Placing communication at the centre of person-centred care
Jane Stein-Parbury
Active listening, p. 226
Authoritative interventions, p. 226
Collaboration with colleagues, p. 217
Communication, p. 210
Emotional intelligence, p. 232
Empathy, p. 228
Facilitative interventions, p. 226
Healthcare environments, p. 213
Interpersonal communication, p. 221
Intrapersonal communication, p. 221
Knowing the patient, p. 212
Mental models, p. 218
Non-verbal communication, p. 222
Paraphrasing, p. 229
Patient-centred communication, p. 213
Presence, p. 227
Self-disclosure, p. 231
Sympathy, p. 228
Team collaboration, p. 217
Therapeutic communication techniques, p. 225
Verbal communication, p. 221
Communication and person-centred nursing practice
Interpersonal communication involves the capacity to convey thoughts, feelings and attitudes through spoken, written and non-verbal means in order to exchange ideas and construct human meaning. Most professional people are required to be effective communicators in the conduct of their work, and the nursing profession is no different. However, the content and process of communication varies across professions according to the particulars of context. For example, professional engineers are often required to communicate effectively through technical report writing; computer programmers are required to communicate through symbolic languages unique to the computing world; and salespeople must acquire skills of persuasion in order to be successful.
While the skills of effective communication may be similar to those in other professions, the knowledge and attitudes required for therapeutic intentions are particular to the nursing context. For example, a nurse encouraging a depressed client to engage in physical exercise may use persuasive communication techniques that are similar to those of a salesperson. However, the intention of encouraging a depressed client to be active is based on knowledge that physical movement affects mood; that is, persuasion is used for the purpose of helping the client. Person-centred care means that communication is always ‘for’ the client; the nurse is morally positioned to communicate in a manner that serves the client’s best interest. Clients perceive that good communication with nurses is centred on their needs and concerns (McCabe 2004). Therefore, effective communication is a core element in person-centred care (Kitson et al 2013).
This chapter presents the basic aspects of effective and therapeutic communication within the context of person-centred nursing practice. The qualities, behaviours and communication techniques described characterise professionalism in therapeutic relationships with clients and collaborative relationships with colleagues. Although the terms ‘client’ and ‘patient’ are often used interchangeably, the same principles can be applied when communicating with any person in any nursing context.
The context of nursing practice
Some aspects of communication stand out as more relevant than others; it is therefore important to consider the particular aspects of effective professional communication within the context of nursing practice. In the particular context of nursing, effective interpersonal communication is required for the exchange of health-related information, the promotion of therapeutic relationships with clients and the development of collaborative relationships with other healthcare professionals. Nurses must be competent in the use of effective interpersonal communication skills and knowledgeable about healthcare matters, while simultaneously assuming an attitude of being ‘for’ the client. Focusing attention on the client is central to communication in nursing practice (O’Hagan et al 2014).
The competent nurse is able to therapeutically adjust and accommodate the use of effective communication skills in response to specific clinical contexts. Context helps to shape client needs. For example, a client who is undergoing diagnostic tests for possible cancer does not need detailed information about managing the possible side effects of radiotherapy (as might a client about to undergo radiotherapy). Such information might increase client anxiety during the diagnostic phase of an illness.
In addition to influencing the content of communication, context also affects the processes of communication. For example, intensive-care nurses rely on non-verbal communication from their patients when interacting with patients who are rendered speechless by mechanical ventilation, and community nurses spend much time enabling client self-care through health education communication. Consideration of context requires critical thinking about what is of benefit in meeting client needs, and such thinking is based on the nurse’s understanding of the therapeutic value of communication.
Why nurses need to communicate
A public expectation that nurses are effective communicators is embedded into standards for practice for nurses (Nursing and Midwifery Board of Australia (NMBA) 2006, Nursing Council of New Zealand (NCNZ) 2007, see also Chapters 10 and 11), and professional codes of ethics and conduct (Australian Nursing and Midwifery Council (ANMC) 2008a, 2008b, Nursing Council of New Zealand 2009, see also Chapter 9). Standards for practice include the nurse’s ability to collect relevant information from clients about their functional health status, and effective communication is required to elicit such data during client interactions. Standards for practice also require a professional nurse to provide relevant healthcare information to clients and their families in an effort to facilitate their understanding of health events and encourage their active participation in healthcare decisions. Effective communication is essential to the provision of such information. Enabling therapeutic relationships with clients through communication is one way that nurses demonstrate expected public standards of professional competency and conduct. The reason that communication is built into standards for practice and codes of conduct in nursing is that effective communication promotes client health and wellbeing (Fleischer et al 2009).
Dynamics of interpersonal communication
Interpersonal communication operates at two levels: content and process. The content level encompasses what is being discussed; that is, the subject matter. For example, when interviewing a client for the first time the content will most likely involve a history of the client’s health status and immediate care needs. The content level of communication is easily identified. The second level, that of process, is more subtle. This level involves how something is communicated rather than what is being communicated. For example, if the nurse conducting an initial interview with a client does so in a cold, clinical manner by simply asking a series of questions that follow a pre-set format, the client may not perceive the nurse to be genuinely concerned and caring. In this way the process level reveals the nature of the relationship between nurse and client. Content and process go hand in hand. For example, if the nurse is warm and open, demonstrating genuine interest in the client (process level), then clients are likely to be willingly forthcoming with information about their health status and concerns (content level).
Interpersonal communication is effective when meanings are shared between people. Messages that are sent are received with understanding when the person receiving the message understands the intent of the sender. However, interpersonal communication is not quite this straightforward. The intention of the sender of a message may not be easily understood by the receiver; and the receiver also has intentions that might not be clear to the sender. There are numerous aspects to consider in being an effective communicator.
Effective communicators are those people who can assert their own ideas while being able to respond with understanding to other people’s ideas. That is, skilled communicators are able to blend and balance two basic types of communication techniques: responsive and assertive. Responsive techniques facilitate mutual understanding between people; that is, from the same point of view. For example, a nurse who expresses empathy towards the suffering of a client is being responsive. Responsive techniques operate from an empathic understanding of a health event from the client’s perspective. In contrast, assertive techniques offer new insights and information from the nurse’s knowledge and professional perspective, for example, health teaching and education. Assertive techniques promote understanding of differing points of view.
Skills in being both responsive and assertive are what constitute effective communication in nursing practice (Figure 12-1). Nurses who are skilled at being assertive yet are not responsive are at risk of being too domineering, and may not take into consideration the feelings and personal perspectives of clients. Such nurses may expect clients to simply ‘do as they are told’. Nurses who are skilled at being responsive yet are not assertive are at risk of becoming overly accommodating, and may not challenge a client’s faulty thinking or misinformation. Moreover, assertive skills are required when collaborating with other healthcare professionals, as nurses present their views of client care from a nursing perspective. Nurses who are skilled in assertive communication techniques are more likely to advocate for clients and peers who are vulnerable, afraid or experiencing a threat to their human rights (MacDonald 2007).

Generally speaking, assertive skills are often used when advocating for clients while responsive skills are employed for the purpose of building relationships with patients and their families, which are based on the nurse’s understanding of their needs, concerns and desires. Developing such understanding is the heart of person-centred care. In recent reviews of the concept of patient-centred care, communication is consistently identified as a key element (Constand et al 2014, Kitson et al 2013, Sidani & Fox 2014). This is because person-centred care is based on collaboration between clients and healthcare professionals in which clients are active participants in their care. Therefore, nurses must use communication and relationship-building skills in order to understand what clients desire in order to respond to their needs ‘as they perceive them to be’.
Knowing the patient
Through communication the nurse comes to know the patient/client, not only as a patient or client, but also as a person with a unique perspective and life history. Termed ‘knowing the patient’, this concept entails understanding what the health situation means to the client (Zolnierek 2014). By understanding the situation from the client’s point of view, nurses are able to not only individualise care but also create a relationship based on empathic understanding (Bundgaard et al 2012, Mantzorou & Mastrogiannis 2011). Knowing the patient as a person is a critical aspect of safety and quality in nursing practice; more importantly, it is the essence of person-centred care.
Liaschenko and Fisher (1999) offer a useful schema to understand the meaning of knowing the patient. They describe three types of knowledge that nurses use in the conduct of their work. The first is termed case knowledge, and encompasses objective facts such as anatomy and physiology, disease processes and pharmacokinetics. The next is patient knowledge, which includes understanding how a client is responding to a particular health event, for example, side effects of medications and the experience of pain. The third type is person knowledge, which includes an intimate understanding of the person’s life history, their values and belief systems and their familial connections. Patient knowledge includes both physiological as well as emotional responses, which can be observed; however, person knowledge requires communication with the client. Figure 12.2 illustrates that the three types of knowledge intersect; it is in the intersecting spaces that nurses work. They use all three types of knowledge in a holistic manner.

According to this schema, the concept of ‘knowing the patient’ is encapsulated in patient and person knowledge. The degree to which a nurse comes to ‘know the patient’ varies with context. For example, in a study conducted in an outpatient endoscopy clinic, the nurse identified ‘knowing the patient’ in a practical sense, for example, their immediate concerns about the procedure they were about to undergo (Bundgaard et al 2012). In an emergency situation, it is unlikely that person knowledge will be of critical relevance (unless making a decision to cease treatment).
Patient-centred communication
Current efforts in healthcare systems reform are aimed at making communication, and care itself, more patient-centred (Newell & Jordan 2015, van Dulmen 2011). Being patient-centred means that the needs and expectations of patients are placed at the heart of communication and, more importantly, their voice in decision-making about their care is heard and heeded. Patient-centred communication contrasts with what has been a more traditional style focused on biomedical matters such as signs and symptoms. In nursing practice, being patient-centred contrasts with being task-focused. There is evidence to suggest that patient-centred communication increases not only patient satisfaction but also adherence to treatment and general improved health (Charlton et al 2008, Newell & Jordan 2015); the reason is that patients become more active participants in their own care.
While it may seem obvious that patient-focused communication should be standard, studies have demonstrated that communication often does not take into account what patients want and how they feel (Bolster & Manias 2010, Nordehn et al 2006). What is important to realise is that patients have varying desires to participate in care; some want to follow orders and ‘toe the line’, while others want to make decisions for themselves (Tobiano et al 2015). Patient-focused communication establishes the degree to which the patient desires to participate and their preferences for treatment.
Using a patient-focused approach to communication not only results in understanding how patients want to participate in care, but also includes understanding their nursing care needs, such as sleep problems, anxiety and pain. Unfortunately, such understandings are not always evident, as nurses often misperceive, underestimate or overestimate patient needs (Florin et al 2005, Sobo 2004). For this reason it is important that nurses share their perceptions with patients, clarify their understanding and paraphrase what the patient seems to be communicating. All of these skills are reviewed later in the chapter.
Healthcare environments and communication
Current healthcare environments can work against effective communication, especially when there is an emphasis on task completion and a sense of little time to do so. There are often competing demands in actual nursing practice that limit nurses’ capacity to spend time interacting and developing therapeutic relationships with clients. Most of the time nurses only interact with patients in hospital when performing a task or function (McCabe 2004, Newell & Jordan 2015). Lack of time is a factor that is often espoused by nurses as they perceive that communication that is focused on relationship-building takes more time than that focused on tasks (Chan et al 2012). The espoused professional value of the importance of therapeutic relationships is often at odds with the values of tasks needed to be completed in set timeframes, especially in organisational settings such as hospitals. In current healthcare systems, which are focused on efficiency, there is little value given to the importance of communication, and relating to and coming to know the patient is often not viewed as nursing ‘work’ (DeFrino 2009). Professional nurses must learn to reduce this variance by remaining true to the value placed on communicating with and relating to clients, in the knowledge that this is central to therapeutic practice. More importantly, they should be active in healthcare reform to redress the devaluing of communication with clients.
Communication and interpersonal relationships
At the core of nursing are caring relationships formed between nurses and clients, and communication is the means of establishing these relationships and coming to know the client. The knowledge gained about the client through relational work is at the heart of nursing practice, and the communication skills required are not simply a matter of ‘being nice’ to patients but rather are a professional duty (DeFrino 2009). The nurse’s ability to relate to others rests on effective interpersonal communication, which includes being able to take the initiative in establishing and maintaining communication, to be authentic (one’s self), and to respond appropriately to the other person.
Professional relationships are created through the nurse’s application of knowledge, understanding of human behaviour and communication, and commitment to the moral stance of being ‘for the client’. Having a philosophy based on caring and respect for others will help the nurse be more successful in establishing relationships of this nature with clients. Being responsive to client needs is basic to therapeutic communication. Nurses also communicate in the context of other professional relationships that may require an emphasis on being assertive. For example, when collaborating with a multidisciplinary healthcare team, nurses must be able to assert their views from the perspective of nursing knowledge.
Nurse–client relationships
Helping relationships with clients are central to therapeutic nursing practice. In such relationships, the nurse assumes the role of professional helper and comes to know the client as an individual who has unique health needs, human responses and patterns of living. Knowing the client is a central caring behaviour that also functions as an aid to clinical problem-solving and decision-making and is also central to client participation in care (Zolnierek 2014). Through knowing the client, nurses are able to understand health events from the experience of the client, adapt their care to the unique needs of the individual and judge how a person is responding to healthcare events. This type of knowing requires effective communication between nurse and client so that mutual understanding can be achieved.
Therapeutic and social relationships
Communication involves complex social activity more than other aspects of nursing practice, such as technical proficiency and skills. Through communication, nurses relate to a variety of people during direct client care and within healthcare organisations. However, the social activity in nursing is different from other forms of social activity, such as friendships. Communication in nursing is professional and therapeutic, and is thus different from communication in friendships.
In therapeutic nurse–client relationships there is an explicit timeframe, a goal-directed approach and a high expectation of confidentiality. The nurse establishes, directs and takes responsibility for the interaction, and the client’s needs take priority over the nurse’s needs. In acting in the client’s best interest, the nurse maintains professional boundaries.
There are clear legal boundaries, as nurses must practise within the scope of their professional knowledge and skill, while codes of conduct (ANMC 2008a, NCNZ 2009) specify ethical boundaries. However, professional boundaries are not always as clearly laid out as geographical ones, for example those between countries. Nurses cross professional boundaries when they do not act in the best interest of the patient (Hartlage 2012), but rather act in a manner that meets their own needs, such as the need to be liked. Having a sexual relationship with a client is a clear boundary violation, as it is focused on the nurse’s needs. More subtly, nurses can cross boundaries when they burden clients with their own problems, such as being short-staffed and under pressure. The relationship is always ‘for the patient’ and this is the best principle to follow in maintaining professional boundaries.
The relationship is also characterised by the nurse’s non-judgemental acceptance of the client. Acceptance conveys a willingness to hear a message or to acknowledge feelings. It does not mean the nurse must always agree with the other person or approve of the client’s decisions or actions.
A therapeutic relationship between nurse and client does not just happen – it is created with care and skill and is built on the client’s trust in the nurse. In her seminal work, Patricia Benner (1984) prefers not to use the term ‘therapeutic’ because of its association with psychotherapy, yet describes a helping role of the nurse in a similar fashion. She states that ‘helping encompasses transformative changes in meanings, and sometimes simply the courage to be with the client, offering whatever comfort the situation allows’ (Benner 1984:48). A helping relationship between nurse and client is one in which the nurse comes to understand the patient as a person with a unique point of view. Forming such relationships enables nurses to provide care that is individualised to that person and their family, therefore providing person-centred nursing care.
The nurse–client relationship is characterised by a natural progression of four goal-directed phases that often begin before the nurse meets the client, and continue until the caregiving relationship ends (Box 12-1). Even a brief interaction uses an abbreviated version of the same pre-interaction, orientation, working and termination phases. For example, the nursing student may gather client information to prepare in advance for caregiving, meet the client and establish trust, accomplish health-related goals through use of the nursing process and say goodbye at the end of the day.
Socialising is often an important initial component of interpersonal communication. It helps people get to know one another and relax. It is easy, superficial and not deeply personal, whereas therapeutic interactions are often more intense, difficult and uncomfortable. A nurse often uses social conversation to help the client feel comfortable and lay a foundation for a closer relationship. Clients value nurses being ‘friendly and chatty’ (Henderson et al 2007, McCabe 2004). An informal and warm communication style helps establish trust, but nurses must get beyond social conversation to talk about issues or concerns affecting the client’s health. During social conversation, clients may ask personal questions about the nurse’s family, place of residence and so on. Students often wonder if it is appropriate to reveal such information; that is, to self-disclose. In an attempt to ‘be professional’ they sometimes assume it is inappropriate to share anything of themselves. Although a high degree of self-disclosure is characteristic of intimate friendships, it does not fit the context of a therapeutic relationship; however, nurses can use self-disclosure to benefit the relationship with the client, provided they remain professional and do not overstep their professional boundaries (Stein-Parbury 2014).
Nurses often encourage clients to share personal stories; in doing so, nurses come to understand the context of other people’s lives and learn what is meaningful for them from their perspective. For example, a nurse asked a client to tell about a time in his life when he had to make a hard decision. He related the following story:
When I was a young man, I worked on the family farm. An uncle died and left me some money. All of a sudden I could afford to go to the city for a university education, but Dad didn’t want me to go because he needed me there. I had to decide whether to stay or go, and it was hard, because at first I just wanted to get away. I talked to our priest, and he said it was up to me, to pray about it and then do what my heart told me to. So I stayed. Oh, I’ve thought from time to time what might have been, but I never regretted it. I’ve had a good life on the land.
From this brief story, the nurse understood that it was important to the client to put his family’s needs above his personal desires, and that seeking spiritual guidance was an important component of his decision-making.
Nurses also provide information and use strategies that help clients understand and change behaviour. The nurse also acts as an advocate to keep the client informed of healthcare alternatives and give support in decision-making. For example, the nurse can ask clients and family members for input and suggestions about goals, interventions and evaluation of the plan of care. This type of mutuality (give-and-take, creative mutual exchanges) has been shown to balance power and respect, and to promote productive provider–client communication (Tejero 2012). It gives the other person a greater sense of purpose and direction, encourages personal responsibility for health, helps establish priorities for care, gives the opportunity for self-expression and strengthens the client’s problem-solving ability. This depends on the vulnerability of the client; that is, the degree to which personal resources are available, adequate and appropriate to the situation at hand. Information is one such possible resource.
Nurse–family relationships
Providing person-centred health care is not only focused on individual clients, but also includes involving families, which is being family-centred (see also Chapter 15). The same principles that guide one-to-one helping relationships apply when the client is a family unit, although communication within families requires additional understanding of the complexities of family dynamics, needs and relationships. For example, when communicating with families there is often a ‘spokesperson’ who may be the primary carer, but could also be the family member who is most knowledgeable about health matters or who knows the client most intimately.
Family members have needs for collaboration and involvement in care when their loved ones are in need of health care (Bauer & Nay 2011, Tallon et al 2015, Wong et al 2015). This is especially true when their loved one is in a highly vulnerable state, such as being a patient in an intensive care unit, being a child in hospital or experiencing cognitive impairment in dementia. The communication needs that are most relevant to family members are the need for information about their family member’s situation. Nurses are well placed to provide such information, especially as families have the most contact with nursing staff in the majority of healthcare settings.
In addition to their need for information, families require emotional support from nurses. Such support is perceived when nurses listen to their concerns (Tallon et al 2015). It is important for nurses to explore these concerns through clarifying and asking relevant questions. Often, their concerns are related to the need for information and assurance as to their loved one’s comfort and wellbeing.
While it is important that nurses recognise and meet the needs of families, it is equally important that they understand that families are an important source of information about clients. They are in a position to provide relevant health information and insights into the person who is the client. In addition, they are often in a position to act as advocates and speak on behalf of the client (Stein-Parbury et al 2015).
Healthcare team relationships
Nurses are members of a larger healthcare community and often function in roles that require interaction with multiple healthcare team members. The basic elements of effective communication that apply to the nurse–client relationship are also relevant in relationships with colleagues. That is, nurses must be responsive in understanding the views of their professional colleagues, and they must also be assertive in stating their views about client care. Communication in relationships with colleagues may be geared towards team-building, facilitating group process, collaboration, consultation, delegation, supervision, leadership and management. Various communication skills are needed, including presentational speaking, persuasion, group problem-solving, providing performance reviews and writing business reports.
Both social and therapeutic interactions are needed between the nurse and other healthcare team members to build morale and strengthen relationships within the work setting. Nurses need friendship, support, guidance and encouragement from one another to cope with the many stressors imposed by the nursing role, and must extend the same caring communication used with clients to build positive relationships with colleagues and co-workers.
Collaboration in healthcare team communication
In the contemporary healthcare climate there is a focus on enhancing teamwork and interprofessional collaboration that is focused on improved quality and safety. In part this is due to reports that demonstrate that poor and inadequate interprofessional communication is a major factor in events that result in patient harm (Brock et al 2013). Pannick et al (2014) identified that staff communication and collaboration with colleagues was a major theme in a review of evidence related to quality and safety of general medical units, rather than specialised units that have more stable teams such as intensive care or operating theatre units. Therefore, improving collaborative teamwork as a way to enhance positive patient outcomes is receiving attention because this is believed to have a greater effect than other strategies (Barrow et al 2015).
Team collaboration works best when members of the team are able to communicate effectively and develop an understanding of each other’s perspective. In doing so they develop what is termed a ‘shared mental model’ (McComb & Simpson 2013). Effective collaboration in the form of interdisciplinary rounds has proven to be an effective way to decrease errors and improve patient safety; these rounds work best when there are structured systems for the communication of patient information. Such systems are ‘shared mental models’, which have been shown to improve quality and safety. One of the most widely used formats is the ISBAR tool, which is used for patient handover, as described in Skill 12-1.
Delegation and other considerations
Patient handover can be conducted by any healthcare professional providing care for the patient. Where possible, the registered or enrolled nurse who is providing direct care for the patient should be the one to provide the handover. If this is not the case, the nurse in charge or a senior nurse familiar with the patient should provide handover.
Therapeutic relationship and patient considerations
• Initiates communication by introductions and clarification of patient’s immediate needs and problems
• Identifies how the skill will affect the patient
• Discusses procedure with the patient to clarify understanding
• Assesses patient knowledge and expectations and ensures patient understanding
• Where necessary, provides further clarification
• Explains actions and potential discomfort at all stages of procedure
| STEPS | RATIONALE | |
|
|
||
| An increasing number of healthcare facilities conduct handover at the bedside. To a patient who is new to the ward or unfamiliar with the handover procedure, this may be confronting or confusing. Remember to ensure patient confidentiality when conducting a bedside handover – all confidential information should be discussed later and in a private area (Higgs et al 2012). | ||
| It is important that you make sure your patient is comfortable and pain-free prior to handover. Although standardised handovers are designed to shorten handover, delays are possible (Street et al 2011). | ||
| Ensuring that all required information is available will prevent interruptions and ensure smooth delivery of patient information. | ||
| Introducing yourself professionally improves collegiality and ongoing or future working relationships. To prevent errors, use a minimum of three (3) identifiers for each patient, when handing over (South Australia Health 2012). | ||
| Explain to the receiver what is happening to the patient and why you are providing handover. Depending on the location and mode of communication, the situation may be obvious. | ||
| Explain the story of the patient and identify the current problem, relevant information and any interventions (medication, IV fluids, CT scans) that have been completed (LeMone et al 2014, Marshall et al 2009). | ||
| It is important to utilise critical thinking based on the assessment of the patient, and not an opinion. Make sure this information is clear and not confusing to the receiver. | ||
| Be specific about what you want from the receiver – patient transfer, patient review, medication or patient handover. | ||
| RECORDING AND REPORTING | HOME CARE CONSIDERATIONS | |
 Critical decision point: Prior to handover, review all your patients and charts to ensure the information that you are going to give is accurate and up to date.
Critical decision point: Prior to handover, review all your patients and charts to ensure the information that you are going to give is accurate and up to date.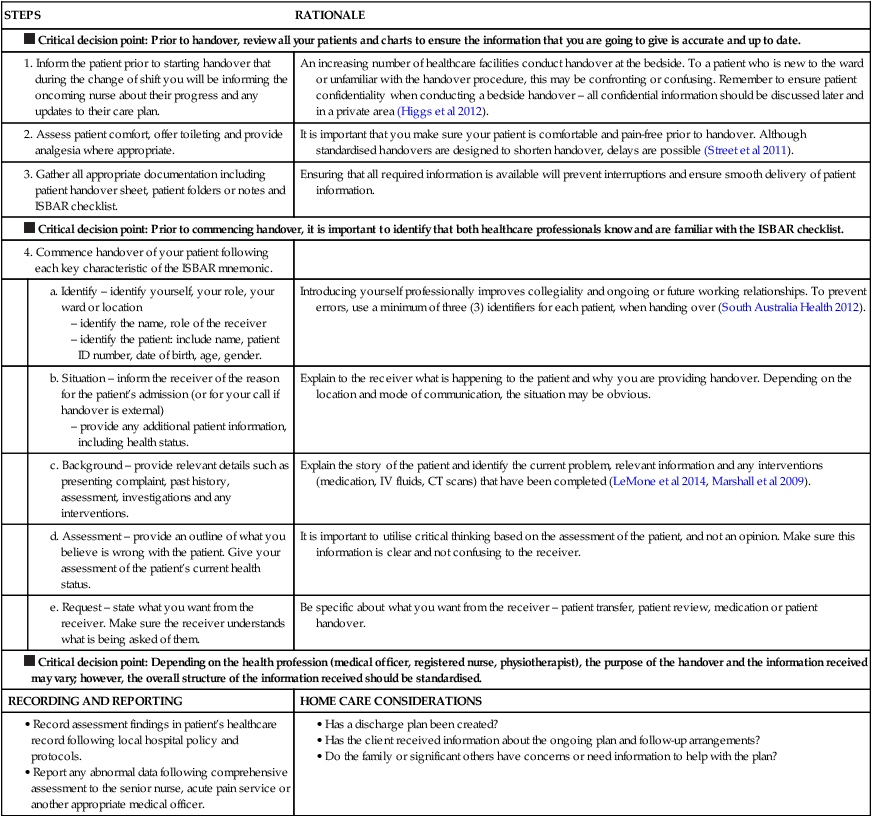
Nursing knowledge and healthcare team collaboration
When nurses collaborate with other healthcare professionals they bring knowledge that is specific to the practice of nursing. While nurses can communicate their knowledge of the patient’s clinical condition (case knowledge), their focus is related more to the patient and person knowledge. Their focus on patient knowledge means that they will bring an understanding of how the patient/client is responding to their clinical condition and its treatment, for example, the degree of distress experienced or a side effect of medication. In addition, they are likely to know the private, idiosyncratic world of the patient (person knowledge), including their values and belief systems. It is for this reason that interprofessional communication can break down because different professionals operate from a different, albeit potentially compatible, knowledge base (Barrow et al 2015, Stein-Parbury & Liaschenko 2007); they do not share the same ‘mental model’.
The potential breakdown in communication may result in conflict between professionals because they simply do not fully understand the perspective of the other and do not make the communicative effort to build mutual understanding. Conflict in communication is not necessarily negative; in workplace situations it can be positive as multiple perspectives are brought to bear in solving problems.
Collaboration and conflict
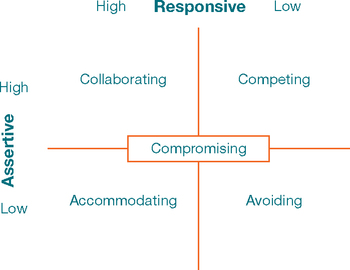
When conflict does arise, there are a number of ways that a healthcare professional can respond. They can become:
• aggressive and competitive – not attending to others’ concerns and running rough shod over others;
• passive and avoidant – not engaging and evading the conflict;
• accommodating and submissive – neglecting own concerns and acquiescing to others;
• compromising and finding the middle ground – partially satisfying both concerns; or
• collaborative and understanding – fully satisfying both concerns (Thomas & Killman 1977).
These ways of responding in a conflict situation directly relate to communication competence as depicted in Figure 12-3. An aggressive response is domineering communication; a submissive response is accommodation communication. Avoiding or evading conflict is considered to be ineffecitive at resolving conflicts. The competent communicator will approach conflict in a collaborative way. A compromising response relates to all aspects of communication competence. Finding a middle ground through compromise, negotiating a ‘give-and-take’ solution, may work in some contexts, such as conflict over workload; but a compromise in the healthcare setting may jeopardise patient safety and wellbeing. Collaboration, where all voices are heard and understood, including the patient’s viewpoint and wishes, has been shown to result in quality and safety in the healthcare arena (Pannick et al 2014).
Evidence shows that nurses who work in a clinical setting tend to be accommodating and submissive when dealing with interprofessional conflict (Iglesias & de Bengoa Vallerjo 2012, Kaitelidou et al 2012, Mahon & Nicotera 2011). They are likely to meet conflict in the workplace in a passive manner, rather than with active and assertive attempts to collaborate. While this tactic may keep the peace, failing to express a viewpoint that is different from others’ can result in poor quality health care. People who use passive strategies are seen as more likeable and this may be one reason nurses behave this way. Another reason is that nurses are trained to communicate therapeutically; they focus on feelings, rather than finding solutions to conflict (Northam 2009). Because they are caring and compassionate towards patients, nurses may suffer under what Street (1992) has termed the ‘tyranny of niceness’. That is, they may think that active assertion, which is required for successful negotiation, is not compatible with being a caring person (McCartan & Hargie 2004).
Not only are passive strategies, such as avoiding and giving in, not always successful in resolving the conflict, but they are also associated with increased stress and decreased mental wellbeing in nurses (Chang et al 2007). Therefore, it is important that nurses learn how to deal with workplace conflict through the use of assertive skills. When used deliberately, compromising and acquiescing can be assertive in their own right; however, more active assertion is often required when dealing with workplace conflict. Successful resolution of conflicts can bring people closer and adds to satisfaction and creativity in the workplace; when handled poorly, conflicts can create extra strain and tension. More importantly, workplace conflict affects patient outcomes and leads to errors (Northam 2009).
Levels of communication
Nurses use different levels of communication in their professional role. The nurse’s communication skills need to include techniques that reflect competence at each level.
Intrapersonal communication
Intrapersonal communication is a powerful form of communication that occurs within an individual. This level of communication is also called self-talk, self-verbalisation, self-instruction, inner thought and inner dialogue. People’s thoughts strongly influence perceptions, feelings, behaviour and self-concept. Intrapersonal communication creates a set of conditions through which life is experienced. Nurses should be aware of the nature and content of their thinking and try to replace negative, self-defeating thoughts with positive assertions. Positive self-talk can be used as a tool to improve the nurse’s or client’s health and self-esteem. Self-instruction can provide a mental rehearsal for difficult tasks or situations so individuals can deal with them more effectively. Nurses and clients can use intrapersonal communication to develop self-awareness and a positive self-concept that will enhance appropriate self-expression.
Interpersonal communication
Interpersonal communication is one-to-one interaction between the nurse and another person that often occurs face to face. It is the level most often used in nursing situations and lies at the heart of nursing practice. It takes place within a social context and includes all the symbols and cues used to give and receive meaning. Since meaning resides in persons and not in words, messages received may be different from messages intended. Nurses work with people who have different opinions, experiences, values and belief systems, so meaning must be validated or mutually negotiated between participants.
Small-group communication
Small-group communication is interaction that occurs when a small number of people meet together. This type of communication is usually goal-directed, and requires an understanding of group dynamics. When nurses work on taskforces or committees, lead client support groups, form research teams or participate in client care conferences, a small-group communication process is used. Small groups are more effective when they are a workable size, have an appropriate meeting place, suitable seating arrangements, and cohesiveness and commitment among group members (Hybels & Weaver 2008). Small-group communication is effective when the group achieves its objectives in a manner that is inclusive of all members and results in satisfaction with decision-making processes.
Forms of communication
Messages are conveyed verbally and non-verbally, concretely and symbolically. As people communicate, they express themselves through words, movements, voice inflection, facial expressions and use of space. These elements can work in harmony to enhance a message, or conflict with one another to contradict and confuse it.
Verbal communication
Verbal communication uses spoken or written words. Verbal language is a code that conveys specific meaning as words are combined. The most important aspects of verbal communication are discussed below.
Vocabulary
Communication is unsuccessful if people cannot translate each other’s words and phrases. When a nurse cares for a client who speaks another language, an interpreter may be necessary. Even those who speak the same language use variations of certain words: dinner may mean a noon meal to one person and the last meal of the day to another. Medical jargon (technical terminology used by healthcare providers) may sound like a foreign language to clients unfamiliar with the healthcare setting, and should be used only with other healthcare team members. Children have a more limited vocabulary than adults. They may use special words to describe bodily functions or a favourite blanket or toy. Teenagers often use words in unique ways that are unfamiliar to adults.
Meanings of words and phrases
A single word can have several meanings. The denotative meaning is shared by individuals who use a common language: ‘tennis’ has the same meaning for everyone who speaks English, but the word ‘drug’ may have different meanings to a healthcare professional and to a layperson. The connotative meaning is the shade or interpretation of a word’s meaning influenced by the thoughts, feelings or ideas people have about the word. Families who are told a loved one is in a serious condition may believe that death is near, but to nurses ‘serious’ may simply describe the nature of the illness. Nurses should carefully select words that cannot be misinterpreted, especially when explaining a client’s medical condition or therapy. Even a much-used phrase such as ‘I’m going to take your observations’, can be unfamiliar to an adult or frightening to a child.
Clarity and brevity
Effective communication is simple, brief and direct. Fewer words result in less confusion. Speaking slowly and using examples to make explanations easier to understand achieves clarity. Repeating important parts of a message also clarifies communication. Phrases such as ‘you know’ or ‘okay?’ at the end of every sentence detract from clarity. Brevity is achieved by using short sentences and words that express an idea simply and directly. ‘Where is your pain?’ is much better than ‘I would like you to describe for me the location of your discomfort’.
Timing and relevance
Timing is critical in communication. Even though a message is clear, poor timing can prevent it from being effective. For example, the nurse should not begin routine teaching when a client is in severe pain or emotional distress. Often the best time for interaction is when a client expresses an interest in communicating. If messages are relevant or important to the situation at hand, they are more effective. When a client is facing emergency surgery, discussing the risks of smoking is less relevant than explaining how to keep the lungs clear postoperatively.
Non-verbal communication
Non-verbal communication is message transmission through body language, without using words. Non-verbal communication often reveals true feelings because it is hard to control: a colleague who says nothing is wrong but has tears in her eyes is probably in distress. Non-verbal cues add depth to verbal messages and help the nurse judge their reliability. Becoming an astute observer of non-verbal behaviour takes practice, concentration and sensitivity to others. Nurses should avoid sending ‘mixed messages’ through non-verbal communication.
Intonation
Tone of voice dramatically affects a message’s meaning. Depending on intonation, even a simple question or statement can express enthusiasm, anger, concern or indifference. The nurse must be aware of voice tone to avoid sending unintended messages. For example, clients may interpret a nurse’s patronising tone of voice as condescending, and further communication may be inhibited. A client’s voice tone often provides information about their emotional state or energy level.
Posture and gait
The ways people sit, stand and move reflect attitudes, emotions, self-concept and health status. For example, an erect posture and a quick, purposeful gait communicate a sense of wellbeing and confidence. Leaning forwards conveys attention. A slumped posture and slow, shuffling gait may indicate depression, illness or fatigue.
Facial expression
The face is the most expressive part of the body. Facial expressions convey emotions such as surprise, fear, anger, disgust, happiness and sadness. Some people have an expressionless face, or flat affect, which reveals little about what they are thinking or feeling. An inappropriate affect is a facial expression that does not match the content of a verbal message, such as smiling when describing a sad situation. People can be unaware of the messages their expressions convey. For example, a nurse may frown in concentration while doing a procedure and the client may interpret this as anger or disapproval. Clients often closely observe nurses. Although it is hard to control all facial expression, the nurse should develop awareness of meanings that are conveyed through facial expression.
Eye contact
People signal readiness to communicate through eye contact. Maintaining eye contact during conversation shows respect and willingness to listen. Eye contact also allows people to closely observe one another. Lack of eye contact may indicate anxiety, defensiveness, discomfort, or lack of confidence in communicating. However, in some cultures, eye contact with a person who is considered superior can be interpreted as offensive and disrespectful (see Chapter 14).
Gestures
Gestures emphasise, punctuate and clarify the spoken word. Gestures alone carry specific meanings, or they may create messages with other communication cues. A finger pointed towards a person may communicate several meanings, but when accompanied by a frown and a stern voice, the gesture becomes an accusation or threat. Pointing to an area of pain may be more accurate than describing the pain’s location.
Territoriality and personal space
Territoriality is the need to gain, maintain and defend one’s right to space. Territory is important because it provides people with a sense of identity, security and control. Territory can be separated and made visible to others, such as a fence around a yard or a bed in a hospital room. Personal space is invisible, individual and travels with the person. During interpersonal interaction, people maintain varying distances between one another depending on their culture, the nature of their relationship, and the situation (Chapter 14). When personal space is threatened, people respond defensively and communicate less effectively. This is especially important when interacting with a client who is in bed, as ‘standing over’ them is often intimidating. Situations dictate whether the interpersonal distance between nurse and client is appropriate. Examples of nursing actions within zones of personal space are listed in Box 12-2, along with zones of touch. Nurses often move into clients’ territory and personal space due to the nature of caregiving. The nurse must convey confidence, gentleness and respect for privacy, especially when actions require intimate contact or involve a client’s vulnerable zone.
Developing communication skills
The complex array of communication skills that nurses are required to develop and maintain is detailed later in this chapter and categorised according to therapeutic intention. Beginning practitioners of nursing will notice that they are inclined to use some skills more than others and that some skills come more naturally than others.
Developing professional communication competence means paying close attention to these personal habits and predilections through critical reflective practice. The deliberate use of skills that do not come naturally requires conscious effort and consideration of therapeutic intention.
Self-awareness is critical to the development of effective communication skills because the way that they are used will be personal and unique to each nurse. Awareness of personal values and beliefs is especially important, as these may interfere with being open with and accepting of clients. For example, a belief that people who engage in behaviours that are harmful to their health, such as smoking and overeating, are weak-willed may hinder a nurse’s effort to be helpful.
The need to ‘unlearn’ previous communication patterns
When interacting with clients in a professional role, beginning nurses will often rely on their usual communication patterns, some of which are neither helpful to the client nor to the development of a therapeutic relationship. These include expressing approval or disapproval, stereotypical responses and false reassurance.
Approval and disapproval
In everyday conversations people often express approval or disapproval, yet in a professional role it is not helpful to clients when nurses impose their own attitudes, values, beliefs and moral standards. Other people have the right to be themselves and make their own decisions. Judgemental responses by the nurse often contain terms such as ‘should’, ‘ought’, ‘good’, ‘bad’, ‘right’ or ‘wrong’. Agreeing or disagreeing sends the subtle message that nurses have the right to make value judgements about client decisions. Approving implies that the behaviour being praised is the only acceptable one. Often, the client shares a decision with the nurse, not in an effort to seek approval but to provide a means for discussing feelings. On the other hand, disapproving implies that the client must meet the nurse’s expectations or standards; for example, commenting that ‘It is silly for you to feel like that’. Instead, the nurse should help clients explore their own feelings, beliefs and decisions. The nursing response ‘I’m surprised you say that you feel that way. Tell me more about it’ gives the client a chance to express ideas or feelings without fear of being judged.
Stereotypical responses
A cliché is a stereotypical comment, such as ‘You can’t win them all’ or ‘Every cloud has a silver lining’ that tends to belittle the other person’s feelings and minimise the importance of their message. These automatic phrases communicate that the nurse is not taking concerns seriously or responding thoughtfully. Most often they are said with a good intention, to reassure a client; however, they are a form of false reassurance and are often not helpful.
False reassurance
Saying ‘Don’t worry, everything will be all right’ may make the nurse feel better, but it does not have the same effect on the client. When a client is seriously ill or distressed, the nurse may be tempted to offer hope to the client with statements such as ‘You’ll be fine’ or ‘There’s nothing to worry about’. When a client is reaching for understanding, false reassurance from the nurse may discourage open communication. Offering reassurance not supported by facts or not based in reality can do more harm than good. Although it might be intended kindly and have the secondary effect of helping the nurse avoid the other person’s distress, it tends to block conversation and discourage further expression.
Elements of professional communication
Professional appearance, demeanour and behaviour are important in establishing the nurse’s trustworthiness and competence. They communicate that the nurse has assumed the professional helping role, is clinically skilled and is focused on the client. An individual nurse’s inappropriate appearance or behaviour can harm nursing’s professional image.
At work a healthcare professional is expected to be clean, neat, well groomed, conservatively dressed and free of strong scent and other odours. Professional behaviour should reflect warmth, friendliness, confidence and competence. Professionals speak in a clear, well-modulated voice, use good grammar, listen to others, help and support team-mates and communicate effectively. Being on time, organised, well prepared and equipped for the responsibilities of the nursing role also communicate one’s professionalism.
Courtesy and use of names
Common courtesy is part of professional communication. To practise courtesy, nurses need to remain friendly, ask permission to enter the client’s space, address clients by name and always introduce themselves to clients by stating their name and explaining their role and purpose for interacting. This last point is particularly important when students are caring for clients in the clinical setting, as it is important that the student role of learner is understood by clients. The nurse’s failure to give a name, indicate status (e.g. student, registered nurse or enrolled nurse) or acknowledge the client by name can convey an impersonal lack of commitment or caring. More importantly, clients have the right to know who is talking to them and in what professional capacity.
Addressing others by name conveys respect for human dignity and uniqueness. Using surnames is respectful in most cultures, but may seem too formal in others (Chapter 14). Therefore, in the initial interaction with clients the nurse should always ask them how they would prefer to be addressed and let others know their personal preference. Using first names is appropriate for infants, young children, confused or unconscious clients and close team members. Terms of endearment such as ‘luv’, ‘dolls’, ‘Grandma’ or ‘darling’ are inappropriate in a professional interaction. Avoid referring to clients by diagnosis, room number or other attribute, as it is demeaning and sends the message that the nurse does not care enough to know the person as an individual.
Privacy and confidentiality
Maintaining confidentiality is a sign of respect and a hallmark of professional behaviour. It is essential that the nurse safeguard the client’s right to privacy by carefully protecting information of a sensitive nature. Sharing personal information or gossiping about others violates nursing ethical codes and practice standards. It sends the message that the nurse cannot be trusted and damages interpersonal relationships. Team members directly involved in the client’s care should be given only relevant information about the client’s status.
Trustworthiness
Trust is relying on someone without doubt or question. Being trustworthy means helping others without hesitation when help is needed. To foster trust, the nurse communicates warmth and demonstrates consistency, reliability, honesty and competence. Sometimes it is not easy for a client to ask for help. Trusting another person involves risk and vulnerability, but it also fosters open, therapeutic communication and enhances the expression of feelings, thoughts and needs. Without trust, a nurse–client relationship rarely progresses beyond superficial interaction and care. Avoid dishonesty at all costs. Knowingly withholding key information, lying or distorting the truth violates both legal and ethical standards of practice.
Respect
Respect is based on the belief that every human has inherent worth and dignity (Stein-Parbury 2014). Demonstrating respect is one of the central keys to effective interpersonal communication in nursing because respect means accepting the client’s perspective and assuming their goodwill. Respect generates from a belief that the client is capable and resourceful. This involves being open and not imposing the nurse’s value system on the client; that is, not judging the client because they hold views and beliefs that are different and possibly foreign to the nurse. Respect is especially relevant when communicating with clients who are of a different cultural background to the nurse.
For example, maintaining eye contact is a sign of trustworthiness in most Western cultures; that is, ‘looking people in the eye’ demonstrates honesty. In other cultures it is disrespectful to make eye contact with a person who is perceived as superior. Clients who avoid eye contact with nurses could be demonstrating respect, not dishonesty. Sensitivity to the culture of other people is needed in respectful communication (Chapter 14).
More importantly, nurses should not base their judgements about client behaviour on the basis of their own culture alone; this is disrespectful. Similarly, it is important to avoid cultural stereotypes that assume all people of a certain background will behave in the same way. Such thinking can lead to misunderstanding and a failure to communicate. An even greater danger of stereotyping is the risk that clients will be rejected or negatively judged because a nurse does not understand and respect their cultural value and belief systems.
Therapeutic communication techniques
The most basic nursing interventions used in communication are therapeutic communication techniques. Therapeutic communication techniques are specific responses that encourage the expression of feelings and ideas and convey the nurse’s acceptance and respect. Learning these techniques helps the student develop awareness of the variety of nursing responses available for use in different situations. Although some of the techniques may seem artificial at first, skill and comfort will increase with practice. Tremendous satisfaction will result as therapeutic relationships and outcomes are achieved.
Heron (2001) offers a useful schema for understanding therapeutic intention through a classification system of two types of communication interventions: authoritative and facilitative. Authoritative interventions take responsibility on behalf of the client; facilitative interventions promote client autonomy and self-responsibility. When a nurse offers a client new knowledge, makes suggestions or directs the client, authoritative intentions are at play. When a nurse encourages a client to solve problems and express emotions, then facilitative interventions are at play.
The basis for Heron’s intervention analysis is similar to the responsive and assertive dimensions of effective communication (presented earlier in this chapter). Authoritative interventions are assertive in nature and focus on new understandings, such as instructing a client newly diagnosed with diabetes on dietary management. Facilitative interventions are responsive and focus on existing understandings, such as how the client is experiencing a health event. Both types of interventions are potentially therapeutic, depending on context.
Facilitative communication techniques form the backbone of therapeutic communication because they help to build a relationship based on mutual understanding, and this type of mutuality is the basis of therapeutic relationships in nursing practice. In order to be of help, nurses must understand the meaning of a health event from the perspective of the client and their experience of that event.
At times, facilitative communication is therapeutically sufficient. For example, clients often find comfort in another person’s human understanding of their situation; they might gain relief through finding humour in their situation. At other times, authoritative communication techniques are necessary to therapeutic endeavours, such as encouraging and persuading a recently disabled adult client to participate in everyday activities like dressing himself.
The choice between the two techniques depends on the vulnerability of the client. Determining the vulnerability of the client requires assessment of the resources available to meet the demands of a health event. The therapeutic communication techniques that follow are categorised according to therapeutic intention, as listed in Box 12-3.
Facilitative communication interventions
Facilitative techniques encourage clients to think for themselves and facilitate mutual understanding between them and the nurse. They are considered the backbone of therapeutic communication and are based on a philosophy of patient-centred care. When using facilitative techniques, the nurse follows the client’s lead.
Active listening
Active listening means listening attentively with one’s whole being – mind, body and spirit. It includes listening for conversational themes, acknowledging and responding, giving appropriate feedback and paying attention to the other person’s total communication, including the content, the intent and the feelings expressed (Stein-Parbury 2014). Active listening allows the nurse to better understand the entire message being communicated, and is an excellent way to build trust. In many nursing situations the other person simply needs someone to listen.
To listen attentively, the nurse faces the client at a distance of about 90 cm, removes any physical barriers if possible, maintains eye contact (if culturally appropriate), assumes a relaxed posture and sits quietly, leans forward slightly and nods in acknowledgment when the client talks about important points or looks for feedback. Fidgeting, breaking eye contact, daydreaming during conversation or only pretending to listen conveys the message that what the other person has to say is not important. These inhibit conversation and undermine trust.
Being available means offering oneself and expressing a willingness to listen, talk or be physically present with another person when the client needs it. By expressing availability, even though the client may not make their needs known, the nurse shows a caring attitude. When clients feel that the nurse is listening they sense a connection that enables the relationship to develop; they value nurses who take the time to listen to them (Kagan 2008, Marshall et al 2012). Therefore, listening is essential to the process element of therapeutic communication.
Availability and active listening are often described as nursing presence, an inter-subjective encounter between a nurse and a client in which the nurse encounters the client as a unique human being in a unique situation and chooses to ‘spend’ themself on the client’s behalf (Zyblock 2010). Presence is the nursing quality of ‘being there’ for the client – not just physically present, but also listening attentively from a caring perspective: ‘I’ll stay with you a while. If you want to talk, I’ll be glad to listen.’ However, the ability to be fully present does not lie simply within the nurse; it requires a healthcare environment that is conducive to the formation of relationships between nurses and clients (Fingeld-Connett 2008, McMahon & Christopher 2011).
Challenges and potential pitfalls when listening
One of the key factors in being able to actively listen to clients is an ability to ‘tune out’ other thoughts in order to fully attend. Often when nurses are attempting to listen they are preoccupied with other matters; for example, they may be thinking about an onerous workload or worrying about a personal matter. More subtle is the tendency to make judgements about what a client is saying; for example, by thinking that the client is being silly or complaining too much. When emotions are being expressed, especially when clients are angry, it is often difficult to hear what they are expressing.
Changing the subject is an indication that the nurse is not listening; for example, saying, ‘Let’s not talk about your problems with the insurance company. It’s time for your walk.’ Changing the subject when another person is trying to communicate something important is rude and shows a lack of empathy. It tends to block further communication, and the client may then withhold important messages or fail to openly express feelings.
Using silence
It takes time and experience to become comfortable with silence. Most people have a natural tendency to fill empty spaces with words, but sometimes those spaces give time for the nurse and client to collect their thoughts and consider what has been communicated. Silence also allows the nurse to pay particular attention to nonverbal messages, such as worried expressions or loss of eye contact. Remaining silent demonstrates the nurse’s patience and willingness to wait for a response when the other person is unable to reply quickly. Silence may be especially therapeutic during times of profound sadness or grief.
Sharing observations
Nurses make observations by commenting on how the other person looks, sounds or acts. Stating observations often helps the client communicate without the need for extensive questioning, focusing or clarification. For example, the nurse observes a young client holding his body rigidly erect and his voice being sharp as he says, ‘Going to surgery is no big deal’. The nurse replies, ‘You say having surgery doesn’t bother you, but you look a little worried. It is natural to worry about surgery.’ This approach may result in encouraging the client to further express current concerns.
Sharing feelings
Emotions are subjective feelings that result from one’s thoughts and perceptions. Feelings are not right, wrong, good or bad, although they may be pleasant or unpleasant. If feelings are not expressed, stress and illness can worsen. Nurses can help clients express emotions by making observations, acknowledging feelings, encouraging communication, giving permission to express ‘negative’ feelings and modelling healthy emotional self-expression. At times, clients may direct anger or frustration prompted by their illness towards the nurse, who should not take such expressions personally. Acknowledging clients’ feelings communicates that the nurse listened to and understood the emotional aspects of their illness.
When nurses care for clients they must be aware of their own emotions, because feelings are difficult to hide. Students may wonder whether it is helpful for the nurse to share feelings with clients. Sharing emotion makes nurses seem more human and can bring people closer. It is appropriate to share feelings of caring, or even cry with others, as long as the nurse is in control of how those feelings are expressed and does so in a way that does not burden the client. Feelings are shared with clients in an effort to assist them, not the nurse.
Expressing empathy
Empathy is the ability to understand and accept another person’s reality and to accurately perceive feelings. Empathic communication conveys that the nurse not only has heard what the client has expressed, but also understands what the client means. In expressing empathy, the nurse communicates this understanding to the client. Such empathic understanding requires the nurse to be both sensitive and imaginative, especially if the nurse has not had similar experiences. Statements reflecting empathy are highly effective because they tell the person that the nurse heard the feeling content, as well as the factual content, of the communication. This results in clients feeling accepted and valued, thereby facilitating the therapeutic relationship.
Challenges and pitfalls in expressing empathy
There is a difference between empathy and sympathy. An example of a sympathetic expression is ‘I feel so sorry about your amputation; it would be terrible to lose a leg.’ Sympathy is concern, sorrow or pity felt for the client generated by the nurse’s personal identification with the client’s needs. Empathy is imagining what it would be like to be in the circumstances of the client; sympathy is assuming that the nurse knows what it is like (Stein-Parbury 2014). Sympathy is a subjective look at another person’s world that prevents a clear perspective of the issues confronting that person. Although sympathy is a compassionate response to another’s situation, it is not as therapeutic as empathy. A more empathic approach would be: ‘Losing your leg has been a major change. How has it affected your life?’ While it may seem that such a response might increase client distress, evidence shows that an empathic response such as this actually decreases their distress and enables them to cope (Lelorain et al 2012).
Offering hope
Hope is productive to healing, and offering hope communicates a ‘sense of possibility’ to clients (Fitzgerald Miller 2007). Appropriate encouragement and belief that the client can cope, along with concrete feedback about how the client is progressing, are important in fostering hope by boosting self-confidence and helping clients achieve their potential. Sharing a vision of the future and reminding others of their resources and strengths can also strengthen hope. Clients can be reassured that there are many kinds of hope and that meaning and personal growth can come from illness experiences (Fitzgerald Miller 2007).
Sharing humour
Humour is an important therapeutic resource in nursing interactions. It serves to build relationships by conveying respect for the personhood of the patient and creates a sense of cohesiveness between nurses and their clients. It helps decrease client anxiety, depression and embarrassment. Laughter can be good medicine when nurses use humour to help clients adjust to stress imposed by illness. Humour can increase the nurse’s effectiveness in providing emotional support to clients and can humanise the illness experience. Laughter provides both a psychological and a physical release for both nurse and client. Humour can help others to interact more openly and comfortably and can make nurses’ own humanity more apparent.
Using touch
Touch is one of the nurse’s most potent forms of communication. Nurses are privileged to experience more of this intimate form of personal contact than almost any other professional. Many messages, such as affection, emotional support, encouragement, tenderness and personal attention, are conveyed through touch. Comfort touch, such as holding a hand, is especially important for vulnerable clients who are experiencing severe illness with its accompanying physical and emotional losses.
Since much of what nurses do involves touching, nurses must learn to be sensitive to others’ reactions to touch and use it wisely. There are times when touch should be withheld; highly suspicious or angry people may respond negatively or even violently to the nurse’s touch.
Asking relevant questions
Asking questions allows nurses to seek information that is vital to client care. Nurses should ask only one question at a time, and fully explore one topic before moving to another area. During client assessment, questions follow a logical sequence and usually proceed from the general to the more specific. Open-ended questions allow the client to take the conversational lead and introduce pertinent information about a topic: ‘What happens when you and your husband argue?’ Focused questions are used when more-specific information is needed in an area: ‘What do you argue about most often?’ The nurse should allow clients to fully respond to an open-ended question before asking more-focused questions. Closed-ended questions elicit a yes, no or single-word response: ‘How many arguments did you have last week?’ They are generally less useful during therapeutic exchanges, although they are often essential to client assessment.
Challenges and potential pitfalls in questioning
Asking too many questions can be dehumanising, because clients can feel as though they are being treated like an object. A useful exercise is to try conversing without asking the other person a single question. By giving general leads (’Tell me about it …’), making observations, paraphrasing, focusing, providing information and so on, nurses can discover much of importance that would have remained hidden if questions alone had been used during the communication process.
A nurse may be tempted to ask clients to explain why they believe, feel or have acted in a certain way. Asking for explanations, for example, ‘Why are you so anxious?’, is not helpful to clients; people often do not know why they feel the way they do, and a question such as this can put them on the defensive. Moreover, clients frequently interpret ‘why’ questions as accusations and this can cause resentment, insecurity and mistrust (Stein-Parbury 2014). They are best avoided and replaced with open-ended questions that explore the situation further.
Asking personal questions that are not relevant to the situation simply to satisfy the nurse’s curiosity, for example ‘Why don’t you and John get married?’, is not appropriate professional communication. Such questions are intrusive and unnecessary. If clients wish to share private information they will. If the nurse needs to know more about the client’s interpersonal roles and relationships, a question such as ‘How would you describe your relationship with John?’ can be asked.
Paraphrasing
Paraphrasing is re-stating another’s message briefly, using one’s own words. Through paraphrasing, the nurse sends feedback that lets others know whether their messages were understood. If the meaning of a message is changed or distorted through paraphrasing, communication may become ineffective. For example, a client may say ‘I’ve been overweight all my life and never had any problems. I can’t understand why I need to be on a diet’. Paraphrasing this statement by saying ‘You don’t care if you’re overweight or not’ is incorrect. It would be more accurate to say ‘You’re not convinced you need a diet because you’ve stayed healthy’.
Paraphrasing is an effective way to clarify what a client is communicating. By putting their words into the nurse’s own words, clients can not only correct any misunderstandings, for example, ‘That’s not exactly what I meant’, but can also expand and elaborate on what they are meaning. A paraphrase is a useful way to encourage further interaction by demonstrating that the nurse is trying to understand the client’s experience.
Challenges and pitfalls in paraphrasing
Paraphrasing is not the same as parroting – repeating what the other person has said word for word. Parroting is easily overused and is not as effective as paraphrasing. A simple ‘Oh?’ can give the nurse time to think if the other person says something that takes the nurse by surprise.
Nurses are sometimes reluctant to paraphrase what clients say out of fear of appearing incompetent; that is, they think that they should just know what the client means without having to say what they think. Another reason for a reluctance to use a paraphrase is the fear of ‘reinforcing’ distressing negative emotions, when that is what the client is conveying. The paraphrase is comforting to clients when they are distressed because it demonstrates that the nurse is listening and trying to understand (Stein-Parbury 2014).
Clarifying
To check whether understanding is accurate, the nurse can re-state an unclear or ambiguous message to clarify the meaning. Instead of paraphrasing the message, the nurse can also ask the other person to rephrase it, explain further or give an example of what the person means. Without clarification, the nurse may make invalid assumptions and miss valuable information. Despite efforts at paraphrasing, the nurse may not understand the client’s message and should let the client know if this is the case: ‘I’m not sure I understand what you mean by “sicker than usual”. What is different now?’
Authoritative communication interventions
Authoritative communication operates from the philosophy that the nurse needs to take charge and lead the client, instead of following the client, as is the case with facilitative techniques. While authoritative techniques can be used to promote client autonomy, for example, through health teaching, often they are not as patient-centred as facilitative techniques. More importantly, they are often overused in healthcare situations.
Providing information
Providing relevant information tells other people what they need or want to know so that they can make decisions, experience less anxiety and feel safe and secure. It is also an integral aspect of health teaching. It is usually not helpful to hide information from clients, particularly when they seek it. Clients have a right to know about their health status and what is happening in their environment.
Research has shown that the provision of information is highly individual in the sense that some clients require more information than others (Tobiano et al 2015). Identification of the amount and type of information needed by an individual client is essential in the use of this intervention.
Suggesting
Nurses often help clients by offering suggestions about what might be of benefit. For example, a nurse might suggest distraction as a useful way to cope with worry about pending diagnostic results. Suggestions should be posed tentatively and operate from an understanding of the client situation and knowledge of health. They are not based on the nurse’s personal opinions or values.
Advising
Nurses are often in a position to offer sound advice about health matters. Like suggestions, advice is not based on personal opinions of the nurse, but rather on an understanding of the health event.
Challenges and pitfalls in advising
Giving personal opinions, for example, ‘If I were you, I’d put your mother in a nursing home’, must be avoided. When the nurse gives a personal opinion, it takes decision-making away from the client. It inhibits spontaneity, stalls problem-solving and creates doubt. Personal opinions differ from professional advice. At times, clients need suggestions and help to make choices. Suggestions are presented to clients as options because the final decision rests with the client. Remember, the problem and its solution belong to the other person and not the nurse. A much better response would be: ‘Let’s talk about what options are available for your mother’s care’.
Persuading
When advising and suggesting do not seem to be helpful to the client, a nurse often has to become persuasive in pursuing a therapeutic aim. For example, emergency-room nurses may need to persuade family members of a client who has died suddenly not to drive themselves home from the hospital while still in a state of shock at the death.
Focusing
Focusing is used to centre on key elements or concepts of a message. If conversation is vague or rambling or clients begin to repeat themselves, focusing is a useful technique. The nurse does not use focusing if it interrupts clients while discussing an important issue. Rather, the nurse uses focusing to guide the direction of conversation to important areas: ‘We’ve talked a lot about your medications, but let’s look more closely at the trouble you’re having in taking your tablets on time.’
Summarising
Summarising is a concise review of key aspects of an interaction. Summarising brings a sense of satisfaction and closure to an individual conversation and is especially helpful during the termination phase of a nurse–client relationship. By reviewing a conversation, participants focus on key issues and can add relevant information as needed. Beginning a new interaction by summarising a previous one helps the client recall topics discussed and shows the client that the nurse has analysed communication. Summarising also clarifies expectations, as in this example of a nurse manager who had been working with a dissatisfied employee: ‘You’ve told me a lot of things about why you don’t like this job and how unhappy you’ve been. We’ve also come up with some possible ways to make things better, and you’ve agreed to try some and let me know if any of them help.’
Self-disclosing
To use self-disclosure, the nurse reveals personal experiences, thoughts, ideas, values or feelings in the context of the relationship with the intent of helping the other person. This is not therapy for the nurse; rather, it shows clients that their experiences can be understood and are not unique. Self-disclosures should be relevant and appropriate and made to benefit the client rather than the nurse. They are used sparingly so that the client is the focus of the interaction: ‘That happened to me once, too. It was devastating, and I had to face some things about myself that I didn’t like. I went for counselling, and it really helped … What are your thoughts about seeing a counsellor?’
Confronting
To confront someone in a therapeutic way, the nurse helps the client to become aware of inconsistencies in his or her feelings, attitudes, beliefs and behaviours. This technique improves client self-awareness and helps the client recognise growth and deal with important issues. Confrontation should be used only after trust has been established, and it should be done gently, with sensitivity: ‘You say you’ve already decided what to do, yet you’re still talking a lot about your options.’
Encouraging
Like offering hope, nurses are often in a position to encourage clients, especially when discouragement is evident. Encouragement is best offered in concrete terms, such as ‘I can see that you are able to walk much better today. It only took you a few minutes to get to the toilet today. A few days ago it took nearly 20 minutes.’
Offering direct assistance
It may seem obvious that nurses assist clients. However, a direct offer of assistance can help when clients are overwhelmed with unpleasant feelings. ‘Here, let me help you with putting on your shoes’ is an example of direct assistance. In doing so, it is important that the nurse does not take over for clients and make them feel useless and more vulnerable.
Putting therapeutic communication techniques into action
The most critical aspect in determining which type of communication intervention to use is the intention of the nurse. For example, sharing observations such as ‘you look a bit worried to me’, is used with the intention of gaining more information about a particular aspect of the client’s wellbeing, while an open-ended question such as ‘how was your day yesterday?’ is employed to gain general information. The former leads clients to discuss something in particular while the latter allows clients to bring up whatever is most relevant to them about the topic. Therefore, choice of technique is dependent on the purpose and intention of the communication. Becoming skilled at using the technique that is appropriate to each situation requires a great deal of self-awareness and reflective practice.
Being reflective is the key to developing effective communication skills in nursing practice. This reflection occurs prior to communicating, for example, to consider the intention of the interaction with a client, and after interacting with a client to determine the degree to which that intention was met. Reflection after communicating enables nurses to consider whether they have been of assistance in helping the client, thus enabling them to develop insight into a situation, and to challenge themselves and change their perspectives (Asselin et al 2013, Bulman et al 2012). More than any other skill in nursing, the ability to communicate effectively is one that requires lifelong learning. And that learning will not be productive without reflection and self-awareness. This is especially true for those situations that are emotionally challenging (Rees 2013).
Emotional intelligence
In nursing, emotional intelligence is required for interpersonal competence (Powell et al 2015). This is because nursing care is delivered through interpersonal relationships which include making an emotional connection with clients (Stein-Parbury 2014). In providing nursing care, emotional responses are inherent, especially in relation to interacting with and building meaningful relationships with clients. Because of the nature of nursing work, these interactions and relationships can be filled with emotions (Dwyer & Hunter Revell 2015). It is for this reason that nurses need to be skilled in managing their emotions as well as understanding others’ emotions. This ability is termed ‘emotional intelligence’, which has been shown not only to improve the quality of nursing care (Adams & Iseler 2014) but also is associated with decreased stress in nurses (Görgens-Ekermans & Brand 2012). In addition, nurses who have a high degree of emotional intelligence are more likely to use collaboration in resolving conflict, while nurses with a low degree are more likely to use an accommodating response when faced with conflict (Morrison 2008).
According to Goleman (1998), who popularised the concept, there are five dimensions of emotional intelligence, which are both interdependent and hierarchical. The first is self-awareness, the basis of emotional intelligence, which involves the accurate assessment and knowledge of self in relation to others. Self awareness enables the regulation of emotions. Self-regulation does not mean that nurses do not experience emotions, but that these emotions do not become so intense as to render the nurse unable to function. With awareness and emotional regulation nurses are able to move to the third dimension – motivation – and engage meaningfully with others. Empathy, the fourth dimension, allows the nurse to understand others. Finally, emotional intelligence involves managing situations that require social skills, especially when dealing with conflict.
Conclusion
Nurses need to be skilled in the art of interpersonal communication in order to provide care that is truly person-centred. The purpose of communication in nursing is to understand the meanings that are conveyed by clients, their families and other healthcare colleagues. It is through understanding such meanings that effective relationships are formed. Effective means that they are helpful to clients and families, and collaborative with colleagues. Communicating with and relating to clients, their families and healthcare colleagues can be some of the most challenging aspects of nursing practice. Nonetheless, forming meaninful relationships with others has the potential to be one of the most rewarding aspects of being a nurse.
Online resources
Australian Institute for Patient and Family Centred Care is an organisation of patients, family members and healthcare professionals that promotes partnerships between patients, families and healthcare professionals. There are two videos of highlights of two healthplays ‘Hear Me’ and ‘Do you know me?’. They depict the importance of involving family and knowing the patient, http://www.aipfcc.org.au/
Communication for Health in Emergency Contexts (CHEC); an interactive learning resource that focuses on communication with patients in an emergency department, www.chec.meu.medicine.unimelb.edu.au
TeamStepps is a teamwork system designed to improve quality and safety in health care. An overall description of the program is found at http://teamstepps.ahrq.gov/about-2cl_3.htm. A pilot of the program conducted in South Australia can be found at www.safetyandquality.gov.au/wp-content/uploads/2012/03/TeamSTEPPS-Implementation-of-a-teamwork-programme-into-an-Australian-Setting-Public-Report-on-Pilot-Study.pdf