Assessment, management and prevention strategies for common wound types
Now that you have a better understanding of how to assess the skin and wounds, you are ready to learn more about assessing, managing and preventing conditions such as skin tears, leg ulcers, diabetic foot ulcers and pressure ulcers.
Acute wounds
Acute wounds are those that proceed through an orderly and timely reparative process to establish sustained anatomical and functional integrity (Franz et al 2008). Acute wounds are the most commonly encountered wound type, and healing of the acute wound is often taken for granted as it is expected to heal within a ‘normal’ wound-healing trajectory.
Acute surgical wounds healing by primary intention require minimal intervention apart from observation for complications as the wound edges are brought together (apposed) and then held in place by mechanical means (adhesive strips, staples or sutures). A wound dressing may be required in the first 24–48 hours postoperatively to protect the wound from physical or pathogenic invasion, to absorb exudate and to maintain wound temperature. Most incisions closed by primary intention are resurfaced within 2–3 days after surgery. A healing ridge is often palpable approximately 5–9 days after surgical incision; this is an area of induration beneath the skin extending to about 1 cm on either side of the wound. Lack of the healing ridge may indicate dehiscence.
Closure of surgical wounds
Surgical wounds are closed with staples or sutures. Sutures are available in a variety of materials, including silk, steel, cotton, linen, wire, nylon and Dacron. Sutures come with or without sharp surgical needles attached. Sutures are placed within tissue layers in deep wounds and superficially as the final means of wound closure. The deeper sutures are usually an absorbable material that disappears in several days. Sutures are foreign bodies and thus are capable of causing local inflammation. The surgeon can minimise tissue injury by using the finest suture possible and the smallest number necessary. Stainless-steel staples may also be used (Figure 26-16); these provide more strength than nylon or silk sutures and tends to cause less irritation to the skin.

Normally, for the first 2–3 days after surgery the skin around sutures or staples is swollen. Continued swelling may indicate that the closures are too tight. The skin can be cut by overly tight suture material, leading to wound separation. Sutures that are too tight are a common cause of wound dehiscence. Early suture removal reduces the formation of defects along the suture line and minimises chances of an unattractive scar formation.
Removal of wound closures
Policies vary within institutions as to who may remove sutures or staples, but usually a medical order is required. An order for suture removal is not written until the wound has closed (usually in 7–10 days). Usually, the number of sutures or staples to be removed is indicated. If the suture line appears to be healing in certain locations better than in others, only some sutures may be removed (e.g. every second one).
To remove staples, the tip of the staple remover is inserted under each wire staple and then squeezed, freeing the staple from the skin (Figure 26-17).

To remove sutures, the type of suturing used must first be identified (Figure 26-18). With intermittent suturing, the surgeon ties each individual suture made in the skin. Continuous suturing, as the name implies, is a series of sutures with only two knots, one at the beginning and one at the end of the suture line. Retention sutures are placed more deeply than skin sutures and may or may not be removed by the nurse, depending on agency policy. The manner in which the suture crosses and penetrates the skin determines the method for removal.
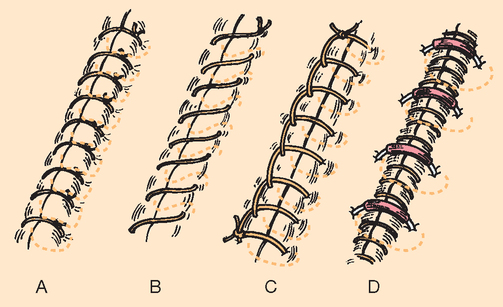
The most important principle in suture removal is never to pull the visible portion of a suture through underlying tissue. Sutures on the skin’s surface harbour microorganisms and debris; the portion of the suture beneath the skin is considered sterile. Pulling the contaminated (external) portion of the suture through tissues may lead to infection. The suture material is cut as close to the skin edge on one side as possible and then the suture is pulled through from the other end.
Every second suture or staple is removed first, and the wound edges are then inspected for healing. The remaining sutures or staples are removed if the wound edges have adhered.
Drains
Drains may be inserted into a surgical wound if a large amount of drainage is expected and if keeping wound layers closed is especially important. Some drains are sutured in place. Caution should be exercised when changing the dressing over drains that are not sutured in place to prevent their being accidentally removed. A drain such as a Penrose drain may lie under a dressing, extend through a dressing or be connected to a drainage bag or a suction apparatus. The surgeon often places a pin or clip through the drain to prevent it from slipping further into a wound. It is usually a medical responsibility to pull or advance the drain as drainage decreases to permit healing deep within the drain site.
The nurse assesses the number of drains, drain placement, the character of drainage and the condition of collecting apparatus. The security of the drain and its location with respect to the wound are observed, and the character of the drainage noted. If there is a collecting device, the drainage volume is measured. Because a drainage system must be patent, drainage flow through the tubing as well as around the tubing should be looked for. A sudden decrease in drainage through the tubing may indicate a blocked drain, and the surgeon should be notified. When a drain is connected to suction, the system is assessed to ensure that the pressure ordered is being exerted. Evacuator units such as a Hemovac or Jackson-Pratt exert a constant low pressure as long as the suction device (bladder or bag) is fully compressed. These types of drainage devices are often referred to as self-suction. When the evacuator device is unable to maintain a vacuum on its own, the surgeon is notified, who can then order a secondary vacuum system (such as wall suction). If fluid is allowed to accumulate within the tissues, wound healing will not progress at an optimal rate, and the risk of infection is increased.
When drainage interferes with healing, drainage evacuation can be achieved by using either a drain alone or a drainage tube with continuous suction. Barrier preparations must be applied to protect the skin surrounding drain sites: drainage then flows on the barrier but not directly on the skin. Drainage evacuators are convenient, portable units that connect to tubular drains lying in a wound bed and exert a safe, constant, low-pressure vacuum to remove and collect drainage. The nurse ensures that suction is exerted and connection points between the evacuator and tubing are intact. The evacuator collects drainage, which is assessed for volume and character every shift and as needed. When the evacuator fills, the output is measured by emptying the contents into a graduated cylinder and immediately resetting the evacuator to apply suction.
Skin grafts
Ideally, wounds heal by primary intention. However, large, surgically created wounds and traumatic and chronic wounds can cause extensive tissue destruction, making primary intention healing impossible. Skin grafts may then be necessary to protect underlying structures or to reconstruct areas for cosmetic or functional purposes. Survival of skin grafts relies on revascularisation of the grafted skin (Beldon 2007).
Skin-graft take is the process by which the donor site is incorporated into a recipient or host bed. Successful graft take requires an unhindered process of restoration of vascular perfusion to the donor skin. A graft will take better if the donor site, the area from where the skin is harvested, is highly vascularised.
For a skin graft to take, it must be closely applied to the recipient bed. Any accumulation of oedema, haematoma or seroma between the skin graft and the recipient bed will prevent the skin graft from taking. Movement between the graft and the recipient bed damages the in-growth of capillaries and prevents revascularisation. When skin grafts are applied to movable body parts, splinting is used to immobilise adjacent joints. Bed rest and positioning of the patient to prevent distortion or tension and shearing forces between the graft and the wound bed is essential. Tie-over dressings that immobilise skin grafts, particularly on the face, may be sufficient to immobilise problematic areas.
Several methods are used to fixate the graft, including the open method, the closed method and topical negative pressure wound therapy. The open method is where the graft is laid onto the recipient site and left open to the air. Initially, the graft is pricked every hour with a sterile needle to express any seroma or haematoma that has built up under the graft. As the wound exudate decreases, the procedure is reduced to every few hours. The closed method of skin grafting is where a pressure dressing is applied over the skin to keep it well approximated to the recipient bed (Terrill 2003). There are many different techniques to achieve this; most involve using a non-adherent dressing on the surface of the graft, such as tulle gras or paraffin-impregnated gauze, and a stack of cotton gauze cut to fit within the defect or a foam sutured/stapled onto the wound margins or a flexible polyamide net coated with soft silicone against the graft with a secondary absorbent dressing secured with sutures or staples (Terrill 2003, Young and Fowler 1998). Sutures or staples are not used if the skin graft is applied in the operating theatre. The fibrin that forms between the skin graft and the recipient bed binds the two surfaces together.
Topical negative-pressure wound therapy is utilised for skin grafts in complex anatomical areas where the base is irregular (Banwell & Teot 2003). A topical negative-pressure dressing achieves good apposition of the skin graft to the recipient site, absorbs exudate, reduces oedema, stimulates the formation of granulation tissue and decreases bacterial colonisation (Banwell & Teot 2003). Excellent graft take (> 95%) has been reported in the literature with this technique for graft fixation (Banwell & Teot 2003).
With the closed or topical negative-pressure wound therapy techniques, the skin grafts are usually reviewed after 5 days and assessed for graft take. A graft that has taken has a purple–pink hue and has adhered to the wound bed. The graft usually needs protection for at least 2 weeks or 3 months if located on the lower limbs. Any graft that has not taken is dressed using normal moist wound-healing principles. After 4–6 weeks, the graft is usually pale pink and the skin depression should be filling in. Further cosmetic improvement can continue with graft maturation over 6–12 months. Cosmesis can be improved using pressure therapy and silicone gel sheeting to soften scars and reduce erythema.
Skin flaps have their own blood supply, and the ability to monitor the status of the flap perfusion or its viability is essential in the prevention, recognition and treatment of complications. A healthy skin flap is similar in colour and texture to the donor site. The colour, temperature, capillary refill time, tissue turgor, dermal bleeding and quantity of exudate are techniques used to assess tissue flap viability.
Donor sites are frequently painful. Factors that affect the healing rate of donor sites are the site, size and depth of tissue excised (Beldon 2007). Healing of donor sites is primarily through re-epithelialisation of the exposed dermis. The sites tend to produce moderate amounts of exudate, and epithelial cells in the hair follicles, sebaceous and sweat glands migrate across the wound bed to form a new layer of epithelium. This process takes approximately 10–21 days. The ideal donor-site dressing should be easy to apply, reduce pain, minimise leakage of exudate, promote rapid wound healing and be inexpensive and acceptable to the patient (Beldon 2007).
Skin tears
A skin tear is a traumatic injury to the skin that occurs as a result of friction alone, or shearing and friction. It separates the epidermis from the dermis (known as a partial-thickness wound) or separates both the epidermis and the dermis from the underlying structures (known as a full-thickness wound). Most skin tears occur on the arms and hands. Other common sites are the lower legs, feet or the head, although they can occur anywhere on the body. Skin tears are the most common type of wound in older people, so it is important to understand why this is so and to be able to identify those most at risk. Most skin tears occur when the person accidentally bumps into an object such as a wheelchair or furniture when being transferred, or following a fall.
There are many risk factors for skin tears. These are explained in Table 26-12.
TABLE 26-12
Risk factors for skin tears
| Risk factor | Explanation |
| History of previous skin tears | If an older person has had one skin tear, they are more likely to have another one because their skin is more fragile. |
| Presence of bruising or discoloured skin (i.e. ecchymosis) | Skin that is bruised or discoloured is likely to tear more easily. This is because the dermis is thinner and there is less connective tissue to support blood vessels. It then takes very little trauma to cause a tear in the skin. |
| Advanced age | With an increase in age, the skin becomes thinner and less elastic because of reduced collagen and elastic fibre production. Collagen provides the strength and structure to the skin. When the skin of an older person is put under pressure, such as when the person is being moved, the small force applied to the skin can cause the layers of the skin to separate or tear apart resulting in a skin flap with jagged edges. |
| Poor nutritional status | Older people are more likely to be malnourished and dehydrated because of reduced oral intake or other health conditions. Dehydrated skin is less elastic, more fragile and more likely to break down. |
| Cognitive impairment or dementia | Lack of awareness of the environment may mean that the person is more likely to bump into an object, resulting in a skin tear. |
| Dependency | Patients who are dependent (i.e. require care for all activities of daily living) are at greatest risk for skin tears. They tend to acquire frequent skin tears from the mechanical trauma involved from the routine activities of bathing, dressing, positioning and transferring. |
| Multiple medications | Some medications that make the blood less likely to clot (e.g. anticoagulants) or steroids (e.g. taken for conditions such as rheumatoid arthritis) make the skin thinner and more likely to tear. |
| Presence of friction or shearing | Dry skin is more likely to tear due to friction and shearing. |
| Impaired mobility | Poor mobility means that the person is more likely to fall and sustain a skin tear. |
| Disease processes | Illnesses such as renal failure, heart failure, a cerebral vascular accident and diabetes increase a person’s risk of suffering a skin tear because of the way these diseases affect all body systems. |
Classification of skin tears
Skin tears vary in size, location and the amount of tissue loss. It is important that you know how to classify the type of skin tear so that you can determine the appropriate management options.
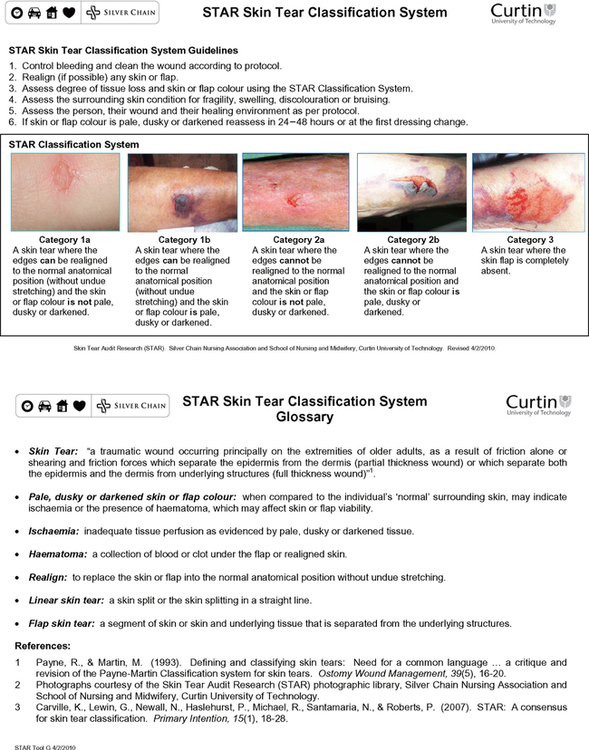
The STAR Skin Tear Classification System (see Figure 26-19) was developed by the Silver Chain Nursing Association and the Curtin University of Technology (2007) to provide an evidence-based consensus on skin tear classification. This means that if you use this system, you are more likely to be able to identify the type of skin tear and be able to select the correct treatment and prevention strategies. Skill 26-3 explains the assessment and management of a skin tear.
SKILL 26-3 Assessment, management and prevention of skin tears
The management and prevention of skin tears can be undertaken by all healthcare professionals. Check organisational policies regarding which wound care interventions can be delegated to health workers. The assessment of a person with or at risk of skin tears requires the problem-solving and knowledge-application skills of a registered nurse.
Therapeutic relationship and patient considerations
• Initiates communication by introductions and clarification of patient’s immediate needs and problems
• Identifies how the skill will affect the patient
• Discusses procedure with the patient to clarify understanding
• Assesses patient knowledge and expectations and ensures patient understanding
• Where necessary, provides further clarification
• Explains actions and potential discomfort at all stages of procedure
| STEPS | RATIONALE |
|
1. Explain procedure to patient. |
Decreases anxiety. |
| Helps to plan for type and amount of supplies required. | |
| Ensures easy disposal of soiled dressings. | |
| Protects nurse from splashes and reduces risk of transfer of infection between patients. | |
| The aim of wound cleansing is to remove both organic and inorganic debris from the wound and periwound skin to facilitate wound healing, and to make wound assessment easier so that the size and extent of the wound can be visualised. | |
|
7. Realign (if possible) any skin or flap.
a. Carefully realign by rolling the skin flap with a moist, sterile cotton bud. The use of a moistened cotton bud assists with approximation of the flap edge.
|
|
|
8. Assess the degree of tissue loss and skin or flap colour:
a. Using the STAR Skin Tear Classification System (see Figure 26-19), select the skin tear category that best describes the type of skin tear you are treating.
|
Provides a combination of subjective and objective data to assess effectiveness of wound management plan and to plan appropriate interventions. |
| A person’s overall medical condition may affect how quickly the wound is likely to heal. This will guide the management and preventive strategies you decide to use. | |
| • Ensure the dressing extends over the wound edge by at least 1.5–2 cm. | Reduces the risk of trauma on removal of the dressing and increases the ability of the dressing to absorb any leakage from the wound. |
|
• Before applying the dressing, draw arrows on top of the dressing with a felt pen to indicate the direction of the skin flap and write the due date for removal. When removing the dressing, ensure that you remove it in the direction of the arrow to avoid pulling back the skin flap. • Leave in place for 5–7 days. Change earlier only if there is 75% leakage on the dressing. • Reapply a new dressing if healing is not established and leave the dressing intact for 5–7 days. • If the wound is healed, leave it open and moisturise twice daily with a pH-neutral emollient. |
|
| Provides relevant information about the patient and the wound, monitors healing process, guides wound management of the person as a whole, evaluates the success of management and fulfils legal requirements. | |
|
14. Monitor the healing of the wound: a. Check the dressing and surrounding skin regularly for signs of complications or infection, but leave the dressing intact unless an inspection is clinically indicated. b. Educate the patient about the signs and symptoms of complications or infection. Advise them to report problems, especially any increase in pain, warmth, odour, redness, purulent exudate or fever. |
|
| 15. Implement skin-tear prevention strategies, including the following: | |
| • Assess and recognise risk. | People with fragile, thin, bruised or discoloured skin are at a high risk for further skin tears. |
|
• Use extreme caution and a gentle touch. • Avoid direct contact with the skin: use slide sheets where possible to reduce the risk of friction or shearing forces on the skin, especially when transferring someone. • Protect fragile skin: if a person has fragile skin or has had repeated skin tears, encourage them to wear long sleeves and long trousers to protect their skin. • Apply a pH-neutral moisturiser and/or barrier cream at least twice daily. This will help to prevent dry skin. • Use soap-free alternatives; avoid using soaps and perfumed lotions as these can dry the skin. Instead, use a pH-neutral cleanser or moisturiser. • Avoid using adhesives. Adhesives may increase the risk of tearing the skin when they are removed. It is advisable to use a limb protector instead. • Use protective padding on furniture and equipment: pad bed rails, wheelchair arms and leg supports to reduce the risk of skin injuries. • Ensure adequate lighting. A well-lit environment helps to reduce risk of people bumping into furniture, doors or equipment. |
Many skin tears occur when performing normal daily activities such as bathing, dressing and transferring individuals at risk. Avoid wearing jewellery or a watch. |
| 17. Document all relevant information in patient’s chart. | Provides relevant information about the patient and the wound, monitors healing process, guides wound management of the person as a whole, evaluates the success of management and fulfils legal requirements. |


Sinus
A sinus is a cavity or a track that extends from the skin surface to underlying tissue. A sinus may be the result of an infection, ulceration or necrosis of the dermis and underlying tissue, or a surgical wound dehiscence. The goal of management is to gently pack the sinus from the base upwards to eliminate dead space in the wound, prevent abscess formation and facilitate granulation tissue formation (Joanna Briggs Institute 2011).
Fistula
A fistula is an abnormal passage between two or more structures or spaces. This can involve a communication tract from one body cavity or organ to another organ or to the skin. The goal of management is the closure of the fistula, either spontaneously or surgically. Fistulae may be internal or external and are often associated with inflammatory diseases or a postoperative complication.
External fistulae may be the result of trauma, infection, malignancy, obstruction, surgery or radiation damage. Management of patients with a fistula requires complex, multidisciplinary care.
Burns
The initial assessment of a burn injury informs the plan of care. Burn injury assessment is notoriously difficult, and therefore access to specialist services for guidance to appropriate assessment, definition/classification and treatment is essential. Types of burn injury include damage to the skin caused by heat (thermal), chemical, electrical or radiation sources. Thermal burns are the most frequent type of burn; severity is related to temperature and duration of contact. Chemical burns are more likely to be full-thickness in depth and it may take several days for the severity of burn injury to develop or ‘declare’ the extent of tissue injury. The severity depends on the manner and duration of contact, the amount of skin and area of the body involved, the concentration of the chemical and how the incidence occurred. Electrical burn injury is most commonly caused by alternating current; severity is due to the voltage (force) and amperage (strength). Tissue injury occurs when electrical energy is converted to heat. Electrical burns have a point of entrance and exit, and the depth of injury can be difficult to determine.
Burn injury is classified according to the mechanism of injury, depth of injury and extent of total body surface area involved (see Table 26-13 and Figure 26-20).
TABLE 26-13
Classification of burn injury
| Classification | Degree of tissue loss |
| Superficial |
Involves the epidermis and is red in appearance with no blisters Usually heals within 7 days with no scarring |
| Superficial partial-thickness | |
| Deep partial-thickness | Extends into the reticular or deeper layer of the dermis and is dark pink in appearance with blisters present Usually takes 2–3 weeks to heal and grafting may be required; scarring may result |
| Full-thickness | |
| Subdermal |
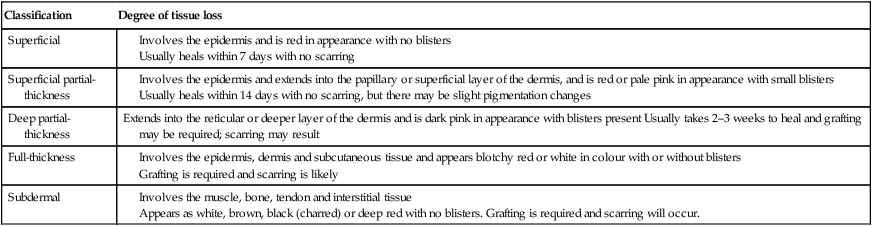
Carville K 2012 Wound care manual. Silver Chain Foundation, Osborne Park, WA.

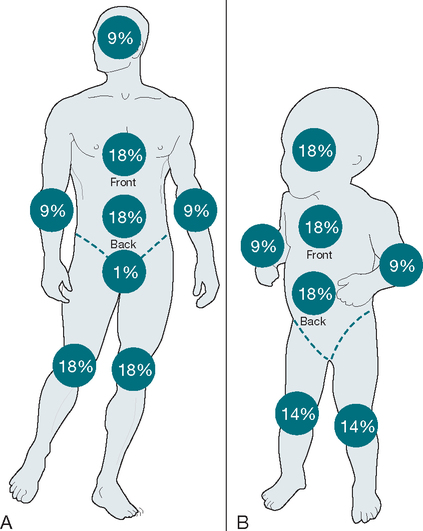
There are several techniques for assessing the amount of tissue damage in relation to total body surface area (TBSA), which is important for clinical management (Joanna Briggs Institute 2010). Wallace’s ‘rule of nines’ tool divides the body surface of adults into areas of 9% (or multiples of 9%), with the exception that the perineum is estimated at 1% (Figure 26-21). This allows the extent of the burn to be estimated with reproducible accuracy. Children have different body surface area (BSA) proportions, and the paediatric rule of nines is adjusted for age by taking 1% BSA from the head and adding 0.5% BSA to each leg for each year of life after 1 year of age, until age 10 years where adult proportions are reached.
Age-dependent burn graphs such as the Lund and Browder chart is the preferred method to estimate BSA burn, especially in children and neonates (Figure 26-22) (Joanna Briggs Institute 2010).
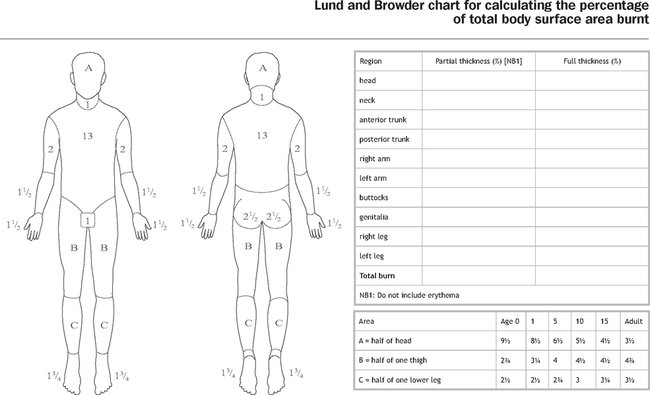
Small burns may be estimated using the area of the palmar surface (fingers and palm) of the patient’s hand, which approximates to 1% BSA.
Chronic wounds
In Australia, it is estimated that more than 433,000 people suffer from chronic wounds such as leg ulcers, pressure ulcers or non-healing surgical wounds at any one time, although the actual incidence is unknown as many people never seek treatment for their wound problems (Australian Institute of Health and Welfare 2008). Chronic wounds are frequently long-term, painful and debilitating, resulting in reduced quality of life for sufferers. They can affect people of any age, although prevalence increases with age and wounds are estimated to affect up to 5–10% of people aged over 80 years in Australia (ABS 2008). Studies on individuals with chronic leg ulcers reveal the average duration is approximately 1 year, 60–70% have recurrent ulcers and most people suffer from the condition for an average of 15 years or more (Araujo 2003, Bergqvist et al 1999, Lindholm et al 1992). Studies with residents in aged care facilities have reported that 25% suffer from a wound (ABS 2008).
Pressure injuries are considered to be largely preventable and yet they are a significant health problem. The prevalence of pressure ulcers in Australia in the acute care hospital setting ranges from 5.4% to 15.6% (AWMA 2001). Foot ulceration affects 15–20% of all individuals with diabetes and precedes up to 85% of amputations in this patient group, and is the most common cause of non-traumatic lower-limb amputation (Australian Centre for Diabetes Strategies 2005). The annual incidence of foot ulcers in people with diabetes is estimated to be 2.5–10.7% in Australia, Finland, the United Kingdom and the United States, and the average age for lower-limb amputation in Australia is 65–79 years (Australian Centre for Diabetes Strategies 2005). The 5-year recurrence rate for ulceration is 70%, and for those undergoing a lower-limb amputation there is a 50% chance of losing the remaining limb within 3 years (Australian Centre for Diabetes Strategies 2005).
Wounds commonly affect disadvantaged groups with the least resources to deal with the condition, such as the elderly, disabled and those in lower socioeconomic groups and with poor social support. Unfortunately, the burden of chronic wounds is rapidly growing globally (Harding 2010). In Australia, it is conservatively estimated that the problem of wounds costs the healthcare system more than $2.6 billion per year (Australian Institute of Health and Welfare 2008).
Assessment is the key to effective prevention and management of chronic wounds. Studies demonstrate that significant improvements in healing rates can occur when assessments are rationalised and based on research-based protocols (Carville & Smith 2004, Mulligan et al 2009). However, many patients have never been referred for specialist opinion despite suffering from ulceration for many years, and consequently may not have had the aetiology of the wound correctly diagnosed.
It must be recognised that there are many factors which need to be considered when caring for patients with or at risk of a chronic wound, including other long-term, chronic health conditions affecting many wound sufferers, and psychosocial and quality-of-life issues affecting many individuals.
Pressure injuries
Pressure ulcer, pressure sore, decubitus ulcer and bed sore are terms commonly used to describe pressure injuries. A pressure injury is an injury to the skin and/or underlying tissue, usually over a bony prominence. It occurs as a result of pressure alone, or pressure in combination with shear and/or friction.
Shearing forces usually occur as a result of sliding or dragging the skin across a support surface such as a mattress. Friction is the abrasion of the epithelial surface of the skin by rubbing against an abrasive or resistant surface. Friction may occur if the patient repeatedly rubs their heels on their mattress or on wheelchair foot plates. The presence of constant moisture from perspiration, urinary and/or faecal incontinence or wound leakage affects the ability of the skin to resist this type of damage.
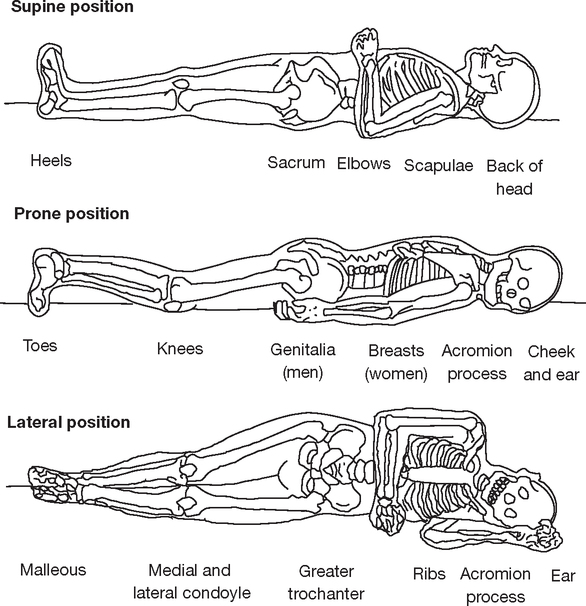
Pressure injuries can occur in any location, but are most commonly found on the sacrum or coccyx and heels. They may also occur on other bony prominences, including the ischium, toes, elbows, ears, ankles, nose or other areas of the body. All patients are at risk of developing a pressure injury. Table 26-14 reviews some key risk factors for the development of pressure injuries.
TABLE 26-14
Risk factors for pressure injuries
| Risk factor | Explanation |
| Alteration in mobility or physical activity | Reduced mobility or physical activity due to contractures, fractures, injury, neurological disease or pain increase the risk of pressure injury developing. This is because the patient is unable to independently reposition themselves to off-load or relieve pressure |
| Malnutrition and dehydration | Malnutrition and dehydration increase the risk of pressure injury. The skin is much drier and less able to withstand the effects of pressure damage |
| Moisture | The presence of constant moisture from wound leakage, urinary or faecal incontinence and perspiration increases the risk of pressure damage. This is because the skin is less able to resist friction or shearing forces |
| Alteration in sensation and consciousness | Decreased sensation or loss of consciousness because of cognitive impairment such as a central nervous system injury, a cerebrovascular accident, degeneration, major surgery, spinal cord injury or medications which increase the risk of pressure damage. This is because the patient may not be aware that an injury to the skin has occurred |
| Other health conditions | Health conditions such as heart disease, diabetes, circulation disorders and a history of smoking can increase the risk of pressure injury |
Pressure is the major cause of tissue injury and is related to the intensity and duration of pressure and the ability of the tissue to tolerate pressure. Sustained pressure on a localised area of tissue results in occlusion of blood flow to the vascular and lymph vessels that supply oxygen and nutrients to the tissues. This results in tissue ischaemia and reperfusion injury, leading to cell destruction and tissue death (Queensland Health 2009).
The likelihood of developing a pressure injury is dependent on a number of factors which affect tissue tolerance (see Table 26-12). The intensity and duration of pressure in combination with other risk factors determine a patient’s capacity to tolerate pressure (Queensland Health 2009).
Stages of pressure injuries
Pressure injuries are staged to help determine how severe the damage to the skin and underlying tissue structures might be. The Pan Pacific clinical practice guidelines for the prevention and management of pressure injury (AWMA 2012) recommend the use of a pressure injury classification system to provide a consistent and accurate means by which the severity of a pressure injury can be communicated and documented. Presently there are four stages of pressure damage. The higher the stage, the deeper the tissue involvement.
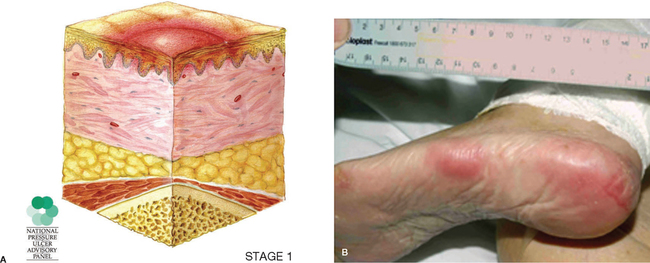
STAGE 1 pressure injuries present as areas of persistent, non-blanchable redness when compared with the surrounding skin. The skin around the wound may be painful or itchy, firm or boggy, and warmer or cooler to the touch when compared to the surrounding skin.
Stage 1 pressure injury may be difficult to detect in individuals with dark skin tones. In lighter skin-toned individuals, if you press on the skin for a few seconds, normal skin typically goes white in colour (blanching) and then returns to a normal pink colour when the pressure is released. However, patients with more darkly pigmented skin may not have visible blanching and skin colour may differ from the surrounding area. This means that when you press on the skin, changes in skin colour are difficult to detect.
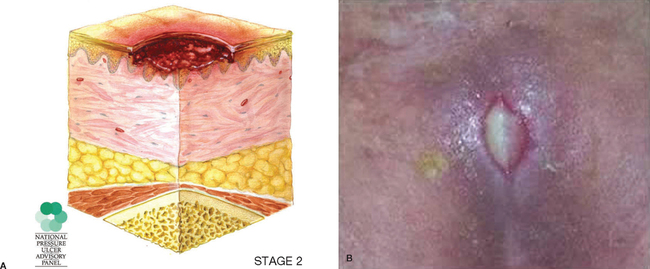
STAGE 2 pressure injuries represent a partial-thickness loss of the dermis, and present as shallow open ulcers with a red or pink wound bed; they may also present as an intact or open/ruptured fluid-filled blister. If a blister is found with clear fluid present and the epidermis is clearly separated from the dermis, this is recorded as a Stage 2 pressure injury.
STAGE 2 pressure injuries present as shiny or dry shallow ulcers without any bruising present, since bruising represents suspected deep-tissue damage.
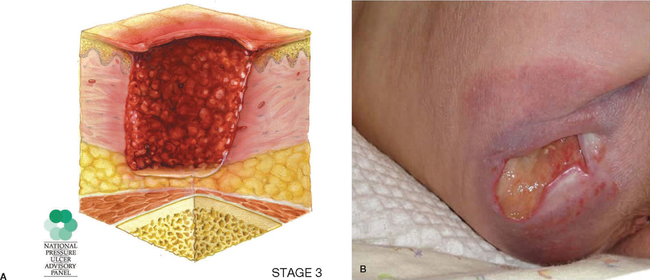
STAGE 3 pressure injuries represent full-thickness skin loss. Subcutaneous fat may be visible, but bone, tendons or muscle are not exposed. Thick yellow tissue (slough) may be present, but this does not obscure the depth of tissue loss. There may be undermining and tunnelling of the wound (i.e. the wound is deeper than it appears on the surface of the skin).
The depth of a Stage 3 pressure injury varies depending on where it is located anatomically. A pressure injury on the bridge of the nose, ear, scalp and ankle does not have subcutaneous tissue and Stage 3 pressure injuries can be shallow. In contrast, areas of significant adiposity or fatty tissue can develop extremely deep Stage 3 pressure injuries, although bone and/or tendon is not visible or directly palpable.
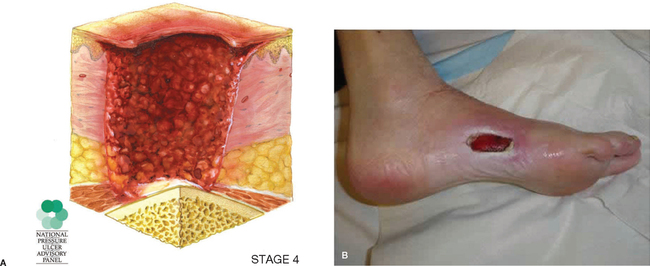
STAGE 4 pressure injuries are the most severe and represent full-thickness tissue loss with exposed bone, tendon or muscle. Thick yellow tissue (slough) or black necrotic tissue may be present in some parts of the wound bed. Often there is undermining and tunnelling of the adjacent tissue.
The depth of a Stage 4 pressure injury varies by anatomical location. The bridge of the nose, ear, scalp and ankles do not have subcutaneous tissue, so ulcers in these locations can be shallow. Stage 4 pressure injuries can extend into muscle and/or supporting structures (e.g. fascia, tendon or joint capsule), making osteomyelitis (infection in the bone) possible. Exposed bone/tendon is visible or directly palpable.
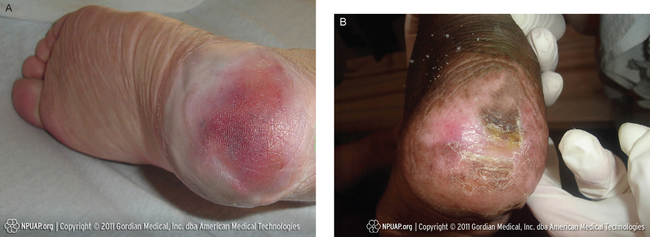
In addition to the above stages of pressure injuries, there are two other categories of tissue damage. Suspected deep tissue injury presents as purple or maroon discoloured intact skin or a blood-filled blister due to damage of the underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, or warmer or cooler as compared with adjacent tissue.
Deep-tissue injury may be difficult to detect in individuals with dark skin tones. The tissue injury may develop into a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Changes may develop rapidly, exposing additional layers of tissue, even with optimal treatment.
Unstageable pressure injuries present as full-thickness tissue loss in which the base of the wound is covered by thick yellow, tan, grey, green or brown tissue and/or eschar (tan, brown or black) in the wound bed. Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore stage, cannot be determined. Stable (i.e. dry, adherent, intact without erythema/redness) eschar on the heels serves as ‘the body’s natural (biological) cover’ and should not be removed.
There are limitations to the staging system for pressure injuries, including the following:
• Reactive hyperaemia may be mistaken for a Stage 1 pressure injury. The presence of non-blanching erythema requires the patient to be repositioned off the area of redness and reassessed in 26 minutes before diagnosing a Stage 1 pressure injury (Queensland Health 2009).
• Stage 1 pressure injury can be difficult to identify in patients with dark-coloured skin (see Figure 26-29).
• Necrotic tissue (eschar or slough) can conceal the extent of tissue injury, so should be debrided where possible to stage the degree of pressure injury correctly and then be reclassified once debridement has occurred.
• Reverse staging of a healing injury is not generally acceptable.
• The progress of pressure injury healing should be documented using objective parameters such as size, depth, amount of necrotic tissue, the amount of exudate and presence of granulation and epithelial tissue.
• The staging system depends on visual observation of tissue involvement. Factors such as location, wound dimensions, description of wound bed, edge of the wound, condition of periwound skin, pain and other factors which may delay wound healing should also be assessed (Australian Wound Management Association 2012).


Sites of pressure injuries
All parts of the body are at risk of pressure injury. The most common sites are those over bony prominences, as shown in Figure 26-30.
Risk assessment
In order to identify patients at risk of pressure injury, patients must all be screened for risk using an acceptable pressure ulcer risk assessment tool, on admission and regularly throughout their episode of care (Queensland Health 2009). Pressure ulcer risk assessment tools have been developed to assist in the identification and assessment of patients at risk for pressure injury. Examples of risk assessment tools include the Waterlow, Braden and Norton tools (copies of each of these tools are available from the Australian Wound Management Association guidelines; see Online resources). Risk assessment tools commonly use a rating scale to weight the severity of risk as no risk, low, medium or high risk (Queensland Health 2009). Risk assessment tools also commonly address risk factors such as mobility, nutritional status, sensory impairment, the level of consciousness, neurological status and incontinence (Queensland Health 2009). The presence of any condition that limits mobility to the point where a patient is unable to move independently or change position to relieve pressure means that the patient is automatically ‘at risk’.
Skill 26-4 demonstrates how to perform an assessment to identify patients at risk of pressure injury; this risk assessment is part of the admission process and ongoing preventative management for each patient (AWMA 2012).
SKILL 26-4 Assessment for risk of pressure injury
The management and prevention of pressure injuries can be undertaken by all healthcare professionals. Check organisational policies regarding which wound care interventions can be delegated to health workers. The assessment of a person at risk for or with a pressure injury requires the problem-solving and knowledge-application skills of a registered nurse.
Therapeutic relationship and patient considerations
• Initiates communication by introductions and clarification of patient’s immediate needs and problems
• Identifies how the skill will affect the patient
• Discusses procedure with the patient to clarify understanding
• Assesses patient knowledge and expectations and ensures patient understanding
• Where necessary, provides further clarification
• Explains actions and potential discomfort at all stages of procedure
| STEPS | RATIONALE |
|
1. A comprehensive risk assessment for pressure injuries should be completed on admission for every patient using a risk assessment tool. Reassessment should be performed at the following intervals:
|
|
|
• Alteration in sensation and consciousness – Central nervous system injury – Degenerative neurological disease Record the patient’s level of risk (no risk/at risk/high risk/very high risk) on the risk assessment chart, patient’s care plan and in the medical record. |
|
| 3. Skin assessment includes: | |
| Ensures privacy and patient comfort. | |
| Reduces anxiety. | |
|
c. Begin assessment with questioning and inspection to identify any existing wounds (refer to Table 26-4). |
|
|
e. Conduct a head-to-toe skin assessment with particular focus on skin covering bony prominences, e.g. sacrum, heels and greater trochanters (hips). Inspection involves observation of the skin and palpation with hands to detect the presence of moisture and colour changes and temperature differences in areas of the skin being inspected. |
|
| Check parts of the body covered by anti-embolic stockings, areas of the body where pressure, friction and shearing is exerted in the course of daily activities and other areas affected by equipment, footwear and clothing, i.e. skin around or under prosthetics, orthotics, skin traction, oxygen appliances, intravenous access, tapes and other objects in contact with the skin. | Many different types of medical devices have been reported as having caused pressure injury. |
| Look for the following characteristics:
• Reactive hyperaemia: when a red mark is found, relieve the pressure, check for blanching (the skin whitens under light finger pressure, which indicates the microcirculation is intact). Review in 26 minutes and the redness should have faded substantially. If the skin does not blanch or the hyperaemia (redness) does not fade, then a stage 1 pressure injury has been identified. |
Localised heat, oedema or induration (hardness), especially in darkly pigmented individuals, are early warning signs for pressure injury development. |
| A number of studies have identified pain as a major factor for patients with pressure injuries, and pain over the site is a precursor to tissue breakdown. | |
| 4. Reposition patient comfortably following procedure. | Promotes patient comfort. |
| 5. Document all skin assessments using a validated risk assessment tool. | Documentation and communication allows for the timely intervention of preventive and therapeutic measures. This minimises the frequency of occurrence and the severity of pressure damage. |
| 6. If evidence of pressure damage is noted, implement appropriate pressure off-loading and management strategies. | Timely implementation of pressure off-loading and management strategies is essential. Patients identified at risk for or with a pressure injury benefit from pressure off-loading strategies and a pressure injury prevention plan to reduce the risk of further tissue damage. |
| 7. Document all relevant information in patient’s chart. | Provides relevant information about the patient and the wound, monitors healing process, guides wound management of the person as a whole, evaluates the success of management and fulfils legal requirements. |


An assessment to determine risk for pressure injury should be performed (Queensland Health 2009):
• on admission to the healthcare facility and regularly throughout the length of stay or episode of care. For patients in acute care, it is recommended that assessment is performed on admission and at least every 24 hours, or sooner if a patient’s condition changes. In long-term care, assessment should be performed on admission, weekly for 4 weeks, and then quarterly and whenever the patient’s condition changes. Patients in the community should be assessed on admission and at every nurse visit
• following any changes in a patient’s condition that places that person at risk, for example, a sudden deterioration in health condition
• prior to, during and following prolonged procedures which involve reduced mobility and hardened surfaces.
All patients identified at risk of developing a pressure injury should have a comprehensive preventative management plan in place which aims to maintain tissue tolerance to pressure and protect the individual against the forces of pressure, shear and friction.
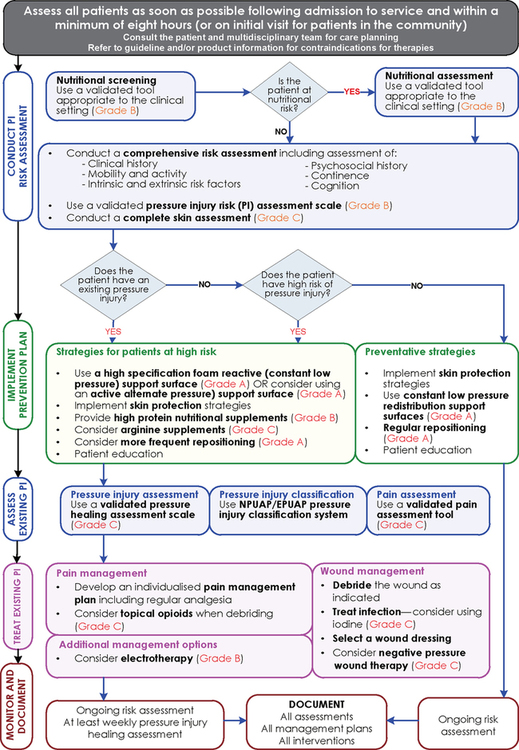
Prevention strategies
The Australian Wound Management Association (AWMA 2012) has recently released clinical guidelines to guide clinicians in identifying patients at risk and in selecting appropriate preventive interventions (see Figure 26-31). These guidelines are freely available online (see Online resources).
BOX 26-2 The Braden Scale for predicting pressure sore risk

© Barbara Braden and Nancy Bergstrom 1988. Reprinted with permission. All rights reserved.
There are many strategies that can be implemented to prevent pressure injuries.
• Maintain regular skin inspections every day and with each repositioning or turn for signs of pressure injury. On inspection, particular attention should be given to skin over bony prominences, for example, the sacral area, heels and greater trochanters, areas of the body where pressure, friction and shearing is exerted during normal daily activities and areas affected by equipment, footwear and clothing.
• Skin hygiene should be maintained to preserve skin integrity. The normal pH of the skin is between 4 and 6.8; maintaining a stable skin pH reduces the risk of infection and skin breakdown. Use of soap-free, pH-neutral cleansers and emollients keep the skin in better condition. Skin that is dry is less likely to be able to withstand the effects of friction and shear. Providing a stable environmental temperature and avoiding extremes of hot and cold decreases the risk of pressure injuries. Limit the patient’s exposure to moisture. Ensure limited or no exposure to excessive moisture such as perspiration, urinary and/or faecal incontinence or wound fluid.
• Avoid rubbing or massaging bony prominences. Massaging or rubbing bony prominences increases the risk of tissue damage. Pillows and foam wedges can be used to reduce pressure on bony prominences if positioned correctly. Avoid using foam rings or donuts, as these increase the risk of pressure damage by pushing or forcing the tissue through a narrow opening. Discourage patients from sitting or lying in one position. Repositioning should occur every 15 to 60 minutes if possible. Use positioning and turning schedules where possible, and consider the patient’s medical condition, comfort and overall plan of care as well as the support surface used.
• Prevent shear and friction. Elevate the foot of the bed 20 degrees when sitting to prevent the patient from sliding; also, limit the amount of time patients spend with the head of the bed elevated. Use of correct manual handling techniques, including slide sheets or equipment to transfer patients, reduces the risk of friction and shear.
• Monitor the patient’s nutrition and hydration. Refer to a dietitian if you are concerned about the patient’s nutritional status.
Working as part of a team is important to ensure that appropriate pressure ulcer-prevention strategies are implemented. Your team includes the patient, family members, general practitioner, nurses, care staff and allied health professionals. Education of the patient, family members and other healthcare professionals is essential so that they understand the causes of skin damage.
Support surfaces
The optimal support surface is one that relieves pressure, shear and friction and maintains a stable skin temperature (AWMA 2012). Support surfaces should distribute bodyweight over a large surface area or totally remove pressure from the body surface, thereby reducing point pressure and tissue damage. Support surfaces alone do not eliminate the risk of pressure injury, as pressure injury prevention requires comprehensive clinical care, regular repositioning and ongoing assessment.
There are many support surfaces available, such as mattresses, overlays or chair cushions, made up of a variety of different fabrics, including foam, gel or air. Comfort equipment includes overlays, pads, cushions and sheepskins; these are mostly used for comfort and in combination with existing mattresses or chairs that a patient is using. They may provide a degree of pressure reduction and reduce shearing and friction because of their low-resistance or non-abrasive properties. Comfort devices are suitable for low-risk patients who are relatively mobile and require minimal intervention.
Constant low-pressure devices conform to body contours and aim to redistribute weight over a wider area, thereby reducing tissue interface pressure (AWMA 2012). These devices include foam- or fibre-filled mattresses and overlays, water beds, gel pads, air overlays and mattresses with both static/constant air and low-air-loss devices (AWMA 2012). These devices may be powered, mechanical devices or non-powered, non-mechanical devices. Constant low-pressure devices may be appropriate for medium-risk patients who are able to reposition themselves or who receive frequent repositioning.
Alternating-pressure devices generate alternating high and low pressure between the body and the support surface by periodically deflating air cells under the body and redistributing the pressure on the tissue, which encourages reperfusion of previously supported areas (Queensland Health 2009). These devices are available as overlays or single or multi-layered mattress replacements. They are suitable for high-risk patients who are immobile or obese.
Specialty beds combine a bed and sleeping surface and are designed for patients at very high risk for pressure injury.
Pressure injury prevention and management requires a collaborative approach. The patient’s risk status and risk factors provide the basis for the formation of an individualised prevention and management plan. The management plan should provide specific details of what care is required, who is responsible for that care, frequency of turning, equipment required, referrals and expected outcomes (AWMA 2012). Clinical interventions must be monitored regularly and documented and communicated to staff, patients, families and carers.

Ulcers
Leg ulcers
A leg ulcer is a wound that occurs between the knee and ankle which takes more than 4 weeks to heal. There are two common types of leg ulcers: venous and arterial leg ulcers. Assessment is the key to effective management of leg ulcers, yet many people with leg ulcers have never had a specialist assessment to identify the type of leg ulcer they are suffering from. Hence, leg ulcers may last for many years and, even if they heal, may soon break out again if the correct treatment and prevention strategies have not been followed.
Every leg ulcer has key features or characteristics that help determine the type of leg ulcer the person is suffering from. The key characteristics for the most common types of leg ulcers are outlined in Table 26-17 on p. 740.
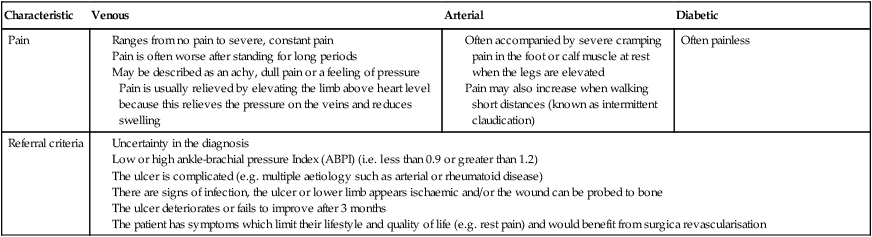
TABLE 26-17
Characteristics of leg ulcers















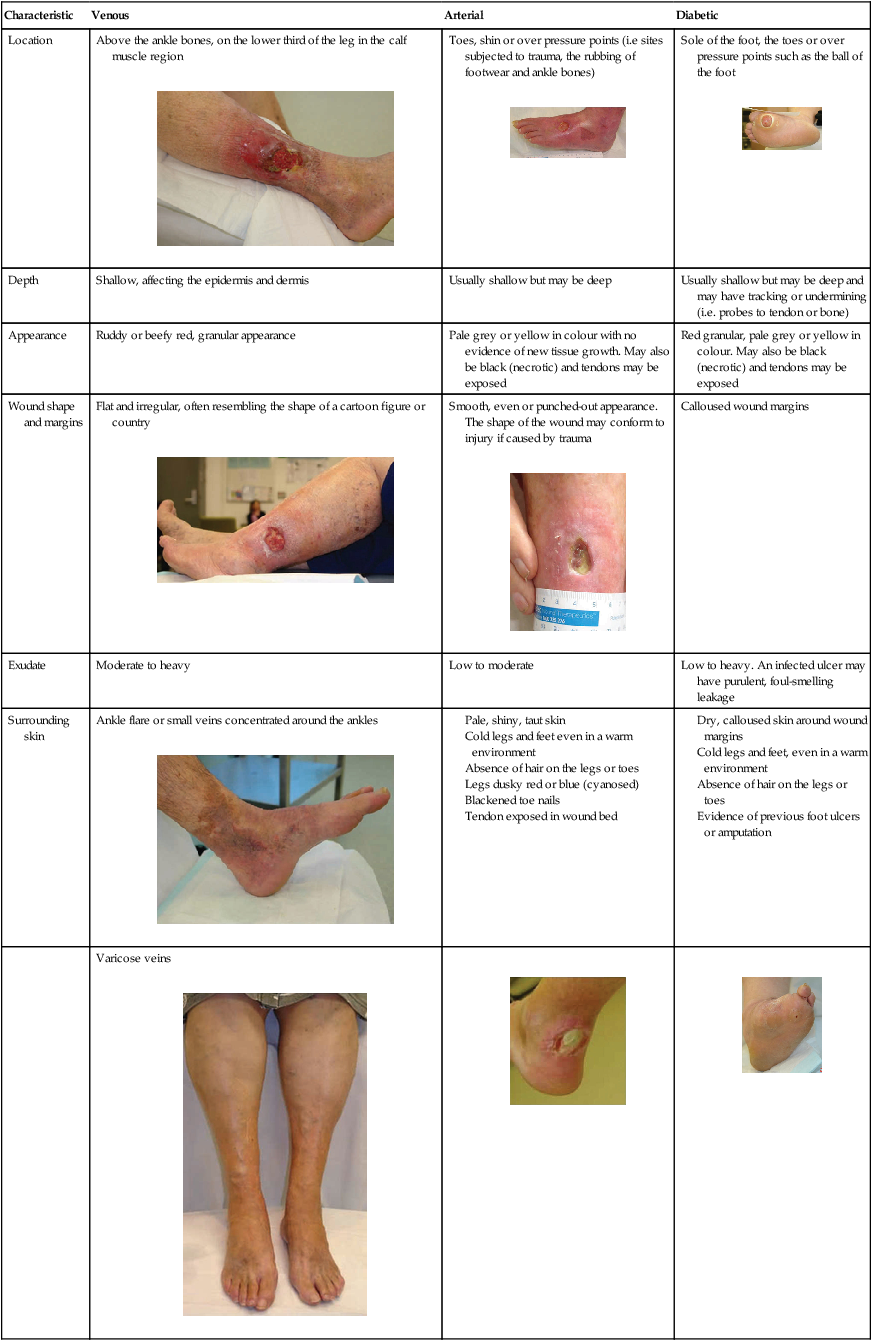
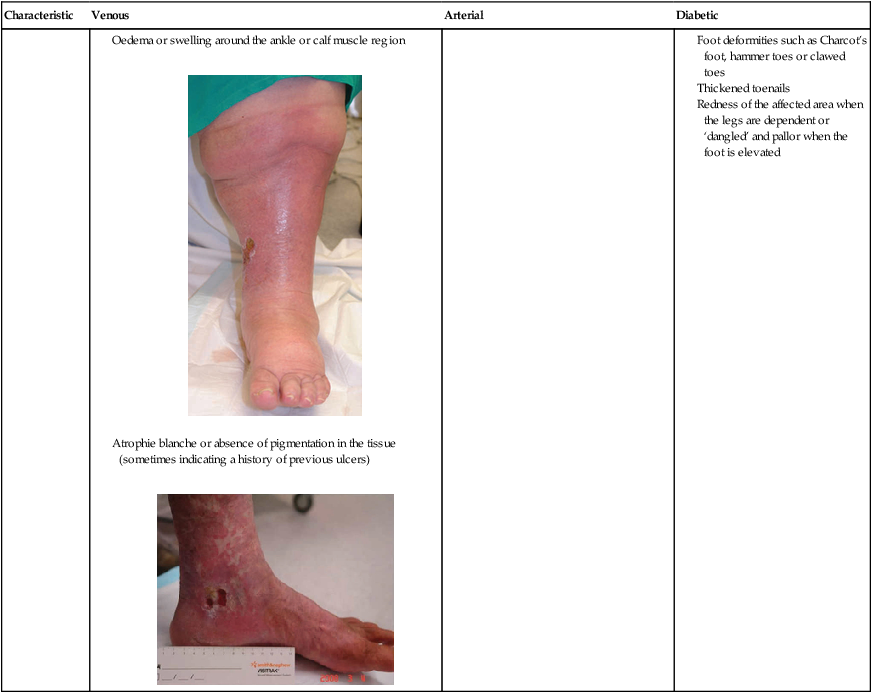
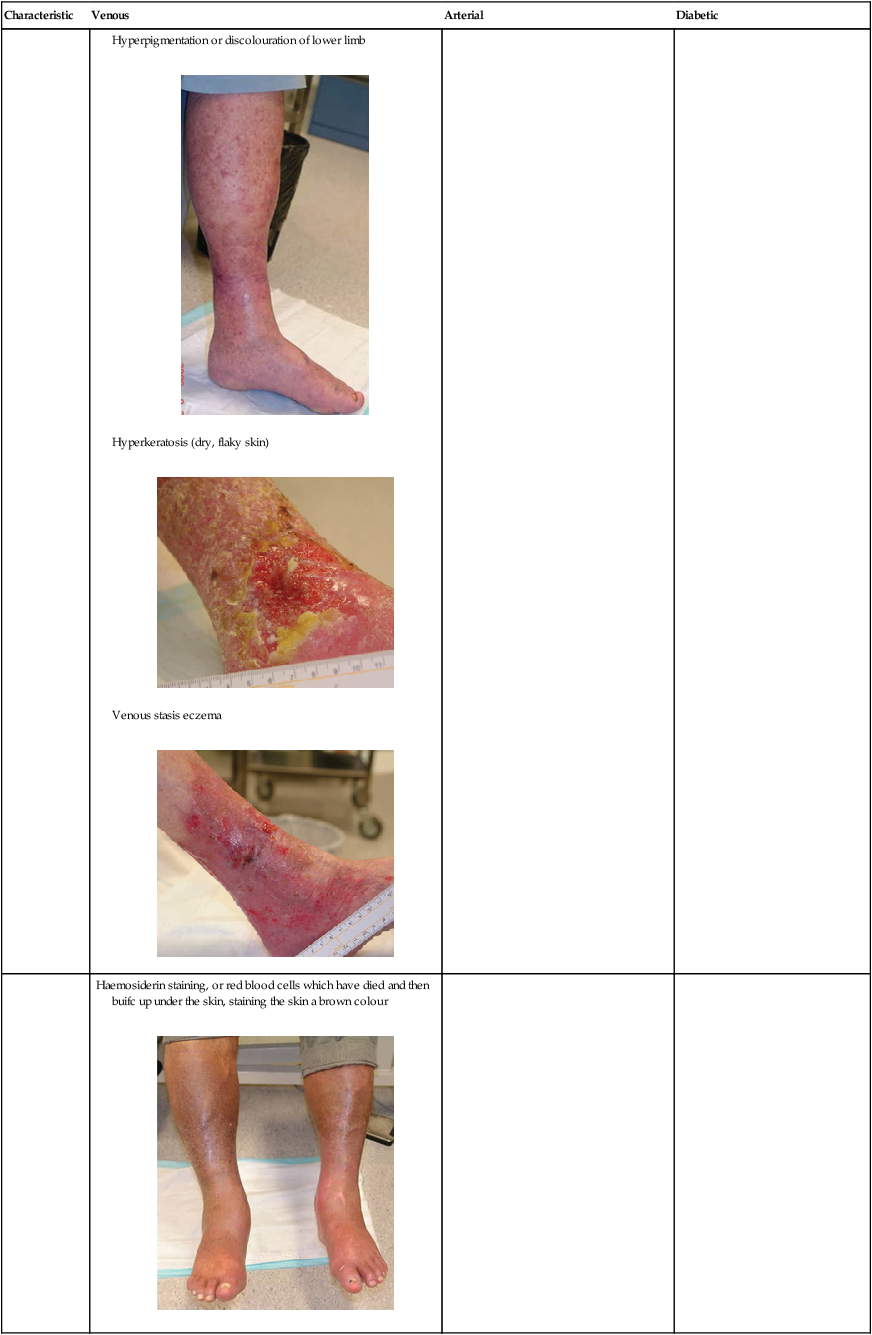
VENOUS LEG ULCERS are the most common type of leg ulcer. They occur because of high blood pressure in the veins in the lower limb (known as venous hypertension). Veins carry blood from the legs back to the heart. Veins in the lower leg have one-way valves to prevent blood from running backwards, and when the calf muscles contract, blood is moved along the veins back towards the heart.
However, sometimes the valves in the veins or the calf muscles fail to work properly, for a number of different reasons (e.g. damage from a past clot in the vein), leading to chronic venous insufficiency or venous disease. The constant high pressure in the veins eventually causes fluid to leak out of the veins and into the surrounding tissues and skin. Although the reason for ulcer formation is not fully understood, the combination of high pressure in the veins and particles in the fluid forced into the tissues causes inflammation. This results in the skin easily breaking down and forming an ulcer. Table 26-15 highlights some of the risk factors for venous leg ulcers.
TABLE 26-15
Risk factors for venous leg ulcers
| Risk factor | Explanation |
| Age | Blood flow decreases as a person ages, and decreased mobility leads to the calf muscles becoming less effective and not being used as much as they should be |
| Obesity | Excess weight, particularly around the waist and thighs, puts extra pressure on the veins and they have to work harder to move blood flow back towards the heart. Note that multiple pregnancies may also be a cause of excess weight |
| Varicose veins | The one-way valves that stop blood from travelling backwards in the veins stop working and this leads to pooling of blood in the lower legs |
| Past deep-vein thrombosis or trauma to lower limbs | A history of deep-vein thrombosis (i.e. blood clot) or trauma may result in permanent damage to the veins |
| Jobs that involve sitting or standing for long periods of time | Occupations that involve sitting or standing for long periods of time may result in less-effective blood flow through the veins and pooling of blood in the lower legs |
| Family history or congenital valvular incompetence | There is a strong link between family history and leg ulcers. In addition, in rare cases some people are born with problems that affect their veins, placing them at higher risk of venous disease |
| Health conditions | Disorders such as congestive cardiac failure lead to swelling of the lower limbs because the heart is not able to process blood flow effectively |
Once you have identified the signs and symptoms of a venous leg ulcer, you then need to determine the appropriate treatment. Key evidence-based management strategies for venous leg ulcers are summarised here.
• Dressings used to treat venous leg ulcers vary depending on the condition of the ulcer and the goals of treatment. Dressings should maintain a moist wound-healing environment, manage wound leakage (exudate), protect the skin around the ulcer, be non-adherent to reduce trauma on removal, and be cost-effective, acceptable to the patient and able to be changed less often where possible.
• Apply graduated compression bandaging. The key to healing a venous leg ulcer is to treat the underlying cause (i.e. reduce the high blood pressure in the veins). Graduated compression bandaging works by improving venous return, reducing swelling in the lower limb and improving foot- and calf-muscle pump action. Bandages are applied from the base of the toes to just below the knee. The bandage is said to be graduated because the ankle is smaller than the calf. Therefore, the pressure exerted by the bandage at the ankle is higher than that applied at the calf. You need special training in how to apply graduated compression bandages correctly because if they are applied incorrectly they can cause signiicant damage to the patient’s circulation and may even make the ulceration worse.
• Apply compression stockings. Graduated compression stockings for life after wound healing help to prevent venous leg ulcers from recurring, because they continue to provide compression to treat the underlying cause of the leg ulcers (i.e. poor circulation). A venous leg ulcer is really a symptom of an underlying disease process. Compression stockings can also be used to prevent venous leg ulcers.
Failure to reach an accurate diagnosis and/or to recognise the signs and symptoms of venous disease may result in the unsafe application of the graduated compression bandaging.
ARTERIAL LEG ULCERS are less common than venous leg ulcers and are the result of peripheral arterial disease. Arteries supply blood and oxygen to the lower limbs; arterial leg ulcers result from inadequate blood supply and oxygen in the arteries. If the blood supply to the lower legs is poor, the leg is starved of oxygen and nutrients; the skin fails to function normally and an ulcer may develop. A patient with arterial disease may have very cool or cold feet, the skin may be pale, blue (cyanosed) or dusky red in colour and they may complain of pain in the foot or calf muscle. Pain is often worse at night when the lower leg is elevated in bed and pain is only relieved when the legs are lowered. During exercise, the muscles in the lower leg need more oxygen; when a person has arterial disease, the blood supply is decreased and pain occurs in the foot or calf muscle on exercising. This pain is known as intermittent claudication. Table 26-16 outlines the patient risk factors for developing arterial leg ulcers.
TABLE 26-16
Risk factors for arterial leg ulcers
| Risk factor | Explanation |
| Atherosclerosis | Hardening, narrowing or blockage of the arteries because fatty deposits (plaques) or cholesterol reduces blood supply to the lower leg |
| Smoking | Cigarette smoking is a well-known risk factor for atherosclerosis and heart disease |
| Hypertension | High blood pressure leads to hardening of the arteries |
| Diabetes | Poorly controlled diabetes leads to high cholesterol levels in the blood and increased the risk of hardening of the arteries. There is also an increased risk of strokes, heart disease and ulceration of the lower limbs |
| High cholesterol | High cholesterol is a major risk factor for hardening of the arteries |
| Stress | There is a link between high levels of stress and arterial disease |
| A history of heart disease, heart attack or stroke | These conditions increase the risk of further problems with the peripheral arteries |
| Obesity | Excess weight, particularly around the waist and thighs, puts extra pressure on the arteries and the heart has to work harder to move blood flow around the body |
Patients with arterial leg ulcers may benefit from a review by a specialist. This is because restoring blood flow by revascularisation is the intervention most likely to heal arterial leg ulcers.
Improving oxygenation of the wound environment promotes healing. Steps to improve oxygen supply to the tissues include avoidance of dehydration, cold, stress and pain. Dressings used to treat arterial leg ulcers vary depending on the condition of the ulcer and goals of the treatment. Topical antimicrobial dressings may be helpful to prevent infection.
Controlling risk factors known to affect the arteries is essential. For example, the healthcare professional should try to ensure that blood glucose levels are kept within normal ranges, blood pressure is controlled, cholesterol levels are reduced, medications are reviewed and the patient has a healthy and balanced diet, stops smoking and is encouraged to maintain a healthy weight relative to their height.
Diabetic foot ulcers
A diabetic foot ulcer is an ulcer located on the foot and is associated with a loss of protective sensation (neuropathy) and/or the presence of ischaemia in a patient with diabetes. Diabetic foot ulcers are more likely to occur if the patient has uncontrolled or prolonged high blood-sugar levels (hyperglycaemia).
Once you have identified the signs and symptoms of a diabetic foot ulcer, you then need to determine the correct treatment. Key evidence-based management strategies for diabetic foot ulcers may include the following:
• Recommend a medical review: patients with diabetic foot ulcers may benefit from review by a specialist.
• Use a team approach to care: care of diabetic foot ulcers should be undertaken by a multidisciplinary team including podiatrists, orthotists, wound-care specialists, the patient’s doctor, an endocrinologist, a dietitian and a diabetic educator.
• Ensure adequate oxygenation: improving oxygenation of the wound environment promotes healing. Steps to improve oxygen supply to the tissues include avoidance of dehydration, cold, stress and pain.
• Ensure off-loading of pressure points: it is essential to review the patient’s footwear and ensure that pressure is relieved. Otherwise, the wound will fail to heal. Areas of abnormal pressure distribution on the diabetic foot are usually located on the plantar aspect of the foot under the hallux, first and fifth metatarsal heads and under the heel (Grey et al 2006).
• Apply suitable dressings: dressings used to treat diabetic foot ulcers vary depending on the condition of the ulcer and goals of treatment. Topical antimicrobial dressings may be helpful at preventing infection.
• Control risk factors: controlling risk factors known to affect the arteries is essential. For example, try to ensure that blood glucose levels are kept within normal ranges, the blood pressure is controlled, cholesterol is reduced, medications are reviewed, and the patient has a healthy and balanced diet, stops smoking and is encouraged to maintain a healthy weight relative to their height.
Assessment and management
Being able to recognise the key signs and symptoms of the different types of ulcers is very important to help obtain an accurate diagnosis. The following steps may assist during clinical examinations to determine the aetiology of ulceration. Table 26-17 compares the key characteristics of venous, arterial and diabetic ulcers. Assessing these characteristics can assist you to determine the aetiology of ulceration.
Prevention strategies
Once you have learned how to assess and manage venous, arterial and diabetic foot ulcers, there are some important evidence-based strategies that can be put in place to reduce the risk of the ulcer recurring. Box 26-3 highlights some of the key prevention strategies.
Malignant/fungating wounds
Malignant fungating or cancerous wounds are those that affect people with cancer. Fortunately, they occur infrequently, but are typically described as a devastating, overwhelming and distressing experience (Alexander 2010). They are caused by the infiltration of the skin by a local tumour such as a squamous-cell carcinoma or melanoma; haematological malignancy such as cutaneous T-cell lymphoma; or metastatic spread from a primary tumour, for example, breast cancer where metastasis occurs along tissue planes, capillaries or lymph vessels (Adderley & Smith 2007, Naylor 2002). Lesions are characterised by a process of both ulcerative (crater-like) and proliferative (nodular or cauliflower-shaped) growth that can cause extensive damage to the skin and surrounding structures (Lewellyn et al 2002).
Although rare, malignant changes may develop in chronic wounds (Marjolin’s ulcer) and are most commonly associated with burn-scar ulcers, pressure or venous ulcers (Naylor 2002). This type of malignancy is usually aggressive and has a high rate of metastatic spread and local recurrence (Naylor 2002). Diagnosis can only be confirmed following biopsy of the wound, although signs of malignant change in a chronic wound are typically characterised by onset of pain or a change in the type or intensity of pain, malodour and change in character, volume or appearance of exudate.
Malignant wounds can have a significant impact on the patient and their family and greatly affect the quality of life. Wound management priorities vary considerably for each patient and strategies should be targeted according to the patient’s preferences. Most patients with a malignant wound will be in the terminal stages of their illness and wound healing is unlikely to occur. The main aim of wound management is aimed at controlling or eliminating the distressing symptoms associated with these wounds.
Malignant wounds often produce copious amounts of exudate, which can be difficult to manage (Naylor 2002). Exudate production is secondary to increased permeability of blood vessels in the tumour and secretion of vascular permeability factor by tumour cells, or increased exudate due to the presence of infection (Naylor 2002). High volumes of exudate may result in maceration and irritation of the skin. There are many dressings available for the management of exudate (e.g. foams and alginates), and selecting a dressing that will absorb exudate but still maintain a moist environment is essential (Adderley & Smith 2007).
An offensive malodour caused by bacterial infection and/or the presence of devitalised tissue within the wound bed is frequently the most distressing aspect of a malignant wound; it can be socially isolating and cause loss of appetite and nausea (Alexander 2010). Debridement of necrotic or devitalised tissue is the main method of treatment for malodorous fungating wounds (Naylor 2002). However, surgical sharp debridement is not recommended due to the high risk of bleeding; autolytic debridement is the preferred method of debridement (Naylor 2002). The use of antimicrobials (e.g. metronidazole gel) can help to reduce the amount of bacteria present in the wound, thereby reducing malodour. The use of topical activated-charcoal dressings and occlusive dressings may help to control odour, and environmental agents such as room deodorants and fragrances for control of odour may also assist (Carville 2007).
Bleeding can occur secondary to the erosion of blood vessels by malignant cells and may be exacerbated by decreased platelet function within the tumour (Naylor 2002). Profuse, spontaneous bleeding can be very distressing and careful management of the wound during dressing changes is essential to minimise the risk of bleeding. Preventative measures to reduce the risk of bleeding, such as the use of non-adherent dressings, maintaining a moist environment, haemostatic dressings (e.g. alginates or haemostatic sponges) and wound cleansing by irrigation, will help to reduce the risk of trauma and bleeding (Naylor 2002).
Pain is caused by a number of mechanisms, including pressure on nerves and blood vessels and exposure of the dermis (Naylor 2002). Pain frequently results in loss of sleep, distress and anxiety and may be exacerbated by wound-dressing changes. Pain should be assessed before, during and after wound-dressing changes and analgesia should be prescribed using the World Health Organization (WHO) guidelines (see Chapter 41) for the control of cancer pain and in accordance with local prescribing guidelines (Naylor 2002). The use of non-adherent dressings and dressings which maintain a moist environment may help to reduce pain associated with wound-dressing changes.
The position of the wound may be a significant source of distress for the patient, particularly if in a highly visible area such as the breast or face. Wound management strategies aimed at devising a cosmetically acceptable dressing may help to promote self-esteem and minimise distress.
The skin around the fungating wound is susceptible to breakdown and must be assessed for signs of bacterial infection, fungal infection, maceration and excoriation. The use of non-traumatic adhesives, skin sealants and creams or ointment barriers can help to provide protection to the periwound skin.
Palliative treatment may include radiotherapy and systemic or topical chemotherapy to reduce tumour size, exudate and malodour (Adderley & Smith 2007). Radiotherapy in the form of X-rays or radioactive substances is used as a localised cancer treatment or in combination with other treatments such as surgery or chemotherapy, and is used to reduce the size of a tumour, to control the spread of disease or to relieve symptoms of advanced disease (Regan 2007). Radiotherapy is unable to differentiate between normal and abnormal cancer cells, and the radiation can damage healthy tissue and may result in skin atrophy, soft-tissue fibrosis and microvascular damage or burn injury (Regan 2007). Skin reactions to radiotherapy typically occur 2 weeks into treatment; the likelihood of developing a reaction depends on a number of factors including the patient’s age, skin integrity, type of radiation and amount of energy used, chemical and skin irritants used by the patient, nutritional status, presence of skin folds and concurrent chemotherapy (Regan 2007). Skin reactions may be mild such as dry skin or may lead to moist desquamation.
Strategies that can be taken to minimise the effects of radiation include preventing mechanical trauma caused by shaving, friction, pressure, adhesive tapes or constrictive clothing; avoiding the use of chemical trauma from soaps, deodorants, shaving creams, astringents or make-up; avoiding extremes of heat and cold to prevent thermal trauma; avoiding skin products that contain metallic substances, including zinc cream and talcum powder; avoiding exposure to the sun; moisturising the skin frequently with a pH-neutral emollient; and ensuring adequate nutrition and hydration (Carville 2007).
Chemotherapy may be used to reduce the size of a malignant wound; it involves the use of systemic or localised cytotoxic drugs (Regan 2007). Chemotherapy can cause skin reactions including transient erythema, hyperpigmentation, photosensitivity, nail changes, palmar/plantar syndrome and inflammatory reactions in tissue that has been previously irradiated, resulting in blisters, vesicle formation, exfoliation and ulceration (Regan 2007). Chemotherapy can decrease the size of a malignant wound by destroying malignant cells, and reduce pressure on nerves and blood or lymph vessels, thereby reducing exudate production and potential to bleed (Regan 2007).
Extravasation of the skin can occur secondary to the use of chemotherapy drugs, resulting in ulceration of the skin, nerve damage, significant pain, disfigurement and potential limb loss (Regan 2007). Extravasation occurs over a few days with maximum severity over 2–3 weeks. The degree of tissue damage is secondary to the amount of drug extravasated, drug concentration, site, needle insertion device and technique (Regan 2007). The affected tissue may appear swollen, tender and red and progressively worsen into ulceration, and may involve tendons and nerves. Severe tissue damage may require surgical intervention (Regan 2007). Prevention of extravasation injuries includes a thorough assessment of the patient, venous access, related risk factors, knowledge of the drug and early recognition of the signs of extravasation injury including burning pain, erythema and oedema at injection site.
Malignant fungating wounds are a significant problem and are challenging for both patients and healthcare professionals. The key to effective management is accurate assessment to improve quality of life through symptom control; however, there is insufficient evidence to provide clear direction for practice with regard to improving quality of life or managing wound symptoms associated with fungating wounds (Adderley & Smith 2007, Lo et al 2008, 2012).
Adjunct wound therapies
Hyperbaric oxygen therapy (HBOT) is a treatment designed to increase the supply of oxygen to wounds that are not responding to other measures to treat them. HBOT involves people breathing pure oxygen in a specially designed chamber (such as that used for deep-sea divers suffering pressure problems after resurfacing). Evidence suggests that HBOT seems to reduce the number of major amputations in people with diabetes who have chronic foot ulcers, and may reduce the size of wounds caused by venous disease, but at this stage there is no evidence to confirm or refute any effect on other wounds caused by lack of blood supply due to arterial disease or pressure injury (Goldman 2009, Kaur et al 2012, Kranke et al 2004).
Online resources
Australian Wound Management Association provides a number of important clinical guidelines such as the Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers and The Pan Pacific clinical practice guideline for the prevention and management of pressure injury, www.awma.com.au/publications/publications.php
STAR Skin Tear Classification System, www.silverchain.org.au/shared-content/assets/documents/research-publications/star-skin-tear-tool-04022010-pdf.pdf/view