Substance Use Assessment

Alcohol Use and Abuse
In 2008, slightly more than half (51.6%) of Americans ages 12 and older reported being current alcohol drinkers.32 More than one fifth (23.3%) of persons ages 12 and older were binge drinkers (≥5 drinks/occasion) and 6.9% reported heavy drinking (binge drinking on at least 5 days in the past 30 days). Thus alcohol is the most used and abused psychoactive drug. People like to drink! Given the rates of alcohol use, it is not surprising that many patients in the hospital and in primary care offices find themselves with alcohol-related disorders.
Morbidity and mortality data reflect the adverse consequences of excessive alcohol use. Alcohol is involved in 40% of the 41,000 annual deaths due to traffic crashes.23 The number of emergency department (ED) visits attributable to alcohol from the period 1992 to 2000 was about 68.6 million,19 with an increasing trend of 18% during that time. In the general population, alcohol consumption of at least 4 standard drinks per day (each containing 12 g alcohol, see Table 6-1) is associated with increased rates of death from cirrhosis and alcoholism; cancers of the mouth, esophagus, pharynx, and liver combined; and injuries and other external causes in men.30 In women, alcohol consumption increases the risk for breast cancer in a dose-response relation, starting at an alcohol intake of 24 g (about 2 drinks) a day.15 The link between chronic alcohol use and alcohol liver disease is well known. Cirrhosis accounted for 27,000 deaths in the United States in 2004, or the 12th leading cause of death.6 There are multiple alcohol effects on the heart. Chronic heavy use increases the risk for alcoholic cardiomyopathy, with an increase in left ventricular mass, dilation of ventricles, and wall thinning.31 Hypertension is a common detrimental effect, with a causal association between consumption of 30 to 60 g alcohol per day (3 to 5 standard drinks) and blood pressure (BP) elevation in men and women.13 Finally, alcohol and illicit drugs are arrhythmogenic and are associated with the rapid heart rate of atrial fibrillation.14
TABLE 6-1
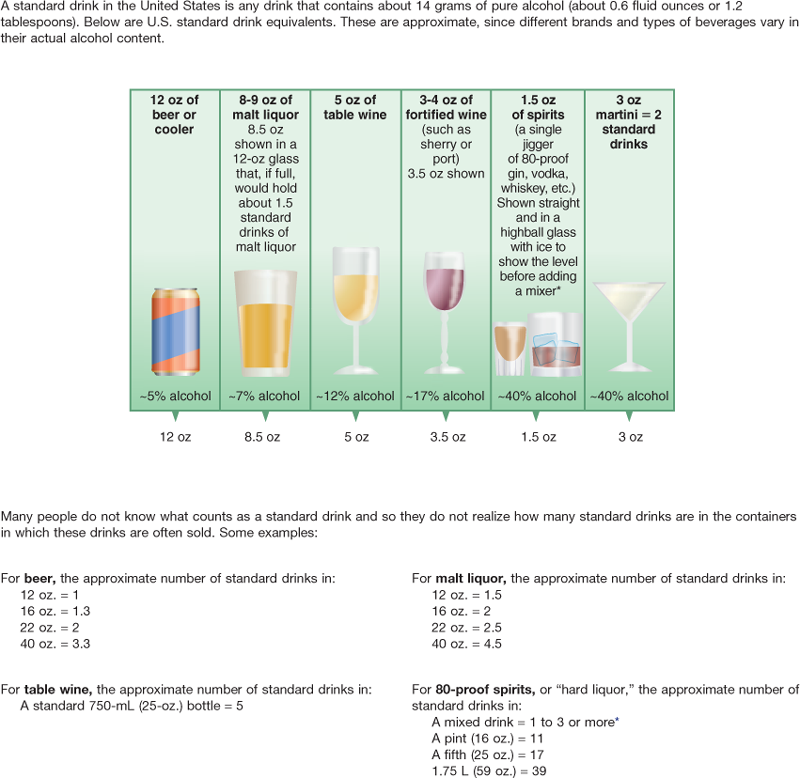
*Note: It can be difficult to estimate the number of standard drinks in a single mixed drink made with hard liquor. Depending on factors such as the type of spirits and the recipe, a mixed drink can contain from one to three or more standard drinks.
Adapted from National Institute on Alcohol Abuse and Alcoholism (NIAAA). (Reprinted 2007). Helping patients who drink too much: a clinician’s guide. Available at http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm.
Because of alcohol-related morbidity, many patients you encounter in primary care settings and in the hospital will have a significant drinking history. Persons visiting primary care providers have a significantly higher rate of past or present alcohol abuse (23%) than those in the general population (9%).17,21a Surveys of hospital ICU admissions show a range of 12% to 21% prevalence of alcohol dependence among their patients.18,24 Excessive alcohol use increases risk for ICU admissions due to trauma, hypothermia, and pancreatitis. Once in the hospital, heavy alcohol use can lead to respiratory failure from acute alcohol intoxication and alcohol withdrawal syndrome. Alcohol dependence increases risk for sepsis, septic shock, and hospital mortality among ICU patients.24
Defining Illicit Drug Use
In 2008, about 8% of Americans ages 12 years and older reported current (past month) illicit drug use.33 Illicit drugs include marijuana/hashish, cocaine (including crack), heroin, hallucinogens, inhalants, and prescription-type drugs used nonmedically. Marijuana was the most commonly used illicit drug, with 6.1% of persons ages 12 years and older reporting past-month use. Among youth ages 12 to 17 years, between 2002 and 2008, the rates of use of illicit drugs in general declined significantly (from 11.6% to 9.3%). Still, that represents 1 out of 10 adolescents as illicit drug users. This warrants our attention and intervention. Any amount of illicit drug use has serious legal consequences, as well as consequences for health, relationships, and future jobs, school, and career.
The abuse of prescription drugs is the fastest growing drug problem in the United States. Between 2004 and 2008, visits to hospital EDs for the nonmedical use of narcotic pain relievers more than doubled, rising 111%.7 The three most frequently abused prescription opioid pain relievers were products using oxycodone, hydrocodone, and methadone. The misuse of prescription drugs has a huge impact not only on health and safety but also on burdens to the ED system.
Diagnosing Substance Abuse
The rate of Americans classified with substance abuse or dependence is 9.2 % of the population ages 12 years and older; of these persons, 68% were dependent on or abused alcohol but not illicit drugs and 14% used both alcohol and illicit drugs. There is a continuum of alcohol drinking ranging from special occasion use, through moderate drinking, to harmful drinking (Table 6-2). Alcohol dependence or alcoholism is a chronic progressive disease that is not curable but is highly treatable. Accurate diagnosis is needed in order to provide advice, brief intervention, appropriate treatment, and follow-up. The gold standard of diagnosis is well defined by the American Psychiatric Association (APA) in their Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV-TR). Tables 6-3 and 6-4 give the criteria for these diagnoses. Unfortunately, alcohol problems are underdiagnosed both in primary care settings and in hospitals. Excessive alcohol use often is unrecognized until patients develop serious complications.
TABLE 6-2
Categories and Definitions for Patterns of Alcohol Use
| Category | Organization | Definition |
| Moderate drinking | NIAAA | Men, ≤2 drinks/day; women, ≤1 drink/day; >65 years, ≤1 drink/day |
| At-risk drinking | NIAAA | Men, >14 drinks/wk or >4 drinks/occasion; women, >7 drinks/wk or >3 drinks/occasion |
| Hazardous drinking | WHO | At risk for adverse consequences from alcohol |
| Harmful drinking | WHO | Alcohol is causing physical or psychological harm |
| Alcohol abuse | APA | ≥1 of the following events in a year: recurrent use resulting in failure to fulfill major role obligations; recurrent use in hazardous situations; recurrent alcohol-related legal problems (e.g., DUI); continued use despite social or interpersonal problems caused or exacerbated by alcohol |
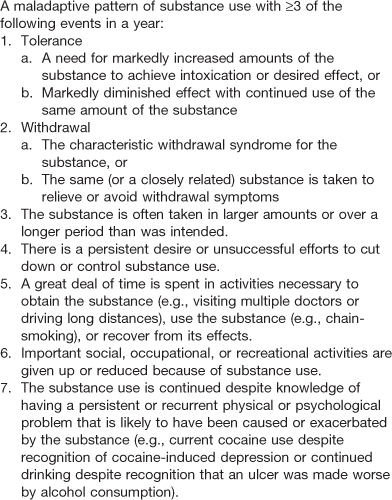
| Alcohol dependence | APA | ≥3 of the following events in a year: tolerance (increased amounts to achieve effect; diminished effect from same amount); withdrawal; a great deal of time spent obtaining alcohol, using it, or recovering from its effect; important activities given up or reduced because of alcohol; drinking more or longer than intended; persistent desire or unsuccessful efforts to cut down or control alcohol use; use continued despite knowledge of having a psychological problem caused or exacerbated by alcohol |
APA, American Psychiatric Association; DUI, driving under the influence; NIAAA, National Institute on Alcohol Abuse and Alcoholism; WHO, World Health Organization.
TABLE 6-3
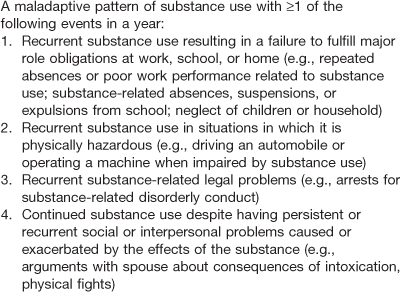
Adapted from American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, DSM-IV-TR (4th ed., pp. 182-183). Washington, DC: Author.
 Developmental Competence
Developmental Competence
The Pregnant Woman
Among pregnant women ages 15 to 44 years, about 10.6% report current alcohol use, with 4.5% reporting binge drinking and 0.8% reporting heavy drinking.32 These rates are much lower than their age-matched counterparts who are not pregnant (54%, 24.2%, and 5.5%, respectively). However, no amount of alcohol has been determined safe for pregnant women. The potential adverse consequences of alcohol use to the fetus are well known. Thus all women contemplating pregnancy and who are pregnant should be screened for alcohol use, and abstinence should be recommended.
The Aging Adult
The prevalence of current alcohol use decreases with increasing age, from 67.4% among those ages 26 to 29 years; down to 50.3% in those ages 60 to 64 years; and to 39.7% in adults ages 65 years and older.32 However, older adults have numerous characteristics that can increase the risk for alcohol use. Liver metabolism and kidney function are decreased, which increases the bioavailability of alcohol in the blood for longer time periods. Aging people lose muscle mass; less tissue for the alcohol to be distributed to means an increased alcohol concentration in the blood. Older adults may be on multiple medications, which can interact adversely with alcohol (e.g., benzodiazepines, antidepressants, antihypertensives, aspirin, to name just a few). Drinking alcohol increases risk for falls, depression, and gastrointestinal problems. Finally, older adults may avoid detection of their alcohol problems; they may avoid alcohol-related consequences such as a DUI just because they no longer drive, or they may avoid job problems just because they no longer work.
Subjective Data
If the patient currently is intoxicated or going through substance withdrawal, collecting any history data is difficult and unreliable. However, when sober, most people are willing and able to give reliable data, provided that the setting is private, confidential, and nonconfrontational.
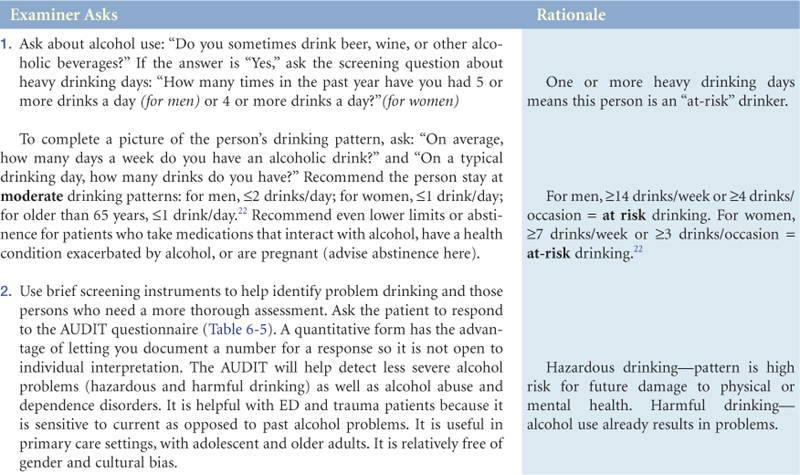
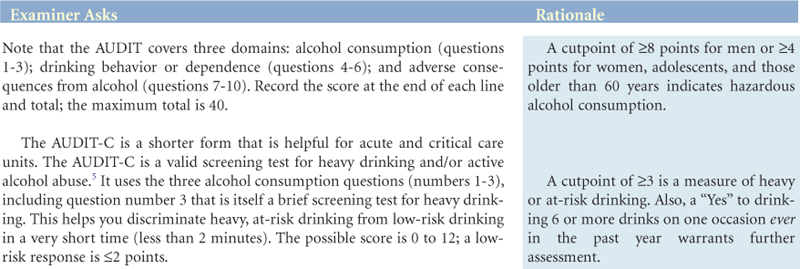

TABLE 6-5
The Alcohol Use Disorders Identification Test—AUDIT*
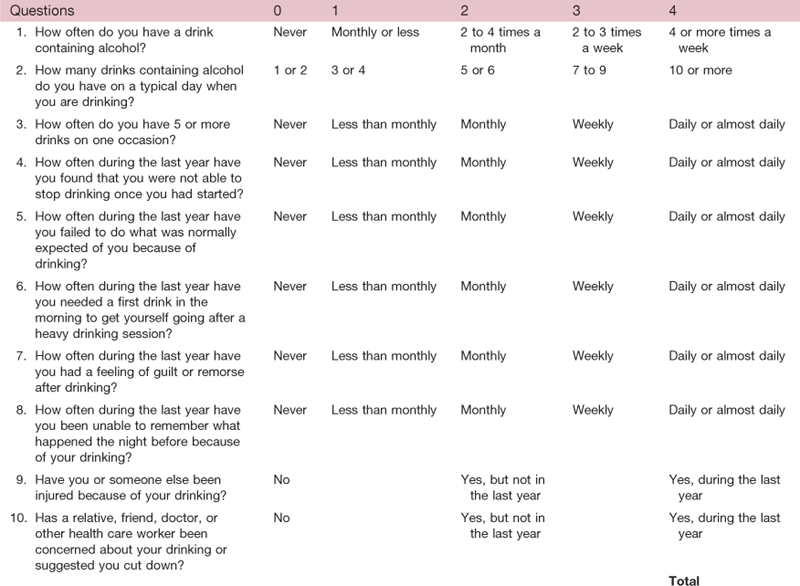
*NOTE: This questionnaire (the AUDIT) is reprinted with permission from the World Health Organization. To reflect standard drink sizes in the United States, the number of drinks in question 3 was changed from 6 to 5. A free AUDIT manual with guidelines for use in primary care settings is available online at www.who.org.
Objective Data
| Normal Range of Findings | Abnormal Findings |
| Clinical laboratory findings give objective evidence of problem drinking. These are less sensitive and specific than self-report questionnaires, but they are useful data to corroborate the subjective data. The serum protein gamma glutamyl transferase (GGT) is the most commonly used biochemical marker of alcohol drinking. Occasional alcohol drinking will not raise this measure, but chronic heavy drinking will. Be aware that nonalcoholic liver disease also can increase GGT levels in the absence of alcohol. | Chronic alcohol drinking of ≥4 drinks/day for 4 to 8 weeks significantly raises GGT. It takes 4 to 5 weeks of abstinence for GGT levels to return to normal range.21 |
| Serum aspartate aminotransferase (AST) is an enzyme found in high concentrations in the heart and liver. | Months of chronic drinking increases AST. |
| From the complete blood count, the mean corpuscular volume (MCV) is an index of red blood cell (RBC) size. MCV is not sensitive enough to use as the only biomarker, but it can detect earlier drinking after a long period of abstinence.21 | Heavy alcohol drinking for 4 to 8 weeks increases MCV. |
| Breath alcohol analysis detects any amount of alcohol in the end of exhaled air following a deep inhalation until all ingested alcohol is metabolized. This measure can be correlated with blood alcohol concentration (BAC) and is the basis for legal interpretation of drinking. Normal values indicating no alcohol are 0.00. | A BAC ≥0.08% = legal intoxication in most states (3 standard drinks), with loss of balance and loss of motor coordination. |
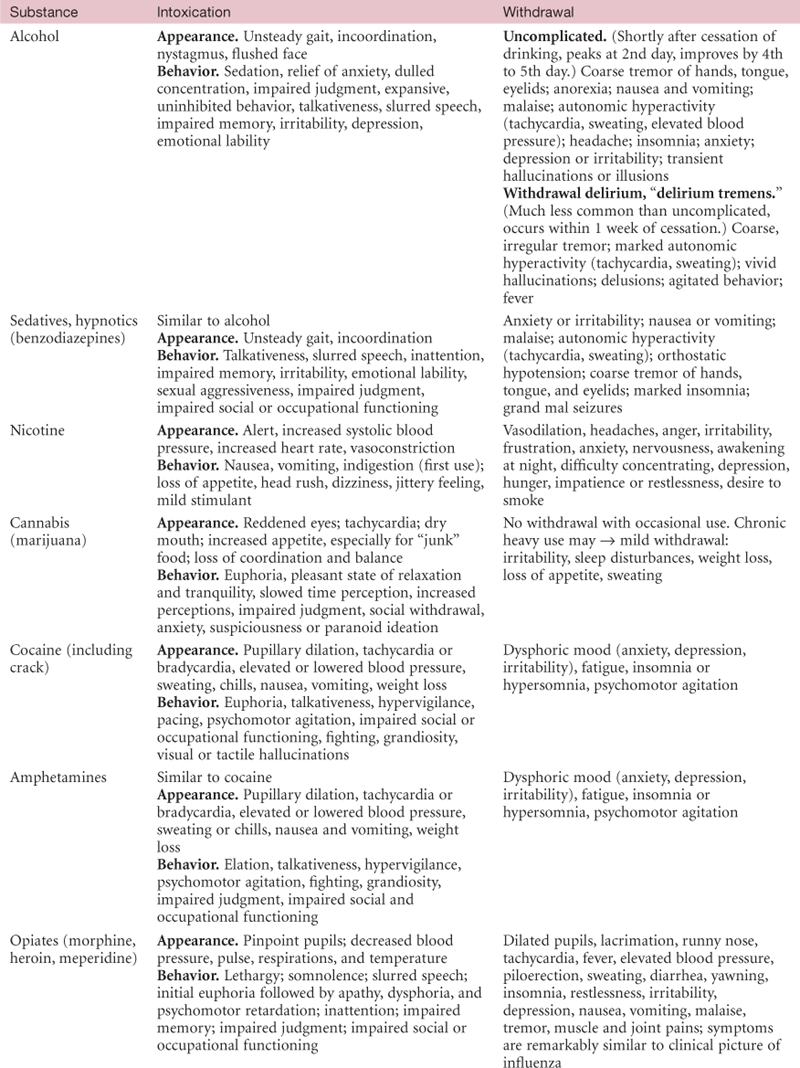
| Clinical appearance and behavioral signs of commonly abused substances are presented in Table 6-7. Note that clinical signs are described both for the intoxicated person and for the person in withdrawal. |

Bibliography
1. Allen NE, Beral V, Casabonne D, et al. Moderate alcohol intake and cancer incidence in women. Journal of the National Cancer Institute. 2009;101(5):296–305.
2. American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders, DSM-IV-TR. 4th ed. Washington, DC: Author; 1994.
3. Becker KL, Walton-Moss B. Detecting and addressing alcohol abuse in women. Nurse Practitioner. 2001;26(10):13–25.
4. Bohn MJ, Babor TF, Kranzler HR. The alcohol use disorders identification test (AUDIT). Journal of Studies on Alcohol. 1995;56(4):423–432.
5. Bush K, Kivlahan DR, McDonell MB, et al. The AUDIT alcohol consumption questions. Archives of Internal Medicine. 1998;158:1789–1795.
6. Centers for Disease Control and Prevention. Deaths: final data for 2004. National Vital Statistics Reports. 2007;55 Retrieved July 2010 from www.cdc.gov/nchs/data/nvsr; 2007.
7. Centers for Disease Control and Prevention. Emergency department visits involving nonmedical use of selected prescription drugs. MMWR Morbidity and Mortality Weekly Report. 2010;59 Retrieved July 2010 from www.cdc.gov/mmwr/pdf/wk/mm5923; 2010.
8. Compton WM, Thomas YF, Stinson FS, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States. Archives of General Psychiatry. 2007;64(5):566–576.
9. Ewing JA. Detecting alcoholism: the CAGE questionnaire. Journal of the American Medical Association. 1984;252(14):1905–1907.
10. Fiellin DA, Reid MC, O’Connor PG. Screening for alcohol problems in primary care: a systematic review. Archives of Internal Medicine. 2000;160(13):1977–1989.
11. Harwood GA. Alcohol abuse: screening in primary care. Nurse Practitioner. 2005;30(2):56–61.
12. Keegan J, Parva M, Finnegan M, et al. Addiction in pregnancy. Journal of Addictive Diseases. 2010;29(2):175–191.
13. Keil U, Liese A, Filipiak B, et al. Alcohol, blood pressure and hypertension. Chichester, UK: Wiley, Novartis Foundation Symposium; 1998.
14. Krishnamoorthy S, Lip GYH, Lane DA. Alcohol and illicit drug use as precipitants of atrial fibrillation in young adults. American Journal of Medicine. 2009;122:851–856.
15. Longnecker MP, Berlin JA, Orza MJ, et al. A meta-analysis of alcohol consumption in relation to risk of breast cancer. Journal of the American Medical Association. 1988;260(5):652–656.
16. Lucey MR, Mathurin P, Morgan TR. Alcoholic hepatitis. New England Journal of Medicine. 2009;360(26):2758–2769.
17. Manwell LB, Fleming MF, Johnson K, et al. Tobacco, alcohol, and drug use in a primary care sample. Journal of Addictive Diseases. 1998;17(1):67–81.
18. Marik P, Mohedin B. Alcohol-related admissions to an inner city hospital intensive care unit. Alcohol and Alcoholism. 1996;31(4):393–396.
19. McDonald AJ, Wang N, Camargo CA. U.S emergency department visits for alcohol-related diseases and injuries between 1992 and 2000. Archives of Internal Medicine. 2004;164:531–537.
20. Naegle MA. Screening for alcohol use and misuse in older adults. American Journal of Nursing. 2008;108(11):50–59.
21. National Institute on Alcohol Abuse and Alcoholism. Alcohol alert #56—screening for alcohol problems: an update. Retrieved July 2010 from http://pubs.niaaa.nih.gov/publications/aa56.htm; 2002.
22. National Institute on Alcohol Abuse and Alcoholism. Helping patients with alcohol problems: a health practitioner’s guide. NIH Pub. No. 03-3769 Rockville, MD: Author; January 2003.
22a. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Retrieved July 2010 from http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/Clinicians_guide.htm; 2005; (Reprinted 2007).
23. National Institutes of Health. Alcohol-related traffic deaths. Retrieved July 2010 from www.nih.gov/about/researchresultforthepublic; 2006.
24. O’Brien JM, Lu B, Ali NA, et al. Alcohol dependence is independently associated with sepsis, septic shock, and hospital mortality among adult intensive care unit patients. Critical Care Medicine. 2007;35(2):345–450.
25. Rehm J, Gmel G, Sempos CT, et al. Alcohol-related morbidity and mortality. Alcohol Research & Health. 2002;27(1):39–51.
26. Russell M, Materier SS, Sokol RJ. Screening for pregnancy risk drinking. Alcoholism: Clinical and Experimental Research. 1994;18(5):1156–1161.
27. Saitz R. Unhealthy alcohol use. New England Journal of Medicine. 2005;352(6):596–607.
27a. Saitz R, Horton NJ, Sullivan LM, et al. Addressing alcohol problems in primary care. Annals of Internal Medicine. 2003;138(5):372–382.
28. Sommers MS, Wray J, Savage C, et al. Assessing acute and critically ill patients for problem drinking. Dimensions of Critical Care Nursing. 2003;22(2):76–88.
29. Steinbauer JR, Cantor SB, Holzer CE, et al. Ethnic and sex bias in primary care screening tests for alcohol use disorders. Annals of Internal Medicine. 1998;129(5):353–362.
30. Thun MJ, Peto R, Lopez AD, et al. Alcohol consumption and mortality among middle-aged and elderly U.S adults. New England Journal of Medicine. 1997;337(24):1705–1714.
31. Urbano-Marquez A, Estruch R, Fernandez-Sola J, et al. The greater risk of alcoholic cardiomyopathy and myopathy in women compared with men. Journal of the American Medical Association. 1995;274(2):149–154.
32. U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. Results from the 2008 national survey on drug use and health. Rockville, MD: USDHHS Pub. No. SMA 09-4434; 2009; Retrieved July 2010 from www.oas.samhsa.gov/nsduh/2k8nsduh/2k8Results.pdf; 2009.
33. Volicer BJ, Quattrochi N, Candelieri R, et al. Depression and alcohol abuse in asthmatic college students. Nurse Practitioner. 2006;31(2):49–54.