Nystagmus in childhood
Frank Antony Proudlock, Irene Gottlob
Introduction
Nystagmus consists of rhythmic ocular oscillations. Pathological nystagmus is involuntary, although it may be modulated when performing certain tasks such as reading. Infantile nystagmus is defined as nystagmus developing in the first 3–6 months of life. Nystagmus can be acquired later in life, usually due to neurological diseases. Patients with acquired nystagmus have oscillopsia, the illusion that the environment is moving. Patients with infantile nystagmus, however, usually have a stable view of the environment, probably due to neuronal plasticity and adaptation during visual development.
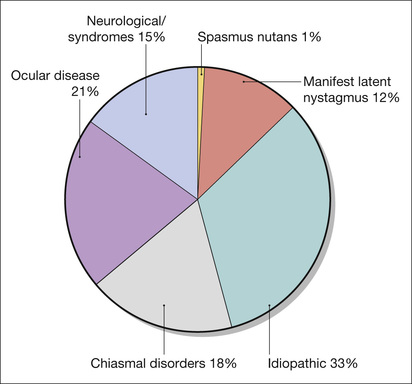
Nystagmus in childhood can be idiopathic or associated with retinal diseases, low vision in infancy, and a variety of syndromes and neurological diseases. Nystagmus associated with neurological disorders in childhood may be similar in appearance and pathophysiology to acquired nystagmus. Onset may also be after 6 months of age. The estimated prevalence of nystagmus (including both infantile and acquired nystagmus) is 24 in 10,000. The prevalence of infantile nystagmus is 14 per 10,000.1 Among the infantile forms of nystagmus, idiopathic nystagmus is the most common, followed by nystagmus associated with ocular disease. The clinical diagnoses associated with infantile nystagmus are shown in Figure 89.1.
Causes of infantile nystagmus
The causes of most forms of infantile nystagmus are as yet unknown, although this is currently an active field of research.2 In general, infantile nystagmus is considered to be a disorder of gaze-holding and slow eye movement systems,3 leading to sinusoidal oscillations and/or drifts of the eye away from the intended point of fixation. These involuntary slow eye movements constitute nystagmus slow phases. The slow phases are interrupted and shaped by the interposition of nystagmus quick phases, which serve to re-align the eyes.
Many types of infantile nystagmus are associated with the presence of sensory abnormalities during early visual development.4–9 With afferent diseases such as achromatopsia and congenital cataract, the nystagmus is clearly the result of changes in the otherwise healthy ocular motor systems in response to afferent deficits present during visual development. For other conditions such as albinism and various syndromes, it is uncertain whether the nystagmus is also due to afferent deficits or directly caused by abnormalities in ocular motor neural circuitry.
Quality of life and infantile nystagmus
Investigations into the quality of life of adults and children with infantile nystagmus show that the effects on visual function are considerable and are comparable to the effects of diseases such as age-related macular degeneration.10 Infantile nystagmus has a much wider impact than simply reducing vision. It affects social interaction, due to lack of confidence caused by the cosmetic appearance of nystagmus, and restriction in mobility of many patients, as they are not able to drive. Consequently, treatment of nystagmus should not only aim at improving visual acuity but also at improving cosmesis. This might include, for example, the correction of abnormal head postures and the reduction of nystagmus intensity in patients with poor visual potential. Patients may also benefit from counseling services and support groups such as Nystagmus Network, UK (http://www.nystagmusnet.org) or the American Nystagmus Network (http://www.nystagmus.org).
Classification of infantile nystagmus
There has been significant controversy over the classification and terminology used in nystagmus. This is because some researchers have been mainly interested in the morphology of nystagmus waveforms and others in clinical etiology.
The advantages of using a clinical classification of infantile nystagmus based on the associated diseases are that the clinical implications such as prognosis, possible genetic counseling, or treatment options are immediately highlighted.11 Figure 89.2 lists examples of disorders using this type of classification. Idiopathic nystagmus has historically been a diagnosis of exclusion where all other eye examinations are negative. The visual acuity is 0.3 LogMAR or better in most patients, suggesting relatively good retinal function.12,13 However, retinal abnormalities have been recently identified in idiopathic nystagmus using optical coherence tomography (OCT).6 Mutations in the FRMD7 gene have been identified as a major cause of X-linked idiopathic nystagmus.14,15 Several genetic mutations are known for other disorders such as albinism16,17 and achromatopsia.18 It is likely that the nystagmus genotype will be the principal method of classification in the future.

The Committee for the Classification of Eye Movement Abnormalities and Strabismus Workshop (CEMAS; http://nei.nih.gov/sites/default/files/nei-pdfs/cemas.pdf) have grouped together idiopathic nystagmus, nystagmus associated with ocular diseases, and nystagmus associated with chiasmal misrouting into one category called “infantile nystagmus syndrome.” In a clinical setting, this classification is less helpful and makes unconfirmed assumptions about a common mechanism leading to nystagmus in all of the underlying pathologies.
Terminology used in nystagmus
Nystagmus can be characterized by clinical examination of the patient. Eye movement recordings can help by providing greater precision in detecting and describing nystagmus waveforms, which can assist in the diagnosis (Figs 89.3 and 89.4). The following parameters can be used to describe nystagmus:
Plane: The plane of oscillation can be horizontal, vertical, torsional, or a combination of more than one plane (e.g. Fig. 89.3C2).
Intensity: The intensity of the nystagmus is a measure of the speed of the eye movements and is obtained by multiplying the nystagmus amplitude (in degrees) and frequency (oscillations per second in Hertz).
Waveform: Nystagmus can be broadly classified into jerk and pendular waveforms. Jerk nystagmus consists of alternating slow and quick phase eye movements. The nystagmus direction is defined using the quick phase. Slow phases can have an increasing velocity profiles where the eyes start slowly and accumulate speed (e.g. Fig. 89.4A in right gaze). Alternatively, slow phases may have decreasing velocity (e.g. Fig. 89.4C) or linear velocity profiles. In contrast, pendular nystagmus consists of approximately sinusoidal oscillations without quick phases (e.g. Fig. 89.4A at null region). Dual jerk nystagmus is a combination of large jerk nystagmus waveforms with small pendular nystagmus waveforms superimposed along the same plane.
Conjugacy: If both eyes move together, i.e. with the same amplitude, frequency and plane, the nystagmus is conjugate. Dysconjugacy or dissociated nystagmus occurs if the eyes move with different amplitude (e.g. torsional eye movements in Fig. 89.3A3), frequency, phase (e.g. vertical eye movements in Fig. 89.3C2) or along different planes.
Foveation: Most types of infantile nystagmus show periods in the nystagmus cycle when the eyes move at a slower velocity. These slow periods are often used to align the fovea with visual targets to improve visual acuity, and hence are called foveation periods.
Null region: Many patients with infantile nystagmus prefer a particular gaze direction where the nystagmus is reduced in intensity and visual acuity is optimal. This is called the null region. If the null region is not in the primary position, patients may adopt an abnormal head posture (AHP) using the null region to improve vision when looking straight ahead. An example is shown in Figure 89.4A2 where the null region is in right gaze.
Infantile nystagmus is not always uniform but can change depending on several factors:
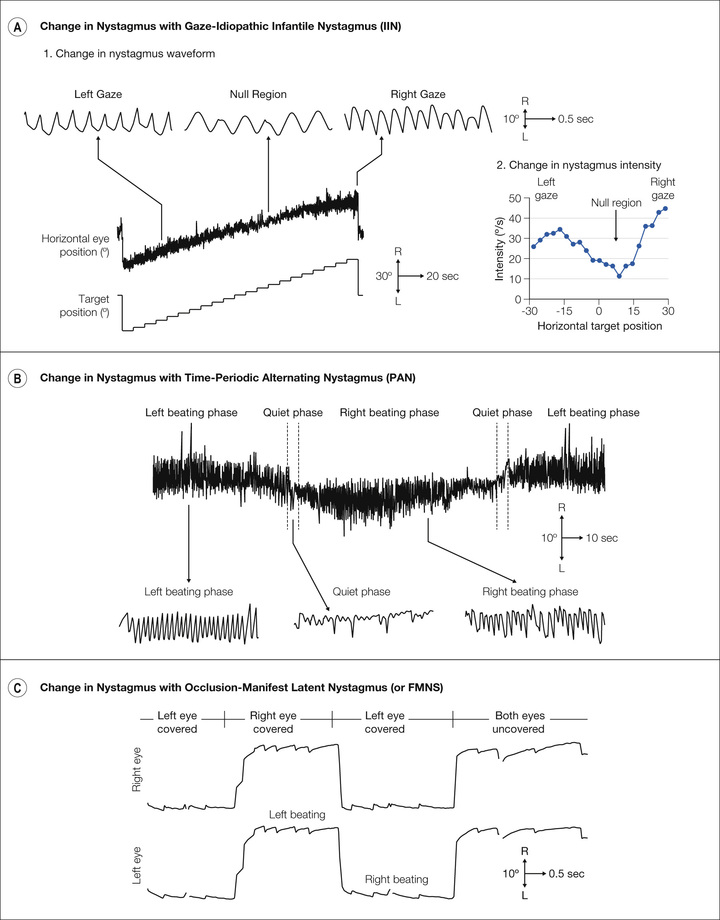
Change with gaze: Patients with nystagmus associated with albinism and idiopathic nystagmus usually have a null region. The nystagmus becomes more jerk-like (see Fig. 89.4A1) and intense (see Fig. 89.4A2) away from the null region.
Change with time: Most patients have a consistent oscillation when attempting to maintain a fixed gaze position. However, certain types of nystagmus vary with time. In periodic alternating nystagmus (PAN) the fast phase beats periodically to the right and to the left with quiet periods at the changeover periods (see Fig. 89.4B).
Change upon covering one eye: In manifest latent nystagmus (MLN), the fast phase of nystagmus changes direction beating towards the open or fixing eye (see Fig. 89.4C).
Clinical assessment
History
It is important to establish the time of onset for the nystagmus since infantile nystagmus occurs usually in the first 3, or sometimes 6, months of life.
As several forms of infantile nystagmus are hereditary, establishing whether other family members have nystagmus or associated ocular diseases can help with the diagnosis. If there is a positive family history, determining the mode of inheritance is very important. Idiopathic nystagmus often occurs in an X-linked pattern in which heterozygous females are fully affected in approximately 50% of cases (i.e. 50% penetrance).14,15 In contrast, only males are fully affected in X-linked congenital stationary night blindness (CSNB),19 blue cone monochromatism,18 or ocular albinism.17 Oculocutaneous albinism16 and achromatopsia18 are usually autosomal recessive. The most common form of autosomal dominant nystagmus is caused by mutation in PAX6 genes.20
Where neurological deficits such as cerebral palsy, metabolic diseases, or other causes of developmental delay are present, they are likely to play a key role in the etiology of the nystagmus.
It is important to establish whether parents think their child has poor vision. Although nystagmus can be of very large amplitude at onset and parents can have the impression that the child is visually unresponsive, usually the nystagmus amplitude is considerably smaller by 6–9 months of age.21 Explaining to parents that nystagmus generally changes and becomes less evident as their child becomes older is important, and therefore caution should be taken about predicting poor vision later in life.
Often children with nystagmus have head nodding or bobbing. This seems to be an independent abnormal head movement, which can decrease or disappear with age. Only in spasmus nutans has head nodding been shown to reduce or abolish nystagmus (Fig. 89.3D).
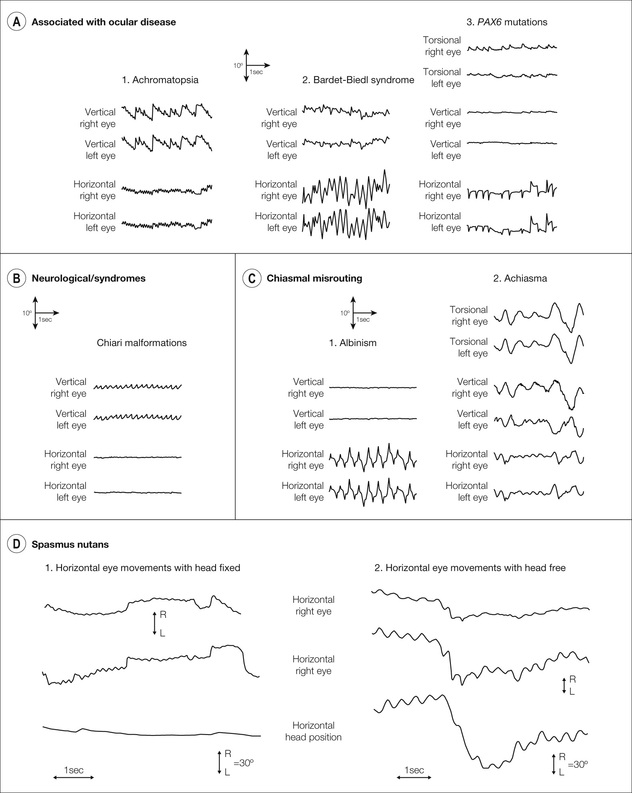
 Fig. 89.4A), nystagmus associated with albinism (C1) can have pendular or jerk waveforms but always along the horizontal plane and usually with a null region. Jerk waveforms can be left beating, right beating, or bidirectional as shown in example here. Achiasmatic disorders (C2) lead to seesaw nystagmus, so called because the eyes give the appearance of rotating around an invisible pivot positioned somewhere between the two eyes. Consequently, as one eye moves up, the other eye moves down, leading to a dysconjugate vertical waveform. The eye moving up intorts and the eye moving down extorts, leading to a large-amplitude torsional nystagmus. There is also a horizontal component to seesaw nystagmus. (D) Spasmus nutans: Nystagmus in spasmus nutans is altered by head movements. When the head is fixed, a rapid pendular oscillation develops, which is dysconjugate between the two eyes. When the head is free, head bobbing occurs with the eyes moving in the opposite direction due to the vestibulo-ocular reflex. This leads to suppression of the rapid oscillation. ([D] Reproduced from Gottlob I, Zubcov AA, Wizov SS, et al. Head nodding is compensatory in spasmus nutans. Ophthalmology 1992; 99: 1024–1031.)
Fig. 89.4A), nystagmus associated with albinism (C1) can have pendular or jerk waveforms but always along the horizontal plane and usually with a null region. Jerk waveforms can be left beating, right beating, or bidirectional as shown in example here. Achiasmatic disorders (C2) lead to seesaw nystagmus, so called because the eyes give the appearance of rotating around an invisible pivot positioned somewhere between the two eyes. Consequently, as one eye moves up, the other eye moves down, leading to a dysconjugate vertical waveform. The eye moving up intorts and the eye moving down extorts, leading to a large-amplitude torsional nystagmus. There is also a horizontal component to seesaw nystagmus. (D) Spasmus nutans: Nystagmus in spasmus nutans is altered by head movements. When the head is fixed, a rapid pendular oscillation develops, which is dysconjugate between the two eyes. When the head is free, head bobbing occurs with the eyes moving in the opposite direction due to the vestibulo-ocular reflex. This leads to suppression of the rapid oscillation. ([D] Reproduced from Gottlob I, Zubcov AA, Wizov SS, et al. Head nodding is compensatory in spasmus nutans. Ophthalmology 1992; 99: 1024–1031.)A history of photophobia should be specifically asked for. This would be indicative of a retinal disease, particularly achromatopsia or blue cone monochromatism. Similarly, a history of night blindness should be specifically asked for. This suggests a rod–cone dystrophy and is common in congenital stationary night blindness.
Symptoms of oscillopsia are a feature of acquired nystagmus and seldom occur in children. Some patients with infantile nystagmus, however, perceive oscillopsia if they look away from the null region22 or if the nystagmus changes, for example in manifest latent nystagmus (MLN), which can change with the degree of strabismus. The oscillopsia in acquired nystagmus is usually sudden in onset and severe. In contrast, the time of onset of oscillopsia in infantile nystagmus is generally not as well defined and the symptoms are milder.
Clinical examination
Visual acuity
Visual acuity (VA) needs to be examined with the best optical correction and tested with both eyes open and either eye covered with a free head position. This is important, as manifest latent nystagmus, alone or superimposed on other infantile nystagmus waveforms, can increase the nystagmus and decrease VA when one eye is covered. VA should also be measured at distance and near. In infants, VA tests can be performed using preferential looking cards. In patients with horizontal nystagmus, measurement of VA can be assisted by vertically aligning the cards,23 making it easier to identify changes in fixation when the child looks up or down at the visual targets on the card. This can be masked by the horizontal nystagmus if the card is aligned horizontally. The presence of vertical optokinetic nystagmus can also be used to predict the likelihood of better VA in horizontal nystagmus.
Abnormal head posture
Abnormal head posture (AHP) (or torticollis) occurs commonly in nystagmus because many patients can reduce their nystagmus by looking in a certain direction of gaze, for example by directing gaze towards the null region. In most patients, the full extent of torticollis is only observed during visual effort. So to identify the full amount of AHP, ask the patient to read or look at pictures (Fig. 89.5A). Glasses can prevent the patient adopting the full head turn due to the spectacle frame and optical decentration. VA measurements should be repeated, therefore, without spectacles. Figure 89.5B shows a child with idiopathic infantile nystagmus (IIN) and a right head turn increasing as he reads smaller letters. With a greater visual demand, a large head turn is adopted and he looks over his glasses or prefers to read without glasses since the full head turn is prevented by the glasses.

Manifest latent nystagmus dampens on adduction. As a result, the patient adopts a head turn to keep the fixing eye adducted (Fig. 89.5C). In manifest latent nystagmus, the head position also needs to be examined with each eye covered, as the head position can change depending on the fixing eye (Fig. 89.5D). Patients with “A” or “V” pattern strabismus may adopt a chin-up or -down head position in order to maintain binocular function and thus reduce the amplitude of the nystagmus (Fig. 89.5E). Eye movement recordings are helpful in understanding abnormal head postures, for example in establishing whether the head posture is due to idiopathic nystagmus (see Fig. 89.4A) or manifest latent waveforms (see Fig. 89.4C). They can also be used to determine whether the adopted head posture leads to a reduction or change in the nystagmus.
Orthoptic examination
Orthoptic examination should include an assessment of strabismus at distance and near, the range of motility of each eye, binocularity, stereopsis, and fusion ranges if binocular vision is present.
Color vision testing
This is important to detect achromatopsia and other retinal or optic nerve diseases.
Examination of light sensitivity and nyctalopia
Photophobia is easily noted on slit-lamp or fundus examination and points to achromatopsia or other retinal dystrophies. Nyctalopia can be objectively measured using dark adaptometry and indicates congenital stationary night blindness or other retinal dystrophies.
Structural examination
The most common abnormal sign of the anterior segment is iris transillumination, which is strongly associated with albinism. The amount of iris transillumination varies and can be easily missed on examination if it is mild, especially in patients with dark irides or in small children. Slit-lamp examination should be performed in a completely dark room with retroillumination. It is helpful to examine the parents also, as carriers commonly have mild iris transillumination. It is important to examine for corneal changes, aniridia, or abnormal iris structure and the presence of cataracts. The retina can appear normal in the early stages of retinal dystrophy. Foveal hypoplasia often manifests as a missing foveal reflex and abnormal vessels in the foveal area. This can be difficult to establish in a child with nystagmus. In retinal diseases such as achromatopsia and congenital stationary night blindness, the retina can appear normal. Optic nerve hypoplasia or atrophy can cause nystagmus, particularly if it is bilateral. Large refractive errors are also commonly a sign of retinal dystrophies, albinism, PAX6 mutations, or other diseases associated with low vision. Paradoxical pupillary response (initial pupillary constriction when the room light is turned off) can be a sign of retinal diseases.
Electrophysiology
Every patient with infantile nystagmus should have an electrophysiological examination. Hemispheric visual evoked potentials (VEPs) represent the gold standard examination for determining increased crossing of the optic nerves in albinism and reduced crossing in achiasma (see Chapters 41 and 57).
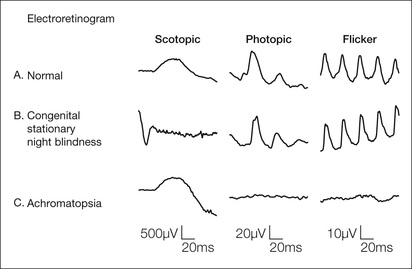
Electroretinography (ERG) is essential to investigate possible retinal dystrophies (Fig. 89.6).
Eye movement recordings
Eye movement recordings are very useful in clarifying the pathophysiology of the nystagmus, in differential diagnosis, and in planning surgery. Figures 89.3 and 89.4 show examples of eye movement recordings in each of the main classes of infantile nystagmus.
Nystagmus associated with albinism (see Fig. 89.3C1) or idiopathic nystagmus (see Fig. 89.4A) is conjugate, almost always horizontal, with a combination of pendular and jerk waveforms that vary with gaze.12 Away from the null region, the slow phases typically increase in velocity and drift towards the null region (see Fig. 89.4A). In contrast, nystagmus associated with manifest latent nystagmus usually has decreasing velocity slow phases (see Fig. 89.4C). Nystagmus waveforms associated with retinal diseases are variable and can be dissociated, vertical, and can have increasing or decreasing slow phase velocities (see Fig. 89.3A). Vertical nystagmus is also often associated with neurological disorders (see Fig. 89.3B).
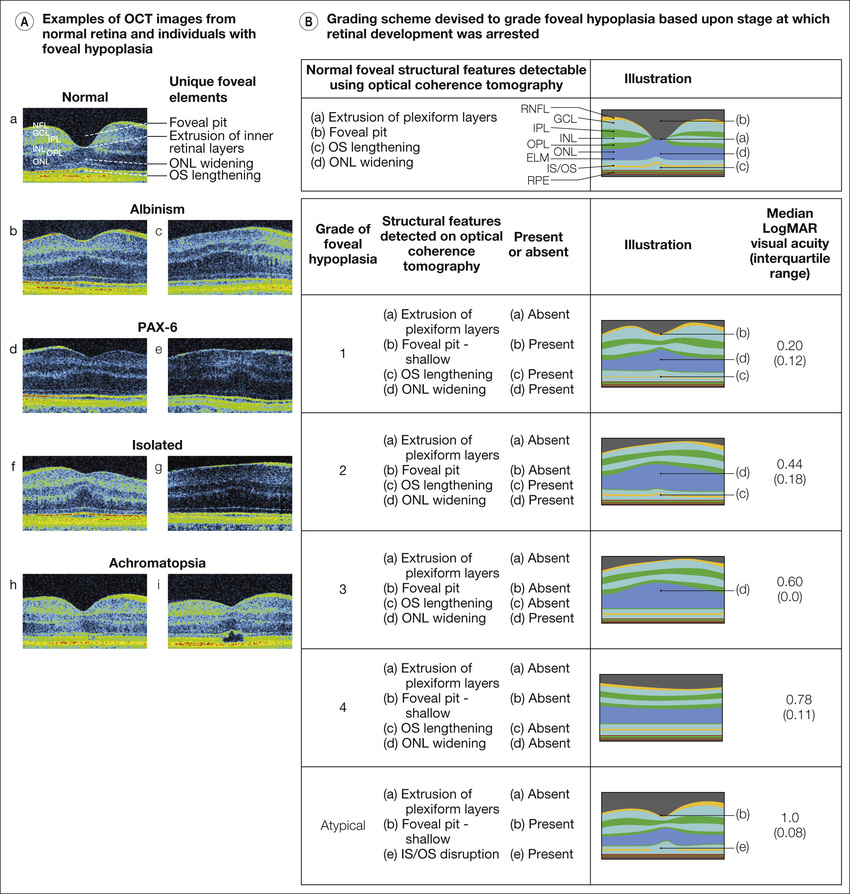
Optical coherence tomography
OCT has recently been added as a useful investigative tool for the differential diagnosis of nystagmus and can be performed easily and quickly.5–9 It is particularly helpful in identifying foveal hypoplasia and results can be obtained at the time of appointment. Figure 89.7 shows OCT images of a control subject and patients with albinism, idiopathic foveal hypoplasia, PAX6 mutation, and achromatopsia. If foveal hypoplasia is detected on OCT, the most likely diagnosis is albinism5; however, mutations in the PAX6 gene or idiopathic foveal hypoplasia cannot be ruled out.8 These diseases have similar morphological changes in the fovea. In contrast, foveal hypoplasia in achromatopsia is atypical.4,7,24 In many patients with achromatopsia, there is a pathological continuation of inner and outer plexiform layers. Typically, there is disruption of the inner segment/outer segment junction and cone outer segment tip, and thinning of the outer nuclear layer. The most striking sign is a “punched out” hyporeflexive zone, which often only appears in older patients. Morphological changes in achromatopsia appear to increase with age on OCT.4,7,24 Structural grading of foveal hypoplasia based on retinal imaging using OCT can be used to estimate VA (Fig. 89.7[2]).5,8
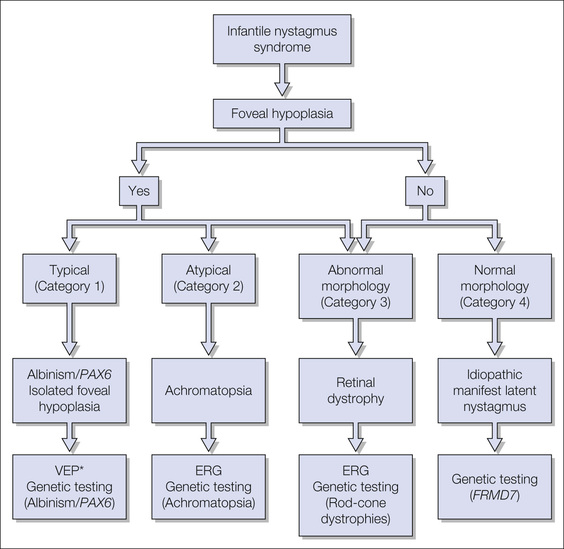
Hand-held OCT is also now available for use in infants and children, and can assist in diagnosing patients that are too young to comply with other diagnostic tests.25 Figure 89.8 shows a diagnostic algorithm for infantile nystagmus that has been developed for use in infants and children using hand-held OCT.
Magnetic resonance imaging of the brain
Magnetic resonance imaging (MRI) is necessary if the nystagmus is not typical of idiopathic nystagmus (i.e. dysconjugate, vertical, or oblique) and cannot be explained by ocular or systemic disease. MRI is generally not indicated when the associated disease (e.g. albinism, achromatopsia, or manifest latent nystagmus/infantile squint syndrome) has been determined and when no other neurological/developmental problem is present. Any suspicion of neurological disease, optic atrophy, optic nerve hypoplasia, or developmental delay should prompt neuroimaging. In the presence of optic nerve hypoplasia, investigation for septo-optic dysplasia (de Morsier syndrome) and hormone deficiency is important.
Clinical characteristics of infantile nystagmus types
Idiopathic infantile nystagmus
IIN has historically been diagnosed by exclusion of other ocular or neurological pathology. Anterior segment, fundus examination, VEPs and ERGs are normal. However, retinal abnormalities may be apparent on OCT imaging such as shallow foveal pits and smaller optic discs, cups, and retinal nerve fiber layer thickness.6 If the IIN is familiar, the most frequent inheritance mode is X-linked, where approximately 50% of female carriers are clinically affected.14,15 Autosomal dominant inheritance has also been described. Recently the first gene (FRMD7) in which mutations cause X-linked IIN has been found.14,15 Knockdown of FRMD7 during neuronal differentiation results in altered neurite function.26
Patients with IIN have a median VA of 6/9.5, strabismus is uncommon (less than 10%), and good stereoacuity is often present.13 Interestingly, patients with mutations in the FRMD7 gene often have less abnormal head postures compared to patients with IIN without mutations in this gene.13 Nystagmus is conjugate and usually horizontal, especially when associated with FRMD7 mutations (see Fig. 89.4A).13 Nystagmus waveforms in IIN have been described as having increasing velocity slow phases. However, the nystagmus is usually more complex, consisting of underlying pendular oscillations regularly interrupted by quick phases (see Fig. 89.4A). Increasing velocity slow phases are more apparent away from the null region.
Nystagmus waveforms are often of very large amplitude in the first few months of life but become smaller as children become older. Changes in waveform characteristics also occur, with more jerk waveforms becoming apparent with age.21 Possibly these are adaptive mechanisms to allow better vision through the development of foveation periods – periods where the eyes move at a relatively slower velocity. Typically, the nystagmus has a null region where nystagmus intensity is reduced, causing an abnormal head posture if the null region is not in the primary position of gaze (see Fig. 89.4A). Over 20% of patients with idiopathic nystagmus due to mutations in FRMD7 have PAN, but this is usually not detected clinically, only on eye movement recordings (see Fig. 89.4B).27 Albeit rare, IIN can be vertical.
Chiasmal misrouting
Albinism has very similar nystagmus characteristics to IIN (see Fig. 89.3A,C). The diagnosis of albinism can be easily missed and signs such as iris transillumination, hypopigmentation of the retina, optic nerve hypoplasia, and abnormal crossing on VEP need to be assessed carefully. OCT is very helpful in detecting foveal hypoplasia (see Fig. 89.7B,C). Albinism is discussed in detail in Chapter 41.
Patients with achiasmia have congenital seesaw nystagmus. The diagnosis is confirmed on MRI and VEP. Achiasma is discussed in detail in Chapter 57.
Nystagmus associated with ocular disease
Nystagmus can occur in most types of retinal dystrophy. The diagnosis of achromatopsia (Fig. 89.6) or blue cone monochromatism is likely in a patient with marked light sensitivity, poor vision, poor color discrimination in combination with a small-amplitude and high-frequency nystagmus. Inheritance is autosomal recessive in achromatopsia, and mutations in four genes have been described for which molecular genetic testing is available.18 Patients with mutations in the same gene can have widely varying phenotypes.18 This can range from profound visual impairment with no color vision, to incomplete achromatopsia with some color perception, and, less commonly, to oligocone trichromacy with almost normal color vision and visual acuity as good as 0.1 LogMAR.28 Patients with achromatopsia often have fast pendular nystagmus superimposed on jerk nystagmus, and also vertical nystagmus (see Fig. 89.3A1).29 Recently, atypical findings on OCT examination have been described in achromatopsia (see Fig. 89.7H,I).4,7,26 The diagnosis can be confirmed by extinguished or severely reduced photopic electroretinography (see Fig. 89.6C). In blue cone monochromatism, the VA is usually better and the inheritance is X-linked.18
Congenital stationary night blindness (CSNB) is often associated with nystagmus that can have waveforms corresponding to infantile or manifest latent nystagmus. Patients have variable VA, reduced night vision, often high myopia, and the ERG is negative (see Fig. 89.6B). Pendular, oblique, and mostly dysconjugate nystagmus of high frequency and low amplitude and dual jerk nystagmus has been described. Inheritance is most commonly X-linked and mutations of two genes have been found to be causative.19 Nystagmus in retinal dystrophies can occur in ciliopathies, which consists of dysfunction of the primary cilium, an organelle involved in intracellular and intercellular sensing and signaling (e.g. Alström syndrome, Bardet–Biedl syndrome, Joubert syndrome, Senior–Løken syndrome, and Leber congenital amaurosis). In retinal dystrophies, nystagmus can occasionally appear later in life as the VA deteriorates.
Nystagmus can be associated with low vision in early infancy due to numerous causes such as retinopathy of prematurity, congenital cataracts, corneal opacity, and optic nerve hypoplasia. In these patients, nystagmus can have the same characteristics as in achromatopsia or CSNB, or have characteristics of manifest latent nystagmus. Early treatment of cataract or other media opacities can prevent the development of nystagmus. Mutations in the PAX6 gene, inherited in an autosomal dominant pattern, are associated with nystagmus that can be horizontal, vertical, or torsional (see Fig. 89.3A3).9,20 OCT typically shows foveal hypoplasia (see Fig. 89.7D,E) but the VEP does not show misrouting of the optic nerve that is characteristic of albinism. Aniridia is common but not always present.
Nystagmus in neurological diseases or syndromes
Childhood nystagmus is a common feature of a range of syndromes, developmental and neurological disorders, for example Down syndrome, Noonan syndrome, structural malformations, space-occupying lesions, periventricular leukomalacia, cerebral palsy, leukodystrophy, Chiari malformation, metabolic disease, or mitochondrial disease.30 Vertical, torsional, seesaw, or dysconjugate nystagmus waveforms are common in neurological disorders (see Fig. 89.3B, showing vertical nystagmus in Chiari malformation). MRI is essential if there are other neurological symptoms, developmental delay, optic atrophy, or any suspicion of atypical nystagmus.
Spasmus nutans
Spasmus nutans consists of a triad of nystagmus, head nodding, and abnormal head posture. The onset is later than in infantile nystagmus, usually developing after 6 months of age. The nystagmus is of high frequency and pendular. The nystagmus may be intermittent and dysconjugate between both eyes or sometimes clinically apparent in only one eye (see Fig. 89.3D).31 Clinically the nystagmus usually disappears spontaneously 1–2 years after onset, although subclinical nystagmus persists on eye movement recordings. In spasmus nutans, head nodding suppresses the nystagmus since the vestibulo-ocular reflex stabilizes the eyes, which can permit development of binocular vision (see Fig. 89.3D).31 The etiology of spasmus nutans remains unclear; however, it has been associated with a lower socioeconomic status.32 The same nystagmus characteristics combined with head nodding and torticollis can also occur in suprasellar tumors such as chiasmal glioma.33 If there is afferent pupillary defect or optic nerve pallor, a tumor should be suspected. Some retinal diseases such as achromatopsia and CSNB can mimic spasmus nutans.34 The authors recommend, therefore, that ERG and/or MRI be performed in children presenting with spasmus nutans.
Manifest latent nystagmus
MLN or fusional maldevelopment nystagmus syndrome (FMNS) is part of the congenital squint syndrome. The nystagmus is typically larger upon covering one eye, the fast phase beats to the fixing or open eye, and the slow phase has decreasing velocity (see Fig. 89.4C). FMNS is discussed in Chapter 76.
Treatment
Spectacles and contact lenses
The incidence of refractive error in nystagmus is high.35 Children with nystagmus under 6 years of age, therefore, need repeated refraction every 3–12 months to prevent amblyopia. Contact lenses can be helpful because they may give better optical correction. Contact lenses allow patients to adopt large AHPs with better optical correction, as contact lenses do not have the problems of decentration and obstruction of the visual axis by spectacle frames (see Fig. 89.5B). Some studies have also suggested that contact lenses reduce nystagmus by providing sensory feedback through the eyelids, although recent studies suggest that improvements are not clinically significant.36
Surgical treatment and treatment with prisms
Patients often use compensatory strategies to reduce nystagmus. These strategies are different in individual patients. Fully understanding the compensatory mechanisms used by a patient allows formulation of a therapeutic plan. Compensatory mechanisms can often be assisted using surgery or prisms. Surgery for abnormal head postures usually yields excellent and sustained improvement.
Kestenbaum-type procedures
Patients with infantile nystagmus, especially idiopathic nystagmus and nystagmus associated with albinism, commonly have a null region, i.e. a direction of gaze in which nystagmus intensity is reduced and foveation is increased. If the null region is not in the primary position, patients often adopt an abnormal head posture using the eccentrically positioned null region for better vision (see Figs. 89.4A [null region on eye movement recordings] and 89.5A,B,F,G; Case study 1). Usually the null region is either in the primary position of gaze or along the horizontal plane. Some patients, however, despite having horizontal nystagmus, have vertical head postures or head tilts, or a combination of abnormal head postures in different planes. Patients with infantile vertical nystagmus can also show horizontal head postures. These mechanisms are not well understood.
If patients have vertical head postures, recess or resect procedures can be performed on vertical and/or oblique rectus muscles. For head tilt, rotatory Kestenbaum procedures can be performed, either by recession and resection of oblique muscles or by inducing torsion by moving the insertion of the rectus muscles.37 If the two horizontal or vertical rectus muscles are operated on in either eye, they can be shifted up and down or left and right from the insertion to induce a rotator effect on the eye. If the patient has manifest strabismus, surgery for the abnormal head posture needs to be performed on the fixing eye. The amount of strabismus resulting from preoperative strabismus and possibly surgery for the abnormal head posture can be corrected in the non-fixing eye (Case study 2). Significant amounts of horizontal muscle recession and resection are necessary for large head turns.38
Surgery for abnormal head postures is usually very successful. Surgery can be performed at any age; however, it is important to wait until the cause of the head turn can be well established. If amblyogenic factors are caused by the child not being able to wear glasses due to a large abnormal head posture, surgery should be performed as early as possible. Otherwise a convenient age for surgery is around 6–8 years of age, when the child is cooperative and can be easily examined. However, the time of surgery needs to be assessed with the parents and child according to the child's symptoms. It should also be borne in mind that head turns do not often fully develop until school age, when the head posture may become more frequent and pronounced with increasing school work. Kestenbaum-type procedures are effective even in adults. It is preferable to record eye movements before and after surgery to better understand mechanisms.
Artificial divergence
Convergence reduces the intensity of infantile nystagmus in many individuals. In these patients, artificial divergence can be induced to increase convergence and to trigger a convergence impulse, even at distance. Good binocular vision is essential for the effectiveness of artificial divergence. Without binocular vision, surgery or prisms would simply change the angle of squint without inducing convergence. Fusion range and the optimal strength of base-out prisms to reduce the nystagmus should be tested. It is often best to wear Fresnel prisms for at least 1 or 2 weeks during normal activities and to adjust the amount of prisms, if needed, before making a surgical decision. If prisms are small, then they can also be incorporated into glasses.
Nystagmus blockage syndrome
Some patients with manifest latent or infantile nystagmus can dampen nystagmus by over-convergence (Fig. 89.9). Bilateral medial rectus recession can help to permanently dampen the nystagmus (Case study 3).39 This forces the patient to maintain convergence in order to keep the eyes straight and in doing so improves the visual acuity.
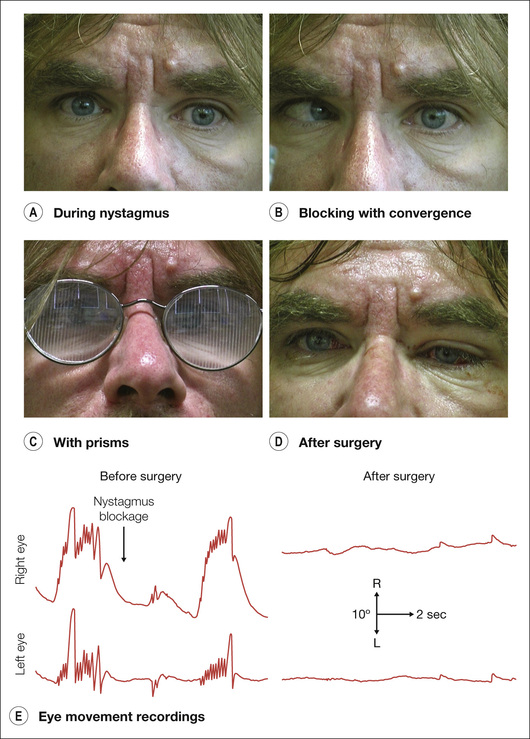
Case study 3
A patient with nystagmus from birth complained about constant “unquiet eyes” and needing to make an effort to turn in one eye in order to have better vision. On examination, he had nystagmus and intermittent large-angle esotropia. Eye movement recordings showed jerk nystagmus with waveforms showing IIN and manifest latent nystagmus reducing on convergence. Bilateral medial rectus recessions of 5 mm reduced the nystagmus and esotropia. Visual acuity with both eyes open improved from 6/12 to 6/9 (Fig. 89.9).
Reproduced from Lorenz B, Brodsky MC, editors. Pediatric Ophthalmology, Neuro-Ophthalmology, Genetics: Strabismus – New Concepts in Pathophysiology, Diagnosis, and Treatment. Berlin; London: Springer, 2010.
Adduction
Adduction dampens manifest latent nystagmus. If, for example, the left eye is dominant, the patient will fix in adduction with the left eye and turn the head to the left (see Fig. 89.5C). If strabismus surgery is performed, the dominant fixing eye should be operated on to correct the abnormal head turn simultaneously. If a patient with manifest latent nystagmus has an alternating strabismus, the head turn can change in the direction of the fixing eye and this can give the false appearance of PAN (Case study 4) where more than one head posture can be adopted (see Fig. 89.5D). If a patient with manifest latent nystagmus fixes with one eye at near and the other at distance, the head turn may change accordingly.
Reduction of strabismus
Reduction of strabismus and improvement of binocular vision in manifest latent nystagmus can reduce nystagmus intensity.40 Thus, patients with “A” and “V” pattern strabismus may adopt a chin-up or chin-down head position in order to reduce the angle of strabismus and improve the nystagmus (see Fig. 89.5E). In patients with manifest latent nystagmus, strabismus surgery, ideally with the objective of achieving a degree of binocular vision with microstrabismus, can substantially improve nystagmus (Case study 5).
Periodic alternating nystagmus
If the quiet phase of PAN is not static, then the head posture can slowly oscillate from left to right. It is very important to recognize if a patient has PAN before surgery is performed, as Kestenbaum procedures may increase the head turn to one side in PAN. About 23% of patients with IIN associated with mutations in FRMD7 and 29% of patients with albinism have PAN.12,27 Ideally patients should have eye movement recordings over a period of at least 8 minutes as the cycle of PAN in infantile nystagmus has been found to be between 90 and 280 seconds (see Fig. 89.4B).27 However, many patients with PAN do not have alternating head position, probably because their null region is not moving. In PAN, one can recess all four horizontal muscles to improve head position.
Tenotomy of four rectus muscles
This procedure consists of detaching and re-attaching the rectus muscles at their insertion. It has been reported that tenotomy reduces nystagmus and broadens the null region due to changes in proprioceptive feedback from the eye muscles.41 The procedure can be performed on horizontal or vertical muscles and be combined with correction of strabismus. More results and corroboration between several research groups need to be obtained before drawing firm conclusions over the value of tenotomies.
Pharmacological treatment
Baclofen, gabapentin, cannabis, memantine, aminopyridines, and several other drugs were primarily used in acquired nystagmus.42 Baclofen was also found to be effective in infantile PAN.43 Recently, gabapentin and memantine have been found to be effective in a double-masked randomized controlled study including patients with infantile nystagmus.44 Gabapentin (up to 2400 mg) and memantine (up to 40 mg) were used in slowly increasing dosages. Although the medications are effective in IIN, it is not clear which patients respond best to which type of treatment. Larger trials are now underway.
Other treatments
Botulinum toxin has been reported to reduce infantile nystagmus.45 However, injections need to be repeated and can induce strabismus and ptosis. Other methods such as auditory feedback have been shown to be ineffective or impractical in infantile nystagmus.
Acknowledgement
The authors wish to thank Rebecca McLean for help with preparation of the video recordings and figures in the chapter. They would also like to thank Geoffrey Woodruff for his careful and critical feedback in reading the manuscript. Finally, they also thank the Ulverscroft Foundation for their continuous support.