Roy’s Adaptation Model in Nursing Practice
Kenneth D. Phillips and Robin Harris
Adaptation is viewed as the process and outcome whereby thinking and feeling persons, as individuals or in groups, use conscious awareness and choice to create human and environmental integration.
Human beings incessantly respond to myriad internal and external environmental stimuli. A stimulus is any entity that provokes a response (Andrews & Roy, 1991a) and that serves as the point of interaction between the person and the environment (Roy & Andrews, 1999). Environmental stimuli either threaten or enhance an individual’s ability to adapt. As an example, loving, supportive behaviors from a parent enhance a child’s ability to successfully adapt, whereas a hostile, abusive parent poses a threat to a child’s adaptation.
Nursing plays a vital role in assisting individuals who are sick or well to respond to a variety of new stressors, move toward optimal well-being, and improve the quality of their lives through adaptation. The Roy Adaptation Model (Roy & Andrews, 1991) provides an effective framework for addressing the adaptive needs of individuals, families, and groups.
As noted in Chapter 1, nursing’s most pressing question is the following: “What is the nature of the knowledge that is needed for the practice of nursing?” Nurses practicing within the Roy Adaptation Model seek the following:
• Greater knowledge of factors that either promote or hinder adaptation
• Better methods and tools for assessing adaptation level
• Specific nursing interventions that either promote or hinder adaptation
• Effective methods for evaluating adaptation as an outcome of nursing care
History and Background
Sister Callista Roy, a Sister of Saint Joseph of Carondelet, developed the Roy Adaptation Model (RAM) in 1964 in response to a challenge by her professor, Dorothy E. Johnson. Since that time, the RAM has been reconceptualized for use in the twenty-first century. The development of the model has been a dynamic process. The preliminary ideas of this conceptual framework were first published in an article titled Adaptation: A Conceptual Framework for Nursing (Roy, 1970). The RAM continues to be refined. The RAM is presented in its most complete and recent form in The Roy Adaptation Model (Roy & Andrews, 1999). Nurses in the United States, in Canada, and around the world practice nursing from the perspective of RAM. The RAM has stimulated other scholars to publish books of their own about adaptation nursing (Rambo, 1984; Randell, Poush Tedrow, & Van Landingham, 1982; Welsh & Clochesy, 1990), has been implemented in numerous hospitals and other health care settings, and has been applied to diverse populations, adaptive needs, and developmental stages (Fawcett, 2005; Phillips, 2006).
Overview of Roy’s Adaptation Model
The RAM provides a useful framework for providing nursing care for persons in health and in acute, chronic, and terminal illness. The RAM views the person as an adaptive system in constant interaction with an internal and external environment. The environment is the source of a variety of stimuli that either threaten or promote the person’s unique wholeness. The person’s major task is to maintain integrity in the face of these environmental stimuli. Integrity is “the degree of wholeness achieved by adapting to changes in needs” (Roy & Andrews, 1999, p. 102). Roy, drawing on the work of Helson (1964), categorizes these types of stimuli as focal, contextual, or residual. The first type of stimulus, focal, is defined as the internal or external stimulus most immediately challenging the person’s adaptation. The focal stimulus is the phenomenon that attracts the most of one’s attention. Contextual stimuli are all other stimuli existing in a situation that strengthen the effect of the focal stimulus. Residual stimuli are any other phenomena arising from a person’s internal or external environment that may affect the focal stimulus but whose effects are unclear (Roy & Andrews, 1999). The three types of stimuli act together and influence the adaptation level, which is a person’s “ability to respond positively in a situation” (Andrews & Roy, 1991a, p. 10). A person’s adaptation level may be described as integrated, compensatory, or compromised (Roy & Andrews, 1999).
A person does not respond passively to environmental stimuli; the adaptation level is modulated by a person’s coping mechanisms and control processes. Roy categorizes the coping mechanisms into either the regulator or the cognator subsystem. The coping mechanisms of the regulator subsystem occur through neural, chemical, and endocrine processes. The coping mechanisms of the cognator subsystem occur through cognitive-emotive processes. Roy has identified two control processes that coincide with the regulator and cognator subsystems when a personresponds to a stimulus. The control processes identified by Roy are the stabilizer subsystem and the innovator subsystem. The stabilizer subsystem refers to “the established structures, values, and daily activities whereby participants accomplish the primary purpose of the group and contribute to common purposes of society” (Roy & Andrews, 1999, p. 47). The innovator subsystem refers to cognitive and emotional strategies that allow a person to change to higher levels of potential (Roy & Andrews, 1999).
Although direct observation of the processes of the regulator and cognator subsystems is not possible, Roy proposes that the behavioral responses of these two subsystems can be observed in any of the four adaptive modes: physiological, self-concept, role function, and interdependence adaptive modes. Roy and her associates describe the function of the adaptive modes in the Theory of the Person as an Adaptive System (Andrews & Roy, 1991a).
Roy’s Theory of the Person as an Adaptive System postulates that the four adaptive modes are interrelated through perception. Either an adaptive response or an ineffective response in one mode influences adaptation in the other modes.
The physiological adaptive mode refers to the “way a person responds as a physical being to stimuli from the environment” (Andrews & Roy, 1991a, p. 15). The five physiological needs of this mode are oxygenation, nutrition, elimination, activity and rest, and protection. Four complex processes that mediate the regulatory activity of this mode are senses, fluids and electrolytes, neurological function, and endocrine function. Physiological integrity is the adaptive response of this adaptive mode (Andrews & Roy, 1991a, 1991c).
The self-concept adaptive mode refers to psychological and spiritual characteristics of the person (Andrews, 1991b; Andrews & Roy, 1991a; Roy & Andrews, 1999). A person’s self-concept consists of all the beliefs and feelings that one has formed about oneself. The self-concept is formed both from internal perceptions and from the perceptions of others. The self-concept changes over time and guides one’s actions. The self-concept incorporates two components: the physical self and the personal self. The physical self incorporates body sensation and body image (Buck, 1991b). The personal self incorporates self-consistency, self-ideal, and moral-ethical-spiritual self (Buck, 1991a). Psychic integrity is the goal of the self-concept mode (Andrews, 1991b; Andrews & Roy, 1991a).
The interdependence adaptive mode refers to coping mechanisms arising from close relationships that result in “the giving and receiving of love, respect, and value” (Andrews & Roy, 1991a, p. 17). In general, these contributive and receptive behaviors occur between the person and the most significant other or between the person and his or her support system. Affectional adequacy is the goal of the interdependence adaptive mode (Roy & Andrews, 1999; Tedrow, 1991).
The role function adaptive mode refers to the primary, secondary, or tertiary roles the person performs in society. According to Andrews and Roy (1991a), “A role, as the functioning unit of society, is defined as a set of expectations about how a person occupying one position behaves toward a person occupying another position” (p. 16). Social integrity is the goal of the role function mode (Andrews, 1991a; Nuwayhid, 1991; Roy & Andrews, 1999).
Adaptive or ineffective responses result from these coping mechanisms. Adaptive responses promote the integrity of the person and the goals of adaptation. The major task of a person is to adapt to environmental stimuli to achieve survival, growth, development, and mastery. Ineffective responses neither promote integrity nor contribute to the goals of adaptation (Andrews & Roy, 1991a).
As described earlier, adaptation is accomplished through two main coping subsystems: regulator and cognator. The mechanisms of regulator and cognator have not been explicated by Roy because these mechanisms cannot be directly observed and remain largely unknown. However, the behaviors of regulator and cognator are manifested indirectly and can be observed and measured in the four adaptive modes (Roy, 1981).
Roy and Andrews (1999) define health as “a state and a process of being and becoming an integrated and whole person” (p. 31). Health is a reflection of how successfully an individual has adapted to environmental stimuli. The goal of nursing therefore is to help a person achieve adaptation by helping the person survive, grow, reproduce, and master. Adaptation leads to optimum health and well-being, to the highest quality of life possible, and to death with dignity (Andrews & Roy, 1991a). Adaptation enables the person to find meaning and purpose in life and to become an integrated whole.
Critical Thinking in Nursing Practice with Roy’s Model
The nursing process is a goal-oriented, problem-solving approach to guide the provision of comprehensive, competent nursing care to a person or groups of persons. According to Andrews and Roy (1991b), the nursing process “relates directly to the view of the person as an adaptive system” (p. 27). Roy has conceptualized the nursing process to comprise the following six simultaneous, ongoing, and dynamic steps (Roy & Andrews, 1999):
Each of these phases of the nursing process is discussed within the RAM. The goal of nursing in the RAM is to promote adaptation in each of the four adaptive modes (Roy & Andrews, 1999).
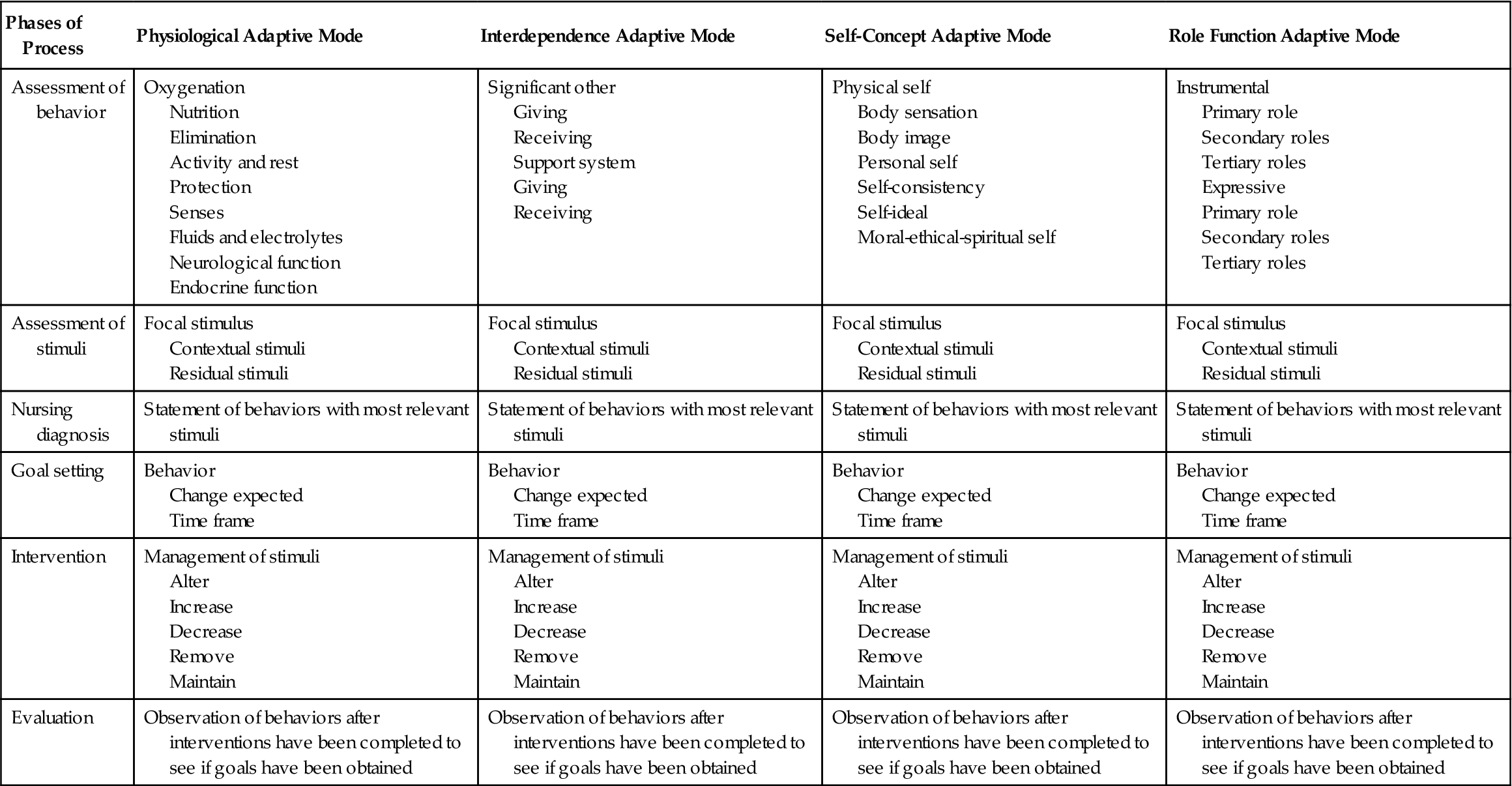
The nursing process alone is limited in promoting critical thinking; however, nursing theory serves as a guide for nursing care. Nursing theory directs the practitioner toward important aspects of assessing, planning, goal setting, implementation, and evaluation. Furthermore, practice within a model allows the practitioner to ignore irrelevant considerations and to selectively choose among a variety of nursing strategies. Another way of saying this is that nursing theory promotes critical thinking. Table 14-1 illustrates how the RAM guides the nurse through the critical thinking process.
TABLE 14-1
Critical Thinking in the Roy Adaptation Model
| Phases of Process | Physiological Adaptive Mode | Interdependence Adaptive Mode | Self-Concept Adaptive Mode | Role Function Adaptive Mode |
| Assessment of behavior | Oxygenation Nutrition Elimination Activity and rest Protection Senses Fluids and electrolytes Neurological function Endocrine function |
Significant other Giving Receiving Support system Giving Receiving |
Physical self Body sensation Body image Personal self Self-consistency Self-ideal Moral-ethical-spiritual self |
Instrumental Primary role Secondary roles Tertiary roles Expressive Primary role Secondary roles Tertiary roles |
| Assessment of stimuli | Focal stimulus Contextual stimuli Residual stimuli |
Focal stimulus Contextual stimuli Residual stimuli |
Focal stimulus Contextual stimuli Residual stimuli |
Focal stimulus Contextual stimuli Residual stimuli |
| Nursing diagnosis | Statement of behaviors with most relevant stimuli | Statement of behaviors with most relevant stimuli | Statement of behaviors with most relevant stimuli | Statement of behaviors with most relevant stimuli |
| Goal setting | Behavior Change expected Time frame |
Behavior Change expected Time frame |
Behavior Change expected Time frame |
Behavior Change expected Time frame |
| Intervention | Management of stimuli Alter Increase Decrease Remove Maintain |
Management of stimuli Alter Increase Decrease Remove Maintain |
Management of stimuli Alter Increase Decrease Remove Maintain |
Management of stimuli Alter Increase Decrease Remove Maintain |
| Evaluation | Observation of behaviors after interventions have been completed to see if goals have been obtained | Observation of behaviors after interventions have been completed to see if goals have been obtained | Observation of behaviors after interventions have been completed to see if goals have been obtained | Observation of behaviors after interventions have been completed to see if goals have been obtained |
Assessment of Behavior
From Roy’s perspective, behavior is an action or a reaction to a stimulus. A behavior may be observable or nonobservable. An example of an observable behavior is pulse rate; a nonobservable behavior is a feeling experienced by the person and reported to the nurse. Exploration of behaviors manifested in the four adaptive modes allows the nurse to achieve an understanding of the current adaptation level and to plan interventions that will promote adaptation. At the beginning of thenurse-client relationship, a thorough assessment of behavior must be performed (Roy & Andrews, 1999) and the assessment must be ongoing. Table 14-1 presents categories of behaviors that are assessed in each of the adaptive modes.
Assessment of Stimuli
A stimulus is any change in the internal or external environment that induces a response in the adaptive system. Stimuli that arise from the environment can be classified as focal, contextual, or residual. In this level of assessment, the nurse analyzes subjective and objective behaviors and looks more deeply for possible causes of a particular set of behaviors (Roy & Andrews, 1999).
Nursing Diagnosis
A nurse’s education and experience enable him or her to make an expert judgment regarding health care and adaptive needs of the client. This judgment is expressed in a diagnostic statement that indicates an actual or a potential problem related to adaptation. The diagnostic statement specifies the behaviors that led to the diagnosis and a judgment regarding stimuli that threaten or promote adaptation (Roy & Andrews, 1999). The RAM defines nursing diagnosis “as a judgment process resulting in statements conveying the adaptation status of the human adaptive system” (Roy & Andrews, 1999, p. 77).
Goal Setting
Goal setting focuses on promoting adaptive behaviors. Together the nurse and the client agree on clear statements about desired behavioral outcomes of nursing care. The outcome statement should reflect a single adaptive behavior, be realistic, and be measurable. The goal statement should include the behavior to be changed, the change expected, and the time frame in which the change in behavior should occur (Roy & Andrews, 1999).
Intervention
According to Andrews and Roy (1991b), “Intervention focuses on the manner in which goals are attained” (p. 44). A nursing intervention is any action taken by a professional nurse that he or she believes will promote adaptive behavior by a client. Nursing interventions arise from a solid knowledge base and are aimed at the focal stimulus whenever possible (Andrews & Roy, 1991b). Intervention is any nursing approach that is intended “to promote adaptation by changing stimuli or strengthening adaptive processes” (Roy & Andrews, 1999, p. 86).
Evaluation
In the RAM, evaluation consists of one question: “Has the person moved toward adaptation?” Evaluation requires that analysis and judgment be made to determine whether those behavioral changes stated in the goal statement have, or have not, been achieved by the recipient of nursing care (Andrews & Roy, 1991b). In the evaluation phase, the nurse judges the effectiveness of the nursing interventions that have been implemented and determines to what degree the mutually agreed upon goals have been achieved (Roy & Andrews, 1999).
Nursing Care of Debbie with Roy’s Model
Physiological Adaptive Mode
Debbie’s health problems are complex. It is impossible to develop interventions for all of her health problems within the space of this chapter; therefore, representative examples are presented.
Assessment of Behavior
Postoperatively, Debbie has been unable to completely empty her urinary bladder. She states that she is numb and unable to tell when she needs to void. Catheterization for residual urine revealed that she was retaining 300 ml of urine after voiding. It will be necessary for her to perform intermittent self-catheterization at home. Unsanitary conditions at Debbie’s home place her at high risk for developing a urinary tract infection. She states that she is scared about performing self-catheterization.
Assessment of Stimuli
In this phase of the nursing process, the nurse searches for stimuli responsible for the observed behavior. After stimuli have been identified, they are classified as focal, contextual, or residual.
The focal stimulus for Debbie’s urinary retention is the disease process. Contextual stimuli include tissue trauma resulting from surgery and radiation therapy. Debbie verified anxiety as a residual stimulus.
Infection is a potential problem. The focal stimulus is the need for intermittent self-catheterization. Contextual stimuli include altered skin integrity related to surgical incision, poor understanding of aseptic principles, and unsanitary conditions at Debbie’s home.
Nursing Diagnosis
From the assessment of behaviors and the assessment of stimuli, the following nursing diagnoses were made:
• Altered elimination: urinary retention related to surgical trauma, radiation therapy, and anxiety
• Potential for infection related to intermittent self-catheterization, altered skin integrity related to surgical incision, poor understanding of aseptic principles, and unsanitary conditions at Debbie’s home
Goal Setting
Goals were set mutually between the nurse and the client for each of the nursing diagnoses. The goals were the following:
Intervention
To help Debbie attain these goals, the following nursing interventions were implemented:
Debbie was taught the importance of performing intermittent self-catheterization every 4 hours to prevent damage to the urinary bladder and kidney. She was taught to assess her abdomen for bladder distention and the proper procedure for intermittent self-catheterization. She was instructed to keep a record of the exact time and amount of voiding and catheterizations. In addition, Debbie was taught relaxation techniques to facilitate voiding so that it would not be necessary for her to catheterize herself as often.
• Potential for infection related to intermittent self-catheterization, altered skin integrity related to surgical incision, poor understanding of aseptic principles, and unsanitary conditions at Debbie’s home
Debbie was taught the importance of washing hands before touching the surgical incision or doing incision care. Following a demonstration of incision care bythe nursing staff, Debbie was asked to perform a return demonstration. After the intermittent self-catheterization procedure was explained and demonstrated, Debbie performed a return demonstration with good technique.
Evaluation
Evaluation of Debbie’s adaptive level was performed each shift. Significant findings included the following:
• It will be necessary for Debbie to perform intermittent self-catheterization at home. She was able to state the importance of performing intermittent self-catheterization on a regular basis. She performed a return demonstration of intermittent self-catheterization before discharge, and she was able to adequately adhere to aseptic principles during the procedure. She accurately recorded the times and amount for each voiding and catheterization.
• Debbie was able to list the signs and symptoms of a wound and a urinary tract infection and to state appropriate steps to take if symptoms occur (i.e., notify physician or nurse practitioner). She was able to discuss the importance of maintaining adequate oral fluid intake. Debbie was given a thermometer and instructed in its use. She correctly demonstrated taking a temperature.
Interdependence Adaptive Mode: Assessment of Behavior
Significant Other
Debbie’s most significant other is her husband. She describes her husband as emotionally distant and abusive at times. He has been at the bedside since Debbie was admitted to the hospital. He appears worried. In addition to these findings, it would be important to determine how Debbie and her husband give and receive love, value, and respect and how they express nurturing and caring behaviors to each other.
Support System
Debbie’s support system includes her mother and her two children. Debbie and her family live in her mother’s home. It is important to know how Debbie and her support system give and receive love, value, and respect and how they express nurturing and caring behaviors to each other.
Assessment of Stimuli
Assessment of stimuli within the interdependence adaptive mode reveals that Debbie’s relationship needs with her husband are not being met. It is encouraging that her husband is displaying nurturing, caring behaviors while Debbie is in the hospital. Further evaluation of Debbie’s self-esteem would be warranted. Debbie and her husband were married at an early age. Their knowledge regarding building friendships and relationships may be limited. It would be important to assess modes of communication as well. The developmental stage for Debbie and her husband is that of young adults. In this stage, the individual becomes independent and establishes his or her own family. Debbie and her family live with her mother. This maybe creating a stress on interdependence. Debbie acknowledges that she and her husband have very little time alone.
The focal stimulus in the interdependence adaptive mode is an emotionally distant relationship with her husband. Contextual stimuli are the following:
Nursing Diagnosis
The following nursing diagnoses of interdependence adaptive needs were made:
• Affectional inadequacy related to emotionally distant relationship, marriage at an early age following an unplanned pregnancy, ineffective communication skills, living with a parent, and having very little time alone
• Potential change in support system dynamics related to potential role changes and changes in health status
Goal Setting
To help Debbie with these adaptive needs, she and the nurse agreed on the following goals:
Intervention
To help Debbie attain these goals, the following nursing interventions were implemented:
• Affectional inadequacy related to emotionally distant relationship, marriage at an early age following an unplanned pregnancy, ineffective communication skills, living with a parent, and having very little time alone
Assessment of interdependence was begun while performing other routine care. Debbie was asked the following questions:
• Can you tell me about your relationship with your husband?
• Do you consider it a good relationship?
• What do you think would make it a good relationship?
• How does your husband express to you that he loves you?
• How do you express to your husband that you love him?
• How do you and your husband talk about things important to you?
Debbie’s husband has been with her much of the time she has been hospitalized, and he seemed worried. Her husband was encouraged to massage Debbie’s back when she was experiencing pain or to just hold her hand when she became tearful.
• Potential change in support system dynamics related to potential role changes and changes in health status
With Debbie’s permission, time was allocated to discuss important aspects of relationship building. Both Debbie and her husband were agreeable. Professional family counseling services were obtained for Debbie’s family through the hospital’s parish nursing ministry.
Evaluation
Debbie was pleased that her husband was talking to her more frequently, and she enjoyed the caring behaviors in which he was participating. They began their counseling sessions before Debbie’s discharge. They both resolved to spend more time alone. They both felt the counseling was worthwhile and wanted to continue the sessions after discharge.
Self-Concept Adaptive Mode
Assessment of Behavior
Debbie is extremely tearful. She expresses great concern over her future and the future of her children. Exploration of Debbie’s tearfulness revealed that she was afraid of dying. She believes that this illness is a punishment for her past behavior. Debbie and her husband were married at a very young age after Debbie became pregnant with their first child.
Debbie has not asked the nurse any questions about sexuality. Her hesitancy to introduce the subject may be related to her cultural background. In this case, the nurse introduces the topic. Salient findings include the following:
• Debbie recently learned of a diagnosis of cervical cancer.
• She has undergone a recent radical hysterectomy.
• She is receiving radiation therapy in the hospital, and the need for this therapy will continue at home.
• Debbie has a lack of information about the effect of cervical cancer, radical hysterectomy, and radiation therapy on sexuality.
• Debbie has unresolved guilt related to unplanned premarital pregnancy.
Assessment of Stimuli
Debbie is a young adult, is married, and has two young children. Debbie has an eighth-grade education. She is in an emotionally distant, sometimes abusive relationship. Being diagnosed with cervical cancer at an early age has resulted in a maturational crisis for Debbie. This is complicated by the fact that several of her relatives have died of cancer. It is important for the nurse to assess coping strategies. One coping strategy that is mentioned is that Debbie is frequently tearful; crying is therapeutic.
Nursing Diagnosis
The following nursing diagnoses were made:
• Fear and anxiety of dying related to medical diagnosis and witnessing other family members’ deaths as a result of cancer
• Spiritual distress related to severe life-threatening illness and unresolved guilt related to unplanned premarital pregnancy
• Sexual dysfunction related to the disease process; recent radical hysterectomy; need for radiation therapy at home; loss of childbearing capacity; weakness; fatigue; pain; anxiety; hormonal changes; and a lack of information about the effect of cervical cancer, radical hysterectomy, and chemotherapy on sexuality
• Grieving related to body image disturbance, loss of self-ideal, changes in roles, and potential for premature death
Goal Setting
To help Debbie achieve adaptation in the self-concept adaptive mode, the following goals were mutually set:
• Decreased fear and anxiety of dying as evidenced by less tearfulness, relaxed facial expression, relaxed body movements, verbalization of new coping strategies, and fewer verbalizations of fear and anxiety
• Decreased spiritual distress as evidenced by verbalization of positive feelings about self, verbalization about the value and meaning of her life, and less tearfulness
• Resumed sexual relationship that is satisfying to both partners as evidenced by verbalization of self as sexually capable and acceptable, verbalization of alternative methods of sexual expression during the first 6 weeks following surgery, and verbalization of when to be able to resume vaginal intercourse
• Progression through the grieving process as evidenced by verbalization of feelings regarding body image, self-ideal, changes in roles, and potential for premature death
Intervention
The following nursing interventions were implemented to help achieve these goals in the self-concept adaptive mode:
• Fear and anxiety of dying related to medical diagnosis and witnessing other family members’ deaths as a result of cancer
Although Debbie’s prognosis appeared good, she remained fearful of dying. Time was taken to sit with Debbie, to make eye contact, and to actively listen to her, especially when she began crying.
Debbie was asked to share an extremely difficult experience she had encountered in the past. She was asked how she coped with that experience. Once her present coping strategies were assessed, new coping strategies were suggested.
Debbie was encouraged to express her feelings openly. After allowing Debbie adequate time to express her feelings, truthful and realistic hope based on Debbie’s medical history was offered. A cancer support group met each Tuesday in the hospital where Debbie was a patient. Debbie was given a schedule of the meeting times and topics. She and her husband were encouraged to attend the cancer support group meetings.
• Spiritual distress related to severe life-threatening illness and unresolved guilt related to unplanned premarital pregnancy
Debbie was encouraged to express her feelings openly about her illness. It was suggested that times of illness are good times to renew spiritual ties. Debbie wassupported in positive aspects of her life (e.g., being a good mother). At Debbie’s request, the parish nursing ministry was consulted and a chaplain was asked to visit Debbie.
• Sexual dysfunction related to the disease process; recent radical hysterectomy; need for radiation therapy at home; loss of childbearing capacity; weakness; fatigue; pain; anxiety; hormonal changes; and a lack of information about the effect of cervical cancer, radical hysterectomy, and chemotherapy on sexuality
A complete sexual assessment was conducted to evaluate the perceived adequacy of Debbie’s sexual relationship and to elicit concerns or issues about sexuality before her diagnosis with cervical cancer. Private conversation with Debbie was initiated to gain an understanding of her sexual concerns resulting from her therapy and her beliefs about the effects of radical hysterectomy in regard to sexual functioning. Debbie was instructed regarding possible changes in sexual functioning, such as a temporary loss of vaginal sensation for up to several months, vaginal dryness, and dyspareunia resulting from vaginal dryness. Because vaginal intercourse would not be possible for up to 6 weeks, alternate forms of sexual expression were discussed. To facilitate communication and sexual expression between Debbie and her husband, long periods of uninterrupted privacy were provided.
• Grieving related to body image disturbance, loss of self-ideal, changes in roles, and potential for premature death
Debbie’s perceptions regarding the effect of the diagnosis of cervical cancer on her body image, self-ideal, roles, and her future were explored. Debbie was encouraged to verbally acknowledge the losses that she was experiencing. She was observed to determine which stage of the grief process she was currently experiencing (denial, anger, bargaining, depression, or acceptance) (Kübler-Ross, 1969). The grieving process was explained to Debbie and to her family, and they were assured that grieving is a normal process. Family members were encouraged to allow Debbie to cry when she needed to cry and to talk about her fears and feelings of grief. The nursing staff offered realistic reassurance about Debbie’s prognosis. Debbie was encouraged to attend the cancer support group so that she could talk to others who better understood her grief.
Evaluation
Debbie’s behavior changed before discharge. At the cancer support group Debbie met Marie, a survivor of cervical cancer. After meeting Marie, Debbie became more hopeful that she could conquer cancer. Less tearful, Debbie appeared more relaxed. Debbie verbalized a good understanding of the sexual changes that would occur and ways to help her adapt to these changes.
Role Function Adaptive Mode
Assessment of Behavior
Assessment in the role function adaptive mode requires the nurse to identify primary, secondary, and tertiary roles. When these roles have been identified, the nurse looks for instrumental and expressive behaviors related to each of these roles. An instrumental behavior is an actual physical act performed by the individual that helps achieve the goal of mastery of a primary, secondary, or tertiary role. Anexpressive behavior is the attitude or feeling a person holds about a primary, secondary, or tertiary role.
Assessment of behaviors in the role function adaptive mode revealed that Debbie loves her husband very much and wants things to be better for them. She is a conscientious mother. She is a dutiful daughter who assists her mother as needed. She enjoys helping elders in her community because it makes her feel good to help others when they need it. She has been diagnosed with cervical cancer, has undergone a radical hysterectomy, and is being treated with radiation therapy.
Assessment of Stimuli
The focal stimulus in the role function adaptive mode is the fear of not being able to care for herself or her children in the future. Contextual stimuli include severe illness, radiation therapy, weakness, fatigue, and increased dependency on others.
Nursing Diagnosis
Goal Setting
To help Debbie achieve adaptation in the role function adaptive mode, the following goals were mutually set:
• Effective primary role transition as manifested by less weakness, less fatigue, willingness to allow others to help her when she needs assistance, and desire to resume self-care activities as she becomes able
• Effective secondary role transition as manifested by fewer verbalizations of anxiety over her ability to care for herself and her children in the future
Intervention
The following nursing interventions were implemented to help achieve these goals in the role function adaptive mode:
• Ineffective primary role transition related to severe illness, radiation therapy, weakness, fatigue, and increased dependency on others
Debbie was monitored for factors that would hinder her from performing self-care activities. A daily routine was established that incorporated periods of activity and periods of rest. Measures were implemented to promote rest (e.g., activity restrictions, minimal noise, restricted visitation, a morning and afternoon nap time, assistance with personal care, needed items close to her bed, back massage, progressive relaxation, guided imagery, soft music). However, maximum independence was encouraged. Family members were instructed regarding the importance of maintaining independence. Debbie was given positive reinforcement for successful accomplishment of self-care behaviors.
Debbie was praised for her performance of her primary, secondary, and tertiary roles. Resumption of these roles was discussed with Debbie. Debbie was asked to identify her support system. She felt that at home she had adequate support for performing her roles. She was encouraged to rely on her support system for help when needed in maintaining these roles.
• Ineffective secondary role transition related to fear of not being able to care for herself or her children in the future
A thorough assessment was performed to gain an understanding of Debbie’s fears and misconceptions about the effects of cancer, radical hysterectomy, and radiation therapy on bodily functioning, her lifestyle, and her ability to perform roles. Debbie verbalized a fear of dying and leaving her children. Interventions to instill hope were implemented. For instance, Debbie was given realistic assurance about her expected prognosis.
Evaluation
Debbie’s husband was exhibiting supportive behaviors in the hospital. Debbie’s mother was at home to help Debbie when she arrived. As Debbie’s energy level increased, she became less anxious about her future. Before discharge, Debbie became increasingly anxious to return home to her children.
Nursing Care of David with Roy’s Model
Assessment of Behavior
David is a 48-year-old who suffered an anterior wall myocardial infarction (MI) 3 weeks ago. Prior to his MI, he was active and exercised regularly. He is a successful and respected professional in his company and in his community. He has experienced increased fatigue, shortness of breath, and lightheadedness/dizziness due to hypotension since his MI. He was admitted to the hospital last week for congestive heart failure. David is frustrated that he has limited activity tolerance due to fatigue and shortness of breath with activity. David is frustrated that he has not been able to return to his previous level of activity for his personal and professional life.
Assessment of Stimuli
Assessment of stimuli revealed the focal stimulus for David’s decreased activity tolerance was reduced left ventricular function from anterior wall MI. Contextual stimuli contributing to the decreased activity tolerance are fatigue, shortness of breath with activity, and symptomatic hypotension.
Nursing Diagnosis
The following nursing diagnoses were made in the physiological adaptive mode:
Goal Setting
Intervention
So that David could achieve his goal to improve his activity and level of understanding of ischemic heart disease, the following interventions were implemented:
David was instructed to keep a home daily weight, blood pressure, and heart rate log to document hypotension and evidence of fluid retention associated with worsening heart failure. Understanding of ischemic heart disease and signs/symptoms associated with worsening heart failure will allow David to communicate changes of his condition to his health care provider for appropriate follow-up and management of his condition. This will also allow David to take an active role in his own care and management of his health condition.
The nurse met with David and his wife to discuss David’s heart condition. The nurse discussed David’s MI and the alteration in left ventricular systolic function that occurred as a result of his MI. The importance of taking his medications as prescribed to manage his heart failure and prevent further reduction in cardiac function was reviewed with David and his wife.
Evaluation
David became more active in his care and felt more in control by keeping a daily log. By keeping this log, he was able to recognize a trend of low blood pressure readings in the evening hours that were associated with times when he was feeling more fatigued. David discussed this with his physician, who was able to adjust his medication regimen to avoid medication-related hypotension in the evening hours.
Interdependence Adaptive Mode
Assessment of Behavior
David has been active throughout his life. He has always been independent and is not used to needing or asking for any assistance with activity. Asking his wife for assistance makes David feel uncomfortable and anxious. He is concerned about returning to his previous level of function in his personal and professional life.
Assessment of Stimuli
The focal stimulus for David’s anxiety is the left ventricular dysfunction from MI. Contextual stimuli are the anxiety and dependence on family members regarding his reduced functional capacity following MI.
Nursing Diagnosis
The following nursing diagnosis of the interdependence adaptive needs was made:
Goal Setting
Intervention
To help David achieve his goal, the following nursing interventions were implemented:
David was advised to plan his activities throughout the day to avoid overexertion and increased fatigue. He was encouraged to rest between activities as needed and increase his activity gradually. David was instructed to begin walking 5 minutes daily and increase walking by 3 to 5 minutes daily to a goal of 30 minutes daily.
Evaluation
David was able to increase his daily activity without becoming overly fatigued. David planned periods of rest after activities such as showering or shaving. Over time, David was gradually able to complete his ADLs independently. David began walking each day for 3 to 5 minutes followed by a rest period. He increased his walking time gradually and was walking for 10 minutes a day by the end of the first week and for 30 minutes a day by the end of the first month.
Self-Concept Adaptive Mode
Assessment of Behavior
David verbalized that he has lost several relatives to heart disease and that he is worried about his risk of dying and leaving behind his wife and children. David expresses that he has a strong spiritual faith and that his primary concern is for his wife and children’s well-being. As part of David’s history, his nurse learned that his father died of sudden cardiac death outside the hospital at the age of 43 when David was just 13 years old.
Assessment of Stimuli
The focal stimulus in this mode is David’s anxiety about death. Contextual stimuli are the MI that he has experienced, the death of his father at an early age, and the well-being of his wife and children.
Nursing Diagnosis
The following nursing diagnosis of the self-concept adaptive mode was made:
Goal Setting
Intervention
A first step with David is to explore what he knows about his heart disease and prognosis. This provides the opportunity to provide additional education about his condition and to correct misunderstandings that he may have. Ask about his specific fears of dying. Although it seems counterintuitive, talking about one’s fear of dying helps to decrease anxiety. The nurse should provide an empathetic understanding of David’s fears and let him know that impending doom is one of the hallmark psychosocial responses to an MI. David should be encouraged to talk with his wife and spiritual counselors about his concerns. David has lost several relatives to heart disease, which may fuel his anxiety about death. The nurse can explore similarities and differences between his relatives’ heart disease and his own heart disease. For instance, knowing how long ago his relatives died may be a key factor in relieving his anxiety. The nurse can talk about new and more effective treatments that are available. Knowing his coping styles will facilitate interventions to reduce his anxiety. As an example, in a very brief intervention during routine care, David’s nurse can help move him from emotional coping to a more active problem-solving coping style while still providing emotional care. His nurse can give him control over his environment by encouraging him to make decisions about his treatment and care. The nurse can encourage him to increase his activity as he is able. His nurse can instill hope during routine encounters by providing David with information about self-care strategies that he can use to help with his recovery.
Evaluation
David will slowly take more responsibility for his own ADLs and begin to increase his activity by sitting in a chair and steadily increasing ambulation while in the hospital. In the hospital the nurse should look for signs of decreasing death anxiety such as verbalizations about the future. At home he can begin a structured exercise program that progressively returns him to his normal activities.
Role Function Adaptive Mode
Assessment of Behavior
David’s primary role is that of a middle-aged adult male. His secondary roles include husband, father, son, brother, and friend. He is an executive. He is concerned about his job and that his professional future could change due to his heart disease.
Assessment of Stimuli
The focal stimulus is reduced left ventricular function from anterior wall MI. Contextual stimuli are the potential for change in employment status and financial effect on his family.
Nursing Diagnosis
The following nursing diagnosis related to role function is:
Goal Setting
Intervention
David was encouraged to discuss his concerns with his spouse and children for open communication about his job status and effect on the family’s future. David was also encouraged to discuss his job and responsibilities with his employer.
Evaluation
David and his family developed good communication about his concerns over his responsibilities to his family as the provider and to his employer. David’s teenage children volunteered to get part-time jobs after school to help with their financial expenses. David talked to his employer, who was willing to adjust his work schedule and work responsibilities so that David would have shorter work hours and less stress. After 3 months David was able to return to his job full-time.