could also be made.
Evaluation
Debbie has a knowledge deficit regarding radiation therapy and needs nurturance in terms of education to help her understand and cope with the situation. A careful assessment to determine Debbie’s understanding of the purpose and goal of treatment is needed. Debbie must be taught preventive health practices that decrease the risk of impaired vaginal membrane integrity and comfort measures such as sitz baths and compresses to the perineum. Alternative methods of sexual intercourse can be discussed, especially because sexual intercourse during treatment is encouraged to prevent adhesions and to prevent shortening of the vagina. Counseling Debbie and her husband can help them create their own special intimacy, sense of affection, and physical gratification. The nurse’s goal of helping restore the patient’s sexual function is tied in closely with goals of restoring or maintaining self-image and self-esteem.
Nursing Care of Mark with Johnson’s Model
Behavioral Assessment
Achievement
Mark looked at the nurse with a great little smile when he described his school and how it is different. He describes it as a “handicap school.” He likes it because there are only “16 kids and 2 teachers and I get lots of help.” He is also proud of what he can do on the computer. Mark attributes his success to the presence or absence of ability and attributes little to motivational factors. He enjoyed the Piagetian testing, which placed him in the concrete operations period. Both the nursing staff and his mother note that he requires verbal prompts to perform self-care activities. His mother notes that he has missed a lot of school during the past 2 years, which is why she and her husband removed Mark from regular public school and placed him in a special education school. The classes are ungraded, but his mother says he has made great progress at this school and now reads at a sixth-grade level and has math skills at a fifth-grade level. Mark is worried about “getting behind” while he is in the hospital. Mark has no idea what he wants to be when he grows up. He has not been to camp, nor has he ever spent the night at another child’s home. Mark has never been home alone; a parent or sibling is always present.
Affiliative
Mark seems emotionally more attached to his mother than to his father. He likes and admires his older brothers and wishes he “could ride dirt bikes with them.” He spends a lot of time at home with his mother and alone watching TV or “messing around on the computer.” He watches football games and other sports on TV with his father on the weekends. Mark cannot name a friend at his school or in his neighborhood. His mother states he likes to be “with other kids” and likes when his brothers’ friends are at the house. She also could not name a child who was a friend. The nursing staff and his mother describe Mark as shy, and the nurse’s observation in the playroom confirms this. He is more talkative when his mother is absent. When Mark’s mother is present, he lets her answer questions or asks her to do so.
Aggressive/Protective
His mother and the nursing staff describe him as passive and more likely to sulk than get angry. When the nurse asked what he would do if someone took something of his or hit him, Mark said he “wouldn’t like it.”
Dependency
Mark refused to answer questions about self-care. The nursing staff states that they saw little evidence of self-care activity during previous admissions. He lets the nursing staff or his mother maintain his blood glucose level, inject his insulin, select his menu, and perform his bowel and bladder care. Mark’s mother states that he has become more dependent on her during the past year. He asks for help to dress in addition to his other requests. The staff has noted more independent behavior when the mother and grandmother are absent. Nurses noticed a tremendous difference between the way he acted with them when his mother and grandmother were not present (adult/child to adult/parent with the nurse; and child/parent with mother and grandmother).
Ingestive
Mark states, “I like to eat.” His mother also describes Mark as “loving food” and “eating too much.” The switch to the “diabetic diet has been difficult for him.” The family eats meals together. Postoperatively, he usually has nausea and vomiting and fluid and food intake is poor. Mark is very observant of what goes on around him. He likes to “have tests and things explained” to him when he is in the hospital.
Eliminative
Mark has minimal bowel and bladder control. He has frequent problems with dribbling of urine. Mark himself admits this bothers him. His mother suspects he does not perform intermittent self-catheterization regularly at school because he is embarrassed about sexual changes and about the fact that he must wear sanitary protection pads. As for his communication pattern, Mark tucks his head to his chest and mumbles when he is talking about his feelings or his parents. Sometimes he simply refuses to answer or looks away. The nurse suspects the mumbling and shyness are a means of coping with his overtalkative and overprotective mother and grandmother.
Sexual
Mark looked away when the nurse asked about changes in his body and “becoming a man.” He did not answer questions. He said he did not like “wearing special pants.” When asked who he was most like in his family, he said his mother, who admits that she and her husband have talked with Mark about sex. “We don’t know what to tell him because of his birth defect.” His father has told him the changes “are part of growing up and becoming a man.” His mother is concerned because Mark “hasn’t asked any questions like the other boys.” Mark is Tanner stage 3. She adds, “I think his brothers have talked with him because they joke around about making out.”
Restorative
Mark sleeps 8 hours a night but sleeps less in the hospital “because they wake you up all the time.” He usually gets up around 7 AM on school days and 8:30 AM on the weekends. He has a somewhat restricted repertoire of interests and activities. He spends much time watching TV and rental videos and plays computer games. He participates in no groups, clubs, or regular physical activity. He enjoys family weekend trips to the lake and dune buggy and boat rides.
Environmental Assessment
Familial
Structure
Mark is the youngest of three boys. His mother works part-time as a secretary and is home in the afternoon when Mark returns from school. His father works as a manager of a large department store. The maternal grandparents live nearby. The grandmother visits frequently.
Dynamics
Mark is included in all family activities, and Mark and his brothers are involved in home activities and chores. It appears that the parents do not fully discuss all aspects of Mark’s illness (sexuality issues, compliance, approaching adolescence) nor do they discuss all issues with Mark. The mother is overly responsible for Mark’s treatments; she encourages Mark’s overdependency. In turn, the mother assumes more responsibility for care.
Social/Cultural
Mark is part of a Protestant, middle-class family who does not attend church regularly. Both parents place a high value on home and family. The father has assumed the patriarchal provider role in the family. The family has lived in the same house for 17 years and has several close friends in the neighborhood who will help whenever needed. The parents have also maintained social relationships with several of the father’s business associates. They belong to no outside social clubs or groups. Insurance covers 90% of Mark’s expenses, and they sometimes face financial troubles. Currently, however, there are no major financial problems.
Developmental
Mark laughed when the nurse said he was about to become a “terrible teen.” He said he has heard adults talk about it, but he would not elaborate. Mark enjoys heavy metal rock, computer games, and watching TV. When asked about girls, he shrugged and looked away. Mark attends a special education school and is behind his grade level. His social skills are not age-appropriate. Medical treatments, parental overprotectiveness, and physical disability all seem to be reinforcing dependence while diminishing any sense of self-control over health. Self-care responsibility is less than what we would expect of a 12-year-old.
Pathological and Biological
Mark stated that he hates “everything about hospitals.” He acknowledged that the increase in restrictions of activity bothered him. The “tests” and “surgery” worry him. He knows the surgery is to try to stop the “leaking” of urine, but Mark is uncertain about where they will operate and exactly what will be done. Mark doesnot like diabetes because he can no longer “eat whatever I want.” Mark has a poor understanding of diabetes. He could not explain the role of insulin and diet in the management of the illness. Mark better understands myelomeningocele and how that affects his walking and bowel and bladder control. On admission, Mark’s vital signs are normal. He is in the 25th percentile for height for his age and 90th percentile for weight. His blood urea nitrogen (BUN), creatinine, and blood glucose levels are slightly elevated. His glycohemoglobin level is elevated, indicating poor long-term glucose control.
Ecological
The family owns a home in the suburbs. A park is located about 1 mile from their home, and a school and playground are located about ½ mile from home. The parents describe the neighborhood as safe. No public transportation is available in the area.
Psychological
As a preadolescent, Mark is concerned about body image and is anxious about any bodily disruption or change. He seems self-conscious about his early sexual maturation. His mother has noted Mark’s childlike behaviors and increasing dependency during the past year (e.g., wants help dressing). He is socially isolated from peers, and interaction with his brothers has decreased during the past 2 years. He also needs more emotional support from his mother. His mother calls Mark shy, and the nursing staff’s observations support this assessment. His scores on the self-esteem interview were low. He copes by withdrawing from situations that make him uncomfortable. He does not like to discuss his feelings about sensitive issues (e.g., parents, sexuality, illness). However, he wants information about specific events that are stressful for him (e.g., surgery).
This case study is presented because it reflects both acute and long-term problems associated with managing a chronic illness. It also demonstrates that children’s developmental domains (behavioral subsystems) are often significantly influenced by their illness. One of the strengths of JBSM is that it identifies not only current acute problems but also chronic subsystem disturbances. These alterations involve a disturbance in normal developmental sequences. Without intervention, these alterations may lead to more serious problems as the child matures. This analysis applies the nursing process to an acute problem related to this admission and to a long-term problem.
Diagnostic Analysis
The essential characteristic of human beings is their purposefulness. This purposefulness is based on their ability to select their goals and make choices for achieving them. To successfully intervene in a clinical situation, it is necessary to consider people’s choices and to understand how people make their choices. The JBSM directs the nurse’s attention to human choice phenomena. The degree to which the nurse can help the client restore behavioral system balance depends on the extent to which the client understands behavioral actions. Once an explanation has beenfound, the client can obtain behavioral system balance by changing his or her goals or by changing the environmental conditions in such a way that previously established goals can be obtained through changes in behavior. To accomplish this, nurses need to adopt an input-oriented approach to their case-model building. To focus on the proper inputs, nurses need to develop an assessment strategy that allows them to thoroughly understand small segments of behavior at the subsystem level and to integrate that understanding for the entire system.
An output-oriented approach describes only the person’s choices, and the description provides only knowledge of the behavior. This information is of some use. However, to understand the behavioral elements in the system, nurses must seek an explanation for a person’s action, and this comes only from an input focus. The JBSM’s focus on environmental assessment, as well as behavioral assessment, provides input-focused data as well as output-focused data. The two diagnoses addressed in this section provide insight about the process.
Acute Problem
Mark has been admitted to the hospital for a bladder augmentation and placement of an artificial sphincter. He is behind his grade level at school. Piagetian testing places him at the concrete operations level of cognitive development. The subjective data inform the nurse that Mark is worried about tests and surgery and is unsure about specific aspects of the surgery. He has some understanding of myelomeningocele and little understanding of diabetes. However, he does like to have “tests and things” explained to him. Also contributing to this problem is the mother’s overprotection of Mark and the apparent failure of the family to openly discuss aspects of the illness.
The goal of the ingestive subsystem is to internalize the external environment, and one of the functions is to obtain knowledge or information useful to the self (Grubbs, 1974). The perseveratory set refers to usual status or habits. All of Mark’s sensory modalities—speech, sight, hearing, and touch—are intact, and he values being informed about tests. In terms of the preparatory set, Mark is in the period of concrete operations. He can assimilate new experiences, has developed an awareness of conservation, is capable of seeing the relationships of the part to the whole, and also has developed a concept of causality. Choice refers to the alternate behaviors Mark himself sees that are available to him in this situation. Because little preoperative teaching has been done, Mark’s choice and actions are limited. The diagnosis is insufficiency of the ingestive subsystem. The major stressor is functional—a lack of information. The nurse’s goal is to protect the basic goal of the subsystem by providing information. A successful intervention will inform Mark about the surgery to clarify the range of choices and actions.
Planning and Intervention
Given the complexity of this case, the intervention needs to be planned carefully. The intervention could also affect the dependency subsystem (self-care), achievement subsystem (sense of mastery), affiliative subsystem (socialization), and eliminative subsystem (expression of feelings). It was mutually agreed that the preoperative teaching would be done with both Mark and his parents together and then alone with Mark. Diagrams and pictures will be used to explain the surgery, and postoperativetreatments and procedures would also be explained and demonstrated. Thus the nurse will provide the functional requirements of protection and nurturance.
The immediate goal of the intervention is to inform Mark about his surgery and postoperative care. The intermediate goal is for Mark to maintain his healthy physiological system through the intake of food, fluids, and medicine during the postoperative period. This will occur as a result of his understanding the surgical procedure and the postoperative care needed for recovery (e.g., internalizing the external environment). The long-term objective is that the intervention will restore Mark’s sense of mastery and of autonomy.
Nursing interventions need to be theory-based. These theories need to be compatible with systems’ theory and the assumptions of the JBSM. For example, the technique selected for this intervention is based on Vygotsky’s Zone of Proximal Development (ZPD) (Vygotsky, 1962). One of the strengths of the JBSM is the ease with which theories can be incorporated into all phases of the plan of care.
Wertsch and Rogoff (1984) have defined the ZPD as “the phase in development in which the child had only partially mastered a task but can participate in its execution with assistance and supervision of an adult or more capable peer” (p. 1). There are two important dimensions of the ZPD—joint collaboration and transfer of responsibility—in which both the child and the adult actively participate and contribute to some aspect of task performance or problem solution. Joint collaboration is based on the child being guided to actively define and redefine the task situation in terms of the adult’s definition (Holaday, LaMontague, & Marciel, 1994).
The second dimension is the transfer of responsibility, which refers to the adult’s decreasing role in regulating and managing behavior task performance. This gradual relinquishment and transfer of adult responsibility is described as “guided participation” (Wertsch & Rogoff, 1984, pp. 1-6). Thus as a child’s competence increases, effective scaffolders gradually withdraw their support in accord with the child’s efforts. Scaffolding refers to the gradual decrease and eventual withdrawal of adult control and support as a function of the child’s increased mastery of a given task or problem.
Chronic Problem
It is helpful to think of parenting in terms of the JBSM as a set of environmental actions performed by the parents or a set of environmental conditions arranged by parents that assists or impedes the child in carrying out his or her functions. It is important to make clear that in this examination of parenting actions and conditions as elements external to the child, the independence of the child and environment is not implied. Rather, the examination occurs only for the purposes of assessment and the convenience of organization.
From a JBSM perspective, the idea of an external regulator of growth and development is also useful. The idea of nursing care as a set of regulatory acts, aimed at successful adaptation and goal attainment for the child (behavioral system), is consistent with most ecological developmental models and with the general precepts of control systems’ theory. However, as potentially useful as the concept of an external regulator might be in classifying the actions and conditions of nursing care (i.e., in terms of adjusting parenting actions or environmental conditions arranged by the parent), it carries with it a practical paradox—external regulation is unlikelyto be a simple matter for a complex organism. The JBSM provides a means to approach this issue, but much work remains in building theory in this area. The next care problem clearly addresses the complexity involved.
The data from the environmental assessment identify Mark’s mother as overprotective and highly responsible for Mark’s care. Mark spends a good deal of time with his mother and seems to be more emotionally attached to her than to his father. Mark takes little responsibility for self-care activities. He is described as shy and cannot name a friend. The goal of the dependency subsystem is to maintain environmental resources needed for obtaining help, assistance, attention, reassurance, and security—in other words, to gain trust and reliance. The primary diagnosis is dominance of the dependency subsystem. The behaviors in the dependency subsystem are being used more than any other subsystem regardless of the situation, to the detriment of other subsystems (Grubbs, 1974). A number of secondary diagnoses could also be made in terms of incompatibility between the dependency subsystem (set, choice, action, and goal) and other subsystems (most notably, achievement and affiliative). Problems for both child and parent are evident in terms of set, choice, and action. In terms of the perseveratory set, both parents and child are unsure about the appropriate age at which a child with a chronic health problem should be expected to meet his or her own needs and at which times and places assistance with tasks should be sought. Mark does not perceive himself as self-sufficient and independent. The preparatory set shows that Mark and his parents have difficulty perceiving whether a situation requires task-oriented assistance. Given the problems with set, it is not surprising that the range of choice is narrow and that actions are not always appropriate.
The major stressors are both functional and structural. The functional stressors arise from the environment and are related to parenting style. The structural stressors involve internal control mechanisms and reflect inconsistencies between the subsystem goal and set, choice, and actions.
The short-term goals in this case are to help the parents gain some insight into their behavior and its impact on Mark’s behavior and to facilitate a change in Mark’s behavior (an increase in independent behaviors while hospitalized). The long-term goal is to promote Mark’s optimal development by designing an external regulatory system to do the following:
• Sustain Mark’s current level of independence.
• Stimulate activity directed at more independent behaviors.
• Control the amount and pattern of experiences (inputs) that reach Mark to achieve an optimal fit between Mark’s current abilities and his projected goals.
The family-centered intervention would be best if carried out by a nurse who has sustained contact with Mark and his parents.
The central goal for the nurse, as an external regulatory force, is to construct a system of caregiving episodes the parents can use to integrate the functional requirements for the environmental/developmental relationship. The nurse helps the parents provide protection and nurturance to maintain Mark’s current level of behavior (his internal organizational coherence and environmental relationships) so he can continue to function. The nurse maintains whatever stability is present to avoid encouraging more dependent behaviors. The nurse stimulates incrementalchange (alter set, choice, and action) for both the parents and Mark through a process of self-construction. New information and new experiences will be introduced in a controlled fashion, which will lead to successive changes in existing structures. Goal setting is one technique that can accomplish this. People can cognitively construct representations of potential future states. By personal goal setting, individuals disrupt their status quo or disorganize themselves and then organize their behavior to resolve the disruption or create a new coherent organization. They become “producers of their own development” (Lerner, 1982, p. 342). Thus in goal setting, negative feedback reduces a discrepancy but it does so by altering the system through incremental change.
Evaluation
The JBSM directs the nurse’s attention toward areas that need to be addressed in practice. Currently no specific interventions delineate this system of caregiving episodes for parents of chronically ill children. What broad, basic regulatory functions of the nurse need to be included in this system of caregiving episodes? The actual episodes and conditions of parenting entail numerous physical/structural properties, not just broad abstractions. From the standpoint of understanding the development of a chronically ill child, what are the more salient dimensions of these real acts and conditions for each of the subsystems? How does the nurse function as an external regulator of chronically ill children’s health and development with the goal of a good fit between the child’s characteristics, environmental opportunities, and constraints? Using JBSM, the nurse learns that a chronically ill child’s developmental pathways do not unfold along a predetermined course; they are constructed through processes of living that involve continuities, discontinuities, and uncertainties. The nurse as an external regulator and source of functional requirements plays a critical role in helping a family achieve optimal development outcomes for a special-needs child.