Neurologic System
Outline

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
• Quick Assessment for Common Conditions
Brain Attack (Stroke, Cerebrovascular Accident)
Structure and Function
The nervous system can be divided into two parts—central and peripheral. The central nervous system (CNS) includes the brain and spinal cord. The peripheral nervous system includes all the nerve fibers outside the brain and spinal cord: the 12 pairs of cranial nerves, the 31 pairs of spinal nerves, and all their branches. The peripheral nervous system carries sensory (afferent) messages to the CNS from sensory receptors, motor (efferent) messages from the CNS out to muscles and glands, as well as autonomic messages that govern the internal organs and blood vessels.
The Central Nervous System (CNS)
Cerebral Cortex
The cerebral cortex is the cerebrum’s outer layer of nerve cell bodies, which looks like “gray matter” because it lacks myelin. Myelin is the white insulation on the axon that increases the conduction velocity of nerve impulses.
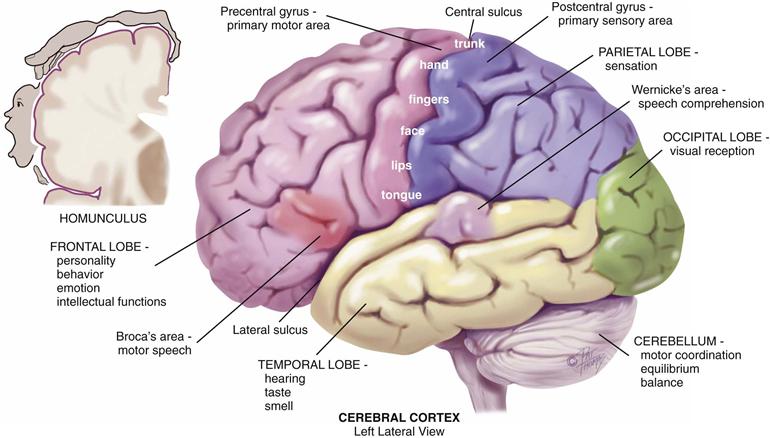
The cerebral cortex is the center for human’s highest functions, governing thought, memory, reasoning, sensation, and voluntary movement (Fig. 23-1). Each half of the cerebrum is a hemisphere; the left hemisphere is dominant in most (95%) people, including those who are left-handed.
23-1 Copyright © (2006) © Pat Thomas, 2006.
Each hemisphere is divided into four lobes: frontal, parietal, temporal, and occipital. The lobes have certain areas that mediate specific functions.
• The frontal lobe has areas concerned with personality, behavior, emotions, and intellectual function.
• The precentral gyrus of the frontal lobe initiates voluntary movement.
• The parietal lobe’s postcentral gyrus is the primary center for sensation.
• The occipital lobe is the primary visual receptor center.
• The temporal lobe behind the ear has the primary auditory reception center with functions of hearing, taste, and smell.
• Wernicke’s area in the temporal lobe is associated with language comprehension. When damaged in the person’s dominant hemisphere, receptive aphasia results. The person hears sound, but it has no meaning, like hearing a foreign language.
• Broca’s area in the frontal lobe mediates motor speech. When injured in the dominant hemisphere, expressive aphasia results; the person cannot talk. The person can understand language and knows what he or she wants to say, but can produce only a garbled sound.
Damage to any of these specific cortical areas produces a corresponding loss of function: motor weakness, paralysis, loss of sensation, or impaired ability to understand and process language. Damage occurs when the highly specialized neurologic cells are deprived of their blood supply, such as when a cerebral artery becomes occluded or when vascular bleeding or vasospasm occurs.
Basal Ganglia
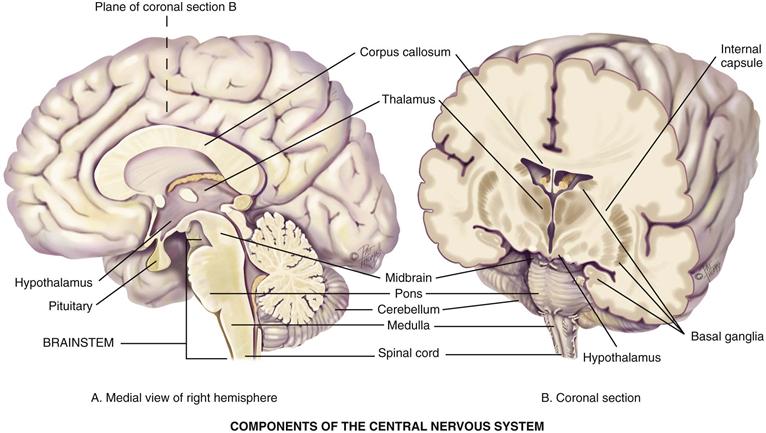
The basal ganglia are large bands of gray matter buried deep within the two cerebral hemispheres that form the subcortical associated motor system (the extrapyramidal system) (Fig. 23-2). They help to initiate and coordinate movement and control automatic associated movements of the body (e.g., the arm swing alternating with the legs during walking).
23-2 Copyright © (2006) © Pat Thomas, 2006.
Thalamus
The thalamus is the main relay station where the sensory pathways of the spinal cord, cerebellum, and brainstem form synapses (sites of contact between two neurons) on their way to the cerebral cortex.
Hypothalamus
The hypothalamus is a major respiratory center with basic vital functions: temperature, appetite, sex drive, heart rate, and blood pressure (BP) control; sleep center; anterior and posterior pituitary gland regulator; and coordinator of autonomic nervous system activity and stress response.
Cerebellum
The cerebellum is a coiled structure located under the occipital lobe that is concerned with motor coordination of voluntary movements, equilibrium (i.e., the postural balance of the body), and muscle tone. It does not initiate movement but coordinates and smoothes it (e.g., the complex and quick coordination of many different muscles needed in playing the piano, swimming, or juggling). It is like the “automatic pilot” on an airplane in that it adjusts and corrects the voluntary movements but operates entirely below the conscious level.
Brainstem
The brainstem is the central core of the brain consisting of mostly nerve fibers. Cranial nerves III through XII originate from nuclei in the brainstem. It has three areas:
1. Midbrain—the most anterior part of the brainstem that still has the basic tubular structure of the spinal cord. It merges into the thalamus and hypothalamus. It contains many motor neurons and tracts.
2. Pons—the enlarged area containing ascending sensory and descending motor tracts. It has two respiratory centers (pneumotaxic and apneustic) that coordinate with the main respiratory center in the medulla.
3. Medulla—the continuation of the spinal cord in the brain that contains all ascending and descending fiber tracts. It has vital autonomic centers (respiration, heart, gastrointestinal function), as well as nuclei for cranial nerves VIII through XII. Pyramidal decussation (crossing of the motor fibers) occurs here (see p. 625).
Spinal Cord
The spinal cord is the long, cylindric structure of nervous tissue about as big around as the little finger. It occupies the upper two thirds of the vertebral canal from the medulla to lumbar vertebrae L1-L2. Its white matter is bundles of myelinated axons that form the main highway for ascending and descending fiber tracts that connect the brain to the spinal nerves. It mediates reflexes of posture control, urination, and pain response. Its nerve cell bodies, or gray matter, are arranged in a butterfly shape with anterior and posterior “horns.”
The vertebral canal continues down beyond the spinal cord for several inches. The lumbar cistern is inside this space and is the favored spot to withdraw samples of cerebrospinal fluid (CSF).
Pathways of the CNS
Crossed representation is a notable feature of the nerve tracts; the left cerebral cortex receives sensory information from and controls motor function to the right side of the body, whereas the right cerebral cortex likewise interacts with the left side of the body. Knowledge of where the fibers cross the midline will help you interpret clinical findings.
Sensory Pathways
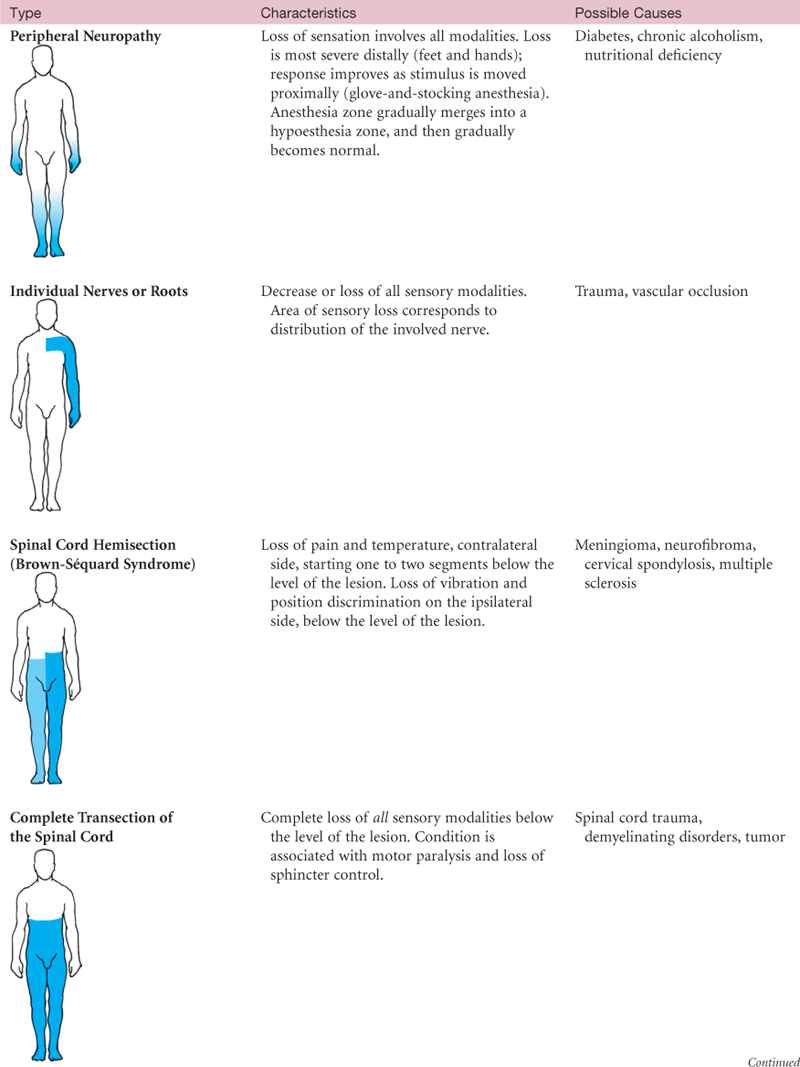
Millions of sensory receptors are embroidered into the skin, mucous membranes, muscles, tendons, and viscera. They monitor conscious sensation, internal organ functions, body position, and reflexes. Sensation travels in the afferent fibers in the peripheral nerve, then through the posterior (dorsal) root, and then into the spinal cord. There, it may take one of two routes—the spinothalamic tract or the posterior (dorsal) columns (Fig. 23-3).
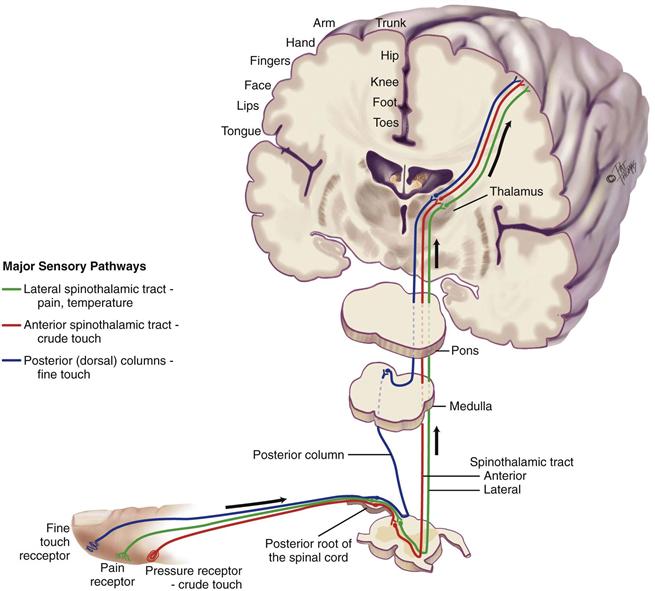
Spinothalamic Tract
The spinothalamic tract contains sensory fibers that transmit the sensations of pain, temperature, and crude or light touch (i.e., not precisely localized). The fibers enter the dorsal root of the spinal cord and synapse with a second sensory neuron. The second-order neuron fibers cross to the opposite side and ascend up the spinothalamic tract to the thalamus. Fibers carrying pain and temperature sensations ascend the lateral spinothalamic tract, whereas those of crude touch form the anterior spinothalamic tract. At the thalamus, the fibers synapse with a third sensory neuron, which carries the message to the sensory cortex for full interpretation.
Posterior (Dorsal) Columns
These fibers conduct the sensations of position, vibration, and finely localized touch.
• Position (proprioception)—Without looking, you know where your body parts are in space and in relation to each other
• Vibration—Feeling vibrating objects
• Finely localized touch (stereognosis)—Without looking, you can identify familiar objects by touch
These fibers enter the dorsal root and proceed immediately up the same side of the spinal cord to the brainstem. At the medulla, they synapse with a second sensory neuron and then cross. They travel to the thalamus, synapse again, and proceed to the sensory cortex, which localizes the sensation and makes full discrimination.
The sensory cortex is arranged in a specific pattern forming a corresponding “map” of the body (see the homunculus in Fig. 23-1). Pain in the right hand is perceived at its specific spot on the left cortex map. Some organs are absent from the brain map, such as the heart, liver, or spleen. You know you have one but you have no “felt image” of it. Pain originating in these organs is referred, because no felt image exists in which to have pain. Pain is felt “by proxy” by another body part that does have a felt image. For example, pain in the heart is referred to the chest, shoulder, and left arm, which were its neighbors in fetal development. Pain originating in the spleen is felt on the top of the left shoulder.
Motor Pathways
Corticospinal or Pyramidal Tract (Fig. 23-4)
The area has been named “pyramidal” because it originates in pyramidal-shaped cells in the motor cortex. Motor nerve fibers originate in the motor cortex and travel to the brainstem, where they cross to the opposite or contralateral side (pyramidal decussation) and then pass down in the lateral column of the spinal cord. At each cord level, they synapse with a lower motor neuron contained in the anterior horn of the spinal cord. Ten percent of corticospinal fibers do not cross, and these descend in the anterior column of the spinal cord. Corticospinal fibers mediate voluntary movement, particularly very skilled, discrete, purposeful movements, such as writing.
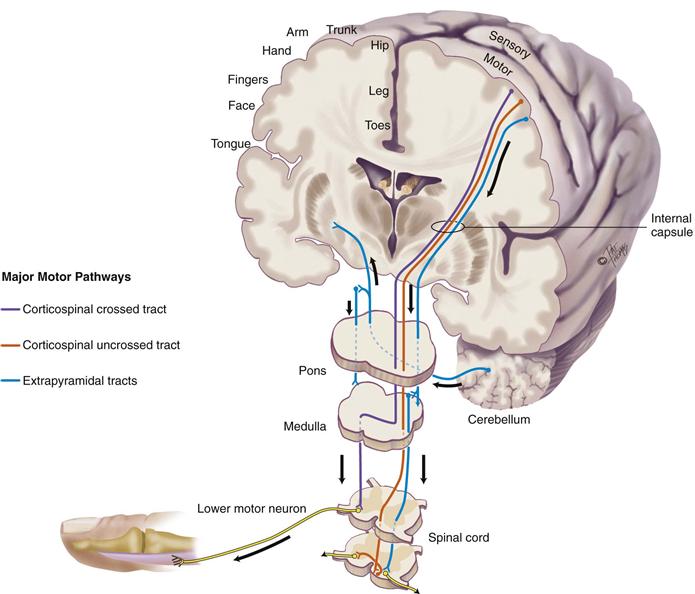
The corticospinal tract is a newer, “higher,” motor system that permits humans to have very skilled and purposeful movements. The tract’s origin in the motor cortex is arranged in a specific pattern called somatotopic organization. It is another body map, this one of a person, or homunculus, hanging “upside down” (see Fig. 23-1). Body parts are not equally represented on the map, and the homunculus looks distorted. To use political terms, it is more like an electoral map than a geographic map. That is, body parts whose movements are relatively more important to humans (e.g., the hand) occupy proportionally more space on the brain map.
Extrapyramidal Tracts
The extrapyramidal tracts include all the motor nerve fibers originating in the motor cortex, basal ganglia, brainstem, and spinal cord that are outside the pyramidal tract. This is a phylogenetically older, “lower,” more primitive motor system. These subcortical motor fibers maintain muscle tone and control body movements, especially gross automatic movements, such as walking.
Cerebellar System
This complex motor system coordinates movement, maintains equilibrium, and helps maintain posture. The cerebellum receives information about the position of muscles and joints, the body’s equilibrium, and what kind of motor messages are being sent from the cortex to the muscles. The information is integrated, and the cerebellum uses feedback pathways to exert its control back on the cortex or down to lower motor neurons in the spinal cord. This entire process occurs on a subconscious level.
Upper and Lower Motor Neurons
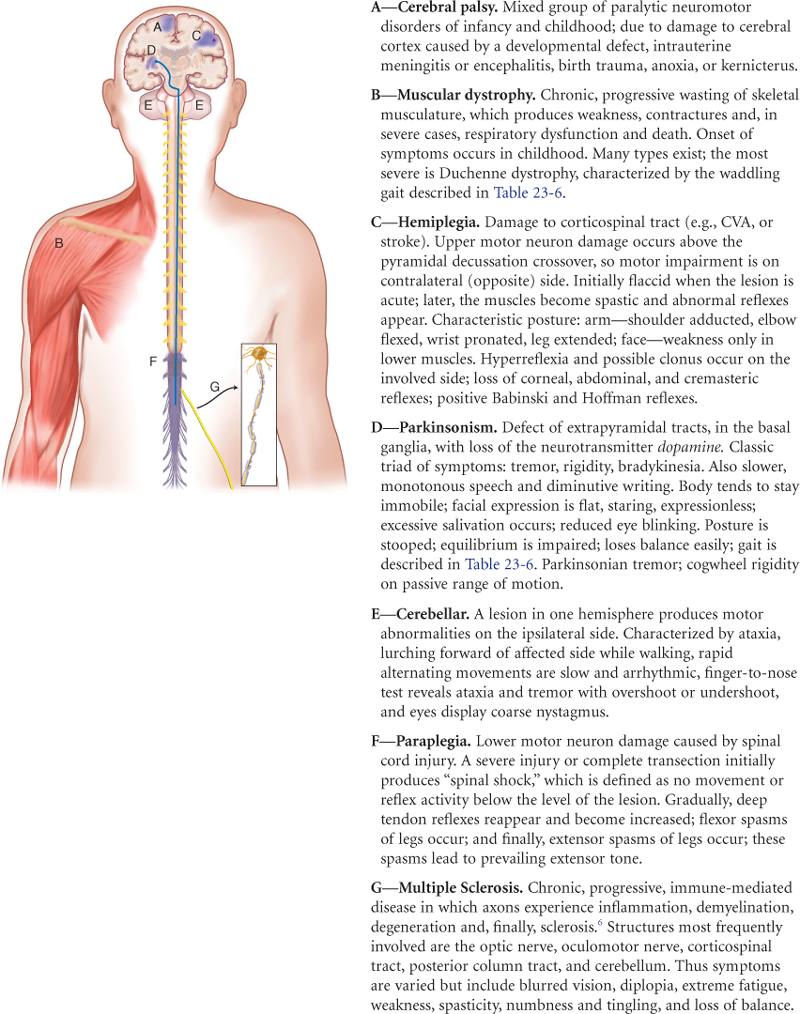
Upper motor neurons are a complex of all the descending motor fibers that can influence or modify the lower motor neurons. Upper motor neurons are located completely within the CNS. The neurons convey impulses from motor areas of the cerebral cortex to the lower motor neurons in the anterior horn cells of the spinal cord (Fig. 23-5). Examples of upper motor neurons are corticospinal, corticobulbar, and extrapyramidal tracts. Examples of upper motor neuron diseases are cerebrovascular accident, cerebral palsy, and multiple sclerosis.
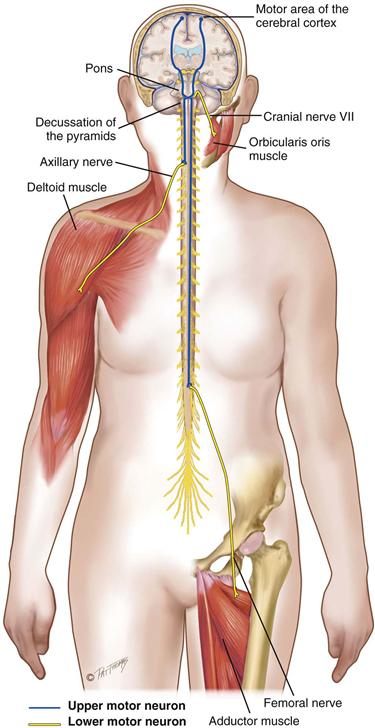
Lower motor neurons are located mostly in the peripheral nervous system. The cell body of the lower motor neuron is located in the anterior gray column of the spinal cord, but the nerve fiber extends from here to the muscle. The lower motor neuron is the “final common pathway,” because it funnels many neural signals here and it provides the final direct contact with the muscles. Any movement must be translated into action by lower motor neuron fibers. Examples of lower motor neurons are cranial nerves and spinal nerves of the peripheral nervous system. Examples of lower motor neuron diseases are spinal cord lesions, poliomyelitis, and amyotrophic lateral sclerosis.
The Peripheral Nervous System
A nerve is a bundle of fibers outside the CNS. The peripheral nerves carry input to the CNS via their sensory afferent fibers and deliver output from the CNS via the efferent fibers.
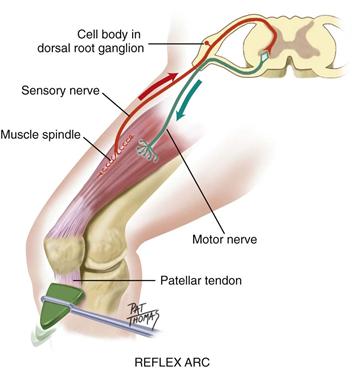
Reflex Arc
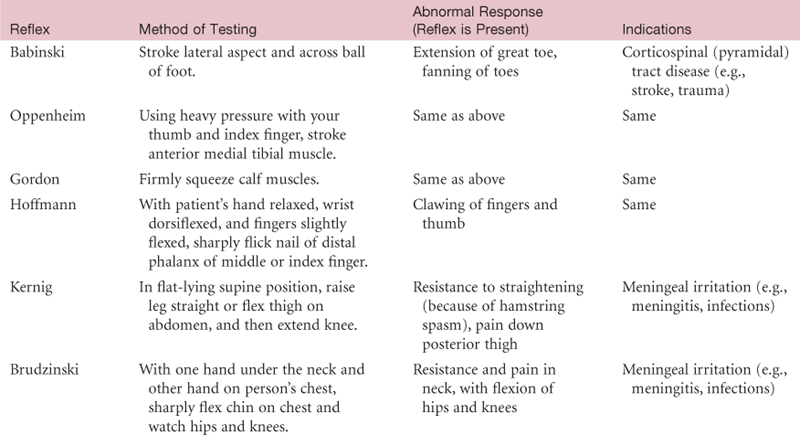
Reflexes are basic defense mechanisms of the nervous system. They are involuntary, operating below the level of conscious control and permitting a quick reaction to potentially painful or damaging situations. Reflexes also help the body maintain balance and appropriate muscle tone. There are four types of reflexes: (1) Deep tendon reflexes (myotatic), e.g., patellar [or knee jerk]; (2) Superficial, e.g., corneal reflex, abdominal reflex; (3) Visceral (organic), e.g., pupillary response to light and accommodation; (4) Pathologic (abnormal), e.g., Babinski (or extensor plantar) reflex.
The fibers that mediate the reflex are carried by a specific spinal nerve. In the simplest reflex, tapping the tendon stretches the muscle spindles in the muscle, which activates the sensory afferent nerve. The sensory afferent fibers carry the message from the receptor and travel through the dorsal root into the spinal cord (Fig. 23-6). They synapse directly in the cord with the motor neuron in the anterior horn. Motor efferent fibers leave via the ventral root and travel to the muscle, stimulating a sudden contraction.
23-6
The deep tendon (myotatic, or stretch) reflex has five components: (1) an intact sensory nerve (afferent); (2) a functional synapse in the cord; (3) an intact motor nerve fiber (efferent); (4) the neuromuscular junction; and (5) a competent muscle.
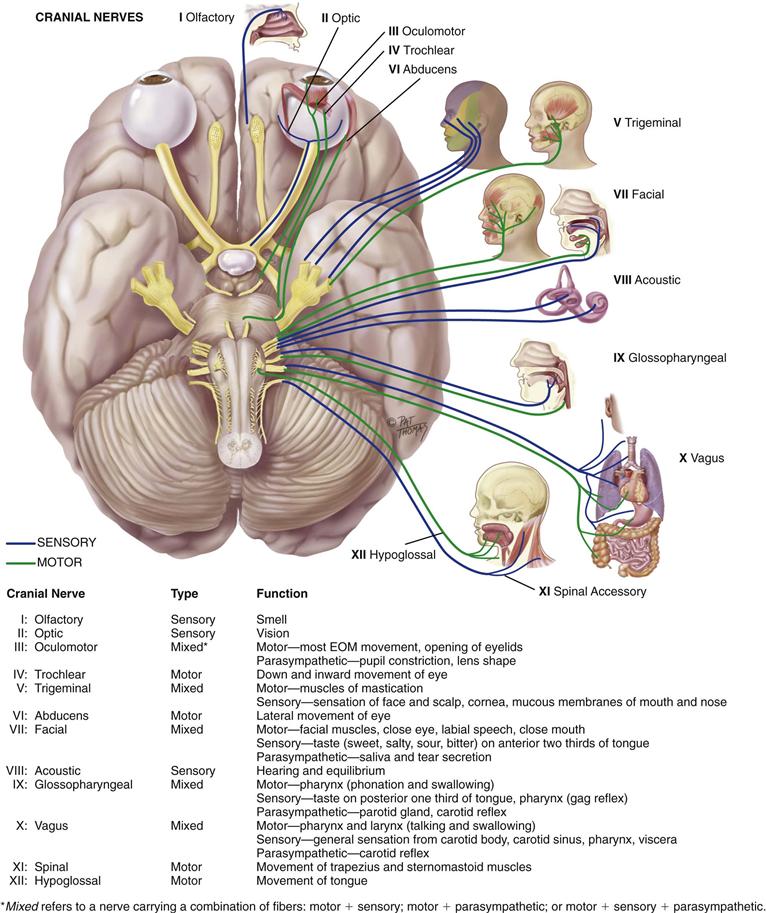
Cranial Nerves
Cranial nerves enter and exit the brain rather than the spinal cord (Fig. 23-7). Cranial nerves I and II extend from the cerebrum; cranial nerves III through XII extend from the lower diencephalon and brainstem. The 12 pairs of cranial nerves supply primarily the head and neck, except the vagus nerve (Lat. vagus, or wanderer, as in “vagabond”), which travels to the heart, respiratory muscles, stomach, and gallbladder.
23-7 Copyright © (2006) © Pat Thomas, 2006.
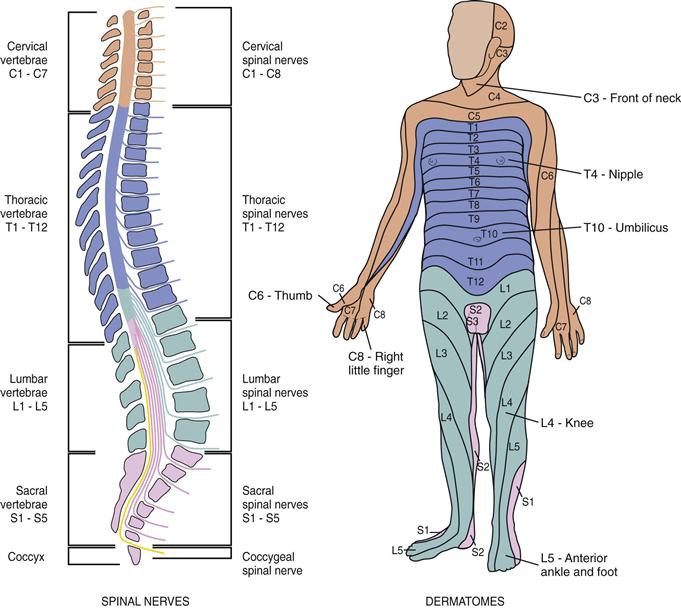
Spinal Nerves
The 31 pairs of spinal nerves arise from the length of the spinal cord and supply the rest of the body. They are named for the region of the spine from which they exit: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. They are “mixed” nerves because they contain both sensory and motor fibers. The nerves enter and exit the cord through roots—sensory afferent fibers through the posterior or dorsal roots, and motor efferent fibers through the anterior or ventral roots.
The nerves exit the spinal cord in an orderly ladder. Each nerve innervates a particular segment of the body. Dermal segmentation is the cutaneous distribution of the various spinal nerves.
A dermatome is a circumscribed skin area that is supplied mainly from one spinal cord segment through a particular spinal nerve (Fig. 23-8). The dermatomes overlap, which is a form of biologic insurance. That is, if one nerve is severed, most of the sensations can be transmitted by the one above and the one below. Do not attempt to memorize all dermatome segments; just focus on the following as useful landmarks:
• The thumb, middle finger, and fifth finger are each in the dermatomes of C6, C7, and C8.
• The axilla is at the level of T1.
• The nipple is at the level of T4.
• The umbilicus is at the level of T10.
23-8
Autonomic Nervous System
The peripheral nervous system is composed of cranial nerves and spinal nerves. These nerves carry fibers that can be divided functionally into two parts—somatic and autonomic. The somatic fibers innervate the skeletal (voluntary) muscles; the autonomic fibers innervate smooth (involuntary) muscles, cardiac muscle, and glands. The autonomic system mediates unconscious activity. Although a description of the autonomic system is beyond the scope of this book, its overall function is to maintain homeostasis of the body.
 Developmental Competence
Developmental Competence
Infants
The neurologic system is not completely developed at birth. Motor activity in the newborn is under the control of the spinal cord and medulla. Very little cortical control exists, and the neurons are not yet myelinated. Movements are directed primarily by primitive reflexes. As the cerebral cortex develops during the first year, it inhibits these reflexes and they disappear at predictable times. Persistence of the primitive reflexes is an indication of CNS dysfunction.
The infant’s sensory and motor development proceed along with the gradual acquisition of myelin, because myelin is needed to conduct most impulses. The process of myelinization follows a cephalocaudal and proximodistal order (head, neck, trunk, and extremities). This is just the order in which we observe the infant gaining motor control (lifts head, lifts head and shoulders, rolls over, moves whole arm, uses hands, walks). As the milestones are achieved, each is more complex and coordinated. Milestones occur in an orderly sequence, although the exact age of occurrence may vary.
Sensation also is rudimentary at birth. The newborn needs a strong stimulus and then responds by crying and with whole body movements. As myelinization develops, the infant is able to localize the stimulus more precisely and to make a more accurate motor response.
The Aging Adult
The aging process causes a general atrophy with a steady loss of neuron structure in the brain and spinal cord. This causes a decrease in weight and volume with a thinning of the cerebral cortex, reduced subcortical brain structures, and expansion of the ventricles.9 Neuron loss leads many people older than 65 years to show signs that, in the younger adult, would be considered abnormal, such as general loss of muscle bulk; loss of muscle tone in the face, in the neck, and around the spine; decreased muscle strength; impaired fine coordination and agility; loss of vibratory sense at the ankle; decreased or absent Achilles reflex; loss of position sense at the big toe; pupillary miosis; irregular pupil shape; and decreased pupillary reflexes.
The velocity of nerve conduction decreases between 5% and 10% with aging, making the reaction time slower in some older persons. An increased delay at the synapse also occurs, so the impulse takes longer to travel. As a result, touch and pain sensation, taste, and smell may be diminished.
The motor system may show a general slowing down of movement. Muscle strength and agility decrease. A generalized decrease occurs in muscle bulk, which is most apparent in the dorsal hand muscles. Muscle tremors may occur in the hands, head, and jaw, along with possible repetitive facial grimacing (dyskinesias).
Aging has a progressive decrease in cerebral blood flow and oxygen consumption. In some people, this causes dizziness and a loss of balance with position change. These people need to be taught to get up slowly. Otherwise they have an increased risk for falls and resulting injuries. In addition, older people may forget they fell, which makes it hard to diagnose the cause of the injury.
When they are in good health, aging people walk about as well as they did during their middle and younger years, except more slowly and more deliberately. Some survey the ground for obstacles or uneven terrain. Some show a hesitation and a slightly wayward path.
 Culture and Genetics
Culture and Genetics
Stroke is the third most common cause of death in the United States.19 The overall prevalence of stroke in adults older than 20 years is 2.9%. There is racial/ethnic disparity here because 6% of American Indian/Alaska Natives have had a stroke, 4% of African Americans, 2.6% of Hispanics, 2.3% of whites, and only 1.6% of Asian/Pacific Islanders. Further, African Americans, American Indian/Alaska Natives (AI/AN), Asian/Pacific Islanders, and Hispanics die from stroke at younger ages than do whites.19
There is geographic disparity; many states with high stroke mortality are concentrated in the U.S. southeast region, called the “stroke belt.” This may occur because of the high proportion of people who live in this region who have two or more of the major modifiable risk factors for stroke (high BP, high cholesterol, diabetes, current smoking, physical inactivity, or obesity). And why would this occur? Perhaps it is a combination of factors: cultural norms for diet and exercise, poverty, lack of economic opportunity, social isolation, lack of access to health care and preventive services.3
The disparity in prevalence among racial groups also is attributed to the disproportion in these groups of having risk factors for stroke. The AI/AN men have a higher prevalence of hypertension and high cholesterol than any other racial/ethnic group, and AI/AN women have the highest rate of obesity, current smoking, and diabetes.4 African Americans also have high rates of stroke, and their risk factors are the following: higher prevalence of hypertension and diabetes than whites, and less likely to have BP controlled or diabetes treated than whites.19 Because we know these risk factors lead to stroke, it is important to develop community policy to control such things as access to healthful foods, reduced tobacco exposure, opportunities for physical activity, and access to health care and health education.5
Objective Data
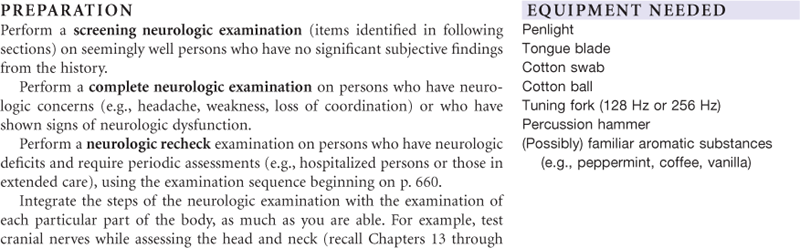
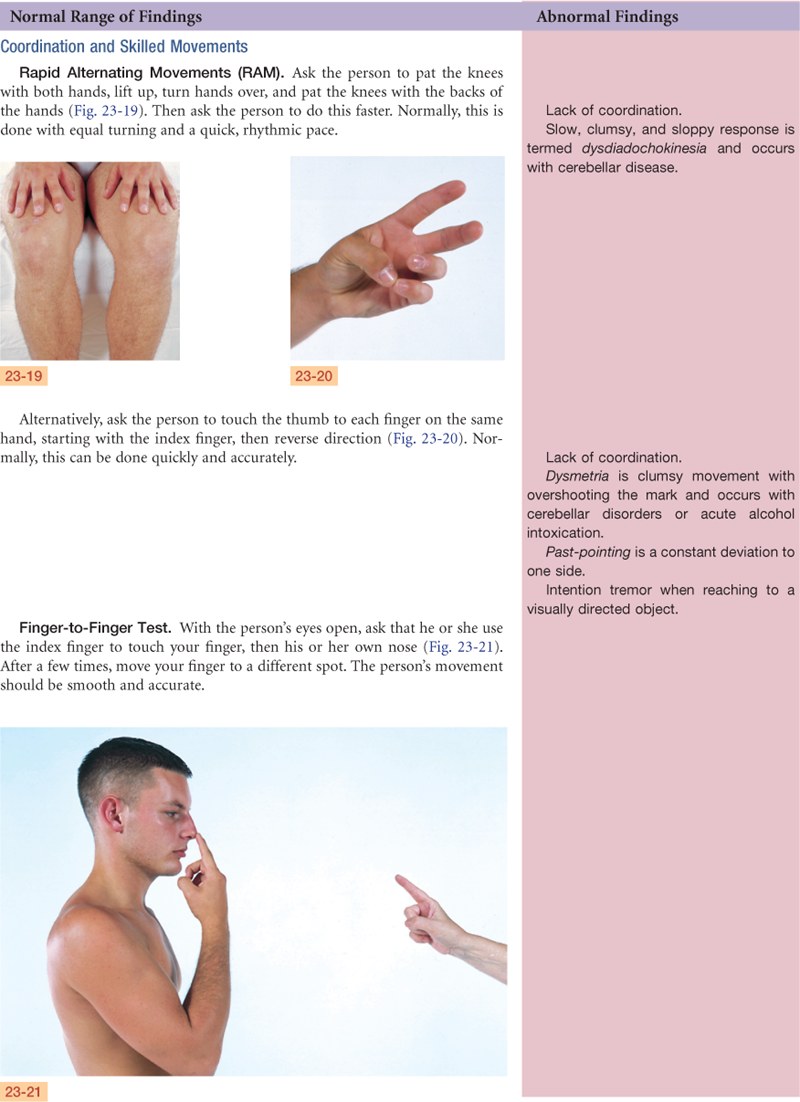
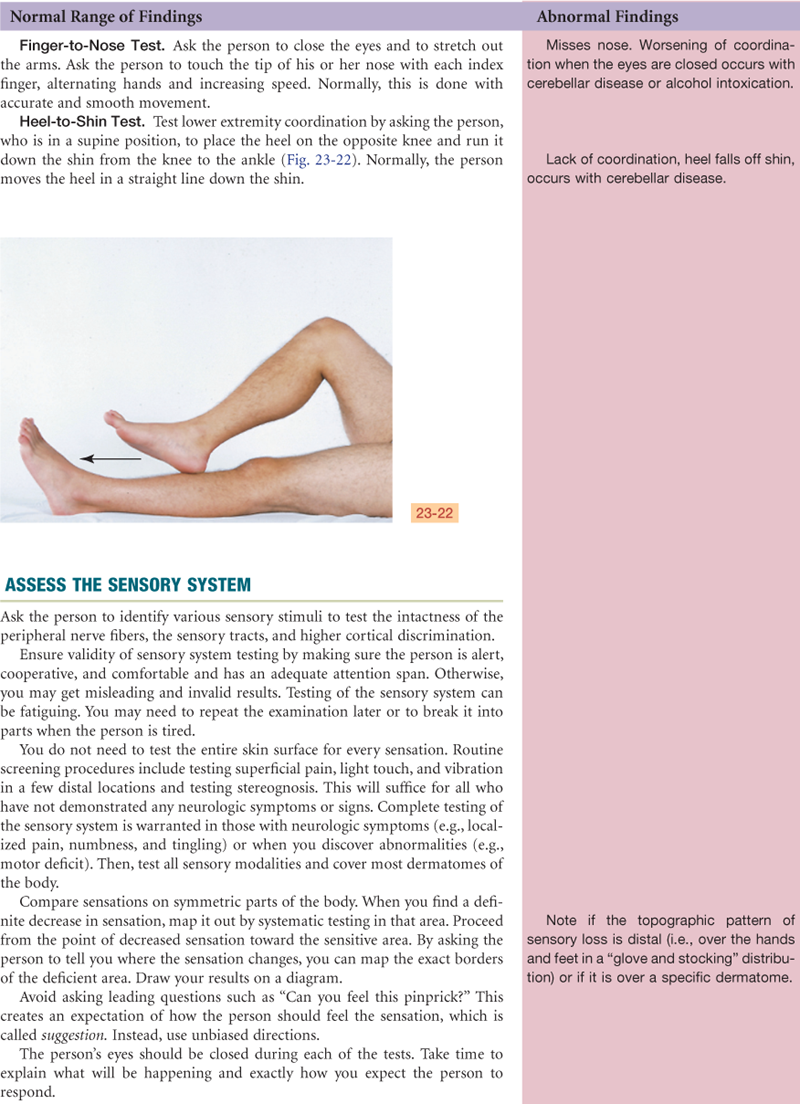


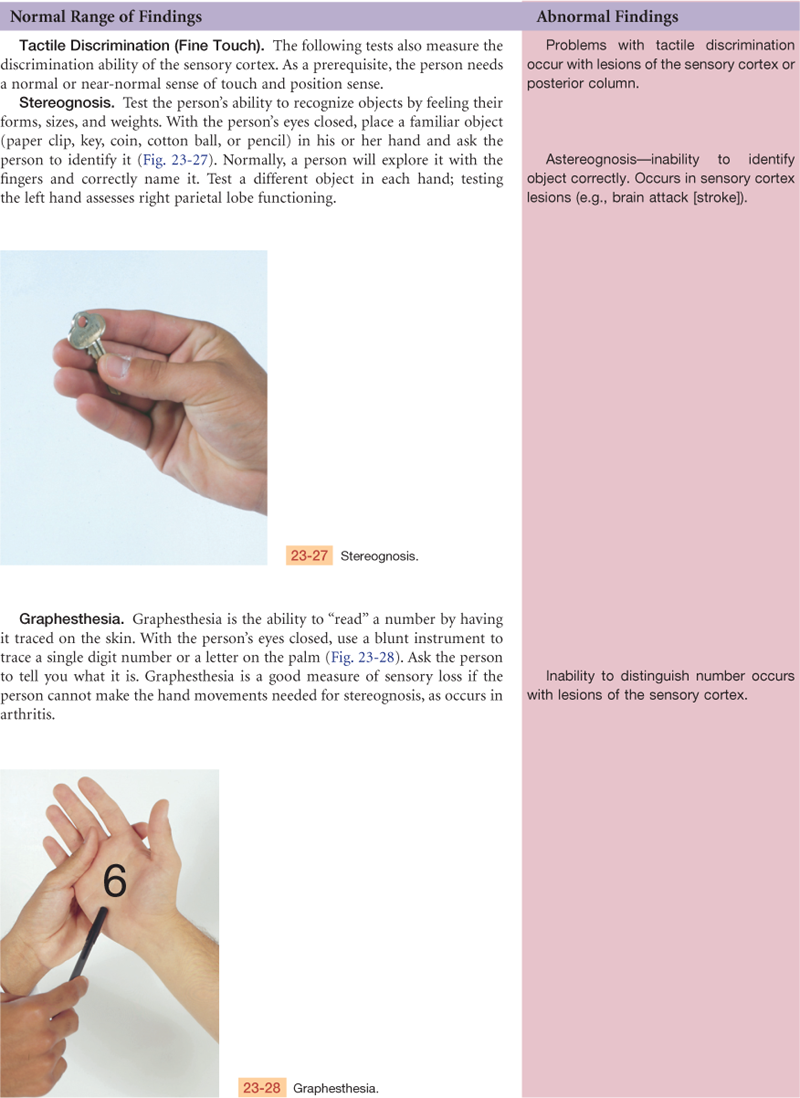
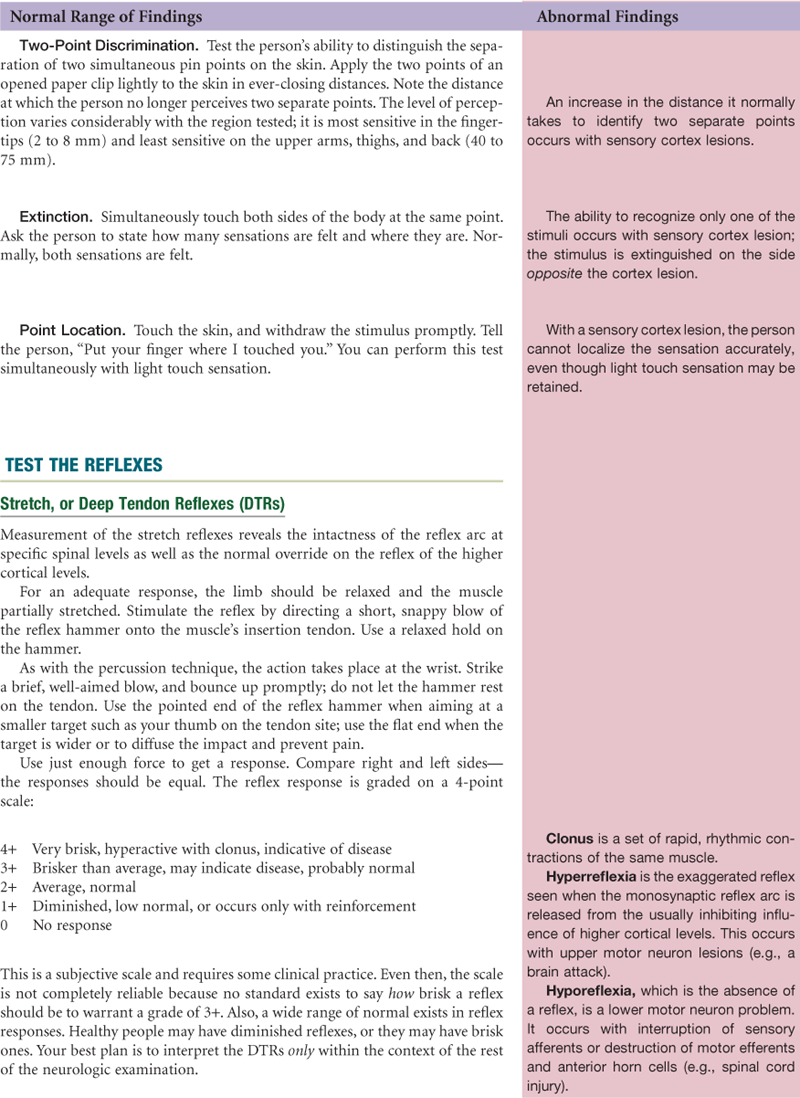
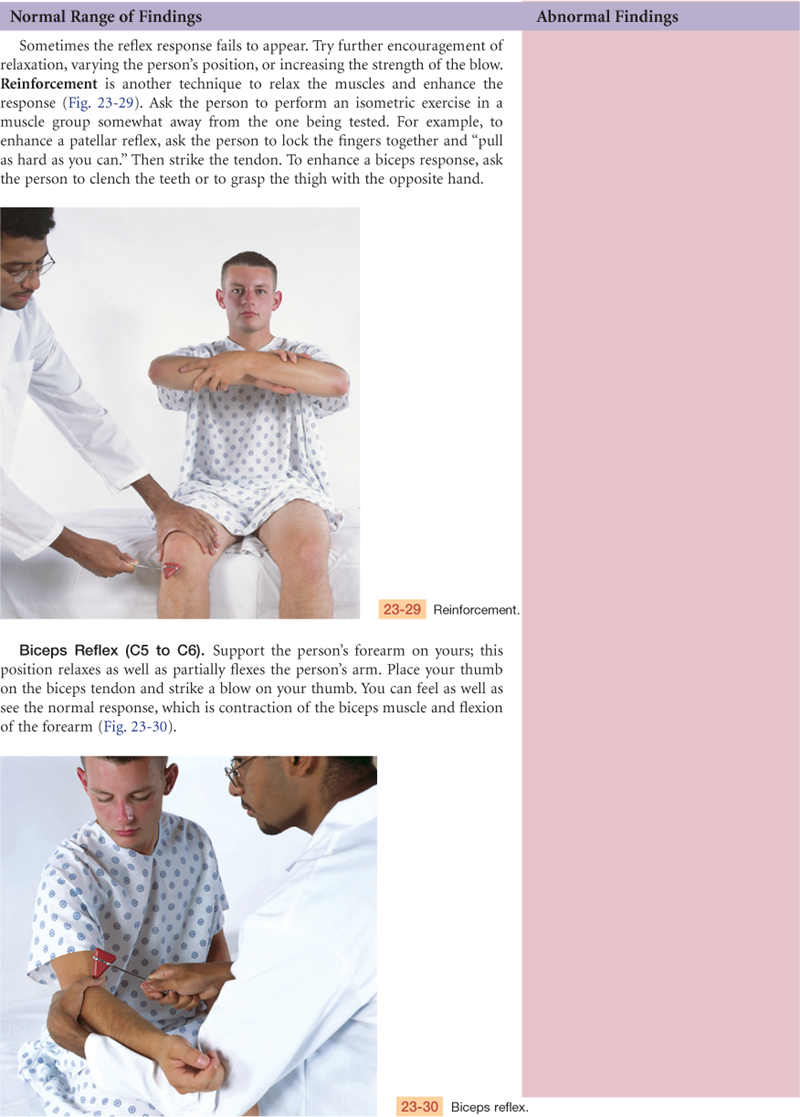
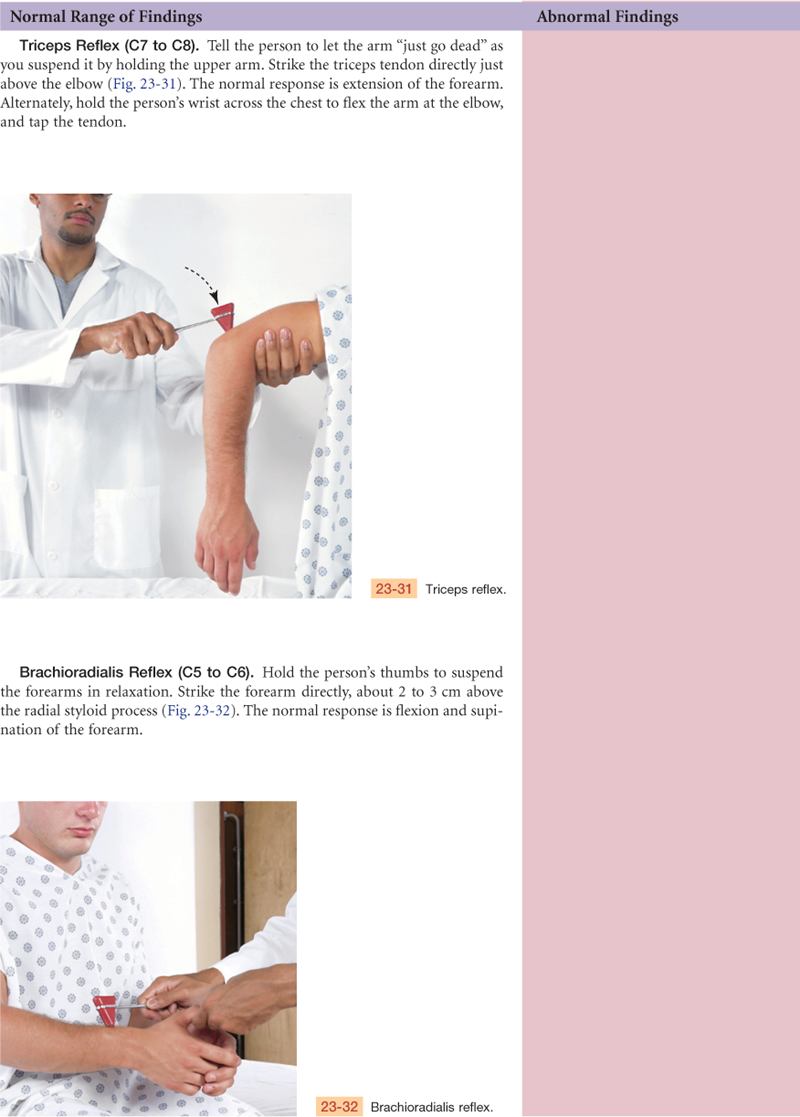
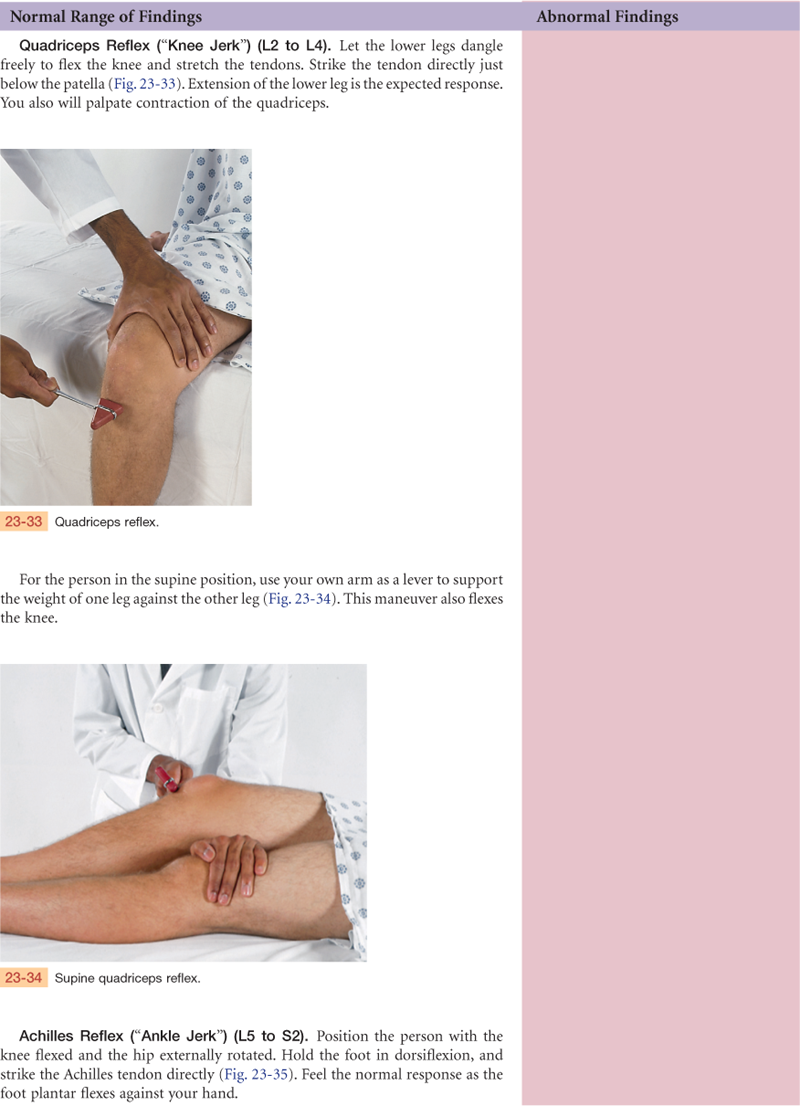
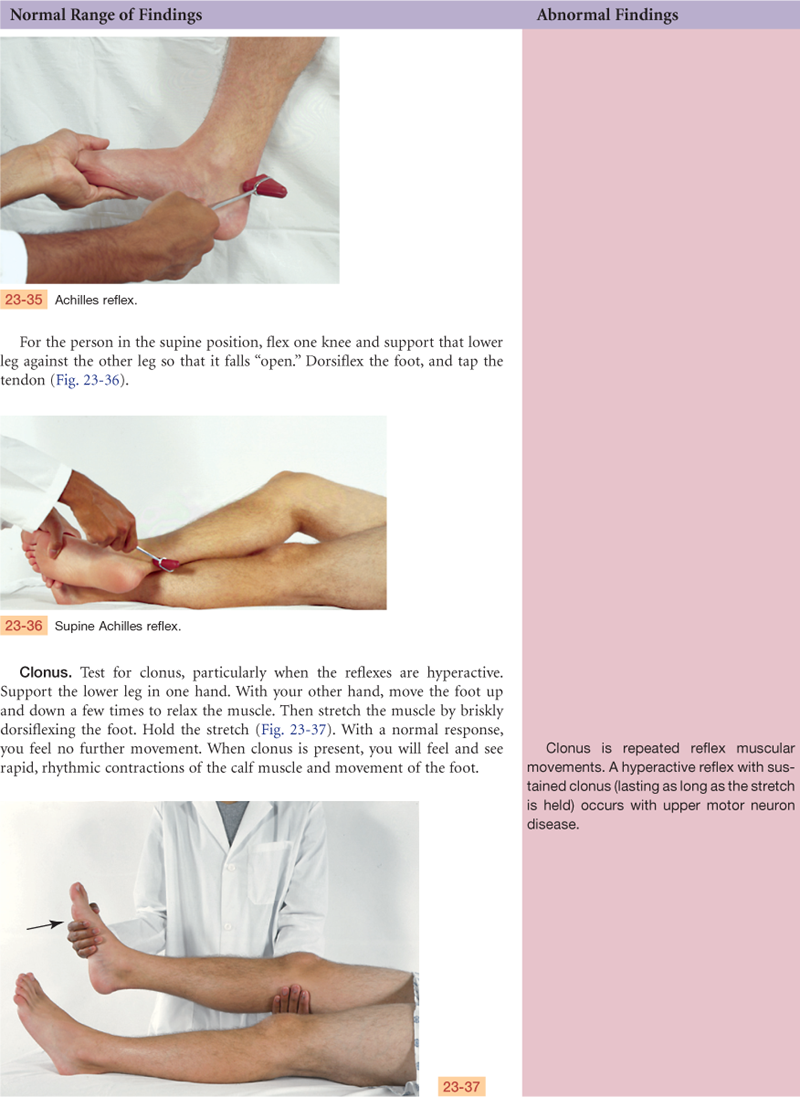
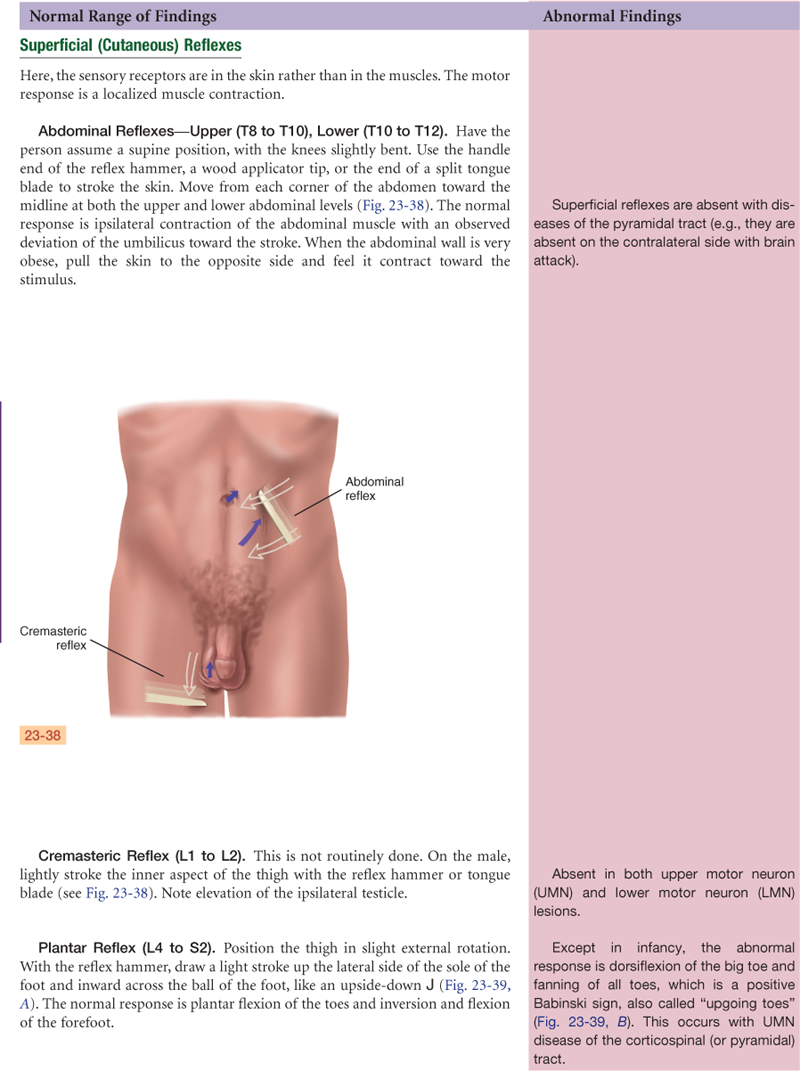
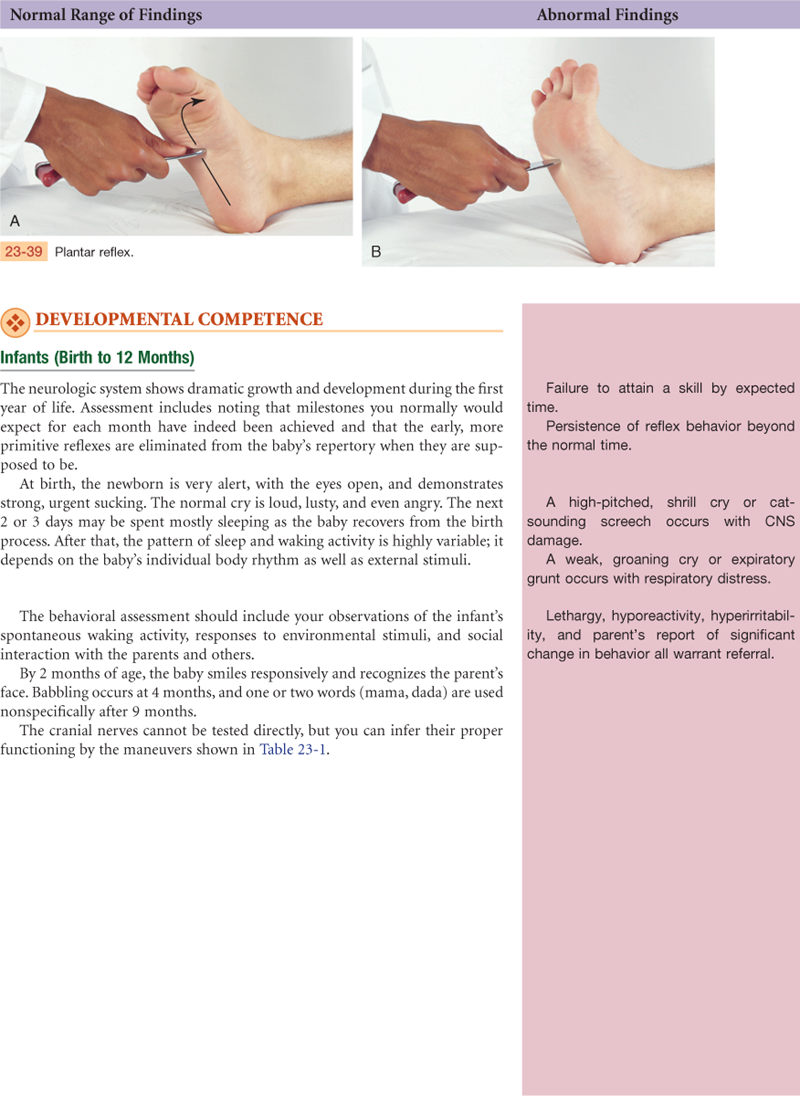
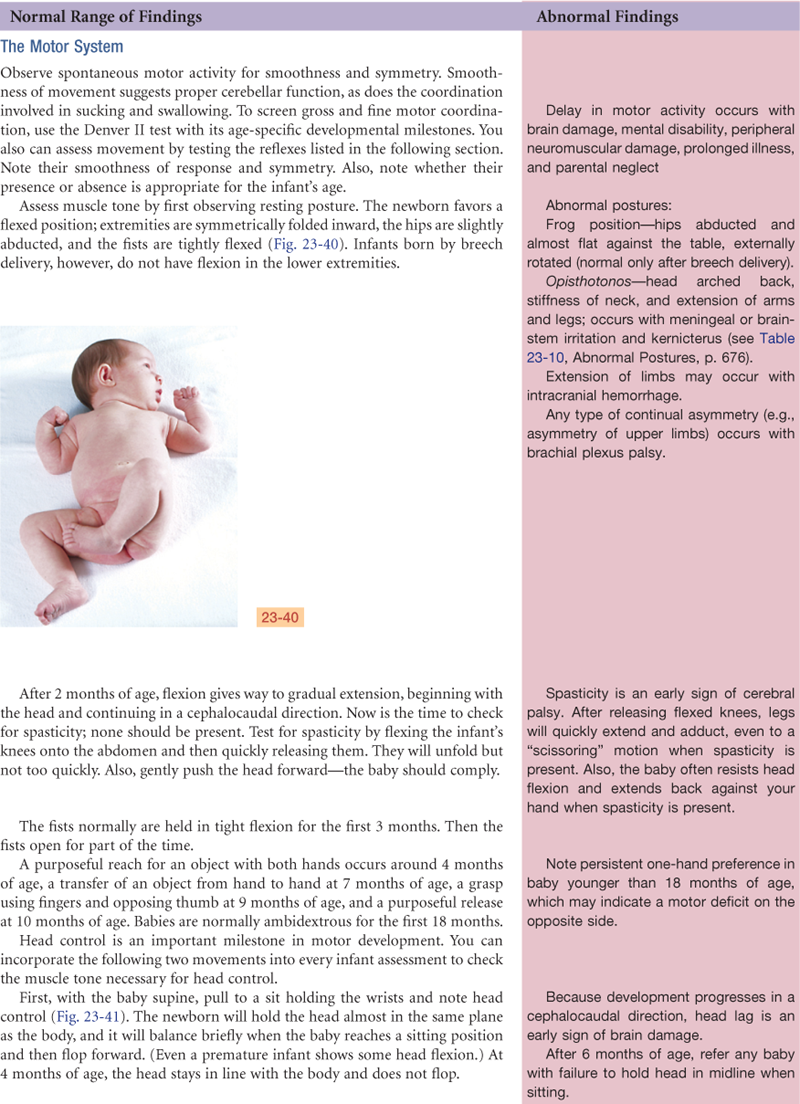
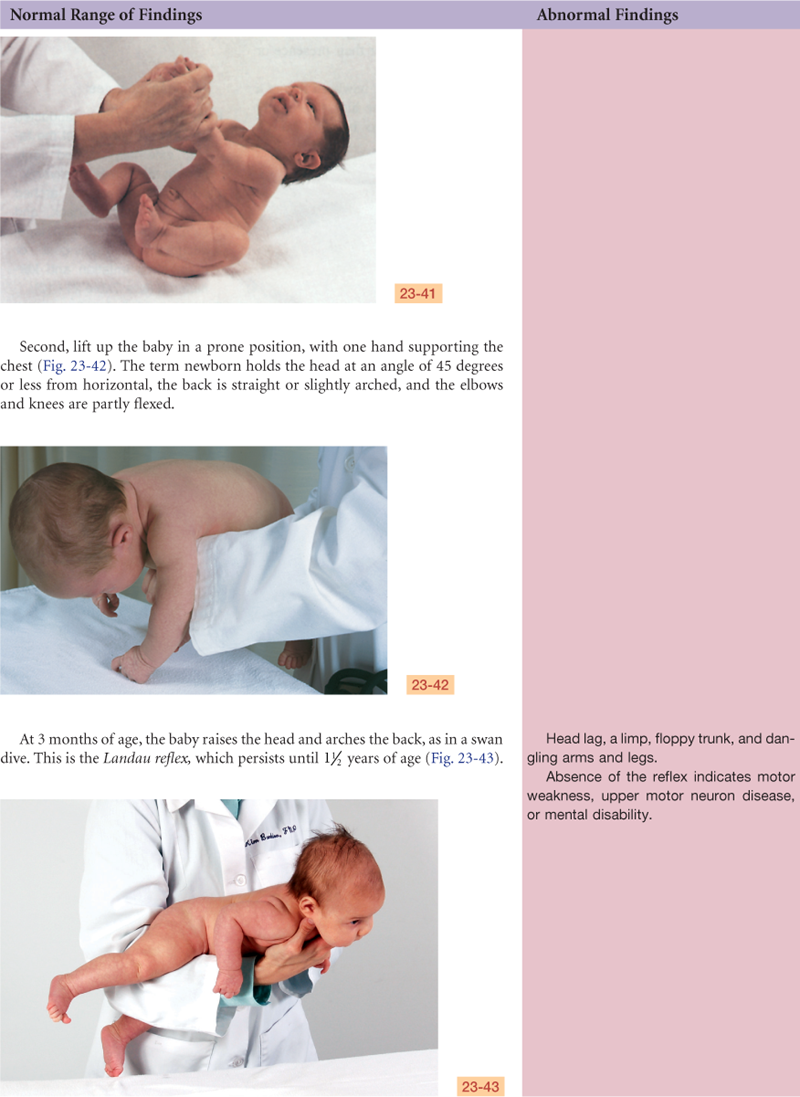
TABLE 23-1
Testing Cranial Nerve Function of Infants
| Cranial Nerve | Response |
| II, III, IV, VI | Optical blink reflex—shine light in open eyes, note rapid closure Size, shape, equality of pupils Regards face or close object Eyes follow movement |
| V | Rooting reflex, sucking reflex |
| VII | Facial movements (e.g., wrinkling forehead and nasolabial folds) symmetric when crying or smiling |
| VIII | Loud noise yields Moro reflex (until 4 mo) Acoustic blink reflex—infant blinks in response to a loud hand clap 30 cm (12 inches) from head (avoid making air current) Eyes follow direction of sound |
| IX, X | Swallowing, gag reflex Coordinated sucking and swallowing |
| XII | Pinch nose, infant’s mouth will open and tongue rise in midline |
 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
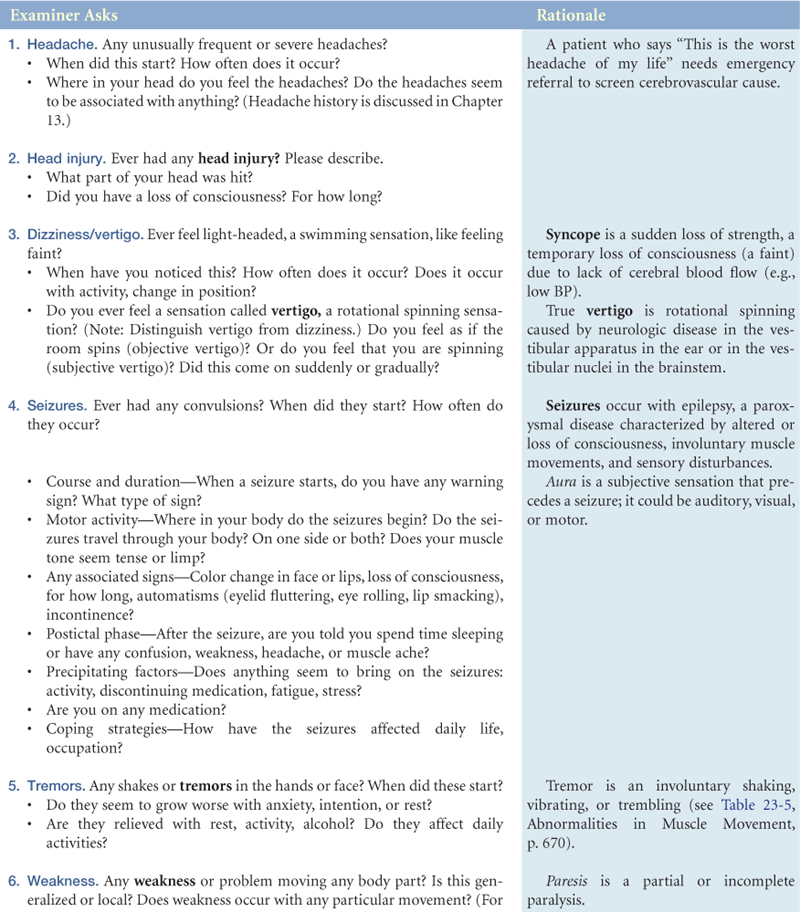
No unusually frequent or severe headaches, no head injury, dizziness or vertigo, seizures or tremors. No weakness, numbness or tingling, difficulty swallowing or speaking. Has no past history of stroke, spinal cord injury, meningitis, or alcoholism.
Objective
Mental Status: Appearance, behavior, and speech appropriate; alert and oriented to person, place, and time; recent and remote memory intact.
Cranial Nerves:
I: Identifies coffee and peppermint.
II: Vision 20/20 left eye, 20/20 right eye; peripheral fields intact by confrontation; fundi normal.
III, IV, VI: EOMs intact, no ptosis or nystagmus; pupils equal, round, react to light and accommodation (PERRLA).
V: Sensation intact and equal bilaterally; jaw strength equal bilaterally.
VII: Facial muscles intact and symmetric.
VIII: Hearing—whispered words heard bilaterally; Weber test—tone is heard midline without lateralization.
IX, X: Swallowing intact, gag reflex present, uvula rises in midline on phonation.
XI: Shoulder shrug, head movement intact and equal bilaterally.
XII: Tongue protrudes midline, no tremors.
Motor: No atrophy, weakness, or tremors. Gait smooth and coordinated, able to tandem walk, negative Romberg. Rapid alternating movements (RAM)—finger-to-nose smoothly intact.
Sensory: Pinprick, light touch, vibration intact. Stereognosis—able to identify key.
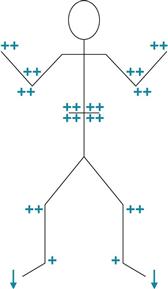
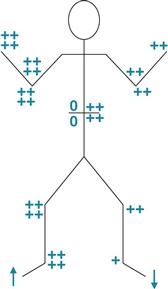
Reflexes: Normal abdominal, no Babinski sign, DTRs 2+ and = bilaterally with downgoing toes; see drawing below:
Assessment
Neurologic system intact, normal function
Focused Assessment: Clinical Case Study
J.T. is a 61-year-old white male carpenter with a large building firm who is admitted to the Rehabilitation Institute with a diagnosis of right hemiplegia and aphasia following a brain attack (CVA) 4 weeks PTA.
Subjective
Because of J.T.’s speech dysfunction, history provided by wife.
4 weeks PTA—complaint of severe headache, then sudden onset of collapse and loss of consciousness while at work. Did not strike head as fell. Transported by ambulance to Memorial Hospital where admitting physician said J.T. “probably had a stroke.” Right arm and leg were limp, and he remained unconscious. Admitted to critical care unit. Regained consciousness day 3 after admission, unable to move right side, unable to speak clearly or write. Remained in ICU 4 more days until “doctors were sure heart and breathing were steady.”
3 weeks PTA—transferred to medical floor where care included physical therapy 2 ×/day and passive ROM 4 ×/day.
Now—some improvement in right motor function. Bowel control achieved with use of commode same time each day (after breakfast). Bladder control improved. Some occasional incontinence, usually when cannot tell people he needs to urinate.
Objective
Mental Status: Dressed in jogging suit, sitting in wheelchair, appears alert with appropriate eye contact, listening intently to history. Speech is slow, requires great effort, able to give one-word answers that are appropriate but lack normal tone. Seems to understand all language spoken to him. Follows requests appropriately, within limits of motor weakness.
Cranial Nerves:
II: Acuity normal, fields by confrontation—right homonymous hemianopsia, fundi normal.
III, IV, VI: EOMs intact, no ptosis or nystagmus, PERRLA.
V: Sensation intact to pinprick and light touch. Jaw strength weak on right.
VII: Flat nasolabial fold on right, motor weakness on right lower face. Able to wrinkle forehead bilaterally, but unable to smile or bare teeth on right.
VIII: Hearing intact.
IX, X: Swallowing intact, gag reflex present, uvula rises midline on phonation.
XI: Shoulder shrug, head movement weaker on right.
XII: Tongue protrudes midline, no tremors.
Sensory: Pinprick and light touch present but diminished on right arm and leg. Vibration intact. Position sense impaired on right side. Stereognosis intact.
Motor: Right hand grip weak, right arm drifts, right leg weak, unable to support weight. Spasticity in right arm and leg muscles, limited range of motion on passive motion. Unable to stand up and walk unassisted. Unable to perform finger-to-nose or heel-to-shin on right side, left side smoothly intact.
Reflexes: Hyperactive 4+ with clonus, and upgoing toes in right leg. Abdominal and cremasteric reflexes absent on right.
Assessment
Impaired verbal communication R/T effects of CVA
Impaired physical mobility R/T neuromuscular impairment
Disturbed body image R/T effects of loss of body function
Self-care deficits: feeding, bathing, toileting, dressing/grooming R/T muscular weakness
Disturbed sensory perception (absent right visual fields) R/T neurologic impairment
Risk for injury R/T visual field deficit
Abnormal Findings
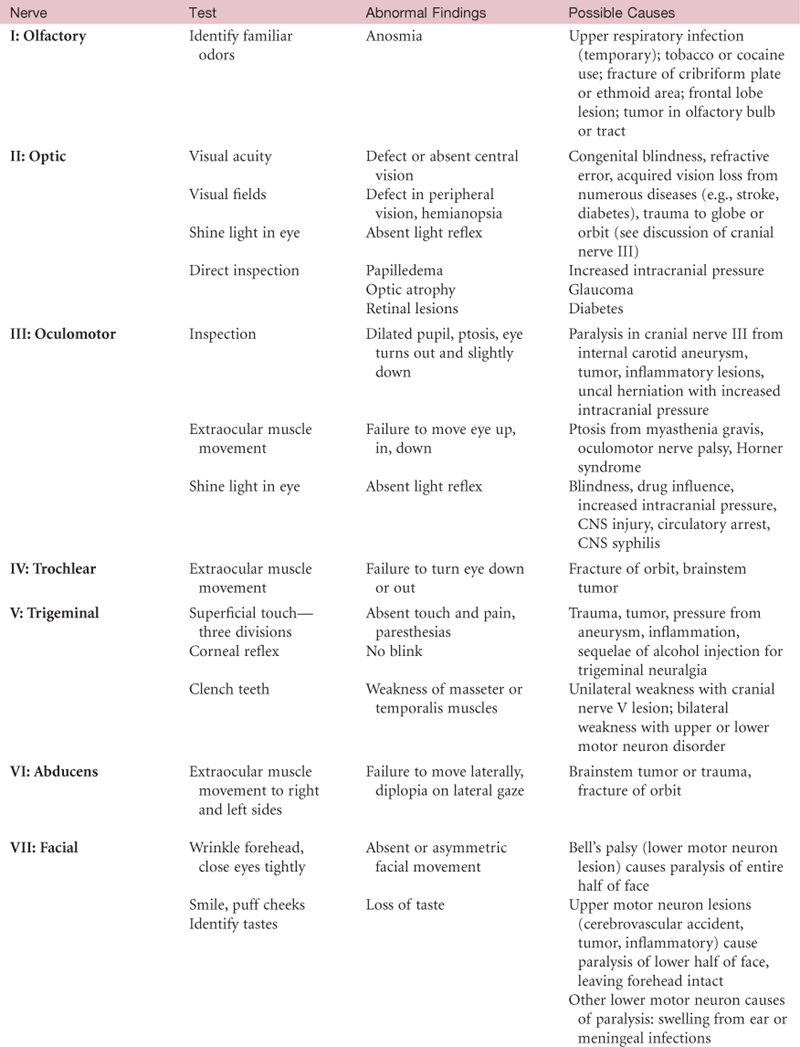
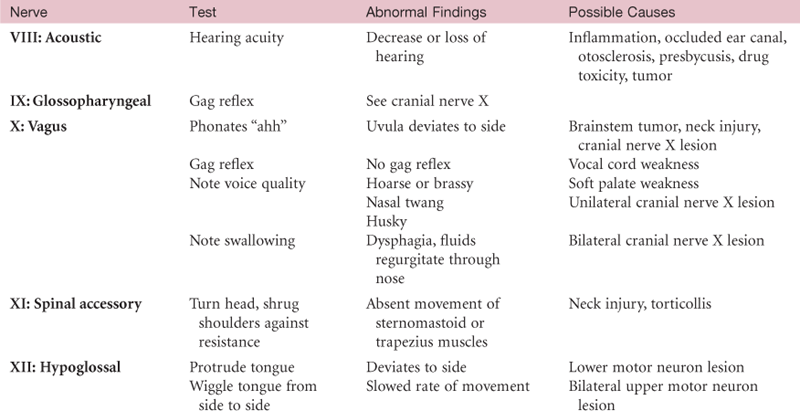
TABLE 23-4
| Condition | Description | Associated With |
| Flaccidity | Decreased muscle tone or hypotonia; muscle feels limp, soft, and flabby; muscle is weak and easily fatigued; limb feels like a rag doll | Lower motor neuron injury anywhere from the anterior horn cell in the spinal cord to the peripheral nerve (peripheral neuritis, poliomyelitis, Guillain-Barré syndrome); early cerebrovascular accident and spinal cord injury are flaccid at first |
| Spasticity | Increased tone or hypertonia; increased resistance to passive lengthening; then may suddenly give way (clasp-knife phenomenon) like a pocket knife sprung open | Upper motor neuron injury to corticospinal motor tract (e.g., paralysis with stroke develops spasticity days or weeks after incident) |
| Rigidity | Constant state of resistance (lead-pipe rigidity); resists passive movement in any direction; dystonia | Injury to extrapyramidal motor tracts (e.g., basal ganglia with parkinsonism) |
| Cogwheel rigidity | Type of rigidity in which the increased tone is released by degrees during passive range of motion so it feels like small, regular jerks | Parkinsonism |
Abnormal findings
For Advanced Practice
TABLE 23-7
Characteristics of Upper and Lower Motor Neuron Lesions
| Upper Motor Neuron Lesion | Lower Motor Neuron Lesion | |
| Weakness/paralysis | In muscles corresponding to distribution of damage in pyramidal tract lesion; usually in hand grip, arm extensors, leg flexors | In specific muscles served by damaged spinal segment, ventral root, or peripheral nerve |
| Location | Descending motor pathways that originate in the motor areas of cerebral cortex and carry impulses to the anterior horn cells of the spinal cord | Nerve cells that originate in the anterior horn of spinal cord or in brainstem and carry impulses by the spinal nerves or cranial nerves to the muscles, the “final common pathway” |
| Example | Brain attack or cerebrovascular accident | Poliomyelitis, herniated intervertebral disk |
| Muscle tone | Increased tone; spasticity | Loss of tone, flaccidity |
| Bulk | May have some atrophy from disuse; otherwise normal | Atrophy (wasting), may be marked |
| Abnormal movements | None | Fasciculations |
| Reflexes | Hyperreflexia, ankle clonus; diminished or absent superficial abdominal reflexes; positive Babinski sign | Hyporeflexia or areflexia; no Babinski sign, no pathologic reflexes |
| Possible nursing diagnoses | Risk for contractures; Impaired Physical Mobility | Impaired Physical Mobility |
Summary Checklist: Neurologic Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Neurologic Screening Examination
III, IV, VI: Extraocular muscles
Knee flexion—hop or shallow knee bend
Superficial pain and light touch—arms and legs
Neurologic Complete Examination
2. Cranial nerves II through XII
Superficial pain and light touch
Stereognosis, graphesthesia, two-point discrimination
Bibliography
1. Alzheimer’s Association. 10 signs of Alzheimer’s. Retrieved June 9, 2010, from www.alz.org/alzheimers_disease_10_signs_of_alzheimers.asp; 2010.
2. Budson A, Price B. Memory dysfunction. New England Journal of Medicine. 2005;352(7):692–699.
3. Casper ML, Barnett E, Williams GI, et al. Atlas of stroke mortality: racial, ethnic, and geographic disparities in the United States. Atlanta: USDHHS; 2003; Retrieved June 9, 2010, from www.cdc.gov/dhdsp/library/maps/strokeatlas/index.htm; 2003.
4. Centers for Disease Control and Prevention. Health status of American Indians compared with other racial/ethnic minority populations. MMWR Morbidity and Mortality Weekly Report. 2003;52:1148–1152.
5. Centers for Disease Control and Prevention. Prevalence of stroke—United States, 2005. MMWR Morbidity and Mortality Weekly Report. 2007;56(19):469–474.
6. Courtney AM, Treadaway K, Remington G, et al. Multiple sclerosis. Medical Clinics of North America. 2009;93(2):451–476.
7. Criddle LM, Bonnono C, Fisher SK. Standardizing stroke assessment using the National Institutes of Health stroke scale. Journal of Emergency Medicine. 2003;29(6):541–546.
8. Dahodwala N, Siderowf A, Xie M, et al. Racial differences in the diagnosis of Parkinson’s disease. Movement Disorders. 2009;24(8):1200–1205.
9. Fjell AM, Walhovd KB, Fennema-Notestine C. One-year brain atrophy evident in healthy aging. Journal of Neuroscience. 2009;29(48):1523–1531.
10. Freedman MS, Cohen B, Dhib-Jalbut S, et al. Recognizing and treating suboptimally controlled multiple sclerosis. Current Medical Research and Opinion. 2009;25(10):2459–2470.
11. Freeman SH, Kandel R, Cruz L. Preservation of neuronal number despite age-related cortical brain atrophy in elderly subjects without Alzheimer disease. Journal of Neuropathology and Experimental Neurology. 2008;67(12):1205–1212.
12. Futagi Y, Toribe Y, Suzuki Y. Neurological assessment of early infants. Current Pediatric Reviews. 2009;5(2):65–70.
13. Gilden D. Clinical practice: Bell’s palsy. New England Journal of Medicine. 2004;351(13):1323–1331.
14. Goldstein LB, Adams R, Alberts MJ, et al. Primary prevention of ischemic stroke. Stroke; A Journal of Cerebral Circulation. 2006;37(6):1583–1633.
15. Hall GR, Gallagher M, Dougherty J. Integrating roles for successful dementia management. Nurse Practitioner. 2009;34(11):35–41.
16. Hindle JV. Ageing, neurodegeneration and Parkinson’s disease. Age and Ageing. 2010;39(2):156–161.
17. Iankova A. The Glasgow Coma Scale: clinical application in emergency departments. Emergency Nurse. 2006;14(8):30–35.
18. Leifer BP. Alzheimer’s disease: seeing the signs early. Journal of the Academy of Nurse Practitioners. 2009;21(11):588–595.
19. Lloyd-Jones D, Adams RJ, Brown T M, et al. Heart disease and stroke statistics—2010 update. for the AHA Circulation. 2010;121(7):948–954.
20. Martin EM, Lu WC, Helmick K, et al. Traumatic brain injuries sustained in Afghanistan and Iraq wars. American Journal of Nursing. 2008;108(4):40–48.
21. McElroy-Cox C. Caring for patients with epilepsy. Nurse Practitioner. 2007;32(10):34–41.
21a. McGee S. Evidence-based physical diagnosis. St. Louis: Saunders; 2007.
22. National Center for Health Statistics. Health, United States, 2009: in brief. Centers for Disease Control and Prevention 2009; Retrieved June 12, 2010, from www.cdc.gov/nchs/hus.htm; 2009.
23. Palmieri RL. Wrapping your head around cranial nerves. Nursing. 2009;39(9):24–31.
24. Sartorius D, Le Manach Y, David JS, et al. Mechanism, Glasgow Coma Scale, age, and arterial pressure (MGAP). Critical Care Medicine. 2010;38(3):831–837.
25. Sauerbeck LR. Primary stroke prevention. American Journal of Nursing. 2006;106(11):40–50.
26. Savva GM, Wharton SB, Ince PG, et al. Age, neuropathology and dementia. New England Journal of Medicine. 2009;360(22):2302–2309.
27. Schutte DL. Alzheimer disease and genetics: anticipating the questions. American Journal of Nursing. 2006;106(12):40–48.
28. Simmons S. Guillain-Barré syndrome: a nursing nightmare that usually ends well. Nursing. 2010;40(1):24–30.
29. Stephens BE, Liu J, Lester B, et al. Neurobehavioral assessment predicts motor outcome in preterm infants. Journal of Pediatrics. 2010;156(3):366–371.
30. Struble LM. Tremors: learning to stop the shakes. Nurse Practitioner. 2010;35(6):18–26.
31. Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. American Family Physician. 2007;76(7):997–1002.
32. Welsh M. Treatment challenges in Parkinson’s disease. Nurse Practitioner. 2008;33(7):32–38.
33. Zuercher M, Ummenhofer W, Baltussen A. The use of the Glasgow Coma Scale in injury assessment. Brain Injury. 2009;23(5):371–384.