Uterovaginal displacements, damage and prolapse
Uterine Displacements
The uterus is an organ that normally pivots about an axis formed by the cardinal ligaments at the level of the internal cervical os. In 90% of women the uterus is anteflexed and anteverted, lying on the urinary bladder and moving backwards as the bladder fills. In 10% of women the uterus is retroflexed and may be retroverted (Fig. 38.1). This is a developmental occurrence. The uterus is mobile and can be moved by inserting a finger in the posterior vaginal fornix. In spite of anecdotal statements, a mobile retroverted uterus is not a cause of infertility, abortion or backache.

Acquired uterine retroversion may occur, but is less common. It is associated with endometriosis of the uterosacral ligaments or the cul-de-sac; with adhesions resulting from pelvic inflammatory disease; or caused by a tumour in front of the uterus pushing it backwards.
Symptoms
Developmental retroversion is symptomless; only when the retroverted uterus is ‘fixed’ may symptoms occur. These include the symptoms associated with the underlying cause. In addition, the woman may complain of dyspareunia on deep penetration, pelvic pain and low backache. A few women who have chronic pelvic pain and are told by their doctor that their uterus is retroverted will obtain some relief if the uterus is manipulated to become anteverted. They often remain pain free when the uterus becomes retroverted again, as it usually does.
Diagnosis
A clinical finding that the uterus is retroverted and is accompanied by symptoms should alert the medical practitioner to determine whether the retroversion can be corrected by manipulation (Fig. 38.2). If it can, it is not the cause of the symptoms. If it cannot be manipulated it may be the cause of the symptoms.

Treatment
In most cases the woman needs reassurance that the retroverted uterus is not the cause of any symptoms she may have, and does not require treatment. If the uterus is ‘fixed’ and the woman has symptoms of deep dyspareunia or chronic pelvic pain, surgery may be suggested, but the patient should be told that, although it may correct the position of the uterus, the symptoms may not be relieved permanently. The procedure is aimed at shortening the round ligaments by plication and treating any pelvic pathology at the same time.
Uterovaginal Damage and Injuries
Injury to the vulvovaginal area may occur, for example, if a girl or woman falls astride some object or is kicked. The vagina may be damaged or a haematoma may form in the vulva (Fig. 38.3). Injury may also occur if a young girl or a postmenopausal woman is sexually assaulted.

During the first sexual intercourse, the hymen is stretched and torn and a small amount of bleeding results; very occasionally more severe bleeding occurs if a large blood vessel is damaged.
Injury resulting from childbirth is discussed on page 84. Occasionally a vaginal tear is not sutured immediately, and the woman attends a medical practitioner some time later. On inspection the vaginal entrance is seen to gape and the perineal muscles are separated (Fig. 38.4). The woman may complain that water enters her vagina when she bathes, or that vaginal flatus occurs.

Vaginal burns may occur following a very hot vaginal douche, or the deliberate insertion of a caustic agent, such as rock salt, to procure an abortion or, in a few cultures, following tightening of the vagina after childbirth to make sexual intercourse more satisfying to the man.
Cervical damage may occur during rough cervical dilatation. The laceration is usually small, but may extend from one or other lateral angle of the external cervical os. This may cause marked bleeding. Cervical damage may also occur during childbirth and is discussed on pages 86 and 87.
Genital Tract Fistulae
Genital tract fistulae occasionally follow childbirth, but in the developed countries they usually result from a complication of surgery or following radiotherapy. Fistulae are very uncommon in the developed countries. They may develop between the vagina and uterus and any adjacent organ. The most frequently encountered fistulae lie between the vagina and the bladder (vesicovaginal fistula) or between the vagina and rectum (rectovaginal fistula).
Obstetrical and surgical fistulae occur immediately after the procedure or 5–14 days after the operation, when the traumatized ischaemic tissue sloughs. The woman complains of continuous leakage of urine in cases of a vesicovaginal fistula, or faeces in the case of a rectovaginal fistula. If the fistula is large it can be seen on vaginal inspection with a Sims speculum, the woman lying in the left lateral position. Small fistulae may require tests to pinpoint the damaged area. One such test is shown in Figure 38.5. Small vesicovaginal fistulae may close spontaneously if the bladder is drained continuously for 14 days, but rectovaginal fistulae and larger fistulae require surgery.

Uterovaginal Prolapse
Uterovaginal prolapse is defined as a descent of the uterus or vagina. A vaginal prolapse may occur independently of any uterine descent, but a prolapsed uterus always carries some part of the upper vagina with it.
To understand how uterovaginal prolapse occurs some knowledge about the supports of the uterus is required. The uterus is supported in the midpelvis by three structures. These are:
• The vagina, the walls of which lie in apposition and are muscular.
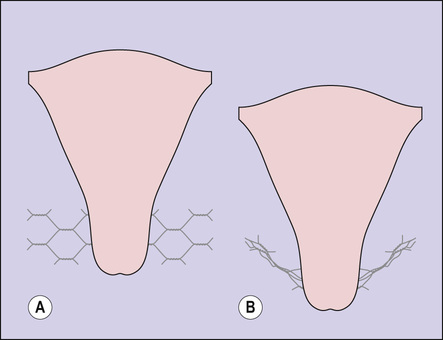
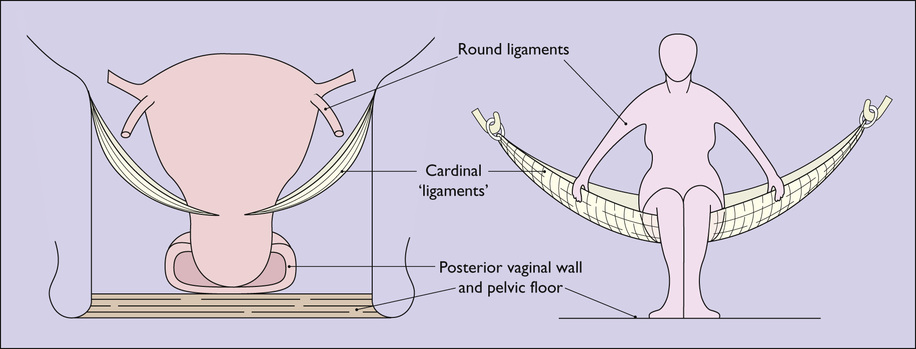
• The transcervical (cardinal) ligaments, which stretch from each pelvic wall and attach to the uterus at the level of the supravaginal cervix. They are not ligaments in the true sense as they are composed of a felted mass of collagenous connective tissue through which blood vessels pass to supply the uterus and bladder (Fig. 38.6). The cardinal ligaments act as the middle support of the uterus and their function can be explained in terms of chicken wire. If the strain is not too great the ligaments have considerable tensile strength, but if the strain is increased or the ligaments are damaged, they stretch (Fig. 38.7). Posteriorly, on each side, condensations of the tissue form the uterosacral ligament.

• The upper supports of the uterus, i.e. the relatively weak round ligaments, which operate mostly by maintaining the uterus in an anteverted position so that the increase in intra-abdominal pressure on straining forces the uterus on to the bladder, rather than directly down towards the vulva.
Acting in conjunction, these supports prevent uterine prolapse (Fig. 38.8). However, this state of affairs may be altered if the supports are stretched during childbirth. This may occur if the woman tries to expel the fetus before the cervix is fully dilated, strains for a long time in the second stage of labour, or if undue force is used to expel the placenta. In these circumstances the cardinal ligament may be stretched, making a uterine prolapse more likely. In consequence, prolapse is more common in women who have had several children and are obese.
Uterovaginal prolapse is more common in the later reproductive years and after the menopause. In most cases it is due to damage to the supporting tissues and pudendal nerve damage occurring during childbirth, but is not apparent until the tissues atrophy in middle age when, deprived of oestrogen, the collagen tissue of the ligaments diminishes and the vaginal muscle becomes weaker, permitting the prolapse to occur. An additional cause may be chronic constipation leading to straining.
A further way in which prolapse occurs in a very few nulliparous women is through the supporting tissues failing to develop properly.
Degrees of uterine prolapse
For descriptive purposes uterovaginal prolapse is divided into three degrees of increasing severity (Fig. 38.9). In each of these the cervix elongates and may become congested or oedematous. When the cervix protrudes from the vagina, as in the third degree of prolapse, the cervical epithelium becomes dry and its superficial layers are keratinized.

With better obstetric care the frequency of uterovaginal prolapse is diminishing and severe cases are not so often seen.
Prolapse of the anterior vaginal wall (cystocele)
This occurs during childbirth, when the fibres of the levator ani muscle, which supports the vagina, are stretched. The weakened anterior vaginal wall bulges into the vagina, bringing the adjacent bladder with it (Fig. 38.10).

Prolapse of the posterior vaginal wall (rectocele)
In this situation the supporting tissues of the distal posterior wall, including the perineal muscles, are stretched or damaged during the delivery of the baby.
With diminished support, the posterior vaginal wall, together with the anterior rectal wall, bulges into the vagina (Fig. 38.11).

If the supports of the proximal vaginal wall are weakened (for example after hysterectomy) it may bulge into the vagina, often containing bowel. This is termed an enterocele.
Symptoms and diagnosis
Many women have no symptoms but are concerned that ‘something is bulging in my vagina’. Some women feel dragging pains in the lower pelvis, and have difficulty or discomfort when they try to micturate or defecate. Other women are mildly incontinent.
The type and degree of uterovaginal prolapse can be diagnosed by looking at the woman's vulvovaginal area when she coughs or strains. A vaginal examination using a Sims speculum will confirm the prolapse. A rectal examination may be needed to differentiate a rectocele from an enterocele.
Treatment
Treatment depends on the age of the woman, her desire to have further children, and the degree of the prolapse. Younger women with mild degrees of symptomless prolapse can delay treatment until the prolapse worsens or the menopause is reached. Hormone replacement during menopause may be appropriate.
First-line treatment for pelvic organ prolapse and urinary stress incontinence involves learning pelvic floor exercises (see Box 39.1), which alone may control the symptoms, providing these are well taught and with good follow-up. It is preferable not to treat a prolapse surgically if the woman wishes to have a further child, as the delivery must then be by caesarean section to avoid damage to the repair. If the woman has a cystocele, a midstream urine sample should be taken to exclude bacteriuria. If the urine is sterile, surgery is not required unless the woman desires it. She should be checked periodically.
Introduction of a pessary into the vagina to restore the prolapsed organs to their normal position is successful in relieving symptoms in over 50% of cases. Whether the woman wishes to take responsibility for her own self-care and cleaning or return to her doctor for this care needs to be discussed.
If the prolapse is marked and is causing symptoms, surgery can be recommended. There are three choices, which should be discussed with the woman. They may or may not involve hysterectomy. The first is uterosacral ligament suspension during which the vaginal apex is resuspended to the uterosacral ligaments. Second, if the vagina is long enough to reach the sacrospinous ligament this can also be used to suspend the vagina. The third involves fixing mesh to the anterior and posterior vagina and attaching to the anterior longitudinal ligament to resuspend the vaginal apex. The use of mesh does carry the risk of complications that include infection and mesh erosion and its long-term effectiveness has still to be evaluated. If urinary incontinence is present it should be treated.
Postmenopausal women should be given oestrogen for 4–6 weeks before the operation to improve the quality of the vaginal tissues. The treatment of a cystocele or a rectocele consists of repairing the vagina by excising a triangular piece of the anterior or posterior vaginal wall, depending on whether a cystocele or a rectocele is present, pushing the bladder or rectum proximally, and suturing the supporting muscles beneath it and then rejoining the cut edges of the vagina.