General Survey, Measurement, Vital Signs
Outline

http://evolve.elsevier.com/Jarvis/
Objective Data
The general survey is a study of the whole person, covering the general health state and any obvious physical characteristics. It is an introduction for the physical examination that will follow; it should give an overall impression, a “gestalt,” of the person (see Sample Charting on p. 153). Objective parameters are used to form the general survey, but these apply to the whole person, not just to one body system.
Launch a general survey at the moment you first encounter the person. What leaves an immediate impression? Does the person stand promptly as his or her name is called and walk easily to meet you? Or does the person look sick, rising slowly or with effort, with shoulders slumped and eyes without luster or downcast? Is the hospitalized patient conversing with visitors, involved in reading or television, or lying perfectly still? Even as you introduce yourself and shake hands, you collect data. Does the person fully extend the arm, shake your hand firmly, make eye contact, or smile? Are the palms dry or wet and clammy? As you proceed through the health history, the measurements, and the vital signs, note the following points that will add up to the general survey. Consider these four areas: physical appearance, body structure, mobility, and behavior.
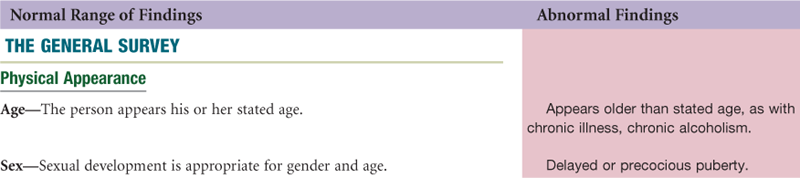
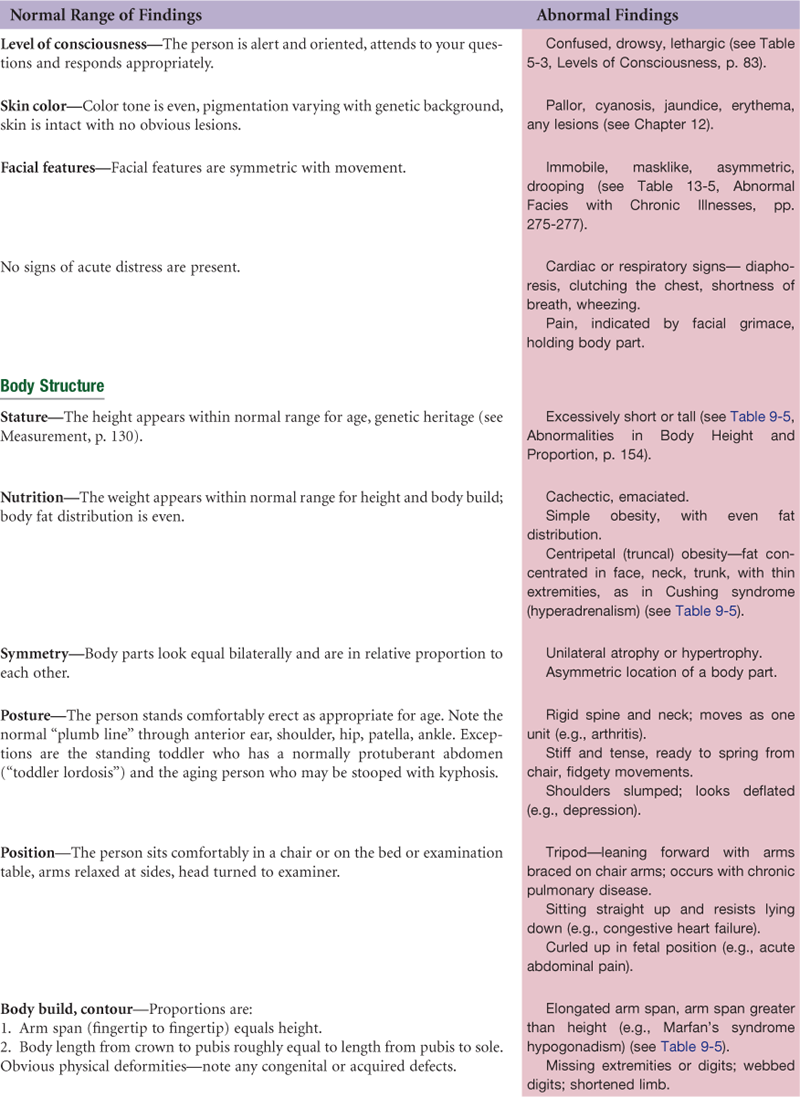
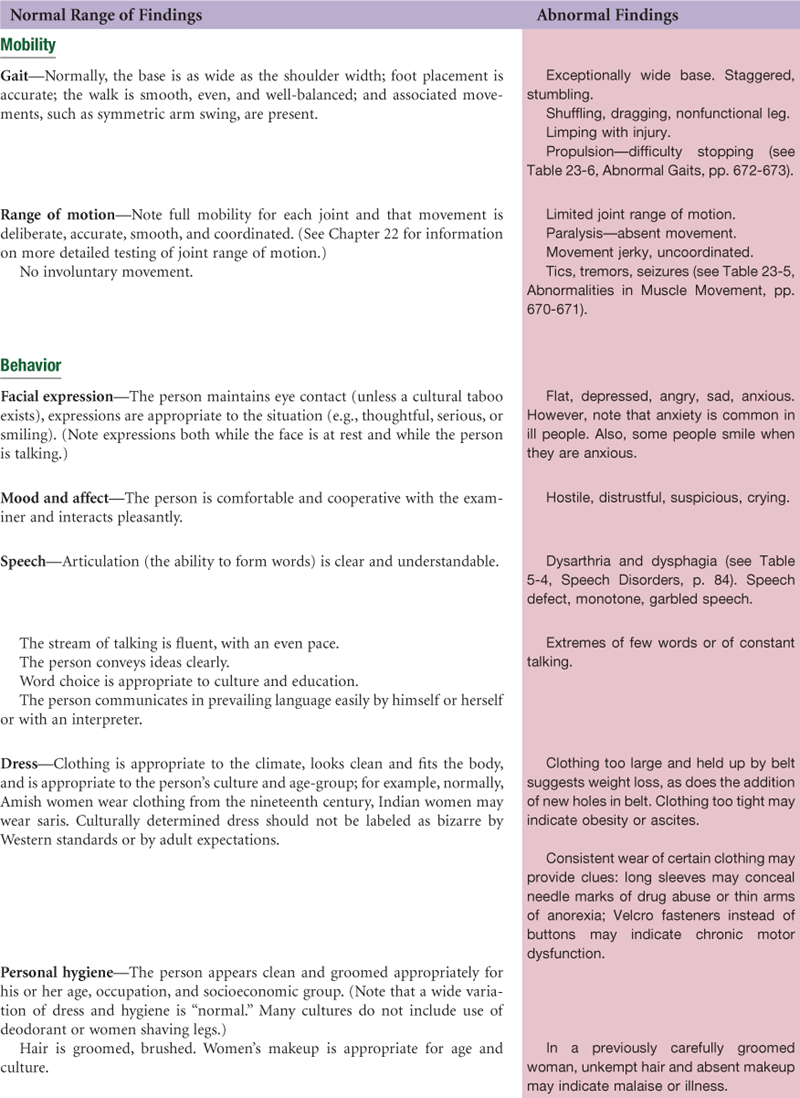


TABLE 9-1
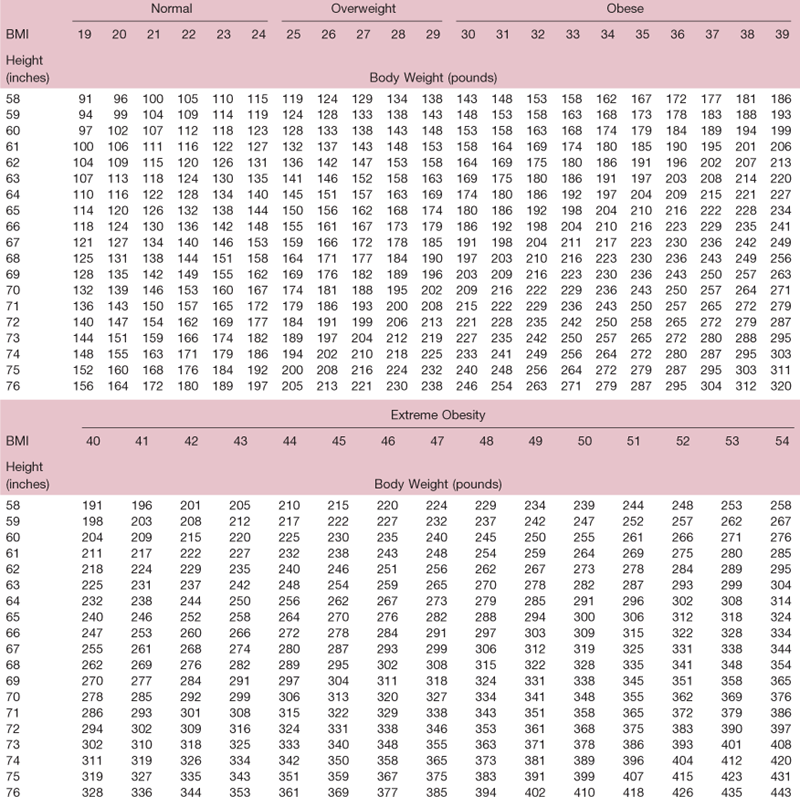
Adapted from Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. AccessedJune 9, 2009, from www.nhlbi.nih.gov/guidelines/obesity/bmi_tbl.pdf.
TABLE 9-2
| Age | Breaths per Minute |
| Neonate | 30-40 |
| 1 yr | 20-40 |
| 2 yr | 25-32 |
| 8-10 yr | 20-26 |
| 12-14 yr | 18-22 |
| 16 yr | 12-20 |
| Adult | 10-20 |
TABLE 9-4
Common Errors in Blood Pressure Measurement
| Common Error | Result | Rationale |
| Taking blood pressure reading when person is anxious or angry or has just been active. | Falsely high | Sympathetic nervous system stimulation |
| Faulty arm position: | ||
| Above level of heart | Falsely low | Eliminates effect of hydrostatic pressure |
| Below level of heart | Falsely high | Additional force of gravity added to brachial artery pressure |
| Person supports own arm | Falsely high diastolic | Sustained isometric muscular contraction |
| Faulty leg position (e.g., person’s legs are crossed) | Falsely high systolic and diastolic | Translocation of blood volume from dependent legs to thoracic area |
| Examiner’s eyes are not level with meniscus of mercury column: | ||
| Looking up at meniscus | Falsely high | Parallax |
| Looking down on meniscus | Falsely low | |
| Inaccurate cuff size (this is the most common error): | ||
| Cuff too narrow for extremity | Falsely high | Needs excessive pressure to occlude brachial artery |
| Cuff wrap is too loose or uneven, or bladder balloons out of wrap | Falsely high | Needs excessive pressure to occlude brachial artery |
| Failure to palpate radial artery while inflating: | ||
| Inflating not high enough | Falsely low systolic | Miss initial systolic tapping or may tune in during auscultatory gap (tapping sounds disappear for 10 to 40 mm Hg and then return; common with hypertension) |
| Inflating cuff too high | Pain | |
| Pushing stethoscope too hard on brachial artery | Falsely low diastolic | Excessive pressure distorts artery and the sounds continue |
| Deflating cuff: | ||
| Too quickly | Falsely low systolic or falsely high diastolic | Insufficient time to hear tapping |
| Too slowly | Falsely high diastolic | Venous congestion in forearm makes sounds less audible |
| Halting during descent and reinflating cuff to recheck systolic | Falsely high diastolic | Venous congestion in forearm |
| Failure to wait 1-2 min before repeating entire reading | Falsely high diastolic | Venous congestion in forearm |
| Any observer error: | ||
| Examiner’s “subconscious bias”; a preconceived idea of what blood pressure reading should be due to person’s age, race, gender, weight, history, or condition | Error anywhere | |
| Examiner’s haste Faulty technique Examiner’s digit preference, “hears” more results that end in zero than would occur by chance alone (e.g., 130/80) Diminished hearing acuity Defective or inaccurately calibrated equipment |
Error anywhere |
 Culture and genetics
Culture and genetics
General Appearance
Genetic differences are found in the body proportions of individuals. In general, white males are 1.27 cm (0.5 in) taller than Black males, whereas white women and Black women are, on the average, the same height. Sitting-to-standing height ratios reveal that Blacks of both genders have longer legs and shorter trunks than whites.13 Because proportionately most of the weight is in the trunk, white men appear more obese than Black men. Asians are markedly shorter, weigh less, and have smaller body frames.
However, genes are not destiny. In the twentieth century, people grew taller in developed countries than they did in developing countries, largely because of environmental influences.1 This is most apparent among children of immigrants1:
Japanese-born men living in Japan are shorter than those living in Hawaii, and shorter still than those living in California, and Hawaiian-born children of Japanese immigrants were significantly taller than their parents. Similarly, Guatemala Mayan refugee children born in the United States were significantly taller than their peers born in Guatemala or in Mexico en route to the United States. In total, Mayan children growing up in the United States are on average 5.5 cm taller than their cohort remaining in Guatemala. In general, subsequent generations of children of immigrants tend to increase in stature until they attain the height of the host population.
Bone length, as revealed by stature, shows definite genetic differences, with Blacks having longer legs and arms than whites. Asians and American Indians have, on the average, proportionately longer trunks and shorter limbs than whites. Blacks tend to be wide shouldered and narrow hipped, whereas Asians tend to be wide hipped and narrow shouldered. Shoulder width is largely produced by the clavicle. Because the clavicle is a long bone, taller people have wide shoulders, whereas shorter people have narrower shoulders.
Obesity
Data from the most recent National Health and Nutrition Examination Survey (NHANES) show that 32.2% of U.S. adults are obese.28 Obesity rates by racial groups include 30% non-Hispanic white adults; 45% non-Hispanic Blacks; and 37% Mexican Americans. When studied by gender, among adult men, no differences in weight are found between racial/ethnic groups. However, Mexican American and non-Hispanic Black women are significantly more likely to be obese than non-Hispanic white women. Trends in children over the past 30 years show that Black children have had larger increases in BMI, weight, and height than white children, with increases for Mexican American children in between.28 What causes the increase in obesity? Probably an interaction of biologic and social factors, but notably a U.S. environment with few opportunities for physical activity and an overabundance of high-calorie food.28
 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
A.J. is a 47-year-old Black female high school principal, who appears healthy and of her stated age. She is alert, oriented, cooperative, with no signs of pain or difficulty breathing. Ht 163 cm (5′4″), Wt 57 kg (126 lb), TPR 37° C - 76 - 14, BP 146/84 right arm, sitting.
Focused Assessment: Clinical Case Study*
Mrs. Grazia Sanchez is a 76-year-old Hispanic female retired secretary, in previous good health, who is brought to the emergency department by her 83-year-old husband. They have both been ill during the night with nausea, vomiting, abdominal pain, and diarrhea, which they attribute to eating “bad food” at a buffet-style restaurant the night before. Mr. Sanchez’s condition has improved during the next day, but Mrs. Sanchez is worse, with severe vomiting, diarrhea, weakness, dizziness, and abdominal pain.
Subjective
Extreme fatigue. Weakness and dizziness occur whenever patient tries to sit or stand up: “Feels like I’m going to black out.” Severe nausea and vomiting, thirsty but cannot keep anything down; even sips of water result in “dry heaves.” Abdominal pain is moderate aching, intermittent. Diarrhea is watery brown stool, profuse during the night, somewhat diminished now.
Objective
Vital signs: Temp 99° F; BP (supine) 102/64 mm Hg; pulse (supine) 70, regular rhythm; respirations 18.
Helped to seated, leg-dangling position; vitals: BP 74/52 mm Hg; pulse 138, regular rhythm; respirations 20. Skin pale and moist (diaphoretic).
Reports light-headed and dizzy in seated position. Returned to supine.
Respiratory: Breath sounds clear in all fields, no adventitious sounds.
Cardiovascular: Regular rate (70 bpm) and rhythm when supine, S1 and S2 are not accentuated or diminished, no extra sounds. All pulses present, 2+ and equal bilaterally. Carotids 2+ with no carotid bruit.
Abdomen: Bowel sounds hyperactive, skin pale and moist, abdomen soft and mildly tender to palpation. No enlargement of liver or spleen.
Neuro: Level of consciousness alert and oriented; pupils equal, round, react to light and accommodation. Sensory status normal. Mild weakness in arms and legs. Gait and standing leg strength not tested due to inability to stand. Deep tendon reflexes 2+ and equal bilaterally. Babinski reflex → down-going toes.
Assessment
Orthostatic hypotension, orthostatic pulse increase, and syncopal symptoms, R/T hypovolemia
Diarrhea, possibly R/T ingestion of contaminated food
Risk for hyperthermia, R/T dehydration and aging
Deficient fluid volume
Abnormal Findings
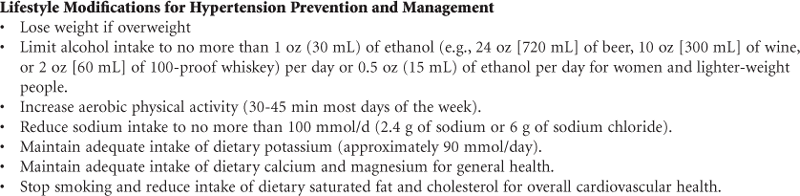
TABLE 9-6
Abnormalities in Blood Pressure
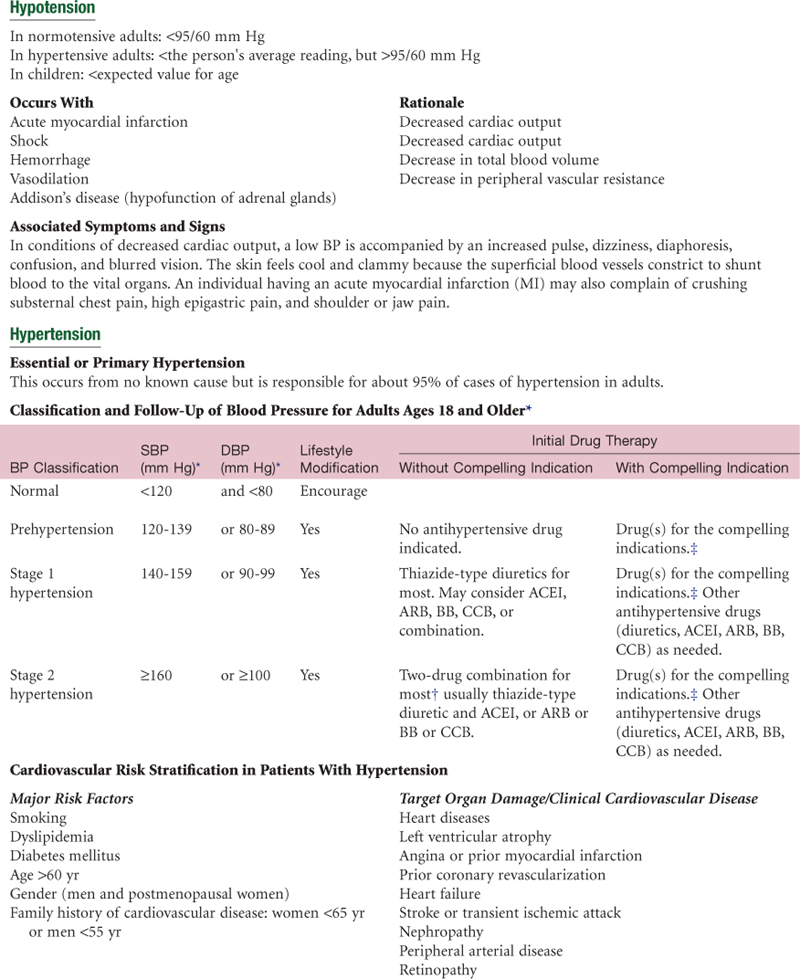
ACEI, Angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BB, beta-blocker; CCB, calcium channel blocker; DBP, diastolic blood pressure; SBP, systolic blood pressure.
*Treatment determined by highest BP category.
†Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension.
‡Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mm Hg.
Data on classification of hypertension in adults adapted from Chobanian, A. V., Bakris, G. L., Black, H. R., et al: National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. (2003). The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. The Journal of the American Medical Association, 289(19):2560-2572; www.nhlbi.nih.gov/guidelines/hypertension.
Bibliography
1. Beard AS, Blaser MJ. The ecology of height: the effect of microbial transmission on human height. Perspectives in Biology and Medicine. 2002;45(4):475–498.
2. Canzanello VJ, Jensen PL, Schwartz GL. Are aneroid sphygmomanometers accurate in hospital and clinic settings? Archives of Internal Medicine. 2001;161(5):729–731.
3. Centers for Disease Control and Prevention. Growth charts. National Center for Health Statistics in collaboration with the National Center for Chronic Disease Prevention and Health Promotion. Retrieved June 17, 2009, from www.cdc.gov/growth_charts; 2000.
4. Chobanian AV, Bakris GL, Black HR, et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee (2003) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure: The JNC 7 Report. JAMA. 2003;289(19):2560–2572.
5. Craig JV, Lancaster GA, Taylor S. Infrared ear thermometry compared with rectal thermometry in children: a systematic review. Lancet. 2002;360(9333):603–609.
6. Cusson RM, Madonia JA, Taekmen JB. The effect of environment on body site temperatures in full-term neonates. Nursing Research. 1997;46(4):202–207.
7. DeMeulenaere S. Pulse oximetry: uses and limitations. The Journal for Nurse Practitioners. 2007;3(5):312–317.
8. Falkenstern SK, Bauer LA. Helping kids grow. The Nurse Practitioner. 2009;34(3):31–41.
9. Fountain C, Goins L, Hartman M, et al. Evaluating the accuracy of four temperature instruments on an adult inpatient oncology unit. Clinical Journal of Oncology Nursing. 2008;12(6):983–987.
10. Freedman DS, Khan LK, Serdula MK, et al. Racial and ethnic differences in secular trends for childhood BMI, weight, and height. Obesity. 2006;14(2):301–307.
11. Frommelt T, Ott C, Hays V. Accuracy of different devices to measure temperature. Medsurg Nursing. 2008;17(3):171–176.
12. Gidding SS. Measuring children’s blood pressure matters. Circulation. 2008;117:3163–3164.
13. Gilsanz V, Skaggs DL, Kovanlikaya A, et al. Differential effect of race on the axial and appendicular skeletons of children. The Journal of Clinical Endocrinology and Metabolism. 1998;83(5):1420–1427.
14. Hwu Y, Coates VE, Lin F. A study of the effectiveness of different measuring times and counting methods of human radial pulse rates. Journal of Clinical Nursing. 2000;9(1):146–152.
15. Jarosz PA, Bellar A. Age-appropriate obesity treatment. The Nurse Practitioner. 2008;33(5):24–32.
16. Jean-Mary MB, DiCanzio J, Shaw J, et al. Limited accuracy and reliability of infrared axillary and aural thermometers in a pediatric outpatient population. The Journal of Pediatrics. 2002;141(5):671–676.
17. Keele-Smith R, Price-Daniel C. Effects of crossing legs on blood pressure measurement. Clinical Nursing Research. 2001;10(2):202–213.
18. Kiekkas P, Brokalaki H. Physical antipyresis in critically ill adults. The American Journal of Nursing. 2008;108(7):40–50.
19. Kimbro RT, Brooks-Gunn J, McLanahan S. Racial and ethnic differentials in overweight and obesity among 3-year-old children. American Journal of Public Health. 2007;97(2):298–305.
20. Lawson L, Bridges EJ, Ballou I, et al. Accuracy and precision of noninvasive temperature measurement in adult intensive care patients. American Journal of Critical Care. 2007;16(5):485–496.
21. Lewis CE, McTigue KM, Burke LE, et al. Mortality, health outcomes, and body mass index in the overweight range. Circulation. 2009;119(25):3263.
22. Lipman TH, McGinley A, Hughes J. Evaluation of the accuracy of height assessment of premenopausal and menopausal women. Journal of Obstetric, Gynecologic, and Neonatal Nursing. 2006;35:516–522.
23. Mitsnefes MM. Hypertension in children and adolescents. Pediatric Clinics of North America. 2006;53(3):493–512.
24. Moore J. Hypertension: catching the silent killer. The Nurse Practitioner. 2005;30(10):16–35.
25. National High Blood Pressure Education Program (NHBPEP). Working Group on High Blood Pressure in Children and Adolescents The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics. 2004;114(2):555–576.
26. National Institutes of Health (NIH). The practical guide to identification, evaluation, and treatment of overweight and obesity in adults. Retrieved June 10, 2009, from www.nhlbi.nih.gov/guidelines/obesity/ob_home_htm; 2000.
27. Nimah MM, Bshesh K, Callahann JD, et al. Infrared tympanic thermometry in comparison with other temperature measurement techniques in febrile children. Pediatric Critical Care Medicine. 2006;7(1):48–55.
28. Ogden CL, Ogden CL, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA: The Journal of the American Medical Association. 2006;295(13):1549–1555.
29. Pesola GR, Pesola HR, Nelson MJ, et al. The normal difference in bilateral indirect blood pressure recordings in normotensive individuals. The American Journal of Emergency Medicine. 2001;19(1):43–45.
30. Pickering TG, Hall JE, Appel LJ, et al. Blood pressure measurement in humans. Hypertension. 2005;45:142–161.
31. Quatrara B, Coffman J, Jenkins T, et al. The effect of respiratory rate and ingestion of hot and cold beverages on the accuracy of oral temperatures measured by electronic thermometers. Medsurg Nursing. 2007;16(2):105–108.
32. Schell KA. Evidence-based practice: noninvasive blood pressure measurement in children. Pediatric Nursing. 2006;32(3):263–267.
33. Schell K, Lyons D, Bradley E, et al. Clinical comparison of autonomic, noninvasive measurements of blood pressure in the forearm and upper arm with the patient supine or with the head of the bed raised 45 degrees: a follow-up study. American Journal of Critical Care. 2006;15(2):196–205.
34. Spodick DH. Normal sinus heart rate: appropriate rate thresholds for sinus tachycardia and bradycardia. Southern Medical Journal. 1996;89(7):666–667.
35. Todd B. Clostridium difficile: familiar pathogen, changing epidemiology. The American Journal of Nursing. 2006;106(5):33–36.
*Please note that space does not allow a detailed plan for each clinical case study in this text. Please consult the appropriate text for current treatment plan.