Rogers’ Science of Unitary Human Beings in Nursing Practice
Kaye Bultemeier
Nursing is both a science and an art. The uniqueness of nursing, like that of any other science, lies in the phenomenon central to its focus. Nurses’ long-established concern with people and the world they live in is a natural forerunner of an organized abstract system encompassing people and their environments. The irreducible nature of individuals is different from the sum of the parts. The integralness of people and environment that coordinate with a multidimensional [later changed to pandimensional] universe of open systems points to a new paradigm: the identity of nursing as a science. The purpose of nurses is to promote health and well-being for all persons wherever they are. The art of nursing is the creative use of the science of nursing for human betterment.
History and Background
First introduced by Rogers in 1970, the Rogerian model is an abstract system of ideas from which to approach the nursing care of unitary human beings. Her ideas were revolutionary and challenged nursing to approach care from a wholistic and dynamic worldview.
Within the Science of Unitary Human Beings (SUHB), assumptions regarding the nature of nursing offer further elaboration. First, nursing science is an organized body of abstract scientific knowledge that develops from research and analysis. This science of nursing helps explain the human experience (Rogers, 1970). Second, Rogers contends that nursing is a learned profession and therefore must be based on solid scientific information. Third, Rogers’ theoretical model places an emphasis on “the essentials, potentials, and possibilities that exist within the wholeness of life” (Cowling, 2001, p. 37). Fourth, formulated knowledge is to be used creatively for human betterment (Rogers, 1970). Additional theoretical understanding and elaboration is needed to assist in the understanding of theabstract model introduced by Rogers. Within SUHB, the following are understood to be fundamental:
Overview of Rogers’ Science of Unitary Human Beings
Within this model, human beings are conceptualized as dynamic, constantly evolving energy fields, rather than as homeostatic beings. Variation is expected and embraced within this homeodynamic perspective. The human field and the environmental field are constantly exchanging energy. There are no boundaries or barriers to inhibit energy flow between fields (Rogers, 1970). “The human being openly participates in energy transformation with the environment creating mutual change” (Leddy, 2004, p. 16). The following concepts are inherent to the model and provide additional clarity regarding the Rogerian SUHB.
Unitary Human Being
A unitary human being is “an irreducible, indivisible, pandimensional energy field identified by pattern and manifesting characteristics that are specific to the whole and which cannot be predicted from knowledge of the parts” (Rogers, 1992, p. 27). The life process of the unitary human being is one of wholeness and continuity as well as dynamic and creative change.
Environment
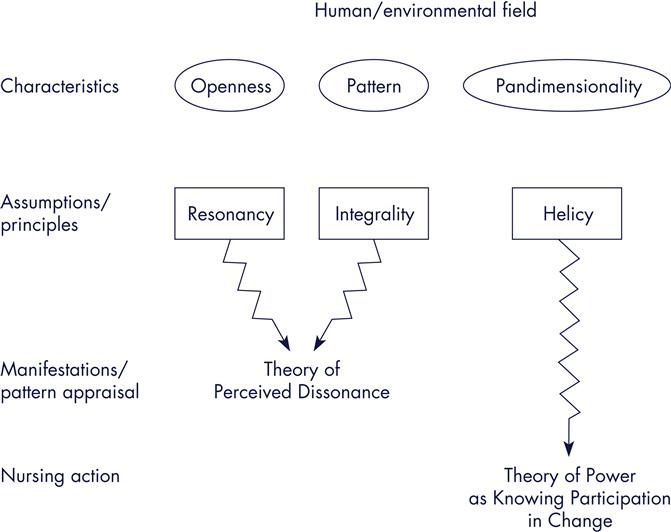
The environment is “an irreducible, pandimensional energy field identified by pattern and integral with the human field” (Rogers, 1992, p. 27). Manifestations emerge from this field and are perceived. Figure 13-1 is an illustration of the coexistence or integrality of the human/environmental fields.

Nursing
The focus of nursing is the care of people within their life process and the lived experience. According to Rogers (1970), “Professional practice in nursing seeks to promote symphonic interaction between human and environmental fields, to strengthen the integrity of the human field, and to direct and redirect patterning of the human and environment fields for realization of maximum health potential” (p. 122). The nurse participates knowingly with the patient and the goal of nursing is human betterment.
Health
The concepts of health and illness are understood as pattern manifestations. The manifestation of health emerges from the mutual, simultaneous patterning process of the human/environmental fields. Pattern manifestation is an expression of the process of life as defined by individuals and their cultures (Rogers, 1970). Therefore, what we know as health and illness are considered continuous expressions or manifestations of the life process in Rogers’ framework.
There are four major concepts of the framework. These concepts describe characteristics of manifestations of the person and environmental mutual process. The major concepts of the framework are as follows:
Pattern
Pattern identifies individuals and reflects their wholeness. Pattern is defined as the distinguishing characteristic of an energy field that is perceived as a single wave. Rogers (1986) clarifies that pattern is “an abstraction” that “gives identity to the field” (p. 5). Patterning “is the dynamic or active process of the life of the human being” (Alligood & Fawcett, 2004, p.11).
Energy Field
Energy is the “potential for process, movement, and change” (Leddy, 2003, p. 21). The energy field is the conceptual boundary of all that is, the living and the nonliving. The energy field “provides a way to perceive people and their environment as irreducible wholes” (Rogers, 1986, p. 4).
Pandimensionality
Pandimensionality is defined as “a nonlinear domain without spatial or temporal attributes” (Rogers, 1990, p. 7). The universe encompasses infinite dimensions, providing an understanding of nonlocality, acausality, and unpredictability (Butcher, 2006).
Openness
The human field and the environmental field are constantly in mutual process. There are no boundaries or barriers to inhibit energy flow between fields (Rogers, 1970). “The human being openly participates in energy transformation with the environment creating mutual change” (Leddy, 2004, p. 16).
The complexity, and yet simplicity, of these paradigm shifting ideas preceded current scientific understanding by several decades. Rogers used her extensive knowledge and diverse educational background to articulate a revolutionary way of viewing the human experience.
Homeodynamic Principles
Rogers’ principles of homeodynamics provide a way of describing, explaining, and envisaging a wide range of perceivable person/environment processes involving change and growth (Rogers, 1986, 1990, 1992). The principles are theoretical assertions that were first proposed by Rogers (1970) as “an ordered arrangement of rhythms characterizing both the human field and the environmental field that undergoes continuous dynamic metamorphosis in the human-environment process” (p. 101) and were later articulated by Rogers (1992) and Phillips (2010). The principles describe the nature of the human/environmental process as follows:
• Resonancy is the continuous change from lower- to higher-frequency wave patterns in the human/environmental fields.
• Helicy is the continuous, innovative, unpredictable, increasing diversity of human/environmental patterns.
• Integrality is the continuous, mutual, continuous human/environmental field process (Rogers, 1992).
Theories for Practice
The Rogerian model provides the abstract philosophical framework from which to view the unitary human being and the environmental field. Though SUHB served as a framework for hundreds of research projects over the past 50 years, recent works have clarified application of SUHB for nursing practice. Rogers states that the nature of nursing is based on theoretical knowledge that guides nursing practice (1970). Barrett’s theory of power (1990b, 1998, 2000, 2010), Butcher’s pattern portrait (2006), and Cowling’s unitary pattern appreciation (1990, 1997, 2001, 2004, 2005) have proposed practice methods for the visionary work of Martha Rogers that guide both research and practice. Emerging from Rogers’ model are many theories that explain human phenomena and direct nursing practice. Cowling (2004) observes, “Research and practice are ‘theory-in-action,’ and practice informs research and theory building” (p. 206). The Rogerian model, with its implicit assumptions, provides broad principles that conceptually direct theory development (Figure 13-2). Theory emerges from each of the principles and unites the art with the science (Alligood, 2002). Some of the midrange theories that have emerged from the SUHB and provide understanding and guidance in the practice of nursing based on Rogers’ homedynamic framework include the Theory of Perceived Dissonance derived by Bultemeier (1997) from the Rogerian model, which provides a theoreticalperspective for exploring situations of varying resonancy as manifested in health care concerns. This theory emerges from the principles of resonancy and integrality and proposes that resonancy is altered periodically and rhythmically during the evolution of energy fields. The perception of dissonance during the rhythmical evolution of the human/environmental field is proposed. During episodes of varying resonancy, the human/environmental field manifestations may be perceived as nonharmonic and as uncomfortable or unsettling to the person; thus the person may view himself or herself as out of harmony, or ill (see Figures 13-1 and 13-2).
Theory of Power as Knowing Participation in Change
The theory proposed by Barrett (1986, 2010), Power as Knowing Participation in Change, emerges from the principle of helicy within the Rogerian model (see Figure 13-2). The theory proposes that as knowledge increases, so does the capacity to participate knowingly. Furthermore, the theory proposes the capacity of human beings to pattern their human/environmental fields. Barrett (2010) explains, “Following the testing and research of the theory and measurement instrument, a practice methodology was developed and the health patterning practice model was initiated” (p. 47). Patterning manifests via the nurse and client patterning process. Barrett (2000) describes power as being aware of what one is choosing to do, feeling free to do it, and doing it. She identifies power as a relative state characterized by the momentary continuously changing pattern. Power is a relative trait characterizedby “the more consistent organization of the human and environmental field pattern” (Barrett, 1986, p. 174). She specifies that as the person is knowledgeable of his or her pattern manifestations, meaningful participation in the patterning process occurs. Barrett’s theory is used widely by nurses around the world. And in 2010, the volume 23, number 1 issue of Nursing Science Quarterly celebrated Barrett’s power theory and Rogers’ SUHB. Barrett (2010) told her story of the development of her power theory in that special issue also pointing out “what’s new and what’s next” (p. 47).
Theory of Self-Transcendence
The Theory of Self-Transcendence by Gulliver (2007) describes the process occurring at the end-of-life. The theory proposes continuously fluctuating imagery boundaries over past, present, and future. With self-transcendence the boundaries become less distinct. The theory further articulates the infinite possibilities for this transition.
Critical Thinking in SUHB Nursing Practice
Critical thinking is a process of conceptualizing, applying, analyzing, synthesizing, and evaluating information gathered from or generated by observation, experience, reflection, reason, and communication as a guide to belief and action. Within Rogers’ model, a critical thinking process was developed that specifies three components: pattern appraisal, mutual patterning, and evaluation (Barrett, 2000; Cowling, 1990, 2004). The activities associated with these components are occurring simultaneously and continuously throughout the care of the client. This is a simultaneous, integral, and constantly evolving process. The life process possesses its own unity and is inseparable from the environment.
Pattern Appraisal
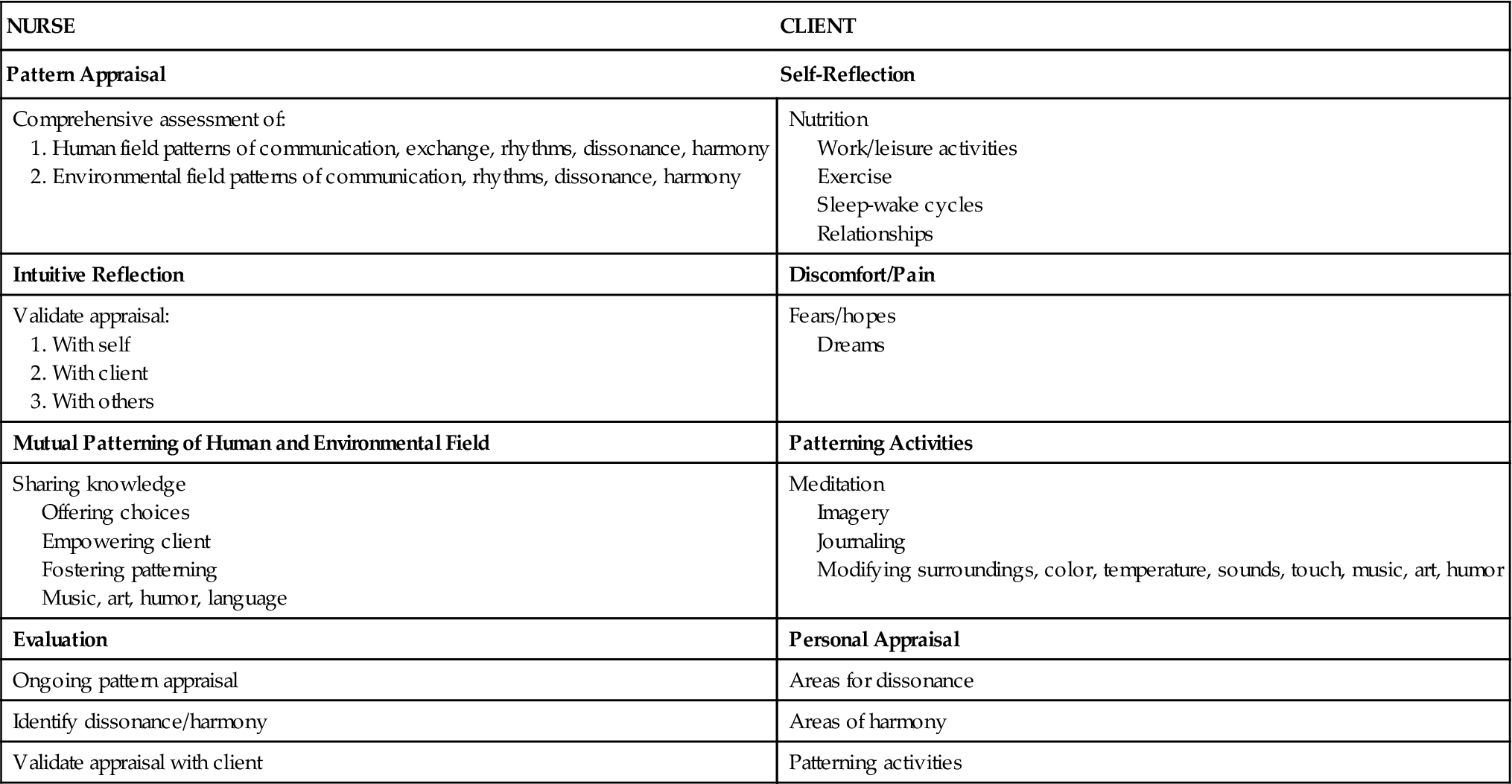
Pattern appraisal requires the identification of pattern manifestations that reflect the whole. Pattern appraisal is integral to the provision of care to unitary human beings. Table 13-1 outlines the critical thinking of the nurse and the self-reflection by the client. Nursing within Rogers’ model focuses on the manifestations that emerge from the mutual human/environmental field process. The meeting of the art and science of nursing is vital to the entire process of caring for the client from a Rogerian framework. Pattern appraisal is a comprehensive assessment that incorporates cognitive input, sensory input, intuition, and language. Intuitive knowledge is gained from both the client and the nurse. The nurse accompanies the client in focusing on personal patterns and rhythms. Identification of emerging pattern manifestations throughout the provision of care allows for a departure from the linear cause-and-effect approach and uses an evolutionary approach. The nurse and client gain awareness of rhythmical fluctuations and their associated manifestations. A change in pattern of the human field and the environmental field is propagated by waves. The manifestations of field patterning that emerge are perceivable events (Rogers, 1992). The identification of patterns that characterize a phenomenon provides knowledge and understanding of the human experience and provides the basis for the care, which results (Rogers, 1970).
TABLE 13-1
Critical Thinking in Rogers’ Model
Patterning “is the dynamic or active process of the life of the human being” that is “accessible to the senses” (Alligood & Fawcett, 2004, p. 11). Pattern information encompasses “phenomena that are categorized as physical/psychological, mental/emotional, social/cultural, and spiritual/mystical” (Cowling, 2005, p. 95). Wholistic pattern appraisal tools are necessary for application of the Rogerian model to the provision of nursing care to the unitary human being.
The nurse incorporates information gained from traditional measurement tools used to care for patients into the wholistic pattern appraisal. All conventional information gained such as vital signs, lab results, biopsy reports, and radiographic reports are integrated into the pattern appraisal and acknowledged as manifestations of the whole. Nurses are asked to incorporate knowledge gained from the use of their senses for the wholistic pattern appraisal. Consequently sight, smell, touch, hearing, and taste all contribute information of emergent patterns. Knowledge gained is via cognitive, sensory, intuitive understanding as well as language. Pattern appraisal includes perceivable rhythms of sleep/wake, mood, pain, movement, and nutrition. Patterning activities are based on probabilistic outcomes as they emergefrom the appraisal of pattern evolution. Emergent human environmental rhythms and patterns are manifestations of the whole; that is, the mutual process of human beings and their environment.
Cowling (2005) provides direction for nurses to study unitary human phenomena such as he has developed for nursing of despairing women. His guidelines assist the assessment and care process. He contends that all pattern appreciation must include the features of being synoptic—viewing together what normally is viewed apart, participatory and collaborative and transformative or reaching for the essence. Butcher (1998) identified additional pattern appraisal methods that include Human Field Motion Tool, Index of Field Energy, Human Field Image Metaphor Scale, Person-Environment Participation Scale, Perceived Field Motion Scale, and the Human Field Rhythms scale.
An important component of the appraisal process involves the work of the client to center and reflect on his or her personal pattern and on the pattern of those with whom he or she shares life. Bultemeier (1997) introduced the use of photographs and written narrative to assist in pattern identification. Pattern appraisal includes multiple lifestyle rhythms, such as nutrition, work, exercise, pain, anger, depression, sleep-wake cycles, and safety. A method for categorizing rhythmicities is by the use of criteria developed by Kim and Moritz (1982). These rhythms include the following: (1) exchanging (eating, elimination, breathing, giving, and receiving); (2) communication (verbal and nonverbal); and (3) relating (spacing, touching, eye contact, belonging, and referencing). During the appraisal, special attention is given to rhythms of pain and discomfort or to areas about which the client is uncomfortable or concerned (Cowling, 1990). Wholistic pattern appraisal methods and practice applications such as the following continue to be developed and refined for human betterment:
• Barrett (1990a,b, 1998, 2000, 2010): Health Patterning
• Butcher (1998, 2006): Pattern Portrait
• Cowling (1990, 1997, 2005): Pattern Appreciation
• Cowling and Swartout (2011): Life Patterning for Healing Praxis
• Greene and Greene (2012): Guided Imagery
• Gueldner, Michel, Bramlett, et al. (2005): the Well-being Picture Scale
• Johnston (1994): Human Field Image Metaphor Scale
• Malinski (2012): Unitary Rhythm of Dying-Grieving
• Willis and Griffith (2010) and Willis & Grace (2011): Healing Patterns
• Wright (2010): Power and Trust
The nurse integrates the feeling or sensing level of knowing, which is often described as intuitive or instinctual into the appraisal process. The intuitive knowledge is best realized through reflection, which assists in pattern appraisal. The nurse realizes that manifestations are not static but are partial perceptions of the synthesis of the past, present, and future. These perceptions provide the basis for reflection and intuitive knowing, which then further expands the appraisal. The manifestations, patterns, and rhythms are an indication of evolutionary emergence of the human field. Pattern appraisal, rhythm identification, and reflection provide the content for appraisal validation with the client. The emergent knowledge provides direction for nursing patterning activities. Maintenance and promotion of health,prevention of disease, nursing diagnosis, intervention, and rehabilitation comprise the scope of nursing (Rogers, 1970).
The unitary human being and the environment are one. Rogers’ theoretical model places an emphasis on “the essentials, potentials, and possibilities that exist within the wholeness of life” (Cowling, 2001, p. 37). Knowledge is used creatively for human betterment (Rogers, 1970). Nursing knowledge provides tools for emergent artistic application as the nurse cares for the unitary human being (Alligood, 2002; Rogers, 1992). Nursing is the creative use of nursing knowledge in the care of unitary human beings. Nursing practice accompanies unitary human beings in their health patterning. Therefore, clients define what health is for them and nurses assist their movement toward that goal.
Mutual Patterning
Once the client and nurse have consensus with respect to the appraisal, nursing action centers on mutual patterning of the human/environmental field. “Voluntary mutual patterning” is defined as the continuous process whereby the nurse assists clients to freely choose, with awareness, ways to participate in their well-being” (Barrett, 1998, p. 136). The goal of nursing is promoting symphonic rhythms of the human and environmental field. This is done to “strengthen the coherence and integrity of the human field and to direct and redirect patterning of the human and environmental fields” (Rogers, 1970, p. 122). Patterning activities in practice may be focused on areas identified as dissonant and described as pain, discomfort, or anxiety. Through mutual patterning of the nurse and the client, manifestations of pattern awareness and power emerge, evidence of Barrett’s knowing participation in change theory.
Mutual patterning emerges from the pattern appraisal and relates to areas of mutually emerging goals. Barrett (1990a, 1998, 2010) identifies components of power that are fundamental to change in the patterning processes: awareness, choice, freedom, and involvement. From the inseparable components of power comes what Barrett (2010) calls a “Power Profile” (p. 49). The power profile indicates “the changing nature of the human and environmental field patterning” (p. 49) as follows:
• Nature of the awareness of experiences
• Type of choices that are made
• Degree to which freedom to act intentionally is operating
• Manner of involvement in creating specific changes (Barrett, 2010, p. 49)
Knowledge of the power profile and various options for patterning are shared with the client. The appraisal guides the knowledge shared, including specific information relating to options. The nurse ensures that the client has adequate knowledge of the appraisal and the various options for patterning. The sharing of the appraisal empowers client participation in the patterning process and choices. Various therapeutic patterning activities are discussed by the client and the nurse. Patterning activities instill hope and are individualized. Modifications are made as needed to accommodate patterning activities to the individual.
The client is empowered in the process of patterning (Barrett, 2010; Cowling, 2004). Power is characterized by continuously changing pattern. Power can be conceptualized as harmonious rhythmicity and as consistent integration of thehuman/environmental field pattern. Cowling (1990) proposes the “goal of patterning is substantive change in health dynamic and change in the direction of health as defined by the client” (p. 51). The nurse’s goal is to assist the client to reach the health potential and foster harmonious patterns, thereby reducing the perception of dissonance.
Barrett (2010) defines patterning as the continuous process whereby the nurse, with the client, patterns the environmental field to promote harmony related to the health event. Rogers (1970) contends that “change proceeds by the continuous patterning of both [person] and environment by resonating waves” (p. 102). Change is specific to energy fields and is perceived through manifestations. Increasing diversity of field patterning characterizes the process of change (Rogers, 1970). Each human possesses rhythmicities of individual uniqueness. The goal is harmonious rhythmicities and human betterment.
Human and Environmental Field Patterning
All treatments and interactions are patterning activities as they are integral to the human/environmental field process. Practice modalities concern human life patterning and reflect the wholeness of the unitary human being in “continuous innovative change with the universe” (Barrett, 1990b, p. 35). The health-related change modalities allow for change; they do not require it. Nurses currently assist clients in the use of meditation, music, art, imagery, visualization, and therapeutic touch with a primary focus of patterning of the human field. Additional practice modalities based on motion, sound, light and color, humor, relaxation, nutrition, affirmation, art and nature, bibliotherapy, and journal keeping are all potentials for patterning. The nurse remembers that the human/environmental field is one without boundaries. “Human energy fields are integral with environmental energy fields; both fields change together toward greater diversity in field patterning” (Yarcheski, Mahon, & Yarcheski, 2004, p. 73). Awareness centers on perception of the human field, as it manifests the human/environmental field process. Centering is vital to all modalities for the nurse and the client. With centering, the client focuses on his or her core or energy field. Centering may be perceivable as a harmonious field manifestation. All manifestations, including those called illness, emerge from the mutual human/environmental field process. Patterning activities assist the client to move to and focus on emergent patterns.
Manifestations emerge from the human/environmental field process. The environment, with its healing quality, or lack of dissonance, is a vital component of patterning. Wholeness implies concern with the totality of the human/environmental field manifestation. The key is integrality—energy patterns flowing through energy patterns. The nurse works with the client in the context of the client’s family, community, and cultural group. The nurse’s concern for unitary human beings incorporates other nurses and health care providers, as well as the family, in the patterning. The nurse recognizes that pattern manifestations as perceived in the attitudes, intentions, and feelings of those with whom the client works are integral to the person/environmental field manifestation. Color, light, sound, and smell are manifestations of the environmental field. Harmony of the fields proposes increased potential for change (Davidson, 2001).
Evaluation
Evaluation is ongoing and simultaneous with appraisal and patterning. Emphasis is placed on identifying perceptions of desire for change. The evaluation process is ongoing and fluid as the nurse reflects on his or her intuitive knowing. Evaluation provides insight as the nurse integrates the pattern appraisal into all components of the nurse/unitary human process of care. The perceptions are then shared with the client and family/friends. Further mutual patterning is guided by the perceptions that emerge. This simultaneous process continues as long as the nurse-client relationship continues.
Analysis and Synthesis
The Rogerian model provides a challenging and innovative means of planning and implementing client care. The abstract ideas presented in Rogers’ model are fertile for fostering theoretical conceptualizations and applications in patient care. The concept of unitary human beings and wholistic approaches offer opportunities for nurses to design and implement innovative healing environments. Creative modalities are continually being designed and implemented for pattern appraisal and patterning processes.
Care of Debbie with Rogers’ Model
Consistent with the Rogerian model, the process of caring for Debbie centers on the mutual process of pattern appraisal, mutual patterning, and reappraisal.
Pattern Appraisal
This appraisal is grouped into exchanging patterns, communication patterns, and relating patterns. The visible human pattern manifests dissonance in elimination (difficulty urinating), pain, extreme underweight, and cancer. The manifestations of vital signs, pathology reports, and lab reports become integral with the pattern appraisal. Dissonance is noted in the progression of the disease and in her pain. Appraisal of Debbie’s sleep patterns, her nutritional status, and her perceptions of self and of healthful or harmonious existence is needed. The history is integral to the pattern appraisal. Debbie has a pattern of smoking, which has been associated with less-than-optimal health manifestation. This visible rhythmical pattern is a manifestation of evolution toward dissonance. In addition, Debbie has a pattern manifestation that has been labeled cervical cancer. This emergent pattern manifests as dissonant.
Communication patterns manifest as dissonant as Debbie has a low educational level, which is relevant as patterning activities are introduced. Sensory data add to the pattern appraisal. Through language, Debbie identifies a perception of dissonance with her husband and with her environment, which she describes as “unsanitary.” Communication dissonance manifests as being withdrawn and emotionally distant from her husband. Relating dissonance is manifested as unclean environment. Providing care within the Rogerian model emphasizes the self-articulation of personal pattern manifestations and self-knowledge.
Relating manifestations are identified as anxious or being withdrawn is integral to the appraisal. Using Power as knowing participation in change to guide the care the nurse dialogues with Debbie and her family to answer questions and give guidance related to potential issues, which may emerge. The entire family becomes the center of the phenomenon and patterning activities involve all. The pattern appraisal is ongoing. Debbie is encouraged to use verbal and intuitive capacity to access manifestations. Sensory data are gained through language, feelings, and perceptions. The nurse has reported that Debbie has a manifestation of fear. Debbie reports the fear of inability to manage her life since the onset of this illness, and the nurse senses this manifestation of fear. Debbie’s self-knowledge links the illness to her personal belief of being punished for past mistakes. History and focusing on the relative present to explore the pattern of punishment are imperative. It is important that the nurse appraise the environment of the hospital and of the others who share her existence. Debbie reports fear, a manifestation of dissonance.
Time with the nurse is needed to foster this comprehensive appraisal of Mary. During this entire process the nurse must rely heavily on personal intuition and insight regarding the pattern that is emergent with Debbie. All of the knowledge gained forms the unitary pattern of Debbie. The ongoing pattern appraisal is shared with the client. Emphasis can be placed on areas in which dissonance and harmonyare noted in the personal and environmental field manifestations. Consensus needs to be reached with Debbie before and while patterning activities are suggested and implemented.
Mutual Patterning
Dissonance can be perceived in many aspects of Debbie’s appraisal. Environmental harmony is lacking, as is noted in Debbie’s perception of it as unsanitary. In addition, dissonance is perceived with respect to her relationship with her husband. Personal dissonance is noted in the manifestations of cancer, weight loss, pain, nausea, and tobacco use. This dissonance is also conceptualized as fear in Debbie’s words and in the emotional distance that she feels. The pattern appraisal is shared with the client. Emphasis is placed on areas in which dissonance and harmony are noted in the personal and environmental field manifestations. Consensus is reached with Debbie before patterning activities can be suggested and implemented.
Many patterning modalities can be introduced. The process is mutual between the nurse and the client. Surgery is a patterning activity. Manifestations will evolve from the surgical intervention and will require reconceptualization and validation with the patient. Medications are patterning modalities. Debbie is receiving medications. Decisions are made in conjunction with Debbie regarding the use of the medications and the patterning that emerges with the introduction of these modalities. Personal knowledge regarding the surgery and the medications empowers Debbie to be integral in the selection of modalities. Debbie possesses freedom and involvement in the selection of modalities. Possible options include therapeutic touch, humor, meditation, visualization, and imagery. Debbie is assessed regarding her ability to understand and select different patterning modalities. Therapeutic touch is introduced to Debbie. The touch is introduced and incorporated into the management of pain manifestations. Touch, in combination with medications, provides patterning that Debbie can direct. The nurse introduces the process of touch to Debbie’s husband and teaches him how to incorporate touch into his wife’s care. This option would be acceptable only if Debbie feels safe being touched by her spouse. Another option is to teach Debbie how to center her energy and channel her energy to the area in pain. Patterning directed at the manifestation of fear is introduced. Options that include imagery, music, light, and meditation are discussed. Fear manifests as apprehension of self-catheterization. Emphasis is placed on having Debbie direct how, where, when, and by whom the self-catheterization will be taught.
Evaluation
Establishing a rhythm to the catheterization schedule that is harmonious with Debbie’s life reduces dissonance. Patterning of nutrition and catheterization based on the pattern appraisal assists in empowering Debbie to learn self-catheterization. A rhythm that is harmonious with Debbie and her energy field rhythm evolves. Specific actions of the nurse with respect to language and knowledge about the catheterization process empower Debbie to direct this phase of her treatment.
Nursing Care of Mary with Rogers’ Model
Nursing care for Mary is guided by the components of Gulliver’s Theory of Self-Transcendence. Self-transcendence at the end of life is a process of merging of the past, present, and future. Nursing care for Mary offers the opportunity to incorporate a variety of patterning activities. Patterning activities will be directed by the knowledge gained during the appraisal. As Mary nears and prepares for the end of her life, many patterning concerns must be addressed for peaceful closure to her life and the change to another energy form.
Pattern Appraisal
The visible rhythmical pattern is a manifestation of peace (Mary) and a human environmental manifestation of anxiety in husband. The pattern is one of movement toward transcendence and death for Mary and many unknowns for Tom and Mary. Using Power as knowing participation in change to guide the care the nurse dialogues with Mary and Tom to answer questions and give guidance related to potential issues, which may emerge. The entire family becomes the center of the phenomenon and care incorporates all. The unknown and preparation for loss is the focus. The pattern appraisal is ongoing. Mary is verbal and intuitive. She readily shares with others the story of her journey with cancer. A sense of sadness and communion with others is perceived.
Dissonance is noted in the progression of the disease, in her pain. Harmony is noted in her relationship with her husband and family and with her sense of how she has progressed through this disease process. Mary has a great deal of knowledge about herself and about the disease.
Sensory data are gained through language, feelings, and perceptions. The nurse perceives that much attention to sensory information is needed. Mary has a great deal to share about her feelings regarding the disease and her thoughts and fears. Dissonance is perceived through her acknowledgment of fear and apprehension regarding her future. It is known that pain is a major component of end of life. Therefore, the pattern appraisal (using all senses) to access the level of comfort ofMary is vital. Pain often manifests as a perceived dissonance. Use of touch to assess and care for Mary is vital to the mutual patterning of Mary and Tom during this transition.
This same appraisal tool can be given to Tom as he cares for her. Evaluation is ongoing and integral to pattern appraisal and not a separate component. Mary and Tom are offered ways to ease pain, discuss fears and concerns and encouraged to pattern their environmental field in ways that are conducive to peace and comfort manifestations. Language provides a valuable addition to the pattern appraisal of Mary and Tom.
Appraisal of Mary’s sleep patterns, her nutritional status, and her perceptions of self and of healthful or harmonious existence is needed. This appraisal can be grouped into exchanging patterns, communication patterns, and relating patterns, as discussed previously. Time with the nurse is needed to foster this comprehensive appraisal of Mary. During this entire process the nurse relies heavily on personal intuition and insight regarding the pattern that is emergent with Mary. All of the knowledge gained forms the unitary pattern of Mary.
Dissonance is perceived in many aspects of Mary and Tom’s appraisal. Personal dissonance is noted in the manifestations of cancer, weight loss, pain, and nausea for Mary. Dissonance is recognized as fear in Mary and Tom as they discuss Mary’s care since she is home.
Mutual Patterning
Many patterning modalities can be discussed. The process is mutual between the nurse and the client. Mary is receiving medications. Decisions are made in conjunction with Mary regarding the use of the medications. Personal knowledge regarding the medications empowers Mary to be integral in the selection of modalities. Mary possesses freedom and involvement in the selection of modalities. Possible options include therapeutic touch, humor, meditation, visualization, and imagery. Therapeutic touch can be introduced to Mary. The touch is introduced and incorporated into the management of pain manifestations. Touch, in combination with medications, is patterning that Mary can direct. The nurse may introduce the process of touch to Tom and teach him how to incorporate touch into his wife’s care. Another option would be to teach Mary how to center her energy and channel her energy to the area in pain. Patterning directed at the integration of past, present, and future is offered to foster self-transcendence. Options that include journaling, imagery, music, light, and meditation can be discussed. A rhythm that is harmonious with Mary and her energy field rhythm will evolve. The entire family is involved in power as knowing participation in change. Language and the use of language are explored to determine what patterning Mary would prefer.
Evaluation
The appraisal process again is ongoing and integrated throughout the care. Specific emphasis is placed on emergent patterns of dissonance or harmony that are evident.
Manifestations of pain, fear, and tension with family members are appraised. A summary of the pattern appraisal is shared with Mary, and mutual patterning is modified or instituted as indicated based on the evaluation.
Options regarding how her physical space is oriented, decorated, and located are explored in the patterning of Mary. She and her family are given latitude in bringing personal effects, artwork, children’s drawings, and photographs. The bed is turned to face the window at Mary’s request. A favorite rocker and a bright rug for the floor are brought into the room. Mary elects to place a beautiful cloth over her bedside table and has her small weaving loom placed in the room. The room radiates a sense of peace, and the feeling of the illness is lost. According to Rogers (1992), dying is moving beyond the pattern visible to human perception. Death is a transformation of energy (Rogers, 1970). At death, the human field ceases to exist and identity as a living human being is gone. The process of dying is a period of transition in which the integrity of the human field as such diminishes and dies (Rogers, 1970). As the pattern of cancer evolves for Mary, manifestations of pain increase and the reality of impending death emerges. Nursing care revolves around the introduction of modalities to assist Mary and her family as the human/environmental field evolves.