Exploring the potential of professional coaching for the growth of clinical supervision in practice
INTRODUCTION
In this chapter we will examine what coaching is and consider whether some of the core skills used in ‘coaching a client’ might also have some resonance with what clinical supervisors are trying to achieve in ‘supervising a supervisee’. Just as important as what is trying to be achieved in coaching or clinical supervision are the roles of the ‘client’ and ‘supervisee’ in the two processes and the nature of the relationship itself. Much of the thinking behind this chapter is borne out of (the first author) John’s continuing developmental journey towards becoming an ‘accredited coach’ and being a recipient of the coaching process. Part of the agreement made with Rachel (John’s coach) has been for him to personally experience coaching by utilizing it as a form of clinical supervision. This has enabled him, with the help of Gerard (the second author), to reflect on the potential of coaching practices in clinical supervision situations, while acting as a clinical supervisor in selected UK healthcare settings.
In over a decade of the emergence of clinical supervision in UK healthcare there is some general agreement that the term ‘supervision’ is not an accurate description of the intentions behind the process and this, in John’s view, continues to act as a barrier in getting started in practice. The development of coaching is an unexplored frontier for clinical supervision and its application to the healthcare practice environment.
At the risk of ‘muddying the water’ (a response a respected academic colleague of John’s made to the notion of introducing elements of coaching into clinical supervision) we suggest that coaching, in particular development coaching, has much to offer the clinical supervision encounter, particularly for senior staff supervisees (in terms of conversational structure, being more demonstrable in terms of outcomes, less ‘problem’ orientated and being a more equal relationship).
For health professionals the term ‘development coaching’ might more accurately be applied to senior and experienced healthcare staff, reserving the term clinical ‘supervision’ for more individualized and performance related activities with more junior staff. If this premise is accepted, the implications are enormous in healthcare in terms of developing coaches as well as supervisors and rethinking what already happens in clinical supervision. On the other hand, existing professional coaches, who undergo long training programmes to become accredited, might feel their role is being usurped by healthcare supervisors.
Our view is that both coaching and nursing as professions have an established history of ‘borrowing’ knowledge from other related disciplines to generally inform their practices, and that the knowledge base of professional coaching, with its emphasis on developing potential and enhancing work performance, has much to offer the development of clinical supervision activities.
Although the chapter is not a broad examination of coaching as a profession per se, it seems sensible to question what happens in ‘coaching’ and analyse the different interventions that might be suitable for use in the clinical supervision encounter. Different types of coaching and a popular coaching framework are outlined, in order to help make some tentative comparisons between the skills used in coaching and clinical supervision. For those of you already engaged in the process of clinical supervision (as a supervisor, supervisee, or supporting the initiative as a healthcare manager) we offer a challenge: consider experimenting with a coaching framework as a potential structure for one of your clinical supervision sessions.
THE LANDSCAPE OF PROFESSIONAL COACHING AS A CLINICAL SUPERVISION CONTINUUM
When one thinks of the term ‘coaching’, competitive sports and winning are brought to mind (Kinlaw 1997:21, Peltier 2001:170, Starr 2003:5). For instance, how many times do you recall successful sportsmen and women, when they are interviewed shortly after an achievement, making direct references to their coaches as being instrumental to their success? Kelly Holmes, the UK double gold medallist in sprinting, was a perfect example (I am writing this during the 2004 Olympics in Athens).
A coaching model often used in competitive sports is the ‘coach’ as ‘expert’ or ‘personal trainer’. For example, in golf this might be helping a player towards winning a major tournament or simply remedying aspects of a player’s game (such as altering the grip used or perfecting the swing of the club). In the UK, as elsewhere in the world, successful sports team coaches are able to capture a nation’s imagination and can even reach legendary status — the late Sir Alf Ramsey (England football World Cup winning coach in 1966) and Sir Clive Woodward (England rugby World Cup winning coach in 2003) to name only two. The reason for this acclaim is simple — successful results.
Effective coaching is not confined to competitive sports; it is evident in other areas that demand high performances. For instance, individualized coaching can enhance the performance of an opera singer and maximize the potential of musicians and others in the performing arts. You can probably think of many other examples in which coaching is cited as improving the abilities or the performance of individuals. Coaching a team, or an individual, to maximize their potential is likely to be based on some of the following attributes of the coach:
 An expert (or having a significant area of expertise).
An expert (or having a significant area of expertise).
A close observer who offers ‘live’ feedback on technique(s).
A motivator towards winning ways.
A setter of ever-increasing levels of performance and endurance.
A person who is willing to be unpopular when necessary.
A person who develops a sense of self-belief at ‘being the best’ or striving toward ‘the best they can be’.
A person who gives time and commitment and expects the same from those being coached.
If as a starting point we agree in principle that coaching (and in particular competitive coaching) is concerned with nurturing potential, maximizing individual or team performance and, most importantly, getting results, it is not surprising that coaching techniques and processes have been applied to the business and industrial sectors. However, Kinlaw (1997:21) points out that a major difference between personal and professional development coaching and sports coaching is that competitive performances often last for a set given period and players only need to be at their best for a defined time span. In contrast, the work of businesses continues unceasingly (unless discontinued) with the consequence that employees are expected to be ‘doing their best all of the time’ and professional coaching in this situation is a much more complex activity to define.
Although professional coaching might be a new term for many of you, the idea of having a periodic one-to-one conversation with someone (usually a manager) at work about development needs has been around for decades. Jarvis (2004:8) asserts that such conversations are largely based on ‘knowing what you need to change’ and this is very different from actually helping to bring about those changes in a person’s lifestyle or work habits (which is the remit of professional coaching). The rapid expansion of professional coaching is due to a number of changes in the work environment (Box 6.1).
BOX 6.1 Key factors leading to the expansion of professional coaching in the workplace
Keeping pace and learning to adapt to increasing amounts of change
Flatter organizational structures and broader management roles requiring individualized support
Learning being considered lifelong and needing to take account of individual learning styles
Targeted and responsive approaches to individual development
The cost of poor performers to the organization
Formalized support for those at the top who are often isolated or a significant distance from employees
Employees having to take individual responsibility as they can no longer rely on employers to provide all their career development
The cost-effectiveness of work-based learning schemes as opposed to just the training room of an educational provider
Adapted from Jarvis (2004:6)
This has in turn led to the surfacing of different areas of coaching expertise, such as personal life coaching, executive coaching and corporate coaching to name but a few. More detailed accounts of the different types of coaching can be found in Hadikin (2004:15), Jarvis (2004:24) and Jay (2001). Interestingly, the term ‘clinical supervision’ was cited in the early 1980s as a method of coaching teachers for higher performance and transforming the work culture in North American schools (Anderson & Snyder 1993:32). Despite such diversity, all professional coaching maintains that the development of relationships between people and the conversations that take place will have different emphases, depending on the context and the needs of the people being coached.
Downey’s (1999:15) broad definition of coaching might also be a definition of individualized clinical supervision in practice:
Coaching (clinical supervision) is the art of facilitating the performance, learning and development of another.
West and Milan (2001) identify three specific types of coaching for leadership which help to further illustrate the different emphases in the coaching relationship:
Skills coaching relates to developing specific skills and abilities in the client for which the coaching parameters and expected outcomes are clearly defined from the beginning, e.g. improving presentation skills at meetings or delivering a conference paper. The relationship may involve directly instructing the client or offering advice and in essence ‘training’ the client. What distinguishes skills coaching from training is that it is delivered on a one-to-one basis rather than in a large group situation. Skills coaching is a highly individualized and intensive relationship, focusing on the specific learning needs of the client, and is usually short term.
(Although similar to mentoring, skills coaching is different; a mentor either implicitly or explicitly assesses a person’s individual level of skill against organizational or professional competencies. A mentor relationship typically involves an experienced senior staff member and a junior staff member. The senior staff member is recruited from within the organization and is expected to directly influence the way the more junior member of staff works; in other words, this is an apprentice–master relationship.)
Performance coaching is wider in scope than skills coaching and intends to enhance a client’s general performance in their role at work (by helping the development of particular behaviours or by raising their awareness of behaviours that limit performance). In this respect there is an expectation that coaching will produce results in a client’s performance. More often than not the client’s role and expected behaviours are defined by the organization as performance objectives or job descriptors. When these objectives are not met, or the client is underperforming, referral for either internal (manager as coach) or external coaching may be necessary.
Thorpe and Clifford (2003:34) not only emphasize the improvement of skills and performance as expected coaching outcomes for the client but also introduce the concept of reflective learning as an important aspect of the process. They define coaching as:
… the process of helping someone enhance or improve their performance through reflection on how they apply a specific skill and/or knowledge.
Their definition, aimed specifically at the coaching role of a trainer and manager in the workplace, states that the process of coaching facilitates reflection on established sets of competencies or preferred behaviours.
It is interesting to note that the objectives in both skills and performance coaching are clearly defined in the shorter term (over one year) in which results or outcomes can be followed up by the organization in the form of an annual appraisal or personal development review.
Development coaching is usually considered a longer-term investment on the parts of both the organization and the individual, for instance 12 to 18 months (but can last longer), and is a more evolving process than the specific task of skills or performance coaching. (Clinical supervision and development coaching are offered to senior or qualified practitioners and are highly individualized.)
The process begins by initially identifying the agenda and development goals, but more often than not the agenda alters depending on the changing circumstances and complexities of the client’s or supervisee’s world (West & Milan 2001:10). For instance, in John’s development coaching, in which his agenda was to discuss the progress of a large clinical supervision project in prison healthcare, the session changed into ways of valuing what he did and putting a price on services that he offered. In turn this led to a complete re-think on managing his business finances which subconsciously he had been having concerns about.
Timothy Gallwey, a former tennis coach and a major influence on the origins of developmental coaching, based his Inner Game thesis (Gallwey 2000) on the realization that a person’s peak performance is often marred by their own ‘self-interference’. For example, the self-doubt and fear of failure that interferes with appreciating an individual’s potential, let alone peak performance, is not able to be reached.
 Based on Gallwey’s (2000) Inner Game thesis, how many work colleagues can you think of who are generally more capable than their current performance suggests and in what ways might ‘self-interference’ manifest itself?
Based on Gallwey’s (2000) Inner Game thesis, how many work colleagues can you think of who are generally more capable than their current performance suggests and in what ways might ‘self-interference’ manifest itself?
Can you think of either a personal or professional example of how ‘self-interference’ might be a factor in reducing your own potential or performance?
Gallwey (2000:177) suggests that unlocking a client’s potential is not so much a process of adding by the development coach (e.g. new skills or behaviours) but subtracting, or having the client unlearn, whatever is getting in the way of the client reaching that potential. In this respect, the task of the development coach is about facilitating the client’s learning or, to be more precise, enabling the client to ‘un-learn’. Somers (2002:6) refers to this as ‘drawing the client out’ rather than ‘putting in’ and helping to draw on the huge reserves of talent and potential laying dormant in the client.
A key element of development coaching places the client as the main problem solver through gaining an increased sense of self-awareness during reflection on their personal or professional performance and would seem to have distinct parallels to a reflective approach in clinical supervision (previously discussed in Chapter 2).
All three types of coaching outlined (skills, performance or development) present two basic coaching models that can be broadly categorized as either being directive in nature (‘showing and telling’) or non-directive (the client retains more control in the learning process). Whatever type of coaching is used, all coaching remains outcomes-orientated or performance-focused and is a highly individualized and person-centred endeavour. The two extremes of directive or non-directive coaching activities can be seen as being on a coaching continuum depending on the client’s experience and needs and has many similarities with the supervision continuum that already exists in UK healthcare. An adapted coaching/supervision continuum is outlined in Box 6.2 based on the original work of West and Milan (2001:3).
BOX 6.2 An adapted continuum of coaching (Milan & West 2001:3) and its relationship to clinical supervision in UK healthcare (in italics)

 Consider the coaching continuum and the different types of coaching with the healthcare supervision continuum in Box 6.2.
Consider the coaching continuum and the different types of coaching with the healthcare supervision continuum in Box 6.2.
In reality there is likely to be some overlap between the three types of coaching or supervision in practice. Most healthcare professionals have undergone lengthy training in which the work of the unqualified practitioner is duly assessed and supervised by a range of more senior qualified practitioners, mentors or trainers. But once qualified, immediate additional skills are then required by a practitioner in making the transition from unqualified to qualified professional. Clinical supervision for the newly qualified junior healthcare professional will initially need to be advisory and directive (e.g. mentoring and preceptoring), focusing on the specific skills of practice. As healthcare practitioners become more experienced and assume more senior roles, they will move towards the right of the coaching-supervision continuum. At this end of the continuum, roles at work become more complex or ambiguous, requiring the less directive skills of development coaching or developmental supervision.
Perhaps junior staff may be considered to be under clinical supervision when they are specifically learning skills and/or working to a minimum performance, whereas more senior practitioners may be considered to be either under developmental supervision or receiving development coaching when they are engaged in continuing professional development (CPD), at which time they will require less direction and more guided reflection.
This gives rise to the question: In what ways might directive or non-directive supervision be a help or a hindrance in clinical practice?
 John’s personal reflections from his own coaching/supervision with Rachel:
John’s personal reflections from his own coaching/supervision with Rachel:
In reality, I would suggest that we all probably have a tendency towards being either directive or less directive depending on our client’s or supervisee’s needs, which are complex. In my past professional situations, having been a senior practitioner in intensive care and a teacher in a university, I have often been looked upon as an ‘expert’ with the expectation that I be directive and guide. (In some cases, being directive to others has been life-saving in the clinical situation.)
In contrast, now working as a full-time externally employed change agent and as a freelance consultant, I intend my role to be much less of an ‘expert’ and directive and more facilitative in nature. As this has not come naturally for me, I am currently ‘un’ learning this in my own coaching/supervision. I have become much more consciously aware of my old tendencies towards retaining a degree of power and control through having some specific knowledge. My client’s expectations are actively wanting me to remain as ‘expert’, provide answers and at the same time pay me for doing so. The contradiction is that I view my ‘expert-ness’ at its worst as being potentially counter-productive in fostering a sense of dependency on my services and one which will not be sustained after my contract expires, and at best, not really being facilitative at all. In other words, my being less directive will increase the ownership and subsequent autonomy to act of those that employ my services.
COMPARING CORE DEVELOPMENT COACHING SKILLS TO CLINICAL SUPERVISION
The International Coach Federation (ICF) is a professional organization for coaches based in the USA. Although not an officially recognized regulatory body it does offer some minimum standards and ethical guidelines for coaches and accredits the quality of coaching training programmes. The ICF (2006a) describes the ‘what’ and ‘how’ of professional coaching as follows:
Professional Coaching is an ongoing professional relationship that helps people produce extraordinary results in their lives, careers, businesses or organizations. Through the process of coaching, clients deepen their learning, improve their performance, and enhance their quality of life.
This definition explains what is expected of a coach and is helpful in reflecting on aspects of development coaching that might be useful in the clinical supervision situation. The ICF’s notions of professional partnership, goal setting, getting results and relevancy in the one-to-one or group situation aligns with the principles and ideas underpinning clinical supervision.
As part of the standardization of a professional coach’s work the ICF (2006b) identifies four key clusters and 11 associated core competencies that are individually examined before a coach can become an accredited member or professional coach (Box 6.3).
Another body, the European Coaching Institute (along with other organizations), promotes an industry standard for coaching practices for both individual coaches and training providers (ECI 2006a). There are also published professional Codes of Ethics (EMCC 2004a, ICF 2006a) and Guidelines on Supervision for coaches (Association for Coaching 2005, EMCC 2004b) which demonstrate the effort to continually improve the coaching industry and protect clients.
 Taking each of the descriptors of the 11 core competencies of coaching in Box 6.3:
Taking each of the descriptors of the 11 core competencies of coaching in Box 6.3:
a) Individually rate what you consider to be the appropriateness (or not) of each core competence for use in your clinical supervision situation, i.e. Very Important, Important, Not Important. What is the rationale for the choices you made?
b) For those competencies you rated as Very Important or Important, download the behavioural descriptors from the ICF website and personally rate your current coaching abilities in clinical supervision. What might be the implications for you with this exercise?
c) How useful might each of the 11 core competencies of coaching be in helping to set minimum clinical supervisor behaviours?
The four clusters may offer a useful content for any clinical supervisor training programme and the 11 core competencies a useful discussion point for the future evaluation and perhaps even regulation of clinical supervisor skills. Major difficulties facing existing clinical supervisors in UK healthcare practice is that there is an absence of literature on the subject and virtually no agreement on what the core competencies of a clinical supervisor are in practice. Training courses vary in length and content and in many cases, having undergone a course, clinical supervisors are not required to update or review their knowledge and skills whatever these might be. The current lack of regulation and minimum standards in healthcare clinical supervision therefore leaves the ‘doing’ of effective clinical supervision to individual interpretation and preference. While it might be argued that adopting a less prescriptive stance for clinical supervision is its strength, there remain unanswered ethical questions about the effects of this on supervisees and what is happening within clinical supervision in organizations.
Using the four clusters of coaching as headings, a number of differences emerge when comparing coaching to clinical supervision (Table 6.1).
TABLE 6.1
Some key differences between coaching and clinical supervision using the four key clusters of a coach’s competence (ICF 2006b)
| Coaching | Clinical Supervision | |
| Setting the foundation |
Incremental levels of coach training based on experiential learning and being coached Mutual contractual agreement made following detailed first interview matching methods and expertise Coaches expected to have ongoing supervision as a requirement of their Ethical Code (EMCC 2004) Coaching working towards becoming regulated that will include supervision as a professional requirement Coaching as an emerging profession in its own right Always an emphasis on client solutions and results for the immediate future |
Often short and variable introductory training given in-house Mutual contractual agreement made based on practitioner experience and expectations Supervisors expected to have ongoing supervision as best practice No regulation of clinical supervisors although clinical practice regulated as a professional activity Supervision viewed as an additional part of a qualified practitioner’s role Often an emphasis on ‘problems’ and ‘problem-solving’ occurring in practice |
| Co-creating the relationship | ||
| Communicating effectively | ||
| Facilitating learning and results |
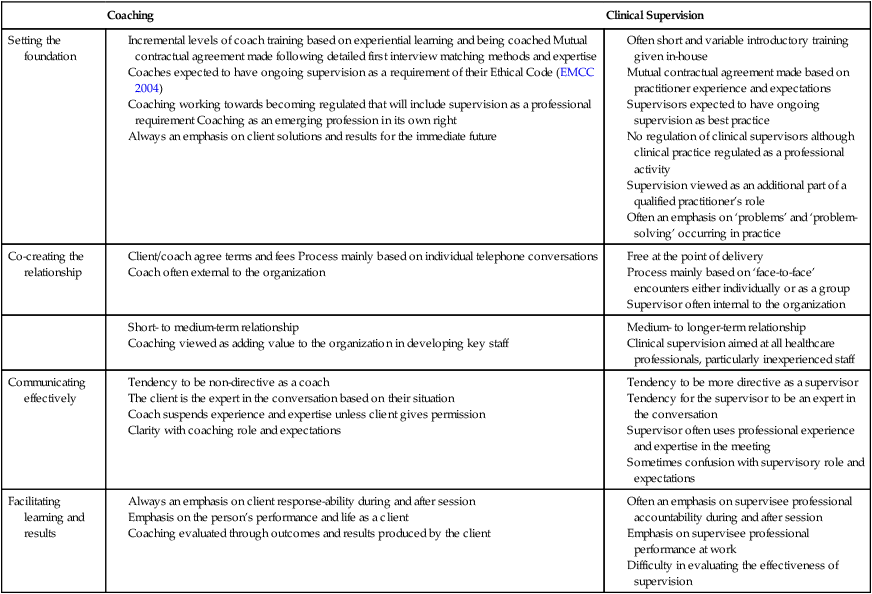
A major difference is that clinical supervision is seen as an additional part of a practitioner’s role following some introductory training but the newly adopted role (if it is adopted) does not relieve the practitioner of existing clinical responsibilities and often no additional time is built in for the activity. In contrast, most coaches have undergone lengthy periods of experiential training to become accredited before practising as a paid professional. While coaching is viewed as adding value to the organization through the individualized development of staff, clinical supervision, which has a similar philosophy, is often viewed as an inconvenience in busy practice.
Both the coaching and clinical supervision literature distance themselves from being any form of therapy, preferring instead to concentrate on the client’s or supervisee’s ‘present’ practices. As O’Donovan & Martin (2000:13) assert:
Unlike therapies, coaching focuses on where you are now and where you want to get to, and the only place you can start from is where you are now.
While professional coaching has an established knowledge base derived from counselling, management consulting and psychology (Hadikin 2004, Peltier 2001, Starr 2003, West & Milan 2001), clinical supervision is only just beginning to explore different psychological frameworks as being relevant for clinical supervisors (discussed in an earlier chapter). This might explain why clinical supervision still largely remains a ‘problem’-orientated intervention — not dissimilar to a medical model in which patient problems (practice problems) are identified in order to help diagnose a condition (why such problems are occurring), before a treatment plan is prescribed (action plan to solve the problem — and if not followed through, creates even more problems).
By contrast (in not adopting a negative fault-finding approach), professional coaching is a focused activity that adopts a more appreciative or positive approach concentrating on creating solutions and results with the client. Embracing a similar approach in the clinical supervision encounter could be transformational by creating deeper self-awareness in supervisees about their practice and focusing on improvement and change as an outcome. In turn, this will make the process more transparent and evaluating the effectiveness of clinical supervision less challenging, which is the subject of a later chapter.
While it is not our suggestion that coaching replaces clinical supervision, some key elements of development coaching can quite easily be adapted for use in the clinical supervision situation, particularly with more senior healthcare practitioners (Driscoll & Cooper 2005). However, this will mean re-negotiating the original clinical supervision intentions and expectations with the supervisee. Despite these obvious differences, coaching in my view shares more similarities than differences with clinical supervision:
The terms coaching and supervision can evoke initial suspicion in the client/supervisee that they are suspected of underperforming.
Client/supervisee can exercise choice in who is their coach/supervisor.
Formal contract/agreement is made at the beginning of the process.
Expectation that the client/supervisee is in control of the process.
Senior managers can be coaches/supervisors.
Both processes are examples of formalized reflection geared to developing personal practice and improving performance.
Sessions begin with present practice and are directed towards future actions.
Reflective questioning and active listening are key tools used by the coach/supervisor.
Both processes offer feedback to the client/supervisee.
Coaches/supervisors are expected to have on going supervision as part of their continuing professional development (CPD).
Both processes are intended to contribute to the personal and professional growth of the client/supervisee.
Coaching is an eclectic discipline and draws on many sources of knowledge, including research findings and discussions in psychological literature. Using this experience from the world of coaching, some key areas could be further developed in clinical supervision training:
placing more emphasis on the use of powerful questions,
designing actions with the supervisee during the session, and
a willingness to embrace a more holistic approach that takes account of the personal as well as the professional life of the person.
It is interesting to contrast the commitment of the supervisee and the supervisor in clinical supervision, which is ‘given freely’ in the NHS, to the commitment of the client who pays for individual sessions or is sponsored by their organization to engage in coaching to maximize their performance at work. Finally, all coaching and clinical supervision is concerned with the personal or professional growth of the person and a powerful metaphor comes to mind that explains the complex nature of both coaching and clinical supervision’s part in this growth — The Rose (cited by Wright 1998:186).

EXPERIMENTING WITH A COACHING FRAMEWORK IN THE CLINICAL SUPERVISION SITUATION
Clinical supervision, like coaching, relies on the sessions being productive for the supervisee. One way of achieving this is to use a framework or structure to help you navigate your way through a session as a clinical supervisor. Within the coaching literature there are many frameworks to choose from but the most widely used is the GROW model (West & Milan 2001:19). Originally developed by Graham Alexander in 1984 it was published by Sir John Whitmore in his seminal coaching text Coaching for Performance (Whitmore 1992). The importance of growth (of the client) is a critical element of coaching highlighted by the following definitions:
… a simple yet effective form of personal development where the client and coach create an alliance that promotes and sustains the client’s personal growth and competence.
European Coaching Institute, 2006b
Coaching is about performing at your best through the individual and private assistance of someone who will challenge, stimulate and guide you to keep growing.
The framework John has been using on his coaching course and experimenting with in clinical supervision is the slightly adapted TGROW model (Downey 1999:29) diagrammatically represented in Figure 6.1. As part of the initial clinical supervision agreement a clinical supervisor is expected to control the structure and process of a meeting but it is the supervisee who controls the content or topic.

 If you are going to try out the TGROW framework in your next clinical supervision session you will need to seek permission to do so from your supervisor first!
If you are going to try out the TGROW framework in your next clinical supervision session you will need to seek permission to do so from your supervisor first!
The supervisee’s chosen topic for discussion in clinical supervision (while this is seemingly obvious) is critical to the overall outcome of the session. More often than not, the agenda set by the supervisee can have several layers that can be difficult to tease out even under questioning. Therefore, to make the sessions more effective the supervisee should be asked to carry out some written preparation beforehand. (Coaching is frequently carried out on a telephone and this is dealt with in more detail in the next chapter.)
It is often helpful for the supervisee to have begun to reflect on what is to be discussed and to have either emailed or faxed a preparation document to the clinical supervisor beforehand. (The format for this can be discussed when the initial agreement is being negotiated.) Such groundwork is useful in giving the clinical supervisor time to prepare for the session.
Some ideas for questions a clinical supervisor might pose (although not all need to be used; you can probably think of others) using a TGROW framework in a clinical supervision session are contained in Box 6.4.
BOX 6.4 Questions using the TGROW framework a clinical supervisor might pose to a supervisee to aid structure and focus a clinical supervision session
What is it you would like to discuss today?
What issue is uppermost in your mind from your preparation for the session?
What is happening to you at the moment?
How do know this to be accurate?
Can you give me a worked example over the last week when this happens?
What effect does this have on you?
What seems to be preventing you from making progress?
What support or resources might you be able to draw on with your situation?
Can you write down six things that you could do right now (however improbable) to improve your situation?
What resources do you have at your disposal to alter your situation?
What might be some of the benefits and burdens of each of your ideas?
Which idea would give you the most happiness in your situation?
What are the possibilities for your future actions (do not all need to be realistic at this stage)?
Who might be able to help you with this?
Would you like some suggestions from me (if client/supervisee stuck)?
Could you rate from 0 to 5 the practicalities of each of your suggestions?
What will your first step(s) be based on today’s session?
What might get in your way and how will you deal with this?
How are you going to remember what you have agreed to do by the time we next meet?
How will you get the support to move forward?
Would you be agreeable to email or telephone me about your progress before we next meet?
Obviously it is less intrusive to have questions in front of you when using the telephone than in the face-to-face encounter, but it is surprising how quickly TGROW can be used once you are familiar with its different elements.
As already mentioned, therapy is different from clinical supervision and coaching in that a goal to aim for is established before the client/supervisee’s actual realities are examined. But, the setting of a positive goal may have little meaning for a client/supervisee who is overwhelmed with the perceived negative realities of the present work situation and this can have an influence on the effectiveness of a session. Thus, in clinical supervision, a session is often ‘problem driven’ instead of being more positive and solution focused, as is the case in coaching. That is why clinical supervision can benefit from adopting the processes involved in coaching: goals that are formed by looking at the situation in the longer term and determining the steps needed to be taken to achieve these goal(s) are motivating and creative for the client/supervisee. In addition to this, setting goals provides not only focus but a way of being able to evaluate the effectiveness of the session based on goal outcomes.
However, keeping in mind the ease with which clinical supervision can fall into a ‘problem-driven’ session, to be able to successfully achieve client/supervisee goals it is important to do a reality check of the client/supervisee situation. This is a critical phase for the coach/supervisor to help the coach/supervisee assess the impact of those realities. Being a neutral or objective listener can help the client/supervisee reframe their situation or view it from a fresh perspective.
An often asked question is: Can someone from outside a professional discipline act as a clinical supervisor? John’s own experience is that it is much easier to be objective when you do not fully understand the supervisee’s realities or situation and this gives you a license as a supervisor to ask ‘silly questions’ that get right to the heart of the matter (Sood & Driscoll 2004).
Another important element of helping the client/supervisee with their realities as a coach/supervisor is to remain ‘in the present’ with the intention of enabling movement forward on the topic. Here using open-ended questions is useful. Sometimes questions can be purposely structured to move the client/supervisee back into ‘today’ with a view to ‘tomorrow’ rather than remaining stuck in ‘yesterday’! Although the ‘past’ might be useful to understand the context of a situation, coaching/clinical supervision is not therapy. And sometimes talking about the past can be an unconscious ploy to avoid facing present reality; the supervisor should remain aware of these pitfalls.
The options phase helps to develop a sense of personal ownership of the issue and encourage choice, once a path has been cleared through the jungle of the client/supervisee’s reality. If the previous phase has been rushed or inadequate time given for detailed questioning, it will reduce those choices and subsequent decision-making by the client/supervisee. Sometimes in exploring options it becomes obvious that more work needs to be done in the initial goal setting or gaining clarity about the client/supervisee’s reality. A key element of this stage is to develop a real sense of the client/supervisee’s ownership by facilitating as many choices or options as possible to move forward, rather than it being a phase in which the ‘right’ answer must be found. The more courses of action the client/supervisee generates, the more likely it is that they will be able to change their perspective of the situation and raise some positive energy, enabling progress to be made with their topic.
A critical success factor in clinical supervision and coaching is the development of a safe and confidential environment in which to explore ideas. The generation of options can be limited if the coach/supervisor pours cold water on ideas being produced because they have an in-depth knowledge of the client/supervisee’s situation (for example, working in the same environment). Therefore, it could be claimed that in contrast to a clinical supervisor, a neutral observer, such as a coach, offers the client/supervisee the big advantage of an unbiased perspective that allows the exploration of even the most unlikely of ideas.
The way forward is the final stage of the process that enables the client/supervisee to convert their images and discussions into decisive actions. This means that the client/supervisee makes final choices and decisions about how to progress. (At this point, a key responsibility, the coach/supervisor summarizes the session, which assists the client/supervisee to come to decisions. This is where it can be of benefit (with permission), for the coach/supervisor to have taken some notes.)
 Taking notes is more awkward in the face-to-face encounter, where in doing so you may stand accused of not actively listening! On a telephone it is much easier, provided you have a headset on which you can listen while you write.
Taking notes is more awkward in the face-to-face encounter, where in doing so you may stand accused of not actively listening! On a telephone it is much easier, provided you have a headset on which you can listen while you write.
The final phase is where the client/supervisee then needs to demonstrate a commitment to act or be response-able. The session ends with the client/supervisee agreeing the steps that will be taken, how these will be taken, and that they will be taken. Most coaches will have been taught (and both myself and Gerard have been on the receiving end of this) to nail down the client at the end of each session by asking the client/supervisee to rate three questions on a score of 1 (definitely not) to 10 (definitely will):
How strong is your intention to take that first step?
Experience suggests that scoring 7 or less on each of these is likely to mean that little or no action will be taken following the session. The language used by the client/supervisee in response to the questions is often just as important as the verbal score. Low intention words such as ‘perhaps’, ‘might’ and ‘if’ can be indicators of intending to act or not after the session.
While the TGROW framework is the most widely known and used in coaching, there are other models that you might wish to explore as an alternative framework for clinical supervision (Dembkowski & Eldridge 2003, Leibling & Prior 2003, Libri 2004, Mackintosh 2003, Martin 2001, Somers 2002). Rushing the stages (because of the lack of time or the inexperience in its use) limits the effectiveness of the TGROW framework. For instance, this may lead to skipping through the stages, and not having a full understanding of the goal(s) representing the gap between the present situation and the desired outcomes or, when generating options, only highlighting a few ‘tried and tested’ choices. Despite such limitations, in my experience TGROW does provide an excellent structure for those new to coaching but more importantly, it is enormously helpful in clinical supervision.
COACHING POSSIBILITIES IN UK HEALTHCARE BEYOND CLINICAL SUPERVISION
According to The Coaching Study (Arnott & Sparrow 2004) involving over 100 UK organizations (including eight NHS organizations), a significant increase in the use of externally facilitated coaching is predicted in the near future. At present the majority of professional coaching is provided at executive/management levels and concerned with supporting both personal and professional development to improve organizational performance. With the emphasis on ensuring that staff continuing professional development needs are met in clinical governance (McSherry & Pearce 2002, Swage 2003), the potential for coaching still remains relatively unexplored as a tool for developing health professionals’ practice.
Although coaching might be viewed as a tool for empowering individuals (Hughes 2003), great coaches know that individuals already have innate power and potential so therefore a coach’s task is to facilitate expression of it (Downey 1999:13). While this chapter has concentrated on the use of coaching as a method for clinical supervision, Hadikin (2004) outlines a powerful case for developing a whole coaching culture in the NHS with a broader application to healthcare and in particular to patients:
… as we move as a society from a sickness/cure model towards a health/prevention model, we should look towards a profession which facilitates growth and change rather than a therapeutic model to ‘cure’ our ‘illness’. Hadikin, 2004:24
Hughes (2003) suggests that coaching, where the client (or the supervisee) is promoted or empowered to see themselves as being an expert in their own situation, can be applied with patients. Current government initiatives are doing just that, promoting the patient as an expert in their own experience of illness (Department of Health 2001). Imagine the vast resources that might be saved if healthcare staff were able to coach patients with chronic conditions to take more control over their lives rather than be dependent on a healthcare system that would seem to favour acute illness. Some evidence is already emerging that coaching can have a favourable effect on patient outcomes (Boyle 2004, Brook et al 2003, Horowitz et al 2002, Hughes 2003, Ream et al 2002, Vale et al 2003, Whittemore et al 2001, Whyte 1997). While a coaching potential for developing healthcare staff in clinical supervision is a distinct possibility, an even greater potential for developing a coaching culture generally in UK healthcare could emerge. Perhaps development coaching might even become the new clinical supervision.
CONCLUSION
The historical development of sporting coaching techniques and psychological processes has moved rapidly from the playing field to transforming the performances of individuals and organizations in corporate business. The professional coaching knowledge that coaches use is only now beginning to be realized in healthcare and, like clinical supervision was, and perhaps still is, is poorly understood.
While I am not advocating development coaching as a replacement for clinical supervision or all clinical supervision to become development coaching, there would seem to be an enormous potential for the principles of professional coaching in clinical supervision as well as in the healthcare setting generally. The processes of both clinical supervision and development coaching seem to support the personal and professional growth of the ‘client’ or ‘supervisee’. The way that this is achieved is through regular reflective but action-orientated conversations intended to increase future performance as a person and a practitioner. Unlike clinical supervision, which undoubtedly has supervisee outcomes, development coaching is more transparent while remaining confidential. It is less ‘problem’ orientated than clinical supervision and has at its core demonstrable results following a structured conversation that increase professional performance, making a positive contribution to the client’s personal wellbeing. The key is that all parties develop an understanding about the intentions and expectations beforehand or when periodically re-negotiating the coaching or clinical supervision agreement or contract.
For those reading this chapter as professional coaches we extend an invitation and point out the potential ‘alliance’ that could exist between healthcare and coaching. Perhaps some of the lessons and expertise of developing clinical supervision in UK healthcare over the last decade might offer the emerging profession of coaching a way forward that requires practising coaches to also engage in ‘regular’ supervision as part of their continuing professional development (CPD) (or might this be development coaching?).
On reflection … chapter summary
Professional coaching remains an unexplored frontier for the continued development of clinical supervision in healthcare
The term ‘development coaching’ might be a more accurate description of clinical supervision for more senior healthcare practitioners
Unlike for professional coaching there is an absence of literature and virtually no agreement on what the core competencies of a clinical supervisor are
Both clinical supervision and professional coaching have as their cores the facilitation of a reflective conversation with another person to enhance their personal and professional growth
Professional coaching frameworks are less ‘problem’ orientated and can offer structure for achieving demonstrable outcomes in clinical supervision
SELECTED COACHING WEBSITE/RESOURCES
http://www.academyofexecutivecoaching.co.uk
http://www.associationforcoaching.com
http://www.coachfederation.org/
http://www.supervisionandcoaching.com
http://www.coachingnetwork.org.uk
http://www.lifecoaching-company.co.uk
http://www.noble-manhattan.com