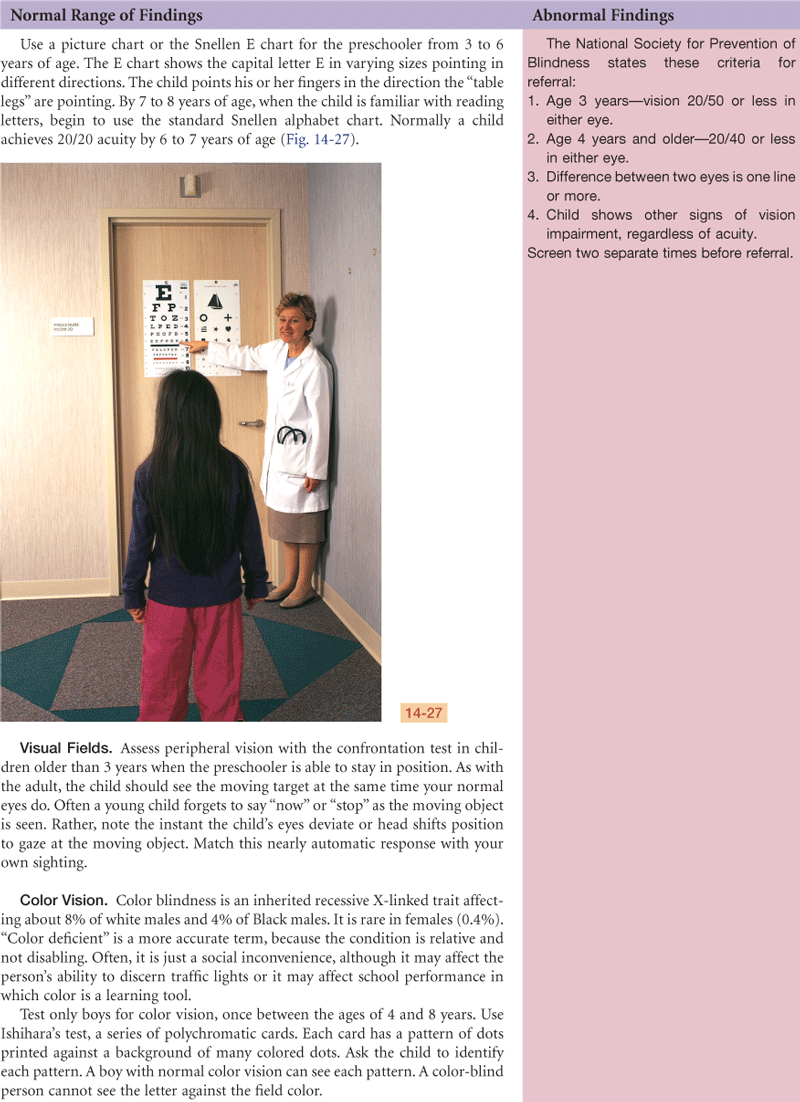
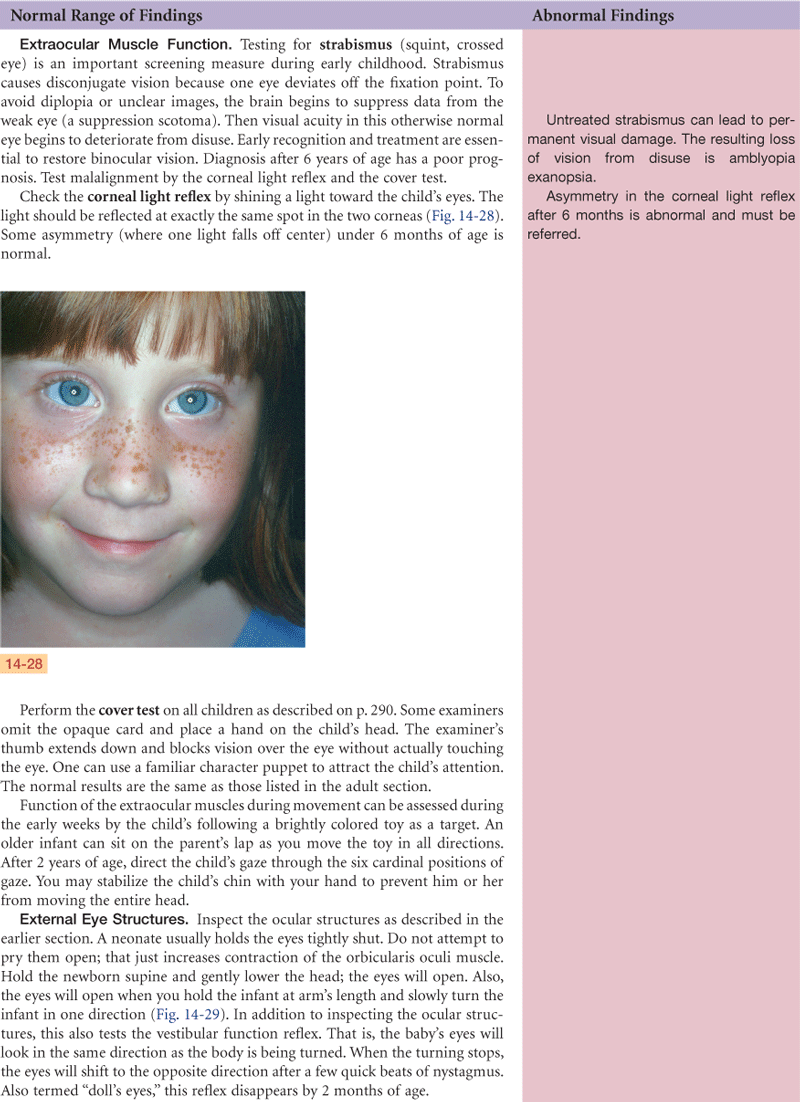
Eyes
Outline

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
Structure and Function
External Anatomy
The eye is the sensory organ of vision. Humans are very visual beings. More than half the neocortex is involved with processing visual information.
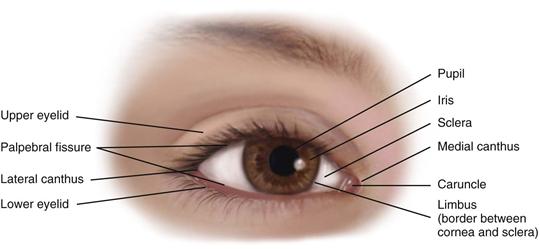
Because this sense is so important to humans, the eye is well protected by the bony orbital cavity, surrounded with a cushion of fat. The eyelids are like two movable shades that further protect the eye from injury, strong light, and dust. The upper eyelid is the larger and more mobile one. The eyelashes are short hairs in double or triple rows that curve outward from the lid margins, filtering out dust and dirt.
The palpebral fissure is the elliptical open space between the eyelids (Fig. 14-1). When closed, the lid margins approximate completely. When open, the upper lid covers part of the iris. The lower lid margin is just at the limbus, the border between the cornea and sclera. The canthus is the corner of the eye, the angle where the lids meet. At the inner canthus, the caruncle is a small, fleshy mass containing sebaceous glands.
14-1 Copyright © (2006) © Pat Thomas, 2006.
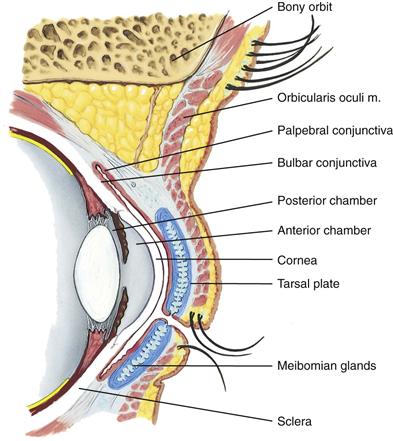
Within the upper lid, tarsal plates are strips of connective tissue that give it shape (Fig. 14-2). The tarsal plates contain the meibomian glands, modified sebaceous glands that secrete an oily lubricating material onto the lids. This stops the tears from overflowing and helps form an airtight seal when the lids are closed.
14-2
The exposed part of the eye has a transparent protective covering, the conjunctiva. The conjunctiva is a thin mucous membrane folded like an envelope between the eyelids and the eyeball. The palpebral conjunctiva lines the lids and is clear, with many small blood vessels. It forms a deep recess and then folds back over the eye. The bulbar conjunctiva overlays the eyeball, with the white sclera showing through. At the limbus, the conjunctiva merges with the cornea. The cornea covers and protects the iris and pupil.
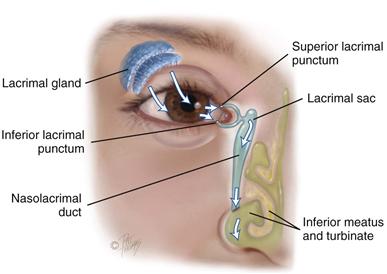
The lacrimal apparatus provides constant irrigation to keep the conjunctiva and cornea moist and lubricated (Fig. 14-3). The lacrimal gland, in the upper outer corner over the eye, secretes tears. The tears wash across the eye and are drawn up evenly as the lid blinks. The tears drain into the puncta, visible on the upper and lower lids at the inner canthus. The tears then drain into the nasolacrimal sac, through the one-half-inch-long nasolacrimal duct, and empty into the inferior meatus inside the nose. A tiny fold of mucous membrane prevents air from being forced up the nasolacrimal duct when the nose is blown.
14-3 Copyright © (2006) Lacrimal apparatus. © Pat Thomas, 2006.
Extraocular Muscles
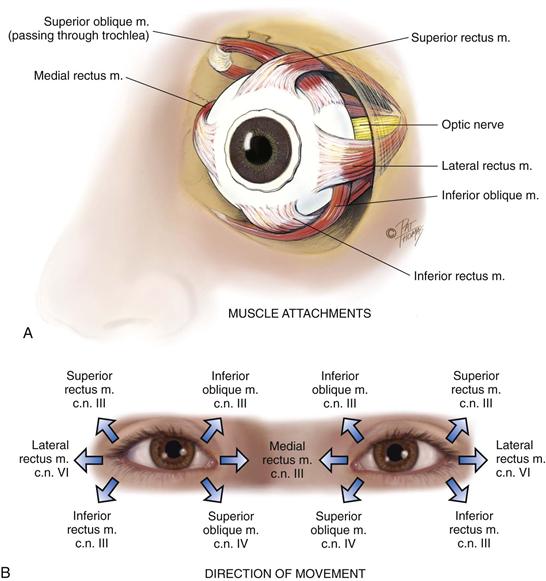
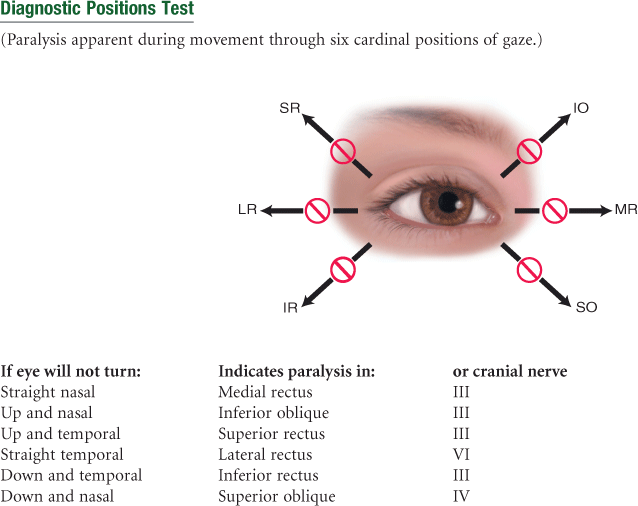
Six muscles attach the eyeball to its orbit (Fig. 14-4, A) and serve to direct the eye to points of the person’s interest. These extraocular muscles give the eye both straight and rotary movement. The four straight, or rectus, muscles are the superior, inferior, lateral, and medial rectus muscles. The two slanting, or oblique, muscles are the superior and inferior muscles.
14-4 Copyright © (2006) © Pat Thomas, 2006.
Each muscle is coordinated, or yoked, with one in the other eye. This ensures that when the two eyes move, their axes always remain parallel (called conjugate movement). Parallel axes are important because the human brain can tolerate seeing only one image. Although some animals can perceive two different pictures through each eye, human beings have a binocular, single-image visual system. This occurs because our eyes move as a pair. For example, the two yoked muscles that allow looking to the far right are the right lateral rectus and the left medial rectus.
Movement of the extraocular muscles (Fig. 14-4, B) is stimulated by three cranial nerves. Cranial nerve VI, the abducens nerve, innervates the lateral rectus muscle (which abducts the eye); cranial nerve IV, the trochlear nerve, innervates the superior oblique muscle; and cranial nerve III, the oculomotor nerve, innervates all the rest—the superior, inferior, and medial rectus and the inferior oblique muscles. Note that the superior oblique muscle is located on the superior aspect of the eyeball, but when it contracts, it enables the person to look downward and inward.
Internal Anatomy
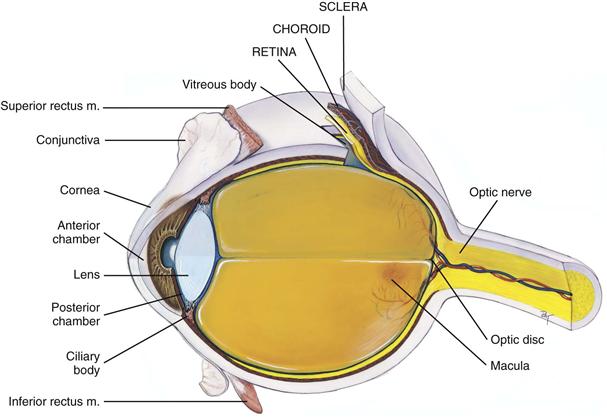
The eye is a sphere composed of three concentric coats: (1) the outer fibrous sclera, (2) the middle vascular choroid, and (3) the inner nervous retina (Fig. 14-5). Inside the retina is the transparent vitreous body. The only parts accessible to examination are the sclera anteriorly and the retina through the ophthalmoscope.
14-5
The Outer Layer
The sclera is a tough, protective, white covering. It is continuous anteriorly with the smooth, transparent cornea, which covers the iris and pupil. The cornea is part of the refracting media of the eye, bending incoming light rays so that they will be focused on the inner retina.
The cornea is very sensitive to touch; contact with a wisp of cotton stimulates a blink in both eyes, called the corneal reflex. The trigeminal nerve (cranial nerve V) carries the afferent sensation into the brain, and the facial nerve (cranial nerve VII) carries the efferent message that stimulates the blink.
The Middle Layer
The choroid has dark pigmentation to prevent light from reflecting internally and is heavily vascularized to deliver blood to the retina. Anteriorly, the choroid is continuous with the ciliary body and the iris. The muscles of the ciliary body control the thickness of the lens. The iris functions as a diaphragm, varying the opening at its center, the pupil. This controls the amount of light admitted into the retina. The muscle fibers of the iris contract the pupil in bright light and to accommodate for near vision; they dilate the pupil in dim light and accommodate for far vision. The color of the iris varies from person to person.
The pupil is round and regular. Its size is determined by a balance between the parasympathetic and sympathetic chains of the autonomic nervous system. Stimulation of the parasympathetic branch, through cranial nerve III, causes constriction of the pupil. Stimulation of the sympathetic branch dilates the pupil and elevates the eyelid. As mentioned earlier, the pupil size also reacts to the amount of ambient light and to accommodation, or focusing an object on the retina.
The lens is a biconvex disc located just posterior to the pupil. The transparent lens serves as a refracting medium, keeping a viewed object in continual focus on the retina. Its thickness is controlled by the ciliary body; the lens bulges for focusing on near objects and flattens for far objects.
The anterior chamber is posterior to the cornea and in front of the iris and lens. The posterior chamber lies behind the iris to the sides of the lens. These contain the clear, watery aqueous humor that is produced continually by the ciliary body. The continuous flow of fluid serves to deliver nutrients to the surrounding tissues and to drain metabolic wastes. Intraocular pressure is determined by a balance between the amount of aqueous produced and resistance to its outflow at the angle of the anterior chamber.
The Inner Layer
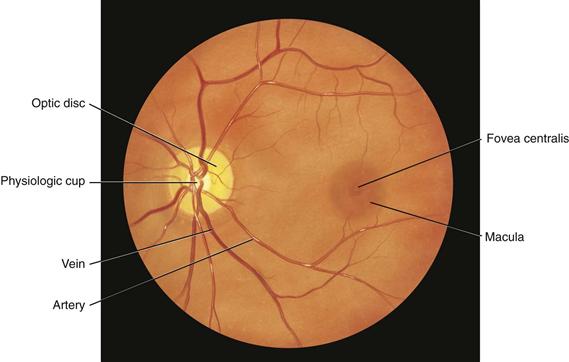
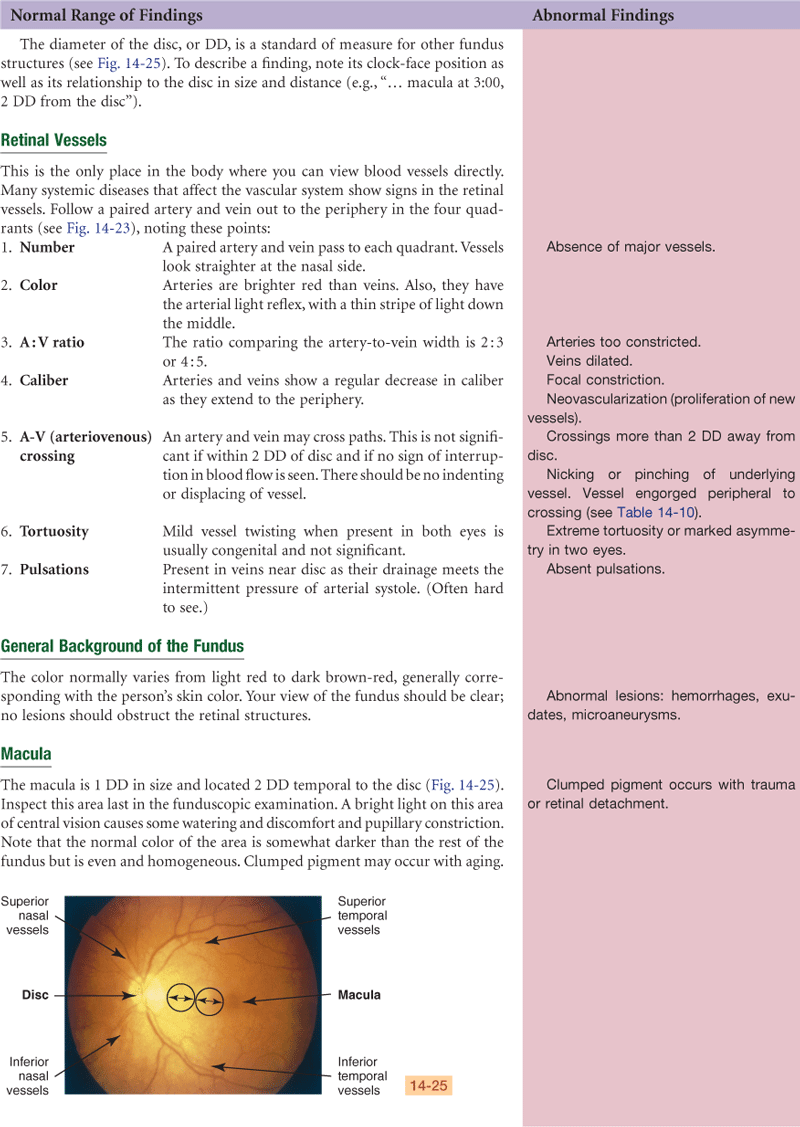
The retina is the visual receptive layer of the eye in which light waves are changed into nerve impulses. The retina surrounds the soft, gelatinous vitreous humor. The retinal structures viewed through the ophthalmoscope are the optic disc, the retinal vessels, the general background, and the macula (Fig. 14-6).
14-6
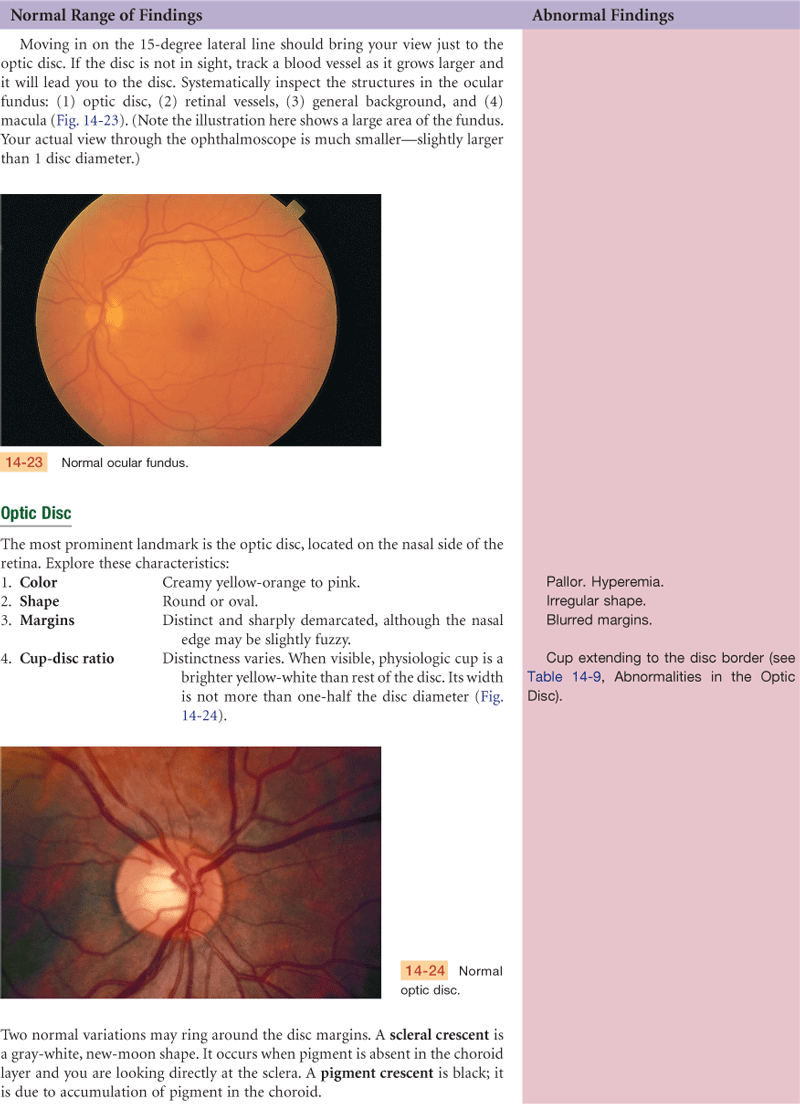
The optic disc (or optic papilla) is the area in which fibers from the retina converge to form the optic nerve. Located toward the nasal side of the retina, it has these characteristics: a color that varies from creamy yellow-orange to pink; a round or oval shape; margins that are distinct and sharply demarcated, especially on the temporal side; and a physiologic cup, the smaller circular area inside the disc where the blood vessels exit and enter.
The retinal vessels normally include a paired artery and vein extending to each quadrant, growing progressively smaller in caliber as they reach the periphery. The arteries appear brighter red and narrower than the veins, and the arteries have a thin sliver of light on them (the arterial light reflex). The general background of the fundus varies in color, depending on the person’s skin color. The macula is located on the temporal side of the fundus. It is a slightly darker pigmented region surrounding the fovea centralis, the area of sharpest and keenest vision. The macula receives and transduces light from the center of the visual field.
Visual Pathways and Visual Fields
Objects reflect light. The light rays are refracted through the transparent media (cornea, aqueous humor, lens, and vitreous body) and strike the retina. The retina transforms the light stimulus into nerve impulses that are conducted through the optic nerve and the optic tract to the visual cortex of the occipital lobe.
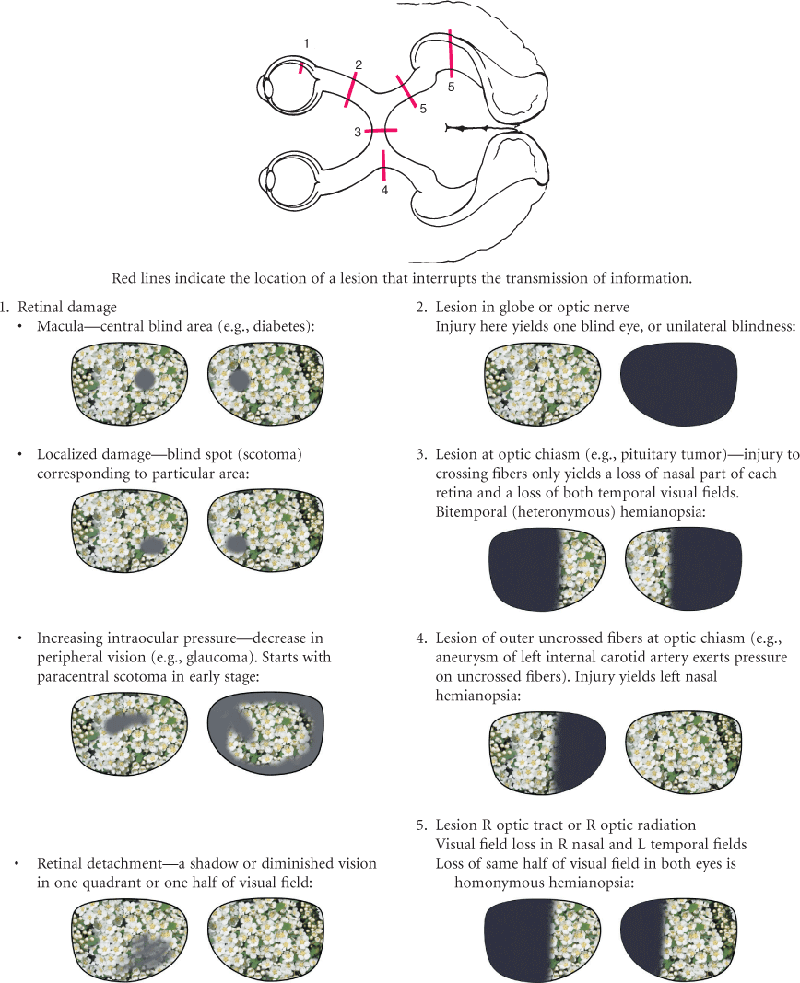
The image formed on the retina is upside down and reversed from its actual appearance in the outside world (Fig. 14-7). That is, an object in the upper temporal visual field of the right eye reflects its image onto the lower nasal area of the retina. All retinal fibers collect to form the optic nerve, but they maintain this same spatial arrangement, with nasal fibers running medially and temporal fibers running laterally.

At the optic chiasm, nasal fibers (from both temporal visual fields) cross over. The left optic tract now has fibers from the left half of each retina, and the right optic tract contains fibers only from the right. Thus the right side of the brain looks at the left side of the world.
Visual Reflexes
Pupillary Light Reflex
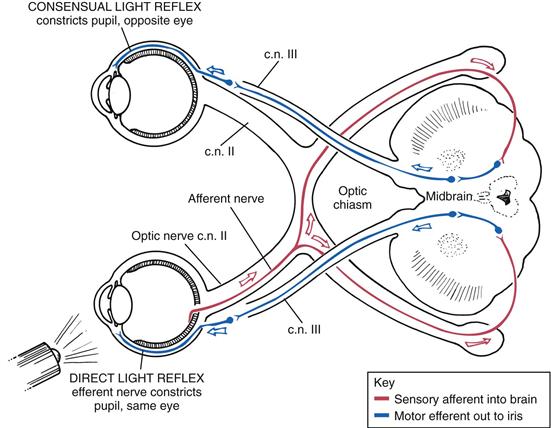
The pupillary light reflex is the normal constriction of the pupils when bright light shines on the retina (Fig. 14-8). It is a subcortical reflex arc (i.e., a person has no conscious control over it); the sensory afferent link is cranial nerve II (the optic nerve), and the motor efferent path is cranial III (the oculomotor nerve).
14-8
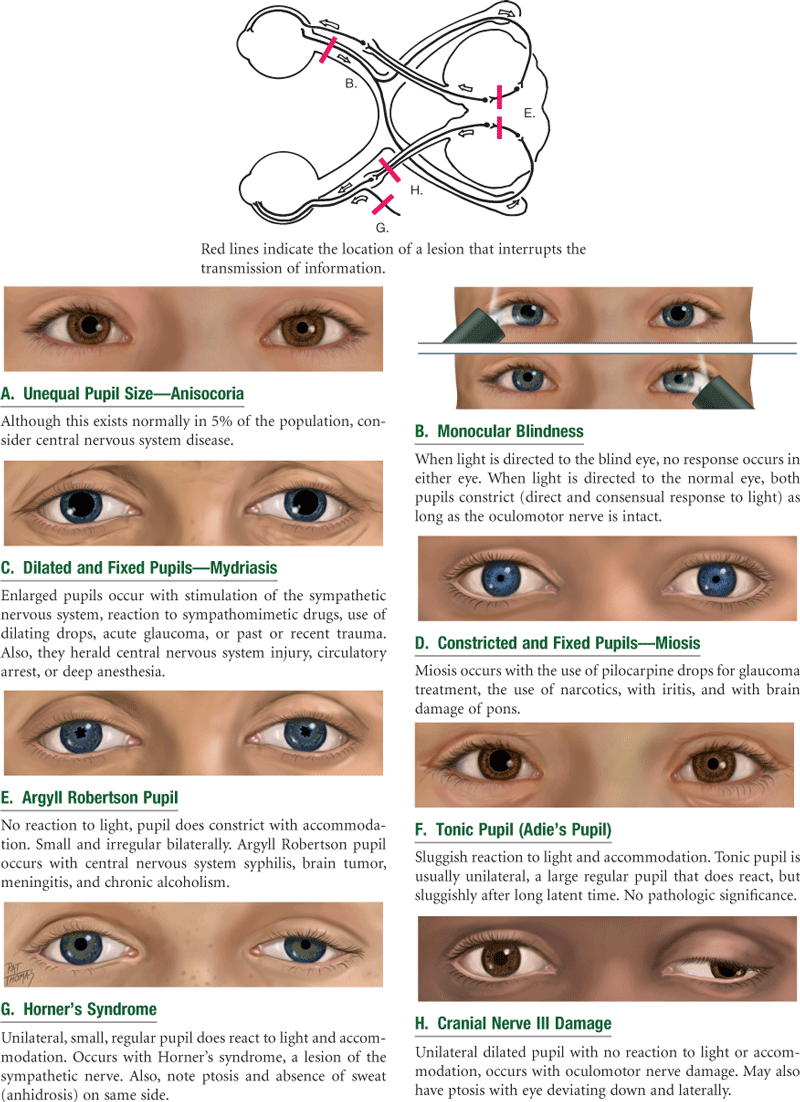
When one eye is exposed to bright light, a direct light reflex occurs (constriction of that pupil) as well as a consensual light reflex (simultaneous constriction of the other pupil). This happens because the optic nerve carries the sensory afferent message in and then synapses with both sides of the brain. For example, consider the light reflex in a person who is blind in one eye. Stimulation of the normal eye produces both a direct and a consensual light reflex. Stimulation of the blind eye causes no response because the sensory afferent in cranial nerve II is destroyed.
Fixation
This is a reflex direction of the eye toward an object attracting a person’s attention. The image is fixed in the center of the visual field, the fovea centralis. This consists of very rapid ocular movements to put the target back on the fovea and somewhat slower (smooth pursuit) movements to track the target and keep its image on the fovea. These ocular movements are impaired by drugs, alcohol, fatigue, and inattention.
Accommodation
This is adaptation of the eye for near vision. It is accomplished by increasing the curvature of the lens through movement of the ciliary muscles. Although the lens cannot be observed directly, the components of accommodation that can be observed are convergence (motion toward) of the axes of the eyeballs and pupillary constriction.
 Developmental Competence
Developmental Competence
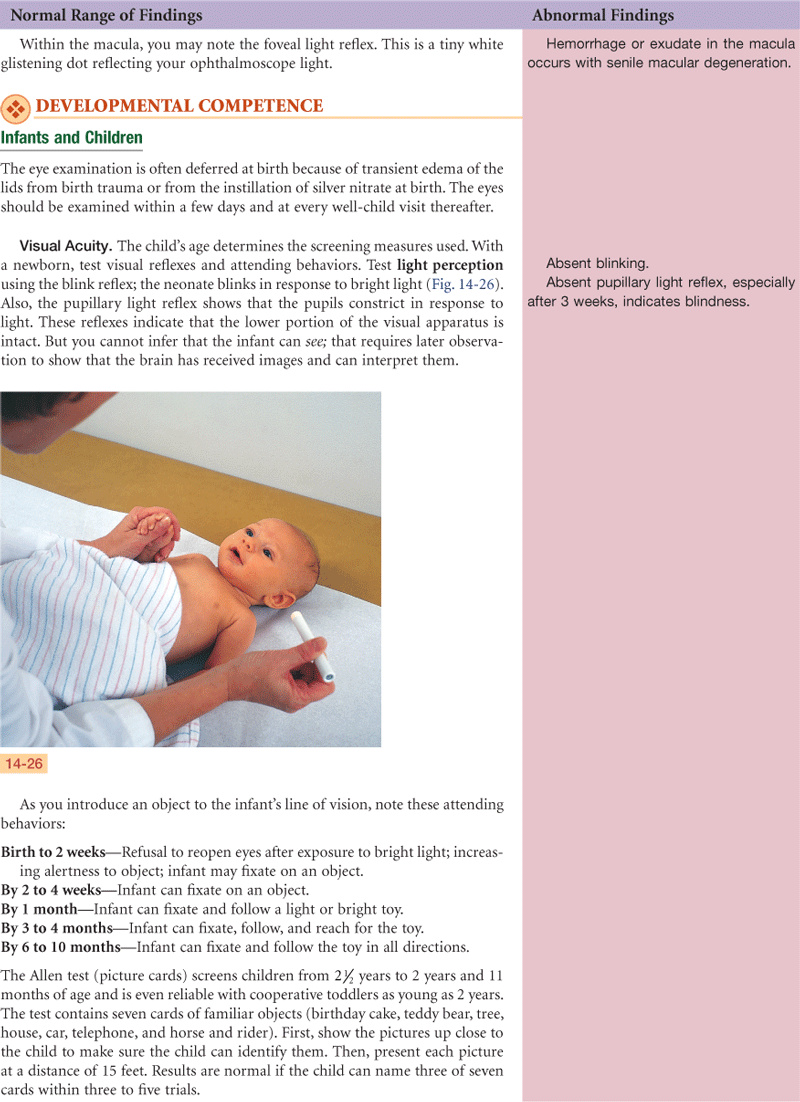
Infants and Children
At birth, eye function is limited, but it matures fully during the early years. Peripheral vision is intact in the newborn infant. The macula, the area of keenest vision, is absent at birth but is developing by 4 months and is mature by 8 months. Eye movements may be poorly coordinated at birth. By 3 to 4 months of age, the infant establishes binocularity and can fixate on a single image with both eyes simultaneously. Most neonates (80%) are born farsighted; this gradually decreases after 7 to 8 years of age.
In structure, the eyeball reaches adult size by 8 years. At birth, the iris shows little pigment and the pupils are small. The lens is nearly spherical at birth, growing flatter throughout life. Its consistency changes from that of soft plastic at birth to rigid glass in old age.
The Aging Adult
Changes in eye structure contribute greatly to the distinct facial changes of the aging person. The skin loses its elasticity, causing wrinkling and drooping; fat tissues and muscles atrophy; and the external eye structures appear as on p. 306. Lacrimal glands involute, causing decreased tear production and a feeling of dryness and burning.
On the globe itself, the cornea may show an infiltration of degenerative lipid material around the limbus (see discussion of arcus senilis, p. 307). Pupil size decreases. The lens loses elasticity, becoming hard and glasslike. This glasslike quality decreases the lens’s ability to change shape to accommodate for near vision; this condition is termed presbyopia. By 40 years of age, 50% of people have presbyopia.6 By 70 years of age, the normally transparent fibers of the lens begin to thicken and yellow; this is the beginning of a senile cataract.
Inside the globe, floaters appear in the vitreous as a result of debris that accumulates because the vitreous is not renewed as continuously as the aqueous humor. Visual acuity may diminish gradually after 50 years of age, and even more so after 70 years. Near vision is commonly affected because of the decreased power of accommodation in the lens (presbyopia). In the early 40s, a person may have blurred vision and difficulty reading. Also, the aging person needs more light to see because of a decreased adaptation to darkness, and this condition may affect the function of night driving.
In older adults, the most common causes of decreased visual functioning are:
1. Cataract formation, or lens opacity, resulting from a clumping of proteins in the lens. Some cataract formation should be expected by age 70 years. Studies indicate that 46% of people ages 75 to 85 years have cataracts.9
2. Glaucoma, or increased intraocular pressure. The incidence increases with age to 7.2% at ages 75 to 85 years, affecting men at higher rates than women.9 Chronic open-angle glaucoma is the most common type; it involves a gradual loss of peripheral vision.
3. Macular degeneration, or the breakdown of cells in the macula of the retina. Loss of central vision, the area of clearest vision, is the most common cause of blindness. It affects 28% of those ages 75 to 85 years, with women affected more often than men.9 With this, the person is unable to read fine print, sew, or do fine work and may have difficulty distinguishing faces. Depending on how much the lifestyle is oriented around activities requiring close work, loss of central vision may cause great distress. Peripheral vision is not affected, so the person can manage self-care and will not become completely disabled.
 Culture and Genetics
Culture and Genetics
Racial differences are evident in the palpebral fissures. Persons of Asian origin are often identified by their characteristic eyes, whereas the presence of narrowed palpebral fissures in non-Asian individuals may be diagnostic of a serious congenital anomaly, Down syndrome.
Culturally based variability exists in the color of the iris and in retinal pigmentation, with darker irides having darker retinas behind them. Individuals with light retinas generally have better night vision but can have pain in an environment that has too much light.
Racial Variations in Disease
Primary open-angle glaucoma affects Blacks three to six times more often than whites and is six times more likely to cause blindness in Blacks than in whites.6 Reasons for this are not known.
The percent of adults 18 years of age and older reporting visual limitations and trouble seeing with glasses in 2006 was the highest, 16.7%, among American Indians and Alaska natives; African Americans 10.4%; and whites 9.5%. Poverty is also an extenuating factor in this problem; 26.4% of the population living within poverty levels report this.15
The prevalence of blindness also has racial and ethnic variations. In whites older than 40 years, the leading cause of blindness is age-related macular degeneration (54%), followed by cataracts (9%).5 In Blacks older than 40 years, cataracts and open-angle glaucoma together cause 60% of blindness. In Hispanics older than 40 years, the leading cause of blindness is open-angle glaucoma.
Subjective Data
| Examiner Asks | Rationale |
| 1. Vision difficulty. Any difficulty seeing or any blurring? Any blind spots? Come on suddenly, or progress slowly? In one eye or both? | |
| •Constant, or does it come and go? | |
| •Do objects appear out of focus, or does it feel like a clouding over objects? Does it feel like “grayness” of vision? | |
| •Do spots move in front of your eyes? One or many? In one or both eyes? | Floaters are common with myopia or after middle age due to condensed vitreous fibers. Usually not significant, but acute onset of floaters (“shade” or “cobwebs”) occurs with retinal detachment. |
| •Any halos/rainbows around objects? Or rings around lights? | Halos around lights occur with acute narrow-angle glaucoma. |
| •Any blind spot? Does it move as you shift your gaze? Any loss of peripheral vision? | Scotoma, a blind spot surrounded by an area of normal or decreased vision, occurs with glaucoma, with optic nerve disorders. |
| •Any night blindness? | Night blindness occurs with optic atrophy, glaucoma, or vitamin A deficiency. |
| 2. Pain. Any eye pain? Please describe. | |
| •Come on suddenly? | Sudden onset of eye symptoms (pain, floaters, blind spot, loss of peripheral vision) is an emergency. Refer immediately. |
| •Quality—a burning or itching? Or sharp, stabbing pain? Pain with bright light? •A foreign body sensation? Or deep aching? Or headache in brow area? | Quality is valuable in diagnosis. Photophobia is the inability to tolerate light. Note: Some common eye diseases cause no pain (e.g., cataract, glaucoma). |
| 3. Strabismus, diplopia. Any history of crossed eyes? Now or in the past? Does this occur with eye fatigue? | Strabismus is a deviation in the axis of the eye. |
| •Ever see double? Constant, or does it come and go? In one eye or both? | Diplopia is the perception of two images of a single object. |
| 4. Redness, swelling. Any redness or swelling in the eyes? •Any infections? Now or in the past? When do these occur? In a particular time of year? | |
| 5. Watering, discharge. Any watering or excessive tearing? | Lacrimation (tearing) and epiphora (excessive tearing) are due to irritants or obstruction in drainage of tears. |
| •Any discharge? Any matter in the eyes? Is it hard to open your eyes in the morning? What color is the discharge? •How do you remove matter from your eyes? | Purulent discharge is thick and yellow. Crusts form at night. Assess hygiene practices and knowledge of cross-contamination. |
| 6. Past history of ocular problems. Any history of injury or surgery to eye? Or any history of allergies? | Allergens cause irritation of conjunctiva or cornea (e.g., makeup, contact lens solution). |
| 7. Glaucoma. Ever been tested for glaucoma? Results? •Any family history of glaucoma? | Glaucoma is characterized by increased intraocular pressure. |
| 8. Use of glasses or contact lenses. Do you wear glasses or contact lenses? How do they work for you? | |
| •Last time your prescription was checked? Was it changed? | |
| •If you wear contact lenses, are there any problems such as pain, photophobia, watering, or swelling? | |
| •How do you care for contacts? How long do you wear them? How do you clean them? Do you remove them for certain activities? | Assess self-care behaviors. |
| 9. Self-care behaviors. Last vision test? Ever tested for color vision? | Self-care behaviors for eyes and vision. |
| •Any environmental conditions at home or at work that may affect your eyes? For example, flying sparks, metal bits, smoke, dust, chemical fumes? If so, do you wear goggles to protect your eyes? | Work-related eye disease (e.g., an auto mechanic with a foreign body from metal working or radiation damage from welding). |
| 10. What medications are you taking? Systemic or topical? Do you take any medication specifically for the eyes? | Some medications affect the eyes (e.g., prednisone may cause cataracts or increased intraocular pressure). |
| 11. If you have experienced a vision loss, how do you cope? Do you have books with large print, books on audio tape or CD, braille? | |
| •Do you maintain your living environment the same? •Do you sometimes fear complete loss of vision? | A constant spatial layout eases navigation through the home. |
| Additional History for Infants and Children | |
| 1. Any vaginal infections in the mother at time of delivery? | Genital herpes and gonorrhea vaginitis have ocular sequelae for the newborn. |
| 2. Considering age of child, which developmental milestones of vision have you (parent) noted? 3. Does the child have routine vision testing at school? 4. Are you (parent) aware of safety measures to protect child’s eyes from trauma? Do you inspect toys? •Have you taught the child safe care of sharp objects and how to carry and how to use them? | The parent is most often the one to detect vision problems. |
| Additional History for the Aging Adult | |
| 1. Have you noticed any visual difficulty with climbing stairs or driving? Any problem with night vision? | Any loss of depth perception or central vision. |
| 2. When was the last time you were tested for glaucoma? | |
| •Any aching pain around eyes? Any loss of peripheral vision? | |
| •If you have glaucoma, how do you manage your eyedrops? | Compliance may be a problem if symptoms are absent. Assess ability to administer eyedrops. |
| 3. Is there a history of cataracts? Any loss or progressive blurring of vision? | |
| 4. Do your eyes ever feel dry? Burning? What do you do for this? | Decreased tear production may occur with aging. |
| 5. Any decrease in usual activities, such as reading or sewing? | Macular degeneration causes a loss in central vision acuity. |
Objective Data
| PREPARATION | EQUIPMENT NEEDED |
| Position the person standing for vision screening; then sitting up with the head at your eye level. | Snellen eye chart Handheld visual screener Opaque card or occluder Penlight Applicator stick Ophthalmoscope |


 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
Vision reported “good” with no recent change. No eye pain, no inflammation, no discharge, no lesions. Wears no corrective lenses, vision last tested 1 year PTA, test for glaucoma at that time was normal.
Objective
Snellen chart—Right 20/20, Left 20/20 −1. Fields normal by confrontation. Corneal light reflex symmetric bilaterally. Diagnostic positions test shows EOMs intact. Brows and lashes present. No ptosis. Conjunctiva clear. Sclera white. No lesions. PERRLA.
Fundi—Red reflex present bilaterally. Discs flat with sharp margins. Vessels present in all quadrants without crossing defects. Retinal background has even color with no hemorrhages or exudates. Macula has even color.
Assessment
Healthy vision function
Healthy eye structures
Focused Assessment: Clinical Case Study 1
Emma K. is a 34-year-old married, white female homemaker brought to the emergency department by police after a reported domestic quarrel.
Subjective
States husband struck her about the face and eyes with his fists about 1 hour PTA. “I ruined the dinner again. I can’t do anything right.” Pain in left cheek and both eyes felt immediately and continues. Alarmed at “bright red blood on eyeball.” No bleeding from eye area or cheek. Vision intact just after trauma. Now reports difficulty opening lids.
Objective
Sitting quietly and hunched over, hands over eyes. Voice tired and flat. L cheek swollen and discolored, no laceration. Lids edematous and discolored both eyes. No skin laceration. L lid swollen almost shut. L eye—round 1-mm bright red patch over lateral aspect of globe. No active bleeding out of eye, iris intact, anterior chamber clear. R eye—conjunctiva clear, sclera white, cornea and iris intact, anterior chamber clear. PERRLA. Pupils R 4/1 = 4/1 L. Vision 14/14 both eyes by Jaeger card.
Assessment
Ecchymoses L cheek and both eyes
Subconjunctival hemorrhage L eye
Pain R/T inflammation
Chronic low self-esteem R/T effects of domestic violence
Focused Assessment: Clinical Case Study 2
Sam T. is a 63-year-old married, white male postal carrier admitted to the medical center for surgery for suspected brain tumor. After postanesthesia recovery, Sam T. is admitted to the neurology ICU, awake, lethargic with slowed but correct verbal responses, oriented × 3, moving all four extremities, vital signs stable. Pupils R 4/2 = 4/2 L with sluggish response. Assessments are made q 15 minutes.
Subjective
No response now to verbal stimuli.
Objective
Semicomatose—no response to verbal stimuli, does withdraw R arm and leg purposefully to painful stimuli. No movement L arm or leg. Pupils R 5/5 ≠ L 4/2. Vitals remain stable as noted on graphic sheet.
Assessment
Unilateral dilated and fixed R pupil
Clouding of consciousness
Focal motor deficit—no movement L side
Ineffective tissue perfusion R/T interruption of cerebral flow
Focused Assessment: Clinical Case Study 3
Trung Q. is a 4-year-old male born in Southeast Asia who arrived in this country 1 month PTA. Lives with parents, 2 siblings. Speaks only native language; here with uncle, who acts as interpreter.
Subjective
Seeks care because RN in church sponsoring family noted “crossed eyes.” Uncle states vision seemed normal to parents. Plays with toys and manipulates small objects without difficulty. Identifies objects in picture books; does not read.
Objective
With uncle interpreting directions for test to Trung, vision by Snellen E chart—Right 20/30, Left 20/50 −1. Fields seem intact by confrontation—jerks head to gaze at object entering field.
EOMs: Asymmetric corneal light reflex with outward deviation L eye. Cover test—as R eye covered, L eye jerks to fixate, R eye steady when uncovered. As L eye covered, R eye holds steady gaze, L eye jerks to fixate as uncovered. Diagnostic positions—able to gaze in six positions, although L eye obviously malaligned at extreme medial gaze.
Eye structures: Brows and lashes present and normal bilaterally. Upward palpebral slant, epicanthal folds bilaterally—consistent with racial heritage. Conjunctiva clear, sclera white, iris intact, PERRLA.
Fundi: Discs flat with sharp margins. Observed vessels normal. Unable to see in all four quadrants or to see macular area.
Assessment
L exotropia
Abnormal vision in L eye
Disturbed visual sensory perception R/T effects of neurologic impairment
Focused Assessment: Clinical Case Study 4
Vera K. is an 87-year-old widowed, Black female homemaker living independently who is admitted to hospital for observation and adjustment of digitalis medication. Cardiac status has been stable during hospital stay.
Subjective
Reports desire to monitor own medication at home but fears problems because of blurred vision. First noted distant vision blurred 5 years ago but near vision seemed to improve at that time. “I started to read better without my glasses!” Since then, blurring at distant vision has increased, near vision now blurred also.
Able to navigate home environment without difficulty. Fixes simple meals with cold foods. Receives hot meal from “Meals on Wheels” at lunch. Enjoys TV, though it looks somewhat blurred. Unable to write letters, sew, or read paper, which she regrets.
Objective
Vision by Jaeger card Right 20/200, Left 20/400 −1, with glasses on. Fields intact by confrontation. EOMs intact. Brow hair absent lateral third. Upper lids have folds of redundant skin, but lids do not droop. Lower lids and lashes intact. Xanthelasma present both inner canthi. Conjunctiva clear, sclera white, iris intact, L pupil looks cloudy, PERRLA, pupils R 3/2 = 3/2 L.
Fundi: Red reflex has central dark spot both eyes. Discs flat, with sharp margins. Observed vessels normal. Unable to see in all four quadrants or macular area because of small pupils.
Assessment
Central opacity, both eyes
Central visual acuity deficit, both eyes
Deficient diversional activity R/T poor vision
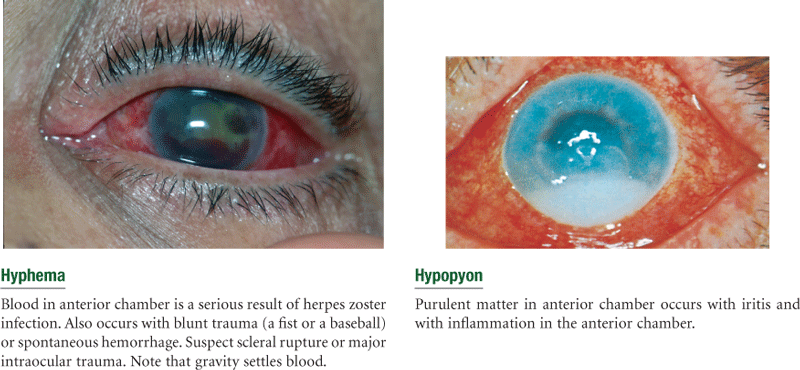
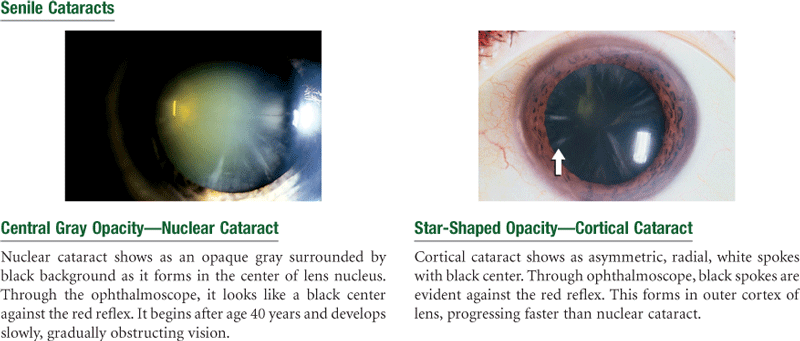
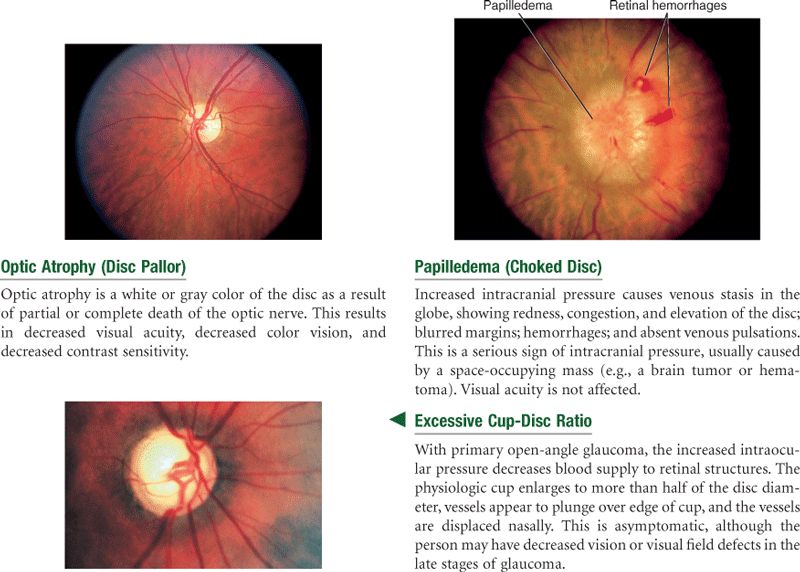
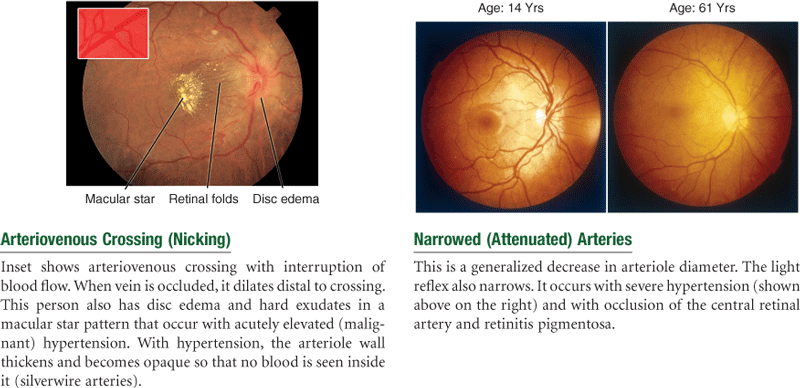
Abnormal Findings for Advanced Practice
Summary Checklist: Eye Exam
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Near vision (those older than 40 years or those having difficulty reading)
2. Test visual fields—confrontation test
3. Inspect extraocular muscle function
Corneal light reflex (Hirschberg test)
4. Inspect external eye structures
5. Inspect anterior eyeball structures
Optic disc (color, shape, margins, cup-disc ratio)
Retinal vessels (number, color, artery-vein [A : V] ratio, caliber, arteriovenous crossings, tortuosity, pulsations)
Bibliography
1. Anderson J, Shuey NH, Wall M. Rapid confrontation screening for peripheral visual field defects and extinction. Clinical and Experimental Optometry. 2009;92(1):45–48.
2. Bakes K, Cadnapaphornchai L. Clinical assessment of vision loss. Emergency Medicine. 2005;37:14–24.
3. Bloomgarden ZT. Screening for and managing diabetic retinopathy: current approaches. American Journal of Health-System Pharmacy. 2007;64(12):S8–S14.
4. Brown G. Retinal, vitreous and macular disorders. (Ed.) Current Opinion in Ophthalmology. 2005;16:139–229.
5. Congdon N, et al. Growing older, seeing less. Archives of Ophthalmology. 2004;122:477–485.
6. Friedman NJ, Kaiser PK, Pineda R. The Massachusetts Eye and Ear Infirmary illustrated manual of ophthalmology. 3rd ed. Philadelphia: Saunders; 2009.
7. Gillig PM, Sanders RD. Cranial nerve II: vision. Psychiatry. 2009;6(9):32–37.
8. Hammersmith K. Corneal and external disorders. (Ed.) Current Opinion in Ophthalmology. 2005;16:231–250.
9. Kane RT, Ouslander JG, Abrass IB. Essentials of clinical geriatrics. 6th ed. New York: McGraw-Hill; 2009.
10. Khare GD, Symons RC, Do DV. Common ophthalmic emergencies. International Journal of Clinical Practice. 2008;62(11):1176–1784.
11. Koch J, Sikes K. Getting the red out: primary angle-closure glaucoma. Nurse Practitioner. 2009;34(5):6–9.
12. Kowing D, Kester E. Keep an eye out for glaucoma. Nurse Practitioner. 2007;32(7):18–23.
13. Levine N. Asymptomatic lesions on eyelids. Geriatrics. 2008;63(8):31.
14. McLaughlin C, Levin A. The red reflex. Pediatric Emergency Care. 2006;22:137–140.
15. National Center for Health Statistics. Health, United States, 2009 with chartbook on trends in the health of Americans. Hyattsville, Md. Accessed February 1, 2010, from www.cdc.gov/nchs/hus/htm; 2009.
16. Nsiah-Kumi P, Ortmeier SR, Brown AE. Disparities in diabetic retinopathy screening and disease for racial and ethnic minority populations. Journal of the National Medical Association. 2009;101(5):430–437.
17. Pham TT, Perry JD. Floppy eyelid syndrome. Current Opinion in Ophthalmology. 2007;18(5):430–433.
18. Robinett DA, Kahn JH. The physical examination of the eye. Emergency Medicine Clinics of North America. 2007;26(1):1–16.
19. Rowe S, MacLean CH. Quality indicators for the care of vision impairment in vulnerable elders. American Geriatrics Society. 2007;55(Suppl 2):S450–S456.
20. Saligan L, Yeh S. Seeing red: guiding the management of ocular hyperemia. Nurse Practitioner. 2008;33(6):13–20.
21. Sharts-Hopko NC, Glynn-Milley C. Primary open-angle glaucoma. American Journal of Nursing. 2009;109(2):40–48.
22. Smith SC. Aging and vision. Journal of American Ophthalmic Registered Nurses. 2008;33(1):16–22.
23. Smith SC. Basic ocular anatomy. Journal of American Registered Nurses. 2008;33(3):19–23.
24. Tingley D. Vision screening essentials: screening today for eye disorders in the pediatric patient. Pediatrics in Review. 2010;28(2):53–61.
25. Wagner H, Fink BA, Zadnik K. Sex- and gender-based differences in healthy and diseased eyes. American Optometric Association. 2008;79(11):636–652.
26. Whiteside M, Wallhagen M, Pettengill E. Sensory impairment in older adults Part 2 Vision loss. American Journal of Nursing. 2006;106:52–62.
27. Zucker JL. The eyelids: some common disorders seen in everyday practice. Geriatrics. 2009;64(4):14–16 19, 28.