Skin, Hair, and Nails

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
Structure and Function
Think of the skin as the body’s largest organ system—it covers 20 square feet of surface area in the average adult. The skin is the sentry that guards the body from environmental stresses (e.g., trauma, pathogens, dirt) and adapts it to other environmental influences (e.g., heat, cold).
Skin
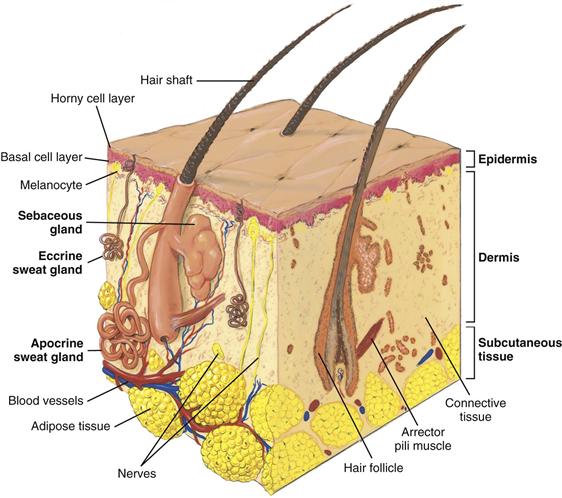
The skin has two layers—the outer, highly differentiated epidermis and the inner, supportive dermis (Fig. 12-1). Beneath these layers is a third layer, the subcutaneous layer of adipose tissue.
12-1
Epidermis
The epidermis is thin but tough. Its cells are bound tightly together into sheets that form a rugged protective barrier. It is stratified into several zones. The inner basal cell layer forms new skin cells. Their major ingredient is the tough, fibrous protein keratin. The melanocytes interspersed along this layer produce the pigment melanin, which gives brown tones to the skin and hair. All people have the same number of melanocytes; however, the amount of melanin they produce varies with genetic, hormonal, and environmental influences.
From the basal layer the new cells migrate up and flatten into the outer horny cell layer. This consists of dead keratinized cells that are interwoven and closely packed. The cells are constantly being shed, or desquamated, and are replaced with new cells from below. The epidermis is completely replaced every 4 weeks. In fact, each person sheds about 1 pound of skin each year.
The epidermis is uniformly thin except on the surfaces that are exposed to friction, such as the palms and the soles. On these surfaces, skin is thicker because of work and weight bearing. The epidermis is avascular; it is nourished by blood vessels in the dermis below.
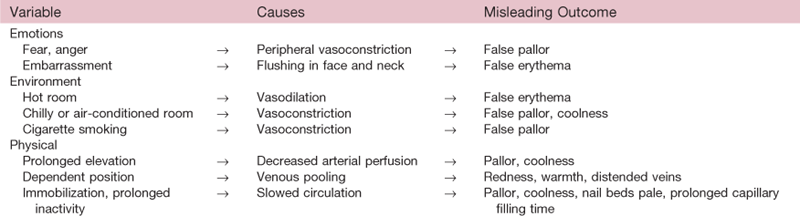
Skin color is derived from three sources: (1) mainly from the brown pigment melanin, (2) also from the yellow-orange tones of the pigment carotene, and (3) from the red-purple tones in the underlying vascular bed. All people have skin of varying shades of brown, yellow, and red; the relative proportion of these shades affects the prevailing color. Skin color is further modified by the thickness of the skin and by the presence of edema.
Dermis
The dermis is the inner supportive layer consisting mostly of connective tissue, or collagen. This is the tough, fibrous protein that enables the skin to resist tearing. The dermis also has resilient elastic tissue that allows the skin to stretch with body movements. The nerves, sensory receptors, blood vessels, and lymphatics lie in the dermis. Also, appendages from the epidermis—such as the hair follicles, sebaceous glands, and sweat glands—are embedded in the dermis.
Subcutaneous Layer
The subcutaneous layer is adipose tissue, which is made up of lobules of fat cells. The subcutaneous tissue stores fat for energy, provides insulation for temperature control, and aids in protection by its soft cushioning effect. Also, the loose subcutaneous layer gives skin its increased mobility over structures underneath.
Epidermal Appendages
These structures are formed by a tubular invagination of the epidermis down into the underlying dermis.
Hair
Hair is vestigial for humans; it no longer is needed for protection from cold or trauma. However, hair is highly significant in most cultures for its cosmetic and psychological meaning (see Culture and Genetics, p. 206).
Hairs are threads of keratin. The hair shaft is the visible projecting part, and the root is below the surface embedded in the follicle. At the root the bulb matrix is the expanded area where new cells are produced at a high rate. Hair growth is cyclical, with active and resting phases. Each follicle functions independently so that while some hairs are resting, others are growing. Around the hair follicle are the muscular arrector pili, which contract and elevate the hair so that it resembles “goose flesh” when the skin is exposed to cold or in emotional states.
People have two types of hair. Fine, faint vellus hair covers most of the body (except the palms and soles, the dorsa of the distal parts of the fingers, the umbilicus, the glans penis, and inside the labia). The other type is terminal hair, the darker, thicker hair that grows on the scalp and eyebrows and, after puberty, on the axillae, the pubic area, and the face and chest in the male.
Sebaceous Glands
These glands produce a protective lipid substance, sebum, which is secreted through the hair follicles. Sebum oils and lubricates the skin and hair and forms an emulsion with water that retards water loss from the skin. (Dry skin results from loss of water, not directly from loss of oil.) Sebaceous glands are everywhere except on the palms and soles. They are most abundant in the scalp, forehead, face, and chin.
Sweat Glands
There are two types of sweat glands. The eccrine glands are coiled tubules that open directly onto the skin surface and produce a dilute saline solution called sweat. The evaporation of sweat reduces body temperature. Eccrine glands are widely distributed through the body and are mature in the 2-month-old infant.
The apocrine glands produce a thick, milky secretion and open into the hair follicles. They are located mainly in the axillae, anogenital area, nipples, and navel and are vestigial in humans. They become active during puberty, and secretion occurs with emotional and sexual stimulation. Bacterial flora residing on the skin surface react with apocrine sweat to produce a characteristic musky body odor. The functioning of apocrine glands decreases in the aging adult.
Nails
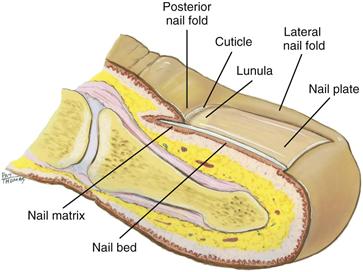
The nails are hard plates of keratin on the dorsal edges of the fingers and toes (Fig. 12-2). The nail plate is clear, with fine longitudinal ridges that become prominent in aging. Nails take their pink color from the underlying nail bed of highly vascular epithelial cells. The lunula is the white, opaque, semilunar area at the proximal end of the nail. It lies over the nail matrix where new keratinized cells are formed. The nail folds overlap the posterior and lateral borders. The cuticle works like a gasket to cover and protect the nail matrix.
12-2
Function of the Skin
The skin is a waterproof, almost indestructible, covering that has protective and adaptive properties:
• Protection. Skin minimizes injury from physical, chemical, thermal, and light-wave sources.
• Prevents penetration. Skin is a barrier that stops invasion of microorganisms and loss of water and electrolytes from within the body.
• Perception. Skin is a vast sensory surface holding the neurosensory end-organs for touch, pain, temperature, and pressure.
• Temperature regulation. Skin allows heat dissipation through sweat glands and heat storage through subcutaneous insulation.
• Identification. People identify one another by unique combinations of facial characteristics, hair, skin color, and even fingerprints. Self-image is often enhanced or deterred by the way society’s standards of beauty measure up to each person’s perceived characteristics.
• Communication. Emotions are expressed in the sign language of the face and in the body posture. Vascular mechanisms such as blushing or blanching also signal emotional states.
• Wound repair. Skin allows cell replacement of surface wounds.
• Absorption and excretion. Skin allows limited excretion of some metabolic wastes, byproducts of cellular decomposition such as minerals, sugars, amino acids, cholesterol, uric acid, and urea.
• Production of vitamin D. The skin is the surface on which ultraviolet light converts cholesterol into vitamin D.
 Developmental Competence
Developmental Competence
Infants and Children
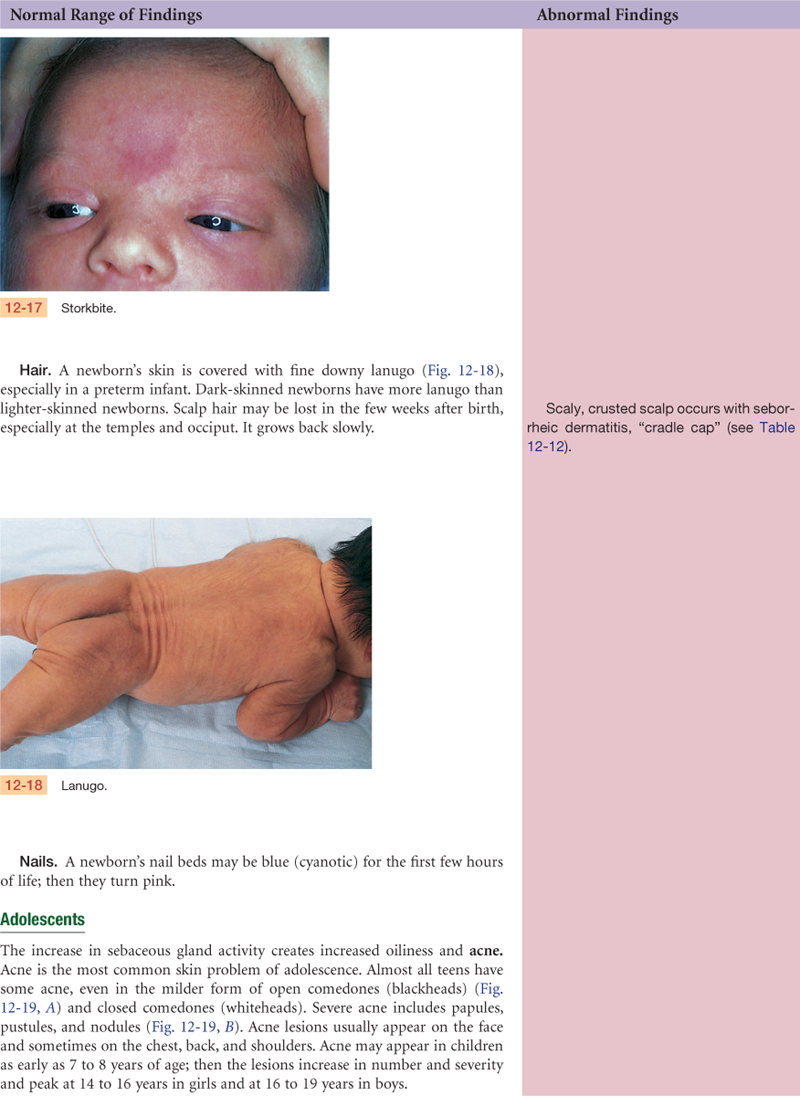
The hair follicles develop in the fetus at 3 months’ gestation; by midgestation, most of the skin is covered with lanugo, the fine downy hair of the newborn infant. In the first few months after birth, this is replaced by fine vellus hair. Terminal hair on the scalp, if present at birth, tends to be soft and to suffer a patchy loss, especially at the temples and occiput. Also present at birth is vernix caseosa, the thick, cheesy substance made up of sebum and shed epithelial cells.
The newborn’s skin is similar in structure to the adult’s, but many of its functions are not fully developed. The newborn’s skin is thin, smooth, and elastic and is relatively more permeable than that of the adult, so the infant is at greater risk for fluid loss. Sebum, which holds water in the skin, is present for the first few weeks of life, producing milia (see p. 222) and cradle cap in some babies. Then sebaceous glands decrease in size and production and do not resume functioning until puberty. Temperature regulation is ineffective. Eccrine sweat glands do not secrete in response to heat until the first few months of life and then only minimally throughout childhood. The skin cannot protect much against cold because it cannot contract and shiver and because the subcutaneous layer is inefficient. Also, the pigment system is inefficient at birth.
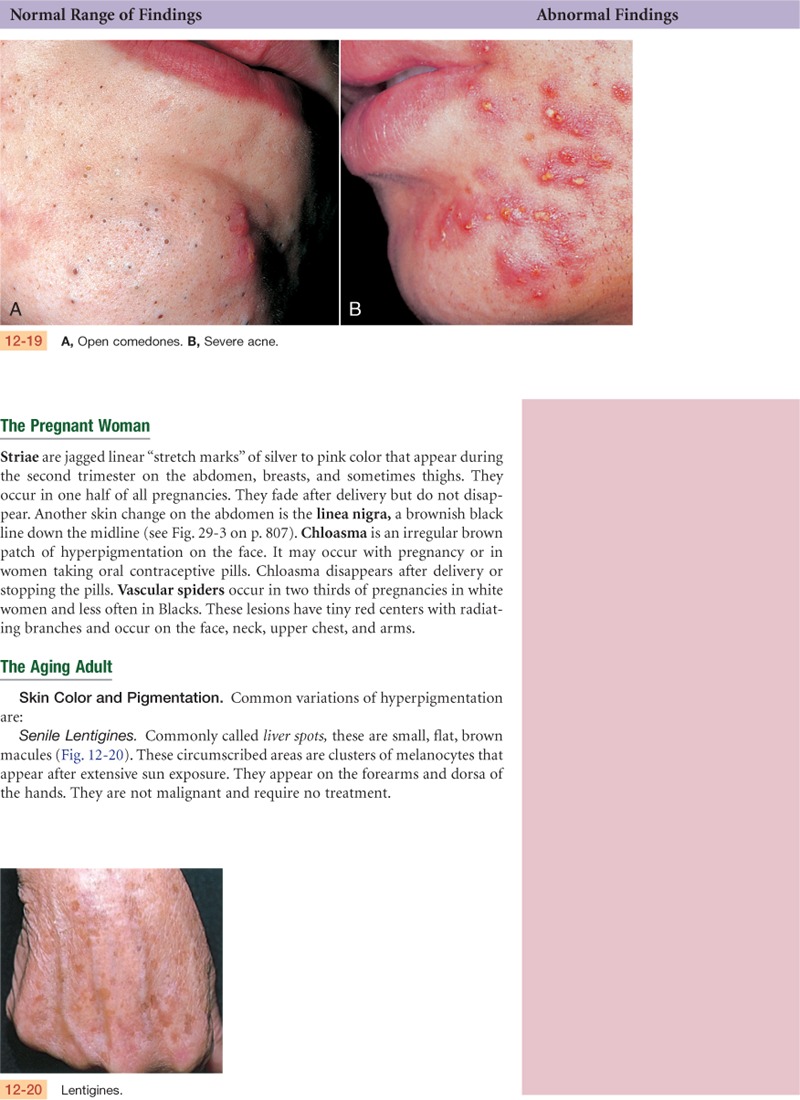
As the child grows, the epidermis thickens, toughens, and darkens and the skin becomes better lubricated. Hair growth accelerates. At puberty, secretion from apocrine sweat glands increases in response to heat and emotional stimuli, producing body odor. Sebaceous glands become more active—the skin looks oily, and acne develops. Subcutaneous fat deposits increase, especially in females.
Secondary sex characteristics that appear during adolescence are evident in the integument (i.e., skin). In the female, the diameter of the areola enlarges and darkens and breast tissue develops. Coarse pubic hair develops in males and females, then axillary hair, and then coarse facial hair in males.
The Pregnant Woman
The change in hormone levels results in increased pigment in the areolae and nipples, vulva, and sometimes in the midline of the abdomen (linea nigra) or in the face (chloasma). Hyperestrogenemia probably also causes the common vascular spiders and palmar erythema. Connective tissue develops increased fragility, resulting in striae gravidarum (stretch marks), which may develop in the skin of the abdomen, breasts, or thighs. Metabolism is increased in pregnancy; as a way to dissipate heat, the peripheral vasculature dilates and the sweat and sebaceous glands increase secretion. Fat deposits are laid down, particularly in the buttocks and hips, as maternal reserves for the nursing baby.
The Aging Adult
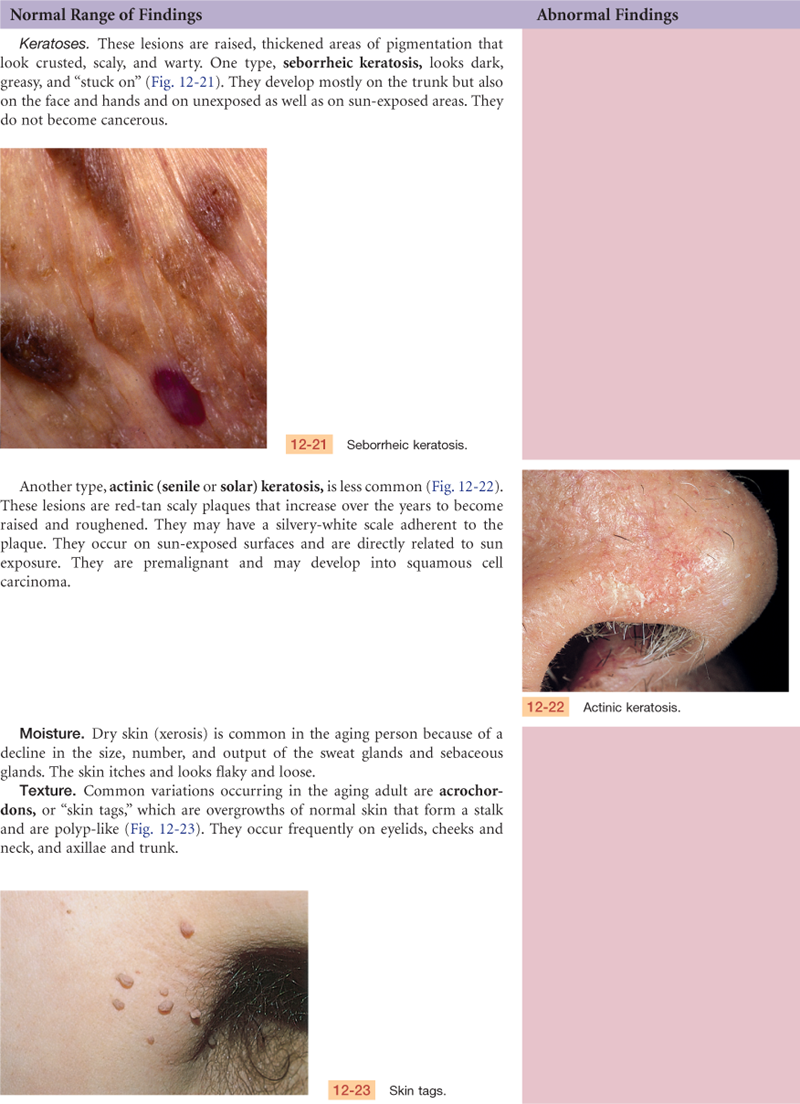
The skin is a mirror that reflects aging changes that proceed in all our organ systems; it just happens to be the one organ we can view directly. The aging process carries a slow atrophy of skin structures. The aging skin loses its elasticity; it folds and sags. By the 70s to 80s, it looks parchment thin, lax, dry, and wrinkled.
The epidermis’s outer layer thins and flattens. This allows chemicals easier access into the body. Wrinkling occurs because the underlying dermis thins and flattens. A loss of elastin, collagen, and subcutaneous fat occurs as well as a reduction in muscle tone. The loss of collagen increases the risk for shearing, tearing injuries.
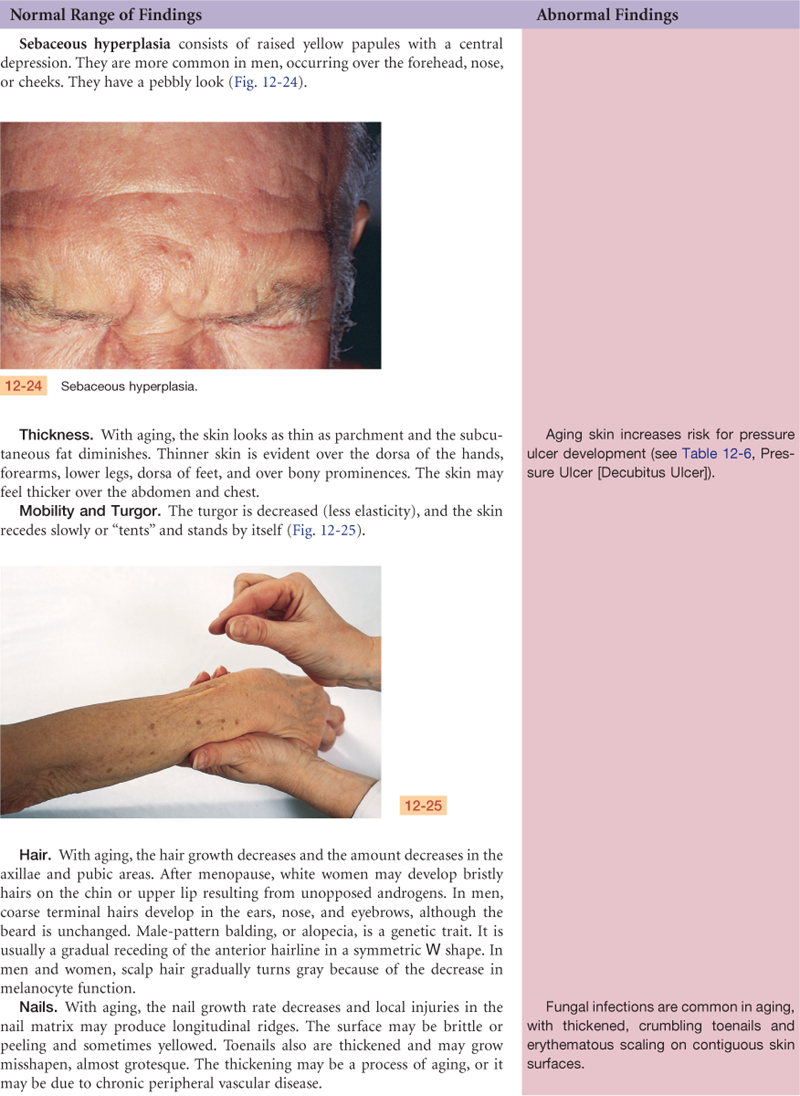
Sweat glands and sebaceous glands decrease in number and function, leaving dry skin. Decreased response of the sweat glands to thermoregulatory demand also puts the aging person at greater risk for heat stroke. The vascularity of the skin diminishes while the vascular fragility increases; a minor trauma may produce dark red discolored areas, or senile purpura.
Sun exposure and cigarette smoking further accentuate aging changes in the skin. Coarse wrinkling, decreased elasticity, atrophy, speckled and uneven coloring, more pigment changes, and a yellowed, leathery texture occur. Chronic sun damage is even more prominent in pale or light-skinned persons.
An accumulation of factors place the aging person at risk for skin disease and breakdown: the thinning of the skin, the decrease in vascularity and nutrients, the loss of protective cushioning of the subcutaneous layer, a lifetime of environmental trauma to skin, the social changes of aging (e.g., less nutrition, limited financial resources), the increasingly sedentary lifestyle, and the chance of immobility. When skin breakdown does occur, subsequent cell replacement is slower and wound healing is delayed.
In the aging hair matrix, the number of functioning melanocytes decreases, so the hair looks gray or white and feels thin and fine. A person’s genetic script determines the onset of graying and the number of gray hairs. Hair distribution changes. Males may have a symmetric W-shaped balding in the frontal areas. Some testosterone is present in both males and females; as it decreases with age, axillary and pubic hair decrease. As the female’s estrogen also decreases, testosterone is unopposed and the female may have some bristly facial hairs. Nails grow more slowly. Their surface is lusterless and is characterized by longitudinal ridges resulting from local trauma at the nail matrix.
Because the aging changes in the skin and hair can be viewed directly, they carry a profound psychological impact. For many people, self-esteem is linked to a youthful appearance. This view is compounded by media advertising in Western society. Although sagging and wrinkling skin and graying and thinning hair are normal processes of aging, they prompt a loss of self-esteem for many adults.
 Culture and genetics
Culture and genetics
Awareness of normal biocultural differences and the ability to recognize the unique clinical manifestations of disease are especially important for darkly pigmented people. As described earlier, melanin is responsible for the various colors and tones of skin observed among people. Melanin protects the skin against harmful ultraviolet rays, a genetic advantage accounting for the lower incidence of skin cancer among darkly pigmented Blacks and American Indians. The incidence of melanoma is 20 times higher among whites than among Blacks and 4 times higher among whites than among Hispanics.25
The apocrine and eccrine sweat glands are important for fluid balance and for thermoregulation. When apocrine gland secretions are contaminated by normal skin flora, odor results. Most Asians and American Indians have a mild body odor or none at all, whereas whites and Blacks tend to have strong body odor. The amount of chloride excreted by sweat glands varies widely, and Blacks have lower salt concentrations in their sweat than whites do.
In Arctic regions, Inuits have made an interesting environmental adaptation; they sweat less than whites on their trunks and extremities but more on their faces. This adaptation allows for temperature regulation without causing perspiration and dampness of their clothes, which would decrease their ability to insulate against severe cold weather and would pose a serious threat to their survival.
There are several skin conditions found among Blacks:
1. Keloids—scars that form at the site of a wound and grow beyond the normal boundaries of the wound (see p. 235)
2. Areas of either postinflammatory hypopigmentation or hyperpigmentation that appear as dark or light spots
3. Pseudofolliculitis—“razor bumps” or “ingrown hairs” caused by shaving too closely with an electric razor or straight razor
4. Melasma—the “mask of pregnancy,” a patchy tan to dark brown discoloration of the face
Perhaps one of the most obvious and widely variable racial differences occurs with the hair. The hair of Blacks varies widely in texture. It is very fragile and ranges from long and straight to short, spiraled, thick, and kinky. The hair and scalp have a natural tendency to be dry and require daily combing, gentle brushing, and the application of oil. Hair care products designed to care specifically for kinky hair should be available in clinical settings. In comparison, people of Asian backgrounds generally have straight, silky hair.
Hair condition is significant in diagnosing and treating certain disease states. For example, hair texture becomes dry, brittle, and lusterless with inadequate nutrition. The hair of Black children with severe malnutrition (e.g., marasmus) frequently changes not only in texture but also in color. The child’s hair often becomes less kinky and assumes a copper-red color.
Subjective Data
1. Past history of skin disease (allergies, hives, psoriasis, eczema)
3. Change in mole (size or color)
4. Excessive dryness or moisture
| Examiner Asks | Rationale |
| 1. Past history of skin disease. Any past skin disease or problem? • How was this treated? • Any family history of allergies or allergic skin problem? | Significant familial predisposition: allergies, hay fever, psoriasis, atopic dermatitis (eczema), acne. |
| • Any known allergies to drugs, plants, animals? | Identify offending allergen. |
| • Any birthmarks, tattoos? | Use of nonsterile equipment to apply tattoos increases risk for hepatitis C. |
| 2. Change in pigmentation. Any change in skin color or pigmentation? | Hypopigmentation (loss of color); hyperpigmentation (increase in color). |
| • A generalized color change (all over), or localized? | Generalized change suggests systemic illness: pallor, jaundice, cyanosis. |
| 3. Change in mole. Any change in a mole: color, size, shape, sudden appearance of tenderness, bleeding, itching? • Any “sores” that do not heal? | Signs suggest neoplasm in pigmented nevus. May be unaware of change in nevus on back or buttocks that he or she cannot see. |
| 4. Excessive dryness or moisture. Any change in the feel of your skin: temperature, moisture, texture? | Seborrhea—oily. |
| • Any excess dryness? Is this seasonal or constant? | Xerosis—dry. |
| 5. Pruritus. Any skin itching? Is this mild (prickling, tingling) or intense (intolerable)? • Does it awaken you from sleep? | Pruritus is the most common skin symptom; occurs with dry skin, aging, drug reactions, allergy, obstructive jaundice, uremia, lice. |
| • Where is the itching? When did it start? | Presence or absence of pruritus helps diagnosis. Scratching causes excoriation of primary lesion. |
| • Any other skin pain or soreness? Where? | |
| 6. Excessive bruising. Any excess bruising? Where on the body? • How did this happen? • How long have you had it? | Multiple cuts and bruises, bruises in various stages of healing, bruises above knees and elbows, and illogical explanation—consider physical abuse. Frequent falls may be due to dizziness of neurologic or cardiovascular origin. Also, frequent minor trauma may be a side effect of alcoholism or other drug abuse. |
| 7. Rash or lesion. Any skin rash or lesion? • Onset. When did you first notice it? | Rashes are a common cause of seeking health care. A careful history is important; it may predict the type of lesion you will see in the examination and its cause. |
| • Location. Where did it start? | Identify the primary site—it may give clue to cause. |
| • Where did it spread? • Character or quality. Describe the color. • Is it raised or flat? Any crust, odor? Does it feel tender, warm? • Duration. How long have you had it? | Migration pattern, evolution. |
| • Setting. Anyone at home or work with a similar rash? Have you been camping, acquired a new pet, tried a new food, drug? Does the rash seem to come with stress? | Identify new or relevant exposure, any household or social contacts with similar symptoms. |
| • Alleviating and aggravating factors. What home care have you tried? Bath, lotions, heat? Do they help, or make it worse? • Associated symptoms. Any itching, fever? | Myriad over-the-counter remedies are available. People try them and seek professional help only when they do not work. |
| • What do you think rash/lesion means? | Assess person’s perception of cause: fear of cancer, tick-borne illnesses, or sexually transmitted infections. |
| • Coping strategies. How has rash/lesion affected your self-care, hygiene, ability to function at work/home/socially? | Assess effectiveness of coping strategies. Chronic skin diseases may increase risk for loss of self-esteem, social isolation, and anxiety. |
| • Any new or increased stress in your life? | Stress can exacerbate chronic skin illness. |
| 8. Medications. What medications do you take? • Prescription and over-the-counter? • Recent change? | Drugs may cause allergic skin eruption: aspirin, antibiotics, barbiturates, some tonics. Drugs may increase sunlight sensitivity and give burn response: sulfonamides, thiazide diuretics, oral hypoglycemic agents, and tetracycline. Drugs can cause hyperpigmentation: antimalarials, antineoplastic agents, hormones, metals, tetracycline. |
| • How long on medication? | Even after a long time on medication, a person may develop sensitivity. |
| 9. Hair loss. Any recent hair loss? • A gradual or sudden onset? Symmetric? Associated with fever, illness, increased stress? | Alopecia is a significant loss. A full head of hair equates with vitality in many cultures. If treated as a trivial problem, the person may seek alternative, unproven methods of treatment. |
| • Any unusual hair growth? • Any recent change in texture, appearance? | Hirsutism is shaggy or excessive hair. |
| 10. Change in nails. Any change in nails: shape, color, brittleness? Do you tend to bite or chew nails? | |
| 11. Environmental or occupational hazards. Any environmental or occupational hazards? | Majority of skin neoplasms result from occupational or environmental agents. |
| • With your occupation, such as dyes, toxic chemicals, radiation? • How about hobbies? Do you perform any household or furniture repair work? | People at risk: outdoor sports enthusiasts, farmers, sailors, outdoor workers; also creosote workers, roofers, coal workers. |
| • How much sun exposure do you get from outdoor work, leisure activities, sunbathing, tanning salons? | Unprotected sun exposure accelerates aging and produces lesions. At more risk: light-skinned people, those older than 40 years, and those regularly in sun. |
| • Recently been bitten by insect: bee, tick, mosquito? | Identify contactants that produce lesions or contact dermatitis. |
| • Any recent exposure to plants, animals in yard work, camping? | Tell people with chronic recurrent urticaria (hives) to keep diary of meals and environment to identify precipitating factors. |
| 12. Self-care behaviors. What do you do to care for your skin, hair, nails? What cosmetics, soaps, chemicals do you use? • Clip cuticles on nails, use adhesive for false fingernails? | Assess self-care and influence on self-concept—may be important with this society’s media stress on high norms of beauty. Many over-the-counter remedies are costly and exacerbate skin problems. |
| • If you have allergies, how do you control your environment to minimize exposure? | |
| • Do you perform a skin self-examination? | |
| Additional History for Infants and Children | |
| 1. Does the child have any birthmarks? | |
| 2. Was there any change in skin color as a newborn? | |
| • Any jaundice? Which day after birth? | Physiologic jaundice, see p. 222. |
| • Any cyanosis? What were the circumstances? | |
| 3. Have you noted any rash or sores? What seems to bring it on? • Have you introduced a new food or formula? When? Does your child eat chocolate, cow’s milk, eggs? |
Generalized rash—consider allergic reaction to new food. Irritability and general fussiness may indicate the presence of pruritus. |
| 4. Does the child have any diaper rash? How do you care for this? How do you wash diapers? How often do you change diapers? How do you clean skin? | Occlusive diapers or infrequent changing may cause rash. Infant may be allergic to certain detergent or to disposable wipes. |
| 5. Does the child have any burns or bruises? • Where? • How did it happen? |
A careful history can distinguish expected childhood bumps and bruises from any lesion that indicates child abuse or neglect: cigarette burns; excessive bruising, especially above knees or elbows; linear whip marks. With abuse, the history often will not coincide with the physical appearance and location of lesion. |
| 6. Has the child had any exposure to contagious skin conditions: scabies, impetigo, lice? Or to communicable diseases: measles, chickenpox, scarlet fever? Or to toxic plants: poison ivy? | |
| • Are the child’s vaccinations up-to-date? | |
| 7. Does the child have any habits or habitual movements, such as nail-biting, twisting hair, rubbing head on mattress? | |
| 8. What steps are taken to protect the child from sun exposure? What about sunscreens and sunblocks? How do you treat a sunburn? | Excessive sun exposure, especially severe or blistering sunburns in childhood, increases risk for melanoma in later life.9 |
| Additional History for the Adolescent | |
| 1. Have you noticed any skin problems such as pimples, blackheads? • How long have you had them? • How do you treat this? • How do you feel about it? |
About 70% of teens will have acne; the psychological effect is more significant than the physical effect. Self-treatment is common. Many myths surround the cause. Cause is unknown; acne is not caused by poor diet, oily complexion, or contagion. |
| Additional History for the Aging Adult | |
| 1. What changes have you noticed in your skin in the past few years? | Assess impact of aging on self-concept. Normal aging changes may cause distress. Many “aging” changes are due to chronic sun damage. Most skin cancers appear in aging people, although sun damage begins decades earlier. |
| 2. Any delay in wound healing? • Any skin itching? |
Pruritus is common with aging. Consider side effects of medicine or systemic disease (e.g., liver or kidney disease, cancer, lymphoma), but senile pruritus is usually due to dry skin (xerosis). Exacerbated by too-frequent bathing or use of soap. Scratching with dirty, jagged fingernails produces excoriations. |
| 3. Any other skin pain? | Some diseases, such as herpes zoster (shingles), produce more intense sensations of pain, itching in aging people. Other diseases (e.g., diabetes) may reduce pain sensation in extremities. Also, some aging people tolerate chronic pain as “part of growing old” and hesitate to “complain.” |
| 4. Any change in feet, toenails? Any bunions? Is it possible to wear shoes? | Some aging people cannot reach down to their feet to give self-care. |
| 5. Do you fall frequently? | Multiple bruises, trauma from falls. |
| 6. Any history of diabetes, peripheral vascular disease? | Risk for skin lesions in feet or ankles. |
| 7. What do you do to care for your skin? | A bland lotion is important to retain moisture in aging skin. Dermatitis may ensue from certain cosmetics, creams, ointments, and dyes applied to achieve a youthful appearance. |
| Aging skin has a delayed inflammatory response when exposed to irritants. If the person is not alerted by warning signs (e.g., pruritus, redness), exposure may continue and dermatitis may ensue. |


 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
No history of skin disease; no present change in pigmentation or in nevi; no pruritus, bruising, rash, or lesions. On no medications. No work-related skin hazards. Uses sun block cream when outdoors.
Objective
Skin: Color tan-pink, even pigmentation, with no suspicious nevi. Warm to touch, dry, smooth, and even. Turgor good, no lesions.
Hair: Even distribution, thick texture, no lesions or pest inhabitants.
Nails: No clubbing or deformities. Nail beds pink with prompt capillary refill.
Assessment
Warm, dry, intact skin.
Focused Assessment: Clinical Case Study 1*
Ethan E. is a 3-year-old white male presenting with his mother, who seeks health care because of Ethan’s fever, fatigue, and rash of 3 days’ duration.
Subjective
2 weeks PTA (prior to arrival)—Ethan was playing with a child who was subsequently diagnosed as having chickenpox.
3 days PTA—mother reports fever 100° to 101° F and fatigue, irritability. That evening noted “tiny blisters” on chest and back.
1 day PTA—blisters on chest changed to white with scab on top. New eruption of blisters on shoulders, thighs, face. Intense itching and scratching.
Objective
Temp 38.0° C (100.4° F), P 110, R 24.
Skin: Generalized vesiculopustular rash covering face, trunk, upper arms, and thighs. Small vesicles on face, pustules and red-honey–colored crusts on trunk. Otherwise skin is warm and dry, turgor good.
Ears: Tympanic membranes pearl gray with landmarks intact. No discharge.
Mouth and throat: Mucosa dark pink, no lesions. Tonsils 1+, no exudate. No lymphadenopathy.
Heart: S1, S2 normal, not accentuated or diminished, no murmurs or extra sounds.
Lungs: Hyperresonant to percussion. Breath sounds clear, no adventitious sounds.
Assessment
Varicella
Impaired skin integrity R/T infection and scratching
Focused Assessment: Clinical Case Study 2
Myra G. is a 79-year-old white widowed retired college professor, in good health until recent hospitalization after a fall.
Problem List 1 Fractured right hip—hip replacement on 11/24
Subjective
11/27, Aching pain in left hip (nonoperative side).
Objective
Erosion 2 × 2 cm with surrounding erythema covering L ischium. Erosion is moist, no active bleeding. Area very warm and tender to touch.
Assessment
Pressure sore, L hip
Impaired skin integrity R/T immobility and pressure
Acute pain
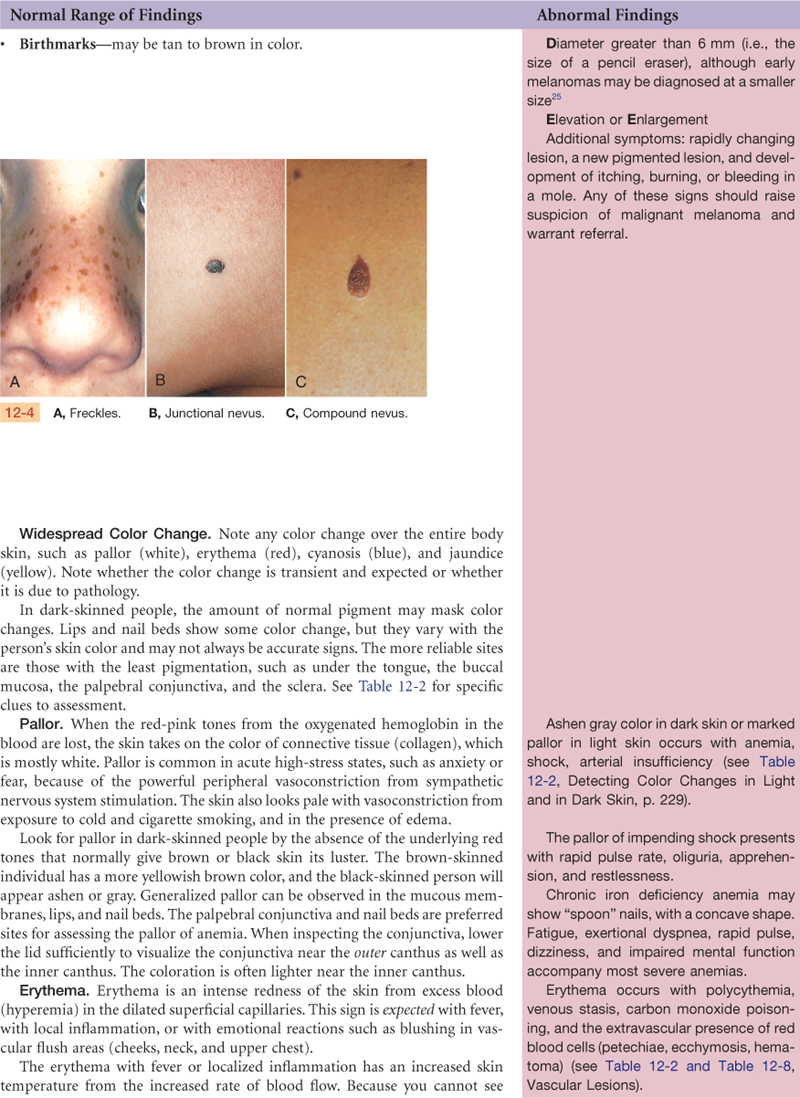
Abnormal Findings
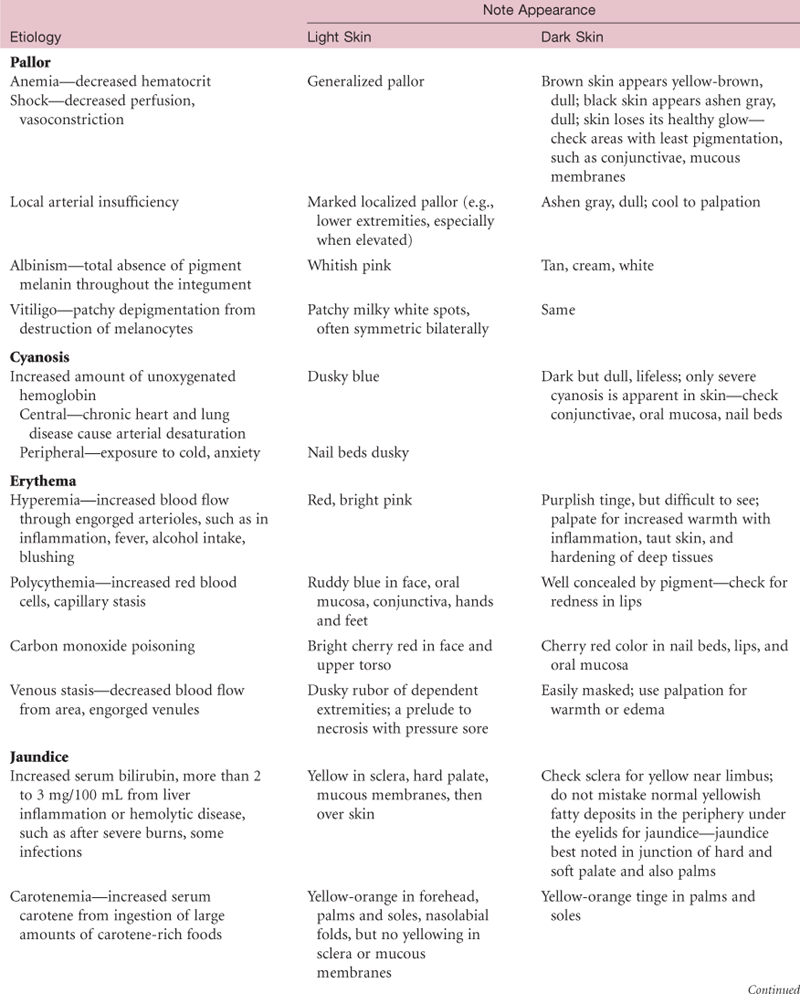
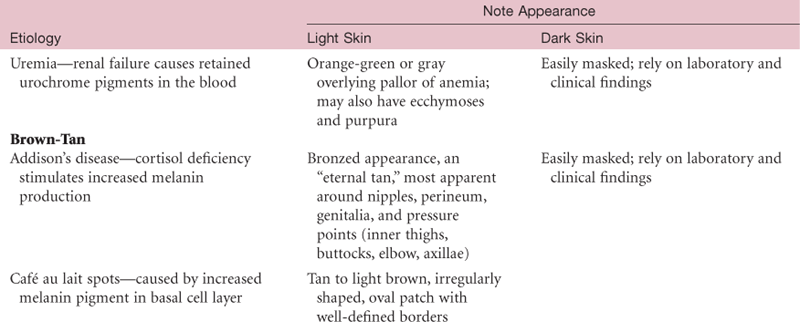
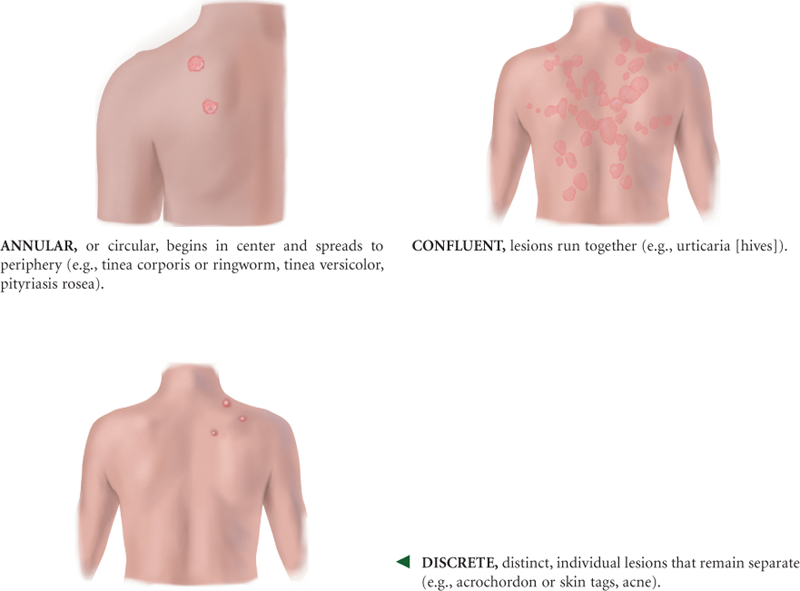
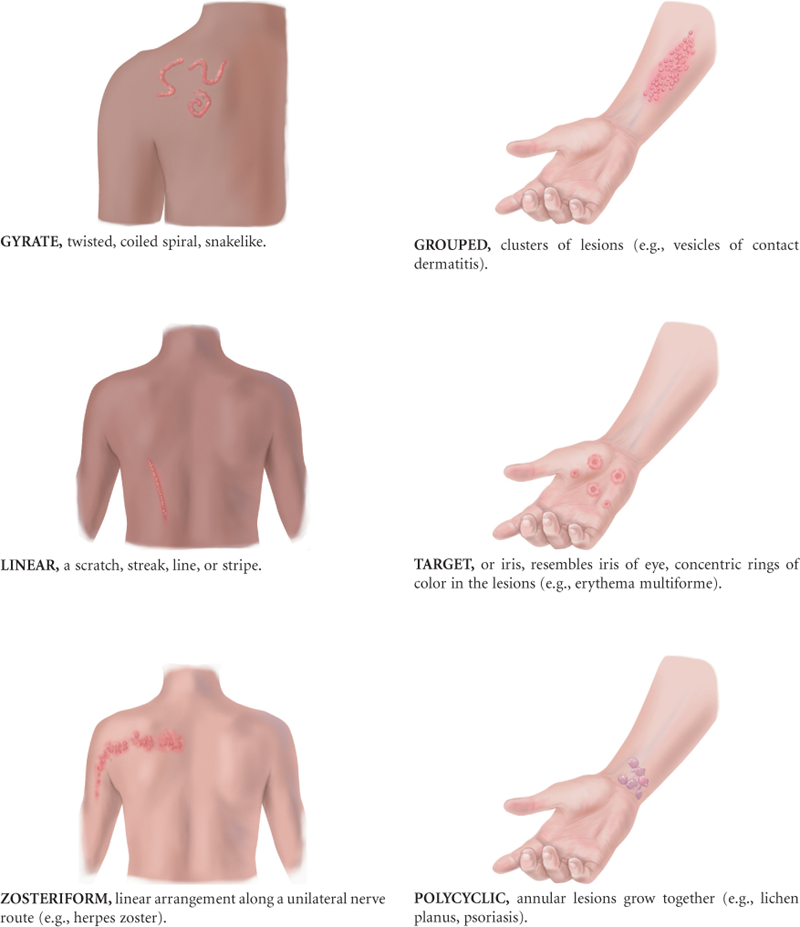
TABLE 12-4
Primary Skin Lesions*
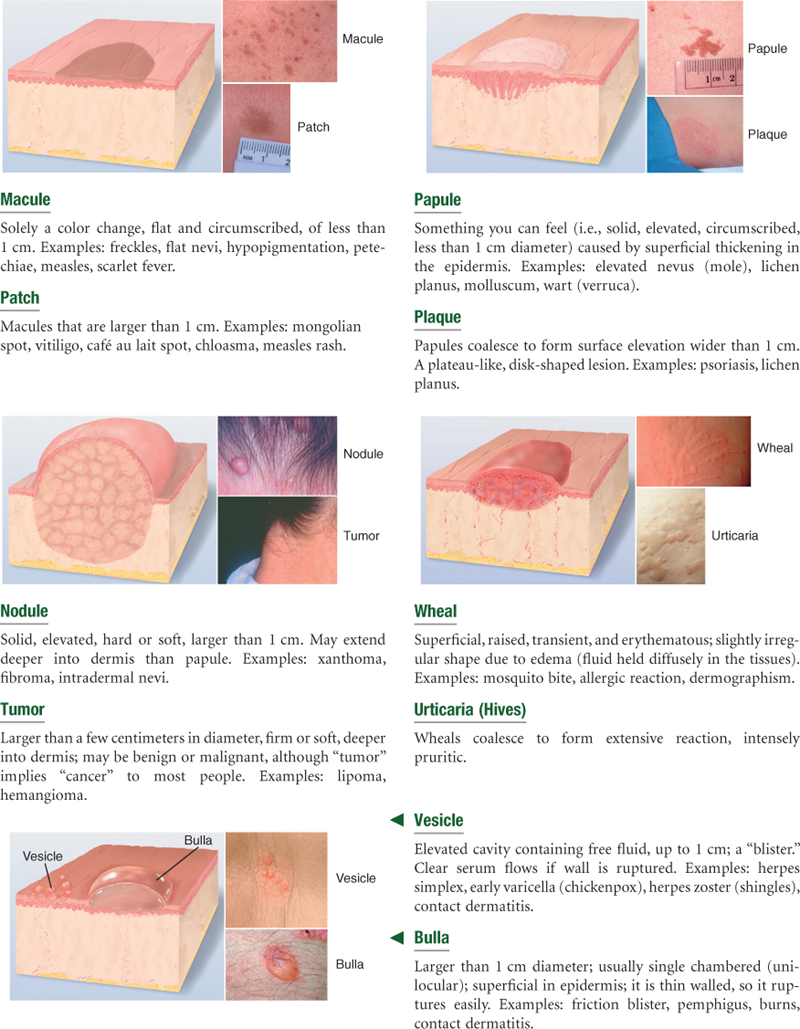
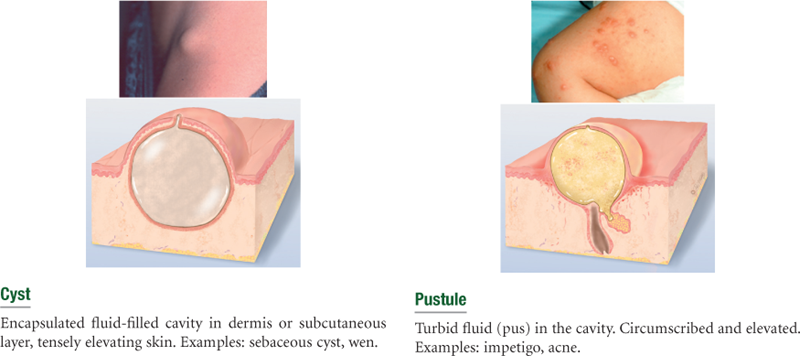
Line drawings © Pat Thomas, 2010.
*The immediate result of a specific causative factor; primary lesions develop on previously unaltered skin.
TABLE 12-5
Secondary Skin Lesions*
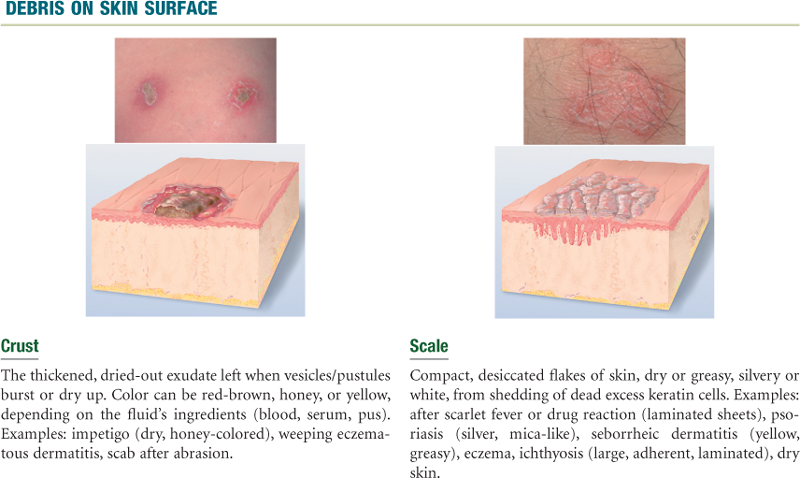
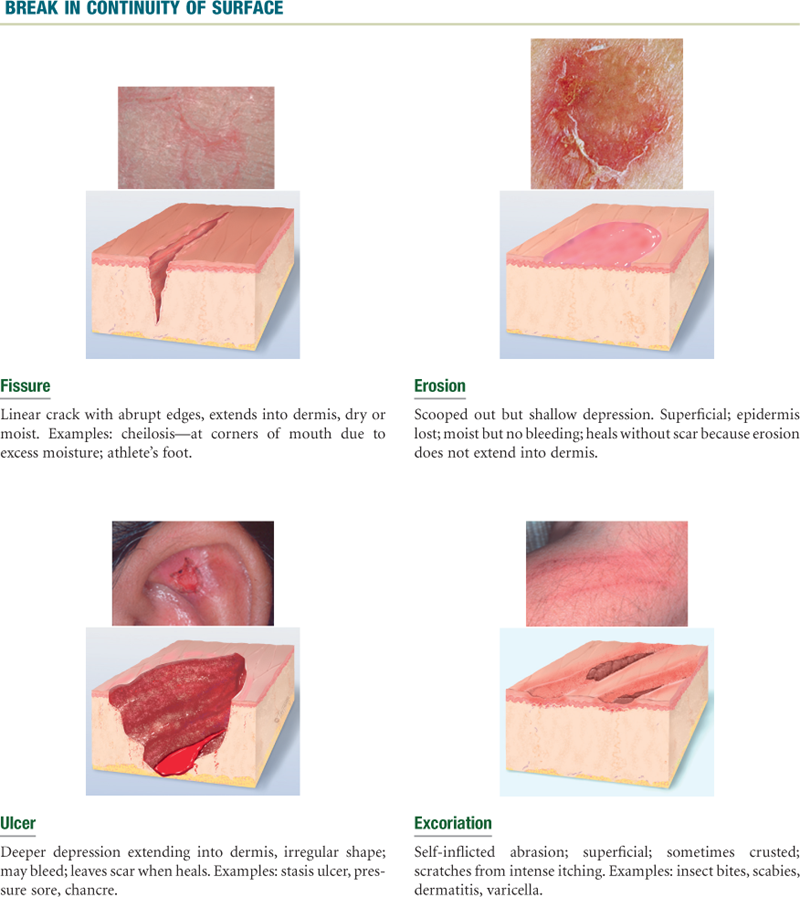
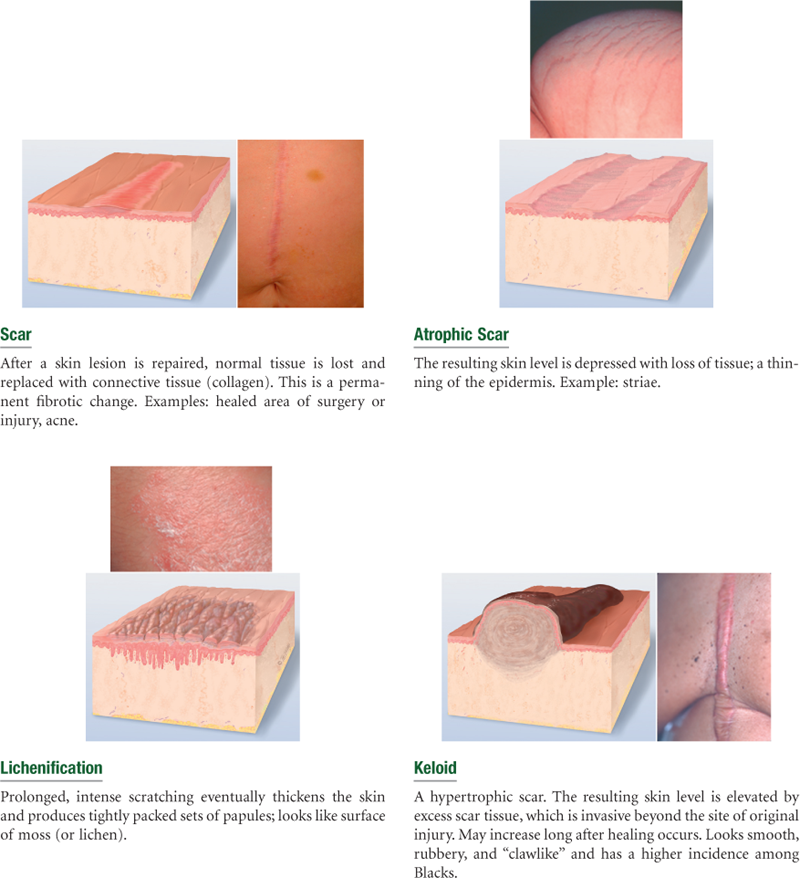
Line drawings © Pat Thomas, 2010.
Note: Combinations of primary and secondary lesions may coexist in the same person. Such combined designations may be termed papulosquamous, maculopapular, vesiculopustular, or papulovesicular.
*Resulting from a change in a primary lesion from the passage of time; an evolutionary change.


Summary Checklist: Skin, Hair, and Nails Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Bibliography
1. American Cancer Society (ACS). Skin cancer. Retrieved September 20, 2009, from www.cancer.org/downloads/PRO/SkinCancer.pdf; 2009.
2. Arora A, Attwood J. Common skin cancers and their precursors. Surgical Clinics of North America. 2009;89(3):703–712.
3. Borfitz JM. Commonly missed dermatologic conditions. Nurse Practitioner. 2009;34(10):35–45.
4. Centers for Disease Control and Prevention. Skin cancer. Retrieved September 20, 2009, from www.cdc.gov/healthyyouth/skincancer/guidelines/summary.htm; 2006.
5. Christopher GF, Meires J. Treating acute onset of psoriasis. Nurse Practitioner. 2008;33(7):7–10.
6. Drugge JM, Allen PJ. A nurse practitioner’s guide to the management of herpes simplex virus-1 in children. Pediatric Nursing. 2008;34(4):310–318.
7. Emond RT, Welsby P, Rowland H. Colour atlas of infectious diseases. 4th ed. St. Louis: Mosby; 2003.
8. Friedman-Kien AE. Color atlas of AIDS. 2nd ed. Philadelphia: Saunders; 1996.
9. Gordon RM. Skin cancer: more than skin deep. The Nurse Practitioner. 2009;34(4):21–28.
10. Habif TP, Campbell Jr JL, Chapman MS. Skin disease: diagnosis and treatment. 2nd ed. St. Louis: Mosby; 2005.
11. Holzberg M. Common nail disorders. Dermatologic Clinics. 2006;24(3):349–354.
12. Howard J, Loiselle J. A clinician’s guide to safe and effective tick removal. Contemporary Pediatrics. 2006;23(5):36–42.
13. Marks JG, Miller J. Lookingbill and Marks’ principles of dermatology. 4th ed. Philadelphia: Saunders; 2006.
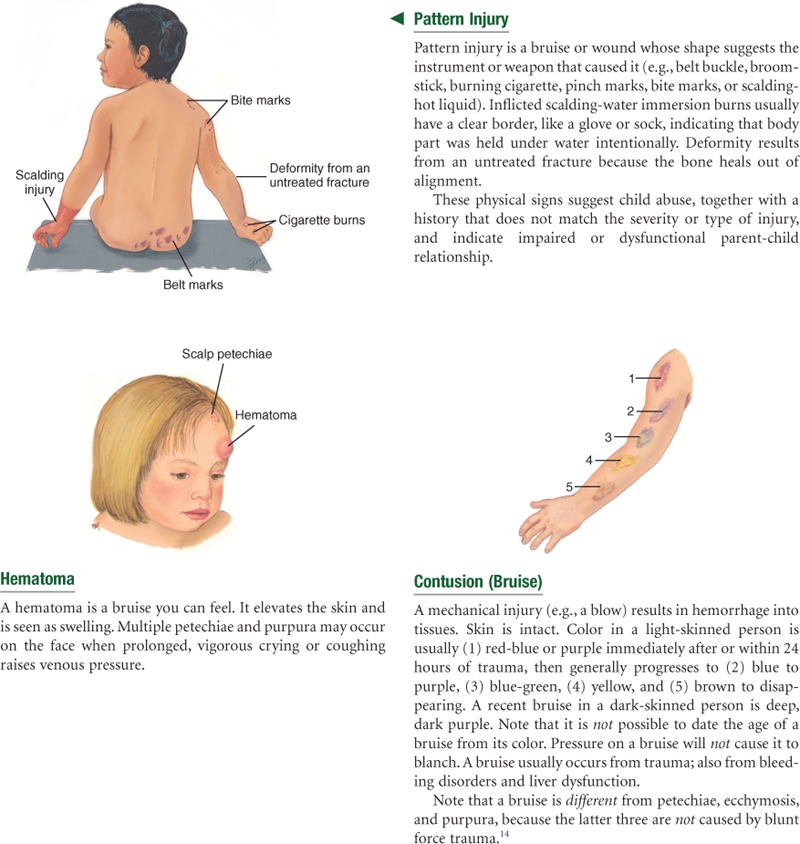
14. Nash KR, Sheridan DJ. Can one accurately date a bruise? State of the science. Journal of Forensic Nursing. 2009;5:31–37.
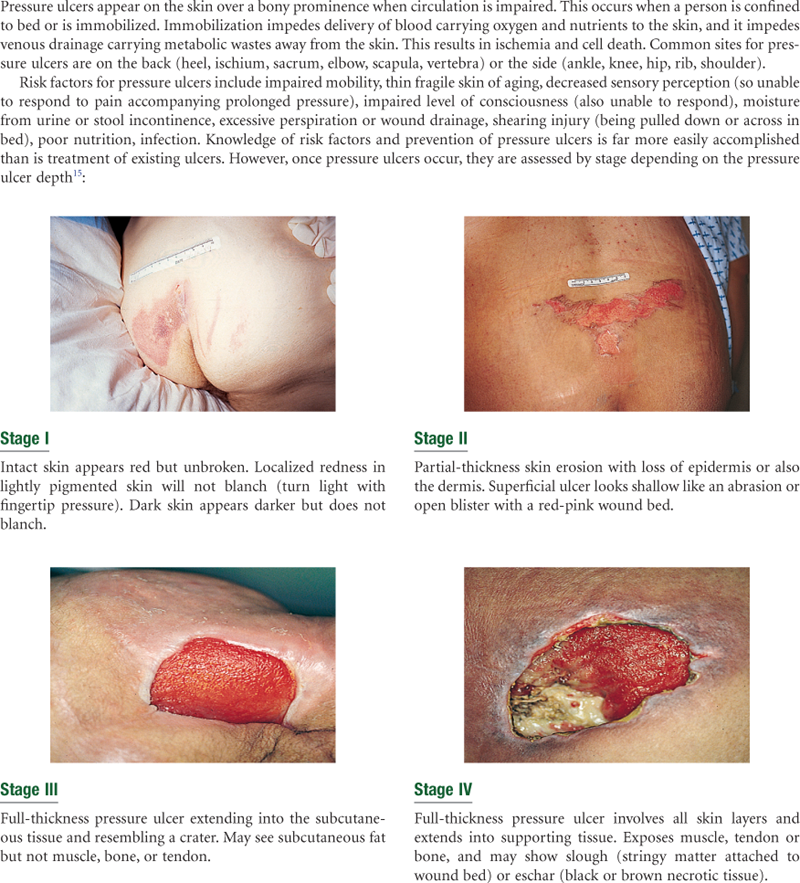
15. National Pressure Ulcer Advisory Panel (NPUAP). Pressure ulcer stages revised by NPUAP. Retrieved September 20, 2009, from www.npaup.org/pr2.htm; 2007.
16. Pandya KA, Radke F. Benign skin lesions: lipomas, epidermal inclusion cysts, muscle and nerve biopsies. Surgical Clinics of North America. 2009;89(3):677–687.
17. Rhoads J. Managing bites and stings. Nurse Practitioner. 2009;34(8):37–43.
18. Roebuck HL. Acne: intervene early. Nurse Practitioner. 2006;31(10):24–45.
19. Roebuck H, Siegel M. The ABCs of melanoma recognition. Nurse Practitioner. 2006;31(6):11–13.
20. Spector RE. Cultural diversity in health and illness. Upper Saddle River, NJ: Prentice Hall; 2004.
21. Spicknall KE, Zirwas MJ, English JC. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. Journal of the American Academy of Dermatology. 2005;52:1020–1028.
22. Stanger CB. Actinic keratosis: do the numbers add up? Nurse Practitioner. 2009;34(2):36–39.
23. Sullivan JR, Shear NH. Drug eruptions and other adverse drug effects in aged skin. Clinics in Geriatric Medicine. 2002;18(1):21–42.
24. Trent J, Kirsner R. Cutaneous manifestations of HIV: a primer. Advances in Skin & Wound Care. 2004;17(3):116–129.
25. U.S. Preventive Services Task Force (USPSTF). Skin cancer screening: guide to clinical preventive services. Retrieved September 20, 2009, from www.ahrq.gov/clinic/prevenix.htm; 2008.
26. Wilson DD. Herpes zoster: prevention, diagnosis, and treatment. Nurse Practitioner. 2007;32(9):19–25.
27. Wolff T, Tai E, Miller T. Screening for skin cancer: an update of the evidence for the U.S Preventive Services Task Force. Annals of Internal Medicine. 2009;150(3):194–198.
*Please note that space does not allow a detailed plan for each sample clinical problem in the text. Please consult the appropriate text for current treatment plans.