3
Tumor Suppressor Genes
Nelson E. Brown and Philip W. Hinds
Introduction
Over the past 40 years, efforts to understand the underlying rules that govern the transformation of somatic cells into their malignant counterparts have led to the identification of discrete alterations in genes and gene products that, in combination, are responsible for the characteristic hallmarks of cancer.1 Broadly speaking, cancer-associated genes can be classified into three groups: oncogenes, tumor suppressor genes, and genes responsible for maintaining genome stability. Oncogenes encode the constitutively active or overexpressed versions of otherwise normal cellular proteins involved in cell growth and proliferation (i.e., tyrosine kinase receptors, transduction kinases, and small GTPases). The “gain of function” capabilities of oncogenes are acquired as a result of genetic and epigenetic mechanisms, including chromosomal translocations, gene amplifications, missense activating mutations, and demethylation of gene promoters. Regardless of the activating mechanism, an oncogene always behaves as a dominant allele (a single allele suffices) in its ability to confer malignant properties on cells.2
In contrast to oncogenes, tumor suppressor genes encode proteins that are functionally integrated into pathways that prevent unscheduled cell proliferation, stimulate cell death, or trigger the induction of permanent cell cycle arrest.2 As expected, tumor suppressor genes may act as negative regulators of oncogenes. In many cases, they are responsible for the orchestration of cell cycle checkpoints that ensure faithful cell division under normal or stress-induced conditions.3 The involvement of tumor suppressor genes in the tumorigenic process is only apparent following complete or partial loss of gene function, which commonly requires the inactivation of both parental alleles in a single cell. This recessive behavior explains the fact that the mutant alleles of these genes can be passed through the germline and cause inherited forms of cancer predisposition in humans.2,4 Inactivating mechanisms of tumor suppressor genes include deletions, nonsense, and missense mutations and methylation-mediated gene silencing.
The third class of cancer-associated genes comprises those primarily involved in cellular processes that maintain basal levels of genomic or chromosomal stability. The proficiency of a cell in accurately repairing various forms of genomic insult depends on its ability to sense acute genomic damage, usually in the form of single- or double-strand DNA breaks, and to mobilize specific repair enzymatic complexes to sites of DNA damage.5 As expected, the inactivation of gene products involved in these processes leads to an increase in the rates of spontaneous mutations. This “mutator phenotype” can, in turn, contribute to the accumulation of mutations in oncogenes and tumor suppressor genes.2 Similar to tumor suppressor genes, defects in genes involved in genomic surveillance underlie a variety of cancer-prone genetic disorders, most of them inherited in a recessive fashion. For example, nucleotide excision repair (a process responsible for the repair of single-strand breaks and crosslinks in DNA produced by UV radiation or chemical mutagens) is defective in xeroderma pigmentosum, a group of human disorders associated with the development of tumors on sun-exposed skin.6
A major contributor to genomic instability in human cancers is the inactivation of TP53, the gene encoding the p53 transcription factor.7 As mentioned later in this chapter, p53 is normally induced in response to a variety of stresses, including DNA damage. Depending on the cell type and the magnitude of the damage, p53 activation can result in cell cycle arrest, senescence, or cell death (apoptosis), processes that effectively prevent the propagation of damaged DNA within a cell population or give an individual cell time to repair the damage. Hence, cells lacking p53 may continue to replicate damaged DNA, increasing the chances of accumulating potentially oncogenic mutations in other loci.2,4,7 Notwithstanding its crucial role in sensing and responding to genotoxic insults, for historical reasons p53 is often described as a prototypical tumor suppressor gene.
Tumor Suppressor Genes: A Historical Perspective
From a historical point of view, the articulation of the modern concept of tumor suppressor gene (TSG) was possible through the convergence of three major lines of research: somatic cell hybridization experiments, the detection of loss of heterozygosity (LOH) in tumors, and the study of highly penetrant familial cancers.8,9 It is worth mentioning, however, that the existence of TSGs had already been anticipated early in the 20th century by Theodor Boveri (1862-1915), one of the founders of the chromosomal theory of inheritance (the modern concept of the gene had not been developed at the time). Boveri suggested that the uncontrolled growth characteristic of tumors arises as a result of an incorrect chromosomal dosage, which could be explained by an abnormal segregation of chromosomes during cell division. Thus, “growth inhibitory chromosomes” are removed from cells during the process of tumorigenesis. As a corollary, Boveri suggested that these inhibitory chromosomes were part of a mechanism that kept normal cells in a proliferation-arrested state unless they were stimulated to divide.10 It was not until the mid-20th century, however, that more sensitive cytogenetic techniques allowed the identification of LOH (loss of heterozygosity), indicative of chromosomal loss, in human tumors.
The next piece of evidence linking loss of function mutations and tumorigenesis came from somatic cell hybridization experiments performed in the early 1970s.11-13 The crucial observation here was that cell hybrids generated through fusion of normal somatic cells with tumor-derived cells were usually nontumorigenic. The dominant effect of normal traits over the malignant phenotype seemed to indicate that loss of growth-regulatory genetic information had contributed to the transformation of the parental tumor cell line in the first place. Conversely, the neoplastic phenotype could be reversed following the reacquisition of the normal complement of genetic information.
Ultimately, however, it was the study of familial cases of cancer predisposition that led to the identification, and subsequent cloning and characterization, of the first TSGs. Highly penetrant cancer susceptibility syndromes constitute a small group of inherited disorders in which the affected individuals develop a unique type of tumor (or a narrow set of tumors) with an unusual high incidence and at a younger age compared with sporadic (noninherited) cases.14 Although cancer-associated syndromes display a dominant mode of inheritance, the experimental evidence gathered from in vitro cell fusion experiments and LOH analyses seemed to indicate that TSGs acted in a recessive manner at the cellular level. A theoretical explanation for this paradox was first provided by Alfred Knudson and became later known as the “two-hit” hypothesis.8,15
In 1971, Knudson was studying the epidemiology of retinoblastoma, a relatively rare pediatric tumor that originates in the fetal retina. Retinoblastoma is associated with an inherited predisposition in approximately 40% of the cases. Most children with an affected parent develop multiple retinoblastomas in both eyes, which are diagnosed at a younger age compared with the sporadic forms of the disease. In contrast, children diagnosed with sporadic retinoblastoma (children with no family history of the disease, about 60% of the cases) show unilateral involvement and typically a single tumor in the affected eye. Based on these differences, Knudson postulated that the cell of origin of retinoblastoma (the retinoblast) must undergo two critical genetic events at a single locus in order to initiate a tumor. Because the first mutation or “hit” is already present in every somatic cell (including retinoblasts) of an individual with hereditary retinoblastoma, an inactivating mutation of the remaining allele (the second “hit”) would be sufficient to drive tumor formation. The increased probability of tumor initiation in the context of a large population of already mutated retinoblasts helps explain the multiplicity of tumors per retina and the characteristic early onset of hereditary retinoblastoma. In cases of sporadic retinoblastoma, on the other hand, the hypothesis postulated that both hits must take place in a single somatic cell, itself a much less probable event, thus explaining the unilateral involvement and the lower number of tumors per retina.15
Evidence for the “two-hit” model was later provided by cytogenetic analyses of blood samples from patients with inherited retinoblastoma. These studies identified germline deletions of chromosomal band 13q14 in these patients, and similar changes were subsequently found in sporadic tumors, providing strong support for the notion that the same genetic locus was affected in both variants of the disease. Although several mechanisms were initially proposed to explain the second hit, their final documentation was only possible through DNA restriction fragment length polymorphism (RFLP) analysis. RFLP-based studies demonstrated that LOH achieved through deletion, mutation, or recombination can all occur as second events in retinoblastomas.16,17 Finally, these studies provided the necessary molecular clues that led to the cloning of the retinoblastoma susceptibility gene (RB-1) in 1986.18
The protein encoded by RB-1 (pRB) is now recognized as a key suppressor of cell cycle progression.19 Evidence for pRB’s function dates back to studies on cellular immortalization mediated by viral oncoproteins, including the simian virus 40 (SV40) large T antigen. These studies demonstrated that cellular immortalization was in part a result of the direct inactivation of pRB by the SV40 large T antigen. Because immortalized cells were especially sensitive to transformation by several oncogenes, the natural conclusion was that inactivation of pRB might represent a common requirement for the initiation of most cancers. However, it soon became evident that inactivating mutations in RB-1 are found in a rather narrow group of human malignancies, most typically in small-cell lung carcinomas and osteosarcomas. As mentioned later in this chapter, we know now that deregulation of numerous cancer-associated genes can lead to the inactivation of pRB in more indirect ways, a hallmark shared by virtually all cancers.19,20
At around the same time, the status of TP53 (also known as p53) as a TSG was also established. Its gene product, the transcription factor p53, was originally identified as an interacting partner of the SV40 large T antigen. Although the mechanisms of tumorigenesis involving p53-large T antigen interaction initially suggested that TP53 acted as an oncogene, further experimental evidence challenged this notion. For example, wild-type p53 was shown to act as a suppressor of transformation in cultured cells, and genetic rearrangements at the TP53 locus, which resulted in loss of function instead of activation, were discovered in some leukemia cell lines.21 In addition, it was suggested that the interaction between p53 and the SV40 large T antigen resulted in loss of p53 function, in a manner reminiscent of pRB inactivation. Nevertheless, it was not until TP53 was mapped within a region consistently deleted in human tumors that the gene gained its final recognition as a bona fide TSG. Seminal among these studies was the discovery that TP53 was biallelically deleted in human colorectal cancers, which was soon followed by the identification of mutations in other malignancies.2 Loss-of-function mutations in TP53 were then linked to Li-Fraumeni syndrome, a known dominantly inherited condition that predisposes individuals to several cancers, most typically breast cancer.22 Over the following 40 years, an explosion of research has confirmed TP53 as one of the most frequently mutated genes in human tumors. As mentioned later, p53 is involved in the orchestration of a variety of tumor-suppressive processes, including cell cycle arrest, apoptosis, and senescence. Deregulation of each one of these processes following p53 inactivation can thus increase the probability that a cell will become malignant.4
In summary, the RB-1 and p53 paradigms defined three important properties of “classic” TSGs: (1) TSGs are recessive at the cellular level, with biallelic inactivation typically found in tumors; (2) inheritance of a single mutant allele increases tumor susceptibility because only one additional inactivating event is required for complete loss of gene function; and (3) the same gene is frequently inactivated in sporadic cancers. Theoretically, reversion of the tumorigenic phenotype following the reintroduction of the relevant TSG into a cancer cell may also serve as a functional criterion to classify a gene as tumor suppressor. However, this requirement is not always met experimentally, presumably because loss of a TSG can allow further genetic changes that may confer resistance to its restoration at a later time.4
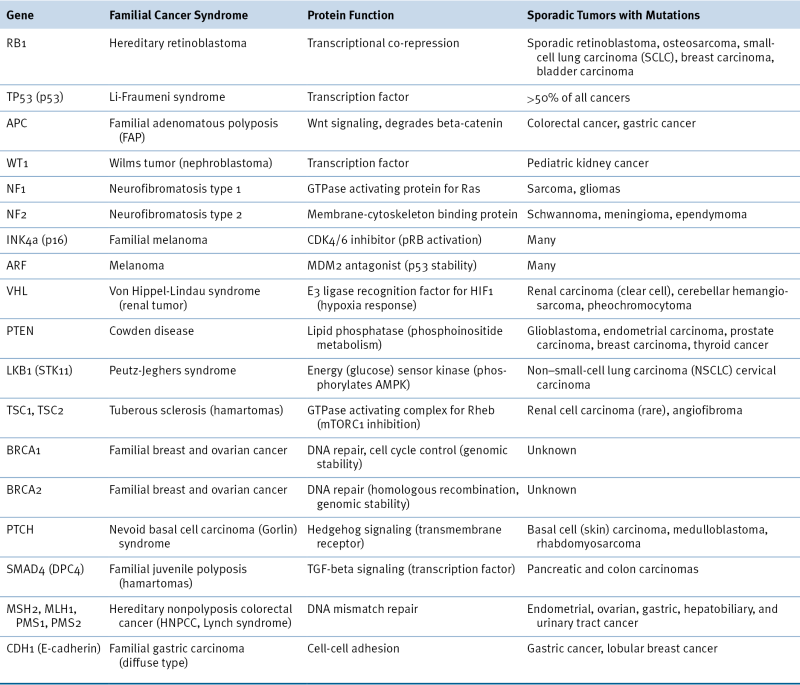
These principles served as guidance for the identification and cloning of other cancer susceptibility loci. Table 3-1 lists selected TSGs along with the function of their encoded proteins, the cancer syndrome they are associated with, and examples of sporadic cancers associated with their loss of function.
Complications of Tumor Suppression
Moderate and Low Penetrance Cancer Susceptibility Loci
Despite their importance in the discovery of TSGs, highly penetrant cancer syndromes account for a relatively small proportion of human malignancies (typically less than 0.1%). In fact, the excess in familial risk for some types of cancer has remained, to a large extent, unexplained. For example, breast cancer shows a pattern in which relative risk increases by two- to threefold in first-degree relatives of early-onset cancer cases. However, mutations in BRCA1 and BRCA2 account for only ∼20% of this overall risk increase. It has been proposed that much of the inherited risk may result from a polygenic mode of cancer predisposition. In this scenario, multiple loci, each one having a modest individual effect, may ultimately dictate the relative risk of an individual to develop cancer.9 In support for this idea, recent reports have identified susceptibility alleles associated with a wide range of risk in human populations. For example, the screening of genes associated with BRCA1- and BRCA2-dependent pathways demonstrated “moderate” breast cancer risk in individuals who are heterozygous for allelic variants of CHEK2. These rare alleles function dominantly, each conferring a moderate but detectable increase in the relative risk of developing breast cancer.23,24 More recently, genome-wide association (GWA) studies based on differences in single-nucleotide polymorphism (SNP) across human populations have begun to identify “low-penetrance” cancer susceptibility loci for the most common types of cancer.25,26
Haploinsufficiency
The two-hit hypothesis has been challenged by recent studies indicating that many chromosomal deletions in cancer cells consistently affect a single allele. Although these monoallelic deletions were initially considered to be mere “passenger events” with no actual causal role, numerous genes that behave as TSGs in vitro have been identified in these regions. This observation implies that a single-copy mutation or loss of these loci might be sufficient to explain their tumorigenic effect, a genetic property known as haploinsufficiency. For some alleles, haploinsufficiency may even confer a relative advantage to cells, most typically in situations where complete loss of function leads to apoptosis or senescence. For example, whereas a monoallelic deletion of the tumor suppressor PTEN is sufficient to produce prostate cancer in mice, loss of both parental alleles triggers a p53-dependent senescence program.8,27 Alternatively, a monoallelic mutation may confer dominant-negative capabilities on TSG products. In this modality, the mutant protein may negatively interfere with the function of the wild-type protein produced by the unaffected allele. Because dominant-negative mutations can result in considerable loss of function, there is no selective pressure in tumors to inactivate or delete the wild-type allele. A classic example of a dominant-negative effect is provided by mutant p53. As part of its function as a transcription factor, wild-type p53 binds DNA as a tetramer, a capacity impaired in mutated p53 because of missense mutations affecting the DNA binding domain. Although the wild-type and the mutant p53 proteins are still able to form hetero-oligomers in cells harboring monoallelic mutations, these complexes show impaired DNA association and transcriptional activity, resulting in loss of p53 function.22
Table 3-1
Representative Tumor Suppressor Genes
A third interpretation of the role of haploinsufficiency in tumorigenesis is based on the exquisite sensitivity of cells to even small changes in the levels of some cancer-associated proteins. Thus, a 50% functional reduction in a TSG product may be sufficient to endow a cell with a relative advantage for proliferation. Experimental evidence for this dosage-sensitivity effect has been shown for several TSGs, including TP53, BRCA1, BRCA2, and PTEN. For example, a subset of tumors arising in p53+/− mice, or in patients with Li-Fraumeni syndrome, retain the wild-type allele, suggesting that haploinsufficiency of TP53 may be sufficient for tumor initiation.28-30 Finally, the pro-tumorigenic effect imparted by haploinsufficiency might also be dependent on the loss or gain of function of other alleles. An example of this interaction is illustrated in mouse models of Pten and Tp53 deficiency. Haploinsufficiency of Pten in the context of wild-type p53 enhances proliferation and subsequent transformation of prostate epithelial cells. In contrast, complete loss of Pten in this tissue triggers a p53-dependent senescence program, with tumors arising only after Tp53 inactivation.8
Interconnecting the pRB, p53, and mTORC1 Pathways
Similar to an evolutionary process driven by natural selection, the acquisition of the malignant phenotype can be best described as an iterative process of somatic mutation followed by clonal expansion. The current consensus is that normal cells must acquire at least four distinct mutational or epigenetic events (including gain- and loss-of-function alterations) in order to bypass proliferative control. These events alter critical signaling networks that ultimately control the decision of a cell to proliferate, senesce, or die. The discovery of these pathways represented a major success in the history of cancer biology, for it made possible the assignment of a growing number of cancer-associated gene products to a much more limited number of interacting networks.2 Because of their high association with human malignancies, a more detailed description of pathways centered on pRB, p53, and mTORC1 is used in the next sections to illustrate the emergent complexities of tumor suppression. Whenever necessary, the relevant nodes interconnecting these pathways are stressed.
The pRB Tumor Suppressor Pathway
Despite the low incidence of RB-1 mutations, it has become clear that deregulation of the pRB pathway is present in most (if not all) human cancers. Deregulation can occur through gain or loss of function of various components of the pathway. In most cases, these alterations ultimately result in pRB phosphorylation, a modification necessary for G1-S cell cycle transition.31,32 In G1, hypophosphorylated (active) pRB forms repressive complexes with E2F transcription factors at gene promoters of S-phase genes, a function in part mediated by the recruitment of histone-modifying complexes to these sites. These modifications result in a silent chromatin configuration that effectively turns off S-phase genes. Signals that promote proliferation must reverse this inhibition, and they do so through pRB phosphorylation.19 In mammalian cells, pRB is phosphorylated by cyclin-dependent kinases (CDKs), a group of enzymes that require the binding of short-lived proteins called cyclins in order to become active. As shown in Figure 3-1, CDK4 and CDK6 form active complexes with D-type cyclins in early G1, whereas CDK2 is activated by E-type cyclins in late G1 and S phase. Following phosphorylation, hyperphosphorylated (inactive) pRB releases E2F transcription factors, which leads to derepression of S-phase genes (see Figure 3-1). Predictably, cyclins and CDKs act as oncoproteins in human cancers. For example, CCD1 (encoding cyclin D1) is amplified or overexpressed in more than 50% of human breast cancers.31,33
CDKs are also subject to negative regulation by two families of CDK inhibitors. Members of the INK4 family, such as p16INK4a, bind to CDK4 or CDK6 and prevent their association with D-type cyclins. On the other hand, members of the CIP1/KIP1 family, which include p21CIP1 and p27KIP1, form inhibitory complexes with CDK2 and cyclin E.31 In both cases, CDK inhibition results in pRB activation and cell cycle arrest (see Figure 3-1). As expected, many CDK inhibitors behave as tumor suppressors in human malignancies. For example, CDKN2A, the gene encoding p16INK4a, is frequently deleted or epigenetically silenced in cases of familial melanoma and in several sporadic tumors.34
The CDKN2A-containing locus is also remarkable in that it encodes a second, structurally and functionally unrelated protein from an alternative reading frame and a different gene promoter.35 This alternative reading frame protein (ARF, also called p14ARF in humans and p19Arf in mice) stabilizes p53 by directly inactivating MDM2, the E3-ubiquitin ligase that targets p53 for degradation. Therefore, loss-of-function mutations affecting ARF, as well as gain-of-function mutations in MDM2, can both have a similar destabilizing effect on p53. ARF-specific inactivating mutations have been described in a subset of human melanomas; MDM2 amplifications, on the other hand, are common in human sarcomas.2 Notice that the unique genomic arrangement of the CDKN2A locus, encoding both p16INK4a and p14ARF, means that deletions of this locus would simultaneously compromise the functions of the pRB and p53 pathways. Hence, in a manner reminiscent of the inactivation of pRB and p53 by the SV40 large T antigen, cells harboring certain CDKN2A mutations display an enhanced proliferative capacity in vitro, which in many cases is sufficient for the establishment of continuously proliferating (immortal) cell lines. This immortalization step, in turn, sensitizes cells to oncogene-mediated transformation.36
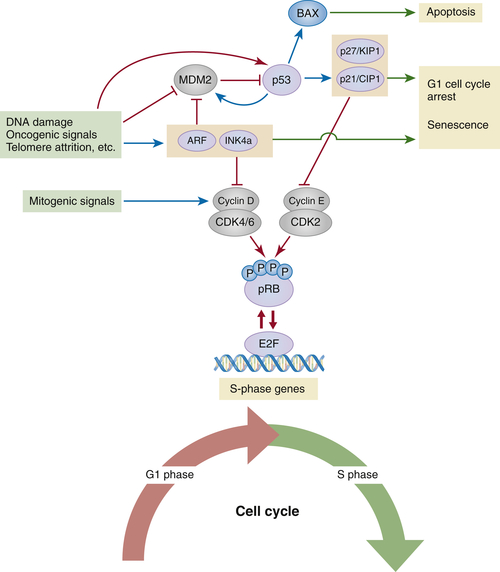
Figure 3-1 The pRB and p53 tumor suppressor pathways Under physiological conditions, signals that promote proliferation (i.e., growth factors) induce the expression of D-type cyclins, short-lived proteins required for the activation of CDK4 and CDK6 (CDK4/6) in early G1. In cooperation with cyclin E–CDK2 complexes, cyclin D1–CDK4/6 complexes contribute to the phosphorylation-mediated inactivation of pRB and the derepression of E2F-responsive (S-phase) genes. A variety of stresses, including DNA damage, telomere erosion, and oncogenic stress, turn on signaling cascades that activate the CDKN2A locus. ARF, one of the tumor suppressors produced from this locus, inhibits MDM2 (the E3-ubiquitin ligase that targets p53 for degradation), resulting in the stabilization of p53 and the induction of p53-dependent transcriptional programs (the transcriptional activity of p53 can also be affected by numerous posttranslational modifications that, for simplicity, are not depicted here). Depending on the cell type and/or the nature and magnitude of the stress, p53 can induce the expression of genes that promote apoptosis or, alternatively, genes involved in cell cycle arrest, such as the gene encoding the CDK inhibitor p21CIP1. p21CIP1, in turn, inhibits cyclin E–CDK2 complexes and leads to pRB-dependent cell cycle arrest. The second tumor suppressor encoded by the CDKN2A locus, p16INK4a (INK4a), is also induced in response to stress (with or without concomitant induction of ARF), most typically oncogenic-dependent stress. By antagonizing CDK4/6, p16INK4a also activates pRB and prevents entry into S phase. Red arrows and red T-shaped connectors indicate activating and inhibitory processes, respectively; blue arrows indicate transcriptional induction; green arrows point to final cellular outcomes.
The p53 Tumor Suppressor Pathway
As already mentioned, p53 is a multifunctional transcription factor that is activated in response to a variety of stress conditions, including DNA damage, activated oncogenes, telomere shortening, spindle damage, hypoxia, and metabolic stress.7 Depending on the cell type and the magnitude or nature of the stress, the transcriptional program activated by p53 can lead to one of three outcomes: cellular senescence, G1/G2 arrest, or apoptosis (see Figure 3-1). Mirroring the diversity of stress signals is the equally diverse number of intracellular networks involved in the transmission of these signals to p53. What all these networks have in common, however, is the ability to activate p53 via posttranslational modifications (including phosphorylation, acetylation, methylation, and sumoylation) that enhance p53’s capacity to transcribe target genes and also increase the half-life of the protein. We have seen already that one way to stabilize p53 involves the ARF-dependent inhibition of MDM2.
Among numerous p53 targets, the gene encoding p21CIP1 (CDKN1A) is probably the best-known example that connects p53 to the pRB pathway (p53-mediated upregulation of p21CIP1 leads to CDK inhibition and pRB-mediated cell cycle arrest). In addition to targets involved in cell cycle arrest, p53 also induces genes that control or promote apoptosis (such as BAX, PUMA, and PIG3), a cellular outcome favored by some cell types undergoing extensive DNA damage.37
Given the pleiotropic roles of p53 in tumor suppression, it is not surprising that mutations in TP53 are almost a universal feature of human cancers. Most of these mutations (∼74%) are missense mutations that fall within the DNA-binding domain and therefore disrupt p53’s ability to bind cognate promoter sequences on target genes.22
pRB and p53 Pathways in Action: Cellular Senescence
The connection between the two major tumor suppressors, pRB and p53, and cellular senescence is a recurrent theme throughout this chapter. Because of the growing awareness that cellular senescence constitutes a physiological barrier against tumor initiation and progression, a brief description of two related variants of senescence, and their connection with the pRB and p53 pathways, is necessary (see Figure 3-1).
Cellular senescence is a form of irreversible cell cycle arrest associated with a unique gene expression profile and distinctive cell morphology.38 The first description of this phenomenon can be traced back to efforts to propagate human cells in vitro. Explanted human cells typically proliferate for a variable period of time but eventually undergo “replicative” senescence in response to the attrition of telomeres (the protective chromosomal termini) that accompanies each cell division. Telomere disruption triggers a stress response that in many respects is identical to a p53-dependent DNA damage response (DDR).39 Before the signs of DDR are evident, however, an early induction of p16INK4a also contributes to limit the proliferative capacity of human cells, which is illustrated by the significant delay in the onset of replicative senescence observed in p16INK4a-deficient cells. Nonetheless, in order to completely bypass senescence, human cells must also overcome the p53 pathway and reactivate telomerase (the enzyme responsible for telomere maintenance).38,40
A form of replicative senescence associated with the induction of p16INK4a and p53 is also observed in primary mouse cells, but, in contrast to human cells, the inactivation of just one of these tumor suppressors suffices to bypass senescence. Because murine cells constitutively express telomerase, senescence in this case might be a response to nonphysiological culture conditions (i.e., high oxygen levels).38
In addition to replicative senescence, primary cells also undergo “premature” senescence in response to oncogenic stress (i.e., overexpression of activated HRAS), a phenomenon known as “oncogene-induced senescence” (OIS). Similar to replicative senescence, OIS is also dependent on the induction of p16INK4a and p53, although the relative contribution of these tumor suppressors varies between species and cell types.38,41 Recently, OIS has been confirmed as a barrier to tumorigenesis in vivo. For example, benign melanocytic tumors called “nevi” are associated with activating mutations in the oncoprotein BRAF. These lesions are typically positive for markers of senescence, including elevated levels of p16INK4a. As expected, loss of p16INK4a in these lesions accelerates the formation of malignant melanomas.42,43
The mTORC1-Dependent Pathways
Alterations in a cell’s ability to respond to metabolic and growth-promoting signals constitute common features of cancers. At the center of these regulatory networks is mTORC1 (mammalian target of rapamycin complex 1), a kinase complex that integrates nutrient and growth factor availability with downstream effectors involved in cell growth and proliferation. mTORC1’s main function is to promote biosynthetic processes (i.e., protein synthesis and ribosome biogenesis) that increase cell mass. Two pathways that converge on mTORC1 (the PI3K- and AMPK-dependent pathways) are particularly relevant to cancer44,45 (Figure 3-2).
Activation of tyrosine kinase receptors, most classically insulin-like growth factor receptor (IGFR), activates the lipid kinase PI3K (class I phosphatidylinositol-3-kinase), an enzymatic complex that catalyzes the production of phosphatidylinositol-3-phosphate (PIP3). The local increase in PIP3 is in turn required for the activation of AKT kinases. AKTs inhibit the GTPase activating complex TSC (tuberous sclerosis complex, composed of TSC1 and TSC2 subunits), a process required to keep Rheb (a small GTPase) in its GTP-bound (active) conformation. As a result, AKT-mediated inactivation of TSC increases the pool of active Rheb, which in turn enables mTORC1 activation (see Figure 3-2). AKT-mediated phosphorylation of substrates other than TSC can also affect proliferation by controlling pRB activity. These substrates include the FoxO (Forkhead box O) family of transcription factors and GSK3-β (glycogen synthase kinase 3-beta). Under basal conditions, FoxOs induce the expression of the CDK inhibitors p21CIP1 and p27KIP1, whereas GSK3-β participates in the degradation of cyclin D1 (see Figure 3-2). Therefore, AKT-mediated inactivation of FoxO and GSK3-β reduces the levels of CDK inhibitors and increases the levels of cyclin D1, outcomes that cooperate to promote cell cycle progression (see Figure 3-2).46
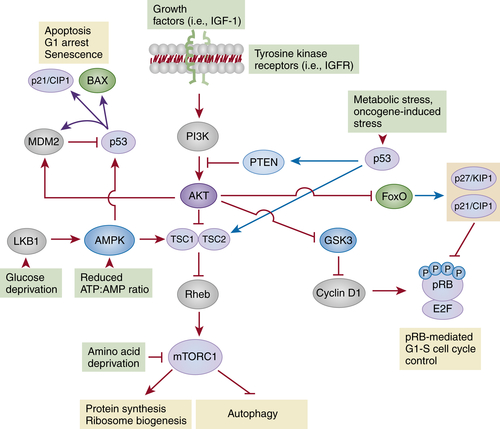
Figure 3-2 The PI3K-AKT-mTORC1 and LKB1-AMPK-mTORC1 pathways The main function of mTORC1 is to regulate biosynthetic pathways involved in cell growth, cell survival and proliferation. The proper function of mTORC1 depends on its ability to integrate inputs from two pathways: the PI3K-AKT axis, involved in the transduction of growth-promoting signals and the LKB1-AMPK axis, which monitors the energy status of the cell. Ligand-mediated activation of tyrosine kinase receptors (i.e., insulin-like growth factor receptor, IGFR) activates PI3K, which increases the local concentration of the lipid second messenger phosphatidylinositol-3-phosphate, PIP3. This activity is counteracted by PTEN, a lipid phosphatase that removes phosphate groups from PIP3. PI3K-mediated increase of PIP3 levels activates the AKT family of kinases, which inhibit the GTPase activating complex TSC (TSC1-TSC2). Inhibition of TSC allows Rheb to remain in its active (GTP-bound) conformation, resulting in mTORC1 activation. In addition, AKT-mediated phosphorylation of FoxO transcription factors and GSK3-β can also lead to pRB inactivation and cell cycle entry by reducing the expression of CDK inhibitors (p21CIP1 and p27KIP1) and increasing the stability of cyclin D1. The AMPK complex and its upstream activator LKB1 monitor the intracellular levels of glucose and ATP and modify the functional status of mTORC1 accordingly. In situations of metabolic stress, the resulting increase in the AMP:ATP ratio leads to the activation of LKB1, which phosphorylates and activates AMPK. Active AMPK can then inhibit mTORC1 through TSC-dependent and TSC-independent mechanisms. As shown here, in response to metabolic stress, p53 can directly induce the expression of TSC2 and PTEN, contributing to mTORC1 inhibition. Conversely, AMPK can also phosphorylate and activate p53. Red arrows and T-shaped connectors indicate activating and inhibitory processes, respectively; blue arrows indicate transcriptional induction.
Normal cells must also implement mechanisms to reduce the PI3K-AKT activity in order to adjust the rates of protein synthesis to the available growth factors. One important mechanism of inhibition involves the activation of PTEN (phosphatase and tensin homologue), a lipid phosphatase that catalyzes the dephosphorylation of PIP3 and thus counteracts PI3K activation (see Figure 3-2).44
In cancer cells, activation of the PI3K-AKT-mTORC1 pathway can occur through several mechanisms. These include aberrant activation of tyrosine kinase receptors (TKRs), activating mutations in PI3KCA (the gene encoding the p110α subunit of PI3K), amplification of AKT1, downregulation of TSC2, or loss-of-function mutations in PTEN.46 Loss of PTEN in particular constitutes a remarkably frequent alteration in human malignancies. Similar to other tumor suppressors, germline mutations in PTEN are also associated with inherited cancer syndromes (including Cowden disease), and hemiallelic loss of Pten in mice results in tumors arising in multiple epithelial tissues, including the intestine, prostate, and mammary gland. However, unlike other tumor suppressors, biallelic deletion of Pten can activate a p53-dependent senescence program that opposes transformation, suggesting that PTEN is an obligate haploinsufficient tumor suppressor. By comparison, mutations affecting other negative regulators of the PI3K-AKT-mTORC1 pathway are rare events in sporadic tumors, although germline deletions of TSC1 or TSC2 are known to be associated with cancer-prone syndromes.44
The second signaling pathway that modulates mTORC1 is the AMP-activated protein kinase (AMPK) pathway. During periods of nutrient deprivation, AMPK is activated by at least two mechanisms: (1) increased levels of AMP (due to a drop in ATP production) and (2) phosphorylation by LKB-1, a kinase that is itself activated in response to metabolic stress (i.e., glucose reduction) (see Figure 3-2). Active AMPK phosphorylates TSC2, leading to the activation of the TSC complex, inactivation of Rheb and mTORC1, and the consequent inhibition of protein synthesis and cell growth.44 An important consequence of mTORC1 inhibition is a shift toward a predominantly catabolic metabolism. This is in part achieved through the induction of autophagy, the process in which organelles and protein complexes are targeted to the lysosome for degradation.47
It follows from this account that cancer cells must overcome the AMPK-dependent checkpoint in order to sustain proliferation under suboptimal metabolic conditions. Among the mechanisms of AMPK inactivation, loss of function of LKB-1 is probably the best known. Inactivating mutations of the gene encoding LKB1 (STK11) have been identified in patients with Peutz-Jeghers syndrome, a condition that predisposes individuals to the development of several types of cancer. Recently, STK11 was also found mutated in sporadic cases of non–small-cell lung and cervical carcinomas.44
In recent years, it has become evident that most alterations in cancer-associated genes can result in metabolic changes that involve mTORC1-dependent pathways to variable degrees. In particular, the role of p53 in mediating adaptation to metabolic stress is becoming increasingly evident. Thus, inhibition of the AKT-mTORC1 axis, as well as activation of AMPK, can both lead to the induction of p53. The first mechanism is a consequence of the ability of AKT to activate MDM2. Therefore, a reduction in AKT function (i.e., secondary to PTEN activation) activates p53 by removing the negative regulation imposed by MDM2. On the other hand, in situations of nutrient deprivation, AMPK-mediated phosphorylation of p53 increases its half-life and transcriptional activity.48
Epigenetic Modifications and Tumor Suppression
Evidence accumulated in the past decade has led to the realization that epigenetic changes affecting oncogenes and TSGs constitute important events contributing to the hallmarks of cancer. The cancer “epigenome” is characterized by global and gene-specific heritable modifications that affect gene expression but do not involve changes in DNA sequence. Three types of cancer-associated epigenetic modifications are currently recognized: DNA methylation, histone modifications, and micro-RNA (miRNA)-mediated gene silencing.49 Although they are discussed separately in this chapter, we should emphasize that these are functionally interdependent mechanisms. For example, some miRNAs can modify the epigenetic landscape by regulating the expression of proteins involved in histone modifications or DNA methylation. Conversely, miRNA expression itself can be altered by DNA methylation or histone modifications (Figure 3-3 is a summary of the most relevant epigenetic changes observed in cancer cells).
DNA Methylation
DNA methylation is the covalent addition of a methyl group to the cytosine ring of a CpG dinucleotide. Although CpG dinucleotides are widely distributed throughout the genomes of eukaryotic organisms, CpG-rich regions (also called CpG islands) are particularly enriched in the promoter regions of genes. The silencing effect of DNA methylation can result from the direct inhibition of transcription factor binding to promoter regions or from the recruitment of repressive protein complexes to methylated regions. As explained later in this chapter, this latter mechanism often results in a more condensed, transcriptionally silent chromatin configuration.49
Genome-wide hypomethylation and promoter-specific hypermethylation are common features of cancer. These alterations can be detected in benign lesions and early-stage tumors, suggesting that they may precede classical genetic events. Global loss of DNA methylation at CpG islands was the first epigenetic alteration identified in cancers. In particular, hypomethylation at repetitive sequences in the genome is associated with genomic instability.50,51 However, the most recognized epigenetic alteration in cancer cells is the promoter hypermethylation affecting TSGs. One of the first examples of this silencing mechanism was discovered in some RB1 alleles associated with retinoblastoma.50 Since then, hypermethylation as a mechanism of gene inactivation has been demonstrated for other TSGs, including INK4a/p16 (CDKN2A), MLH1, BRCA1, VHL and CDH1 (encoding E-cadherin). In many cases, collaboration between hypermethylation and genetic inactivation can also be documented. For example, promoter hypermethylation contributes to the inactivation of the wild-type allele of CDKN2A in colorectal cancer cells that have already lost one allele through deletion. That hypermethylation is causally involved in the repression of TSGs has been confirmed through the use of demethylating procedures. For example, acute elimination or inhibition of DNMT1 (a DNA methyltransferase) in colon cancer cells is sufficient to reactivate INK4a/p16 and induce cell cycle arrest.51
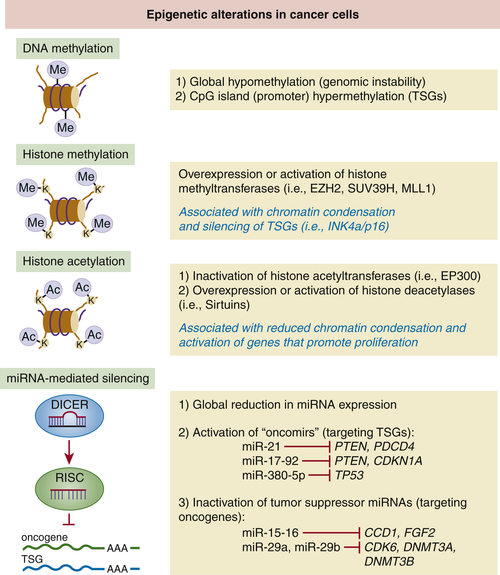
Figure 3-3 Epigenetic mechanisms involved in tumor suppression A brief summary of the main epigenetic changes affecting cancer cells.
Histone Modifications
The second group of cancer-associated epigenetic changes involves the covalent modification of histones, the proteins that form the core of nucleosomes. Among numerous modifications, acetylation and methylation of lysine (K) residues at the N termini of histones H3 and H4 are probably the best known. It has been proposed that the combinatorial addition or removal of acetyl and methyl groups to several K residues of H3 and H4 may serve as a “histone code” that dictates the degree of chromatin condensation and, therefore, the extent to which a genomic locus becomes transcriptionally active. For example, trimethylation of lysines 4, 36, or 79 and acetylation of lysines 9 or 14 of histone H3 are both associated with a relaxed chromatin configuration that facilitates transcription. Conversely, di- or trimethylation of lysine 9 or 27 of histone H3 is associated with a more condensed, transcriptionally silent chromatin configuration. It is important to keep in mind that the enzymatic complexes involved in these modifications (see later discussion) cooperate extensively with DNA methyltransferases (the enzymes that catalyze DNA methylation) to produce stable chromatin states.51
Although systematic analyses of histone modifications at the global level are still limited, some studies indicate that the disruption of normal patterns of histone acetylation can enhance tumorigenesis. For example, inactivation of two histone acetyltransferases (HATs), EP300 and CREBBP, by viral oncoproteins leads to a global reduction in acetylation of H3K18 (lysine 18 of histone H3), a modification that results in the transcriptional activation of a subset of genes that promote proliferation. Moreover, inactivating mutations of EP300 have been reported in colorectal, gastric, breast, and pancreatic tumors. Similarly, the overexpression of histone deacetylases (HDACs) and Sirtuins (a class of HDAC) is also associated with cellular transformation, as observed in a variety of malignancies51 (see Figure 3-3).
Finally, aberrant expression or activation of histone methyltransferases (HMTs) and histone demethylases (HDMs) is also associated with cancer. For example, overexpression of EZH2 (an H3K27-specific HMT) is found in prostate, breast, and lung cancers. In prostate cancer, EZH2 overexpression correlates with H3K27 trimethylation and the silencing of TSGs. Similarly, the H3K9-specific methyltransferase SUV39H has been linked to tumor initiation and progression through silencing of the CDKN2A tumor suppressor locus in several cancers.51 Perhaps the most paradigmatic and clinically relevant example of HMT activation is observed in leukemias affecting children. Translocation-mediated activation of MLL1, a gene encoding a H3K4 methyltransferase, has been reported in up to 80% of leukemias. Almost universally, translocations involving MLL1 result in fusion proteins that function as constitutively active transcription factors, leading to the deregulation of several leukemia-promoting pathways.49
In contrast to HMTs, much less is known about the role of HDMs in tumorigenesis. So far, both overexpression and inactivation of HDMs seem to contribute to tumorigenesis.51
Micro-RNAs
The discovery of noncoding RNAs has unveiled unexpected complexities in the regulation of gene expression. As described here, these new regulatory factors can play significant roles during cancer initiation and progression by way of modulating classic oncogenic pathways.
Micro-RNAs (miRNAs) are small (18 to 25 nucleotides long), evolutionarily conserved, noncoding RNAs that control the translation and stability of protein-encoding messenger RNAs (mRNAs). miRNAs are produced through the sequential processing of primary transcripts (pri-miRNAs) by the ribonucleases Drosha and Dicer1. After processing, the guide RNA strand of a mature miRNA (which is complementary to a mRNA target) combines with Argonaut proteins to form an RNA-induced silencing complex (RISC), the final effector that targets mRNAs for cleavage or translational repression.52
High-throughput genetic screens have identified more than 1000 miRNA-encoding sequences in the human genome, which are typically arranged in large clusters expressed polycistronically. Together, they are predicted to control the expression of thousands of protein-encoding genes. Given their wide spectrum of functions, it is hardly surprising that aberrant miRNA expression contributes to tumorigenesis. Remarkably, although many miRNA-encoding sequences have been mapped to genomic regions that are amplified in human cancers, miRNA expression profiles reveal a global downregulation of miRNA expression in cancer cells. Although the mechanisms responsible for this phenomenon are not completely understood, it has been proposed that some oncoproteins (i.e., MYC) can directly contribute to the global silencing of miRNAs. Alternatively, cancer initiation may require the partial repression of miRNA biogenesis. In support of this idea, human tumors often show monoallelic deletions of DICER1 and, accordingly, tumor formation is accelerated by monoallelic deletion of DROSHA or DICER1 in mouse models.52,53
Deregulation of individual miRNAs can contribute to tumorigenesis by altering the expression of conventional oncogenes and TSGs. For example, “oncogenic miRNAs” (also known as oncomirs) negatively regulate the expression of TSGs, whereas “tumor suppressor miRNAs” downregulate the expression of oncogenes. Among oncomirs, miR-21 was one of the first miRNAs found to be elevated in human cancers. In animal models, overexpression of miR-21 enhances the tumorigenic effect of K-Ras in the lung in part by targeting PTEN. Similarly, amplification of the miR-17∼92 cluster has been documented in both solid and hematopoietic cancers. Genes targeted by individual miRNAs in this cluster include the tumor suppressors PTEN, BIM, and CDKN1A.53,54
The first tumor suppressor miRNA identified was miR-15∼16, a cluster localized in a genomic region that is deleted in more than 50% of patients with B-cell chronic lymphocytic leukemia (B-CLL). Targets of this cluster include the oncogenes CCD1, FGF2, and FGFR1. Similarly, miR-29a and miR-29b, which are inactivated in mantle cell lymphoma, can target multiple cell cycle regulators and oncogenes.52
Given the relevance of the TP53 tumor suppressor in human cancers, efforts to link p53 function to miRNA regulation have already led to important discoveries. For example, p53 induces several miRNAs, including miR-34, miR-200, and miR-192. Among these, the miR-34 family represses genes that promote proliferation and survival, such as CDK6 and BCL2. Conversely, TP53 can be itself targeted by oncomirs in some cancers.53
It is worth mentioning that the extent to which an individual miRNA or miRNA cluster behaves as an oncomir or tumor suppressor is highly dependent on cellular context. Because a single miRNA can target multiple mRNAs, the differential expression of potential target mRNAs in different cell types means that the deregulation of a miRNA may lead to different outcomes depending on the cell type. For example, despite the fact that the miR-29 family acts as a tumor suppressor in many tumors, it can behave as an oncomir in breast cancer, presumably because of the particular constellation of target mRNAs in breast cancer cells.
Conclusions
During the past 40 years, the exhaustive characterization of TSG products has provided us with a relatively robust conceptual framework to understand the genetic and epigenetic bases of cancer. From the preceding sections, it should be clear that tumor suppressor proteins and cancer-associated micro-RNAs are involved in the control of almost any cellular function, and yet the disruption of their activities must somehow confer a proliferative advantage by influencing the decision of a cell to continue cycling. This feature helps explain the almost universal involvement of the pRB and p53 signaling networks in the pathogenesis of most human cancers. It is believed that a better understanding of this Achilles’ heel of cancer will lead some day to more effective therapies. As data accumulate, however, it is becoming increasingly evident that the emergent picture calls for a much-needed contextualization of TSG functions. A full understanding of the different contexts in which (or against which) a TSG functions remains a daunting task for the future. So far, significant progress has been made in the identification of signaling or metabolic pathways disrupted by the loss of function of some TSGs. By comparison, we know much less about the relationships between various genetic alterations, or the relevance of their temporal appearance, for the tumorigenic outcome. On a different level, given the rather universal functions that most TSGs have in normal cells, it is remarkable that the inactivation of many TSGs leads to specific tumor types. Although we still do not understand the basis of tissue specificity, answers to this question will be most certainly provided by a better understanding of the connection among tumor suppression, tissue development, and processes that govern the differentiation and self-renewal of normal stem cells. Finally, advances in whole-genome sequencing are already revealing the existence of low-penetrance cancer susceptibility genes, which might play an important role as modifiers of cancer risk in human populations.
References
1. Hanahan D., Weinberg R.A. Hallmarks of cancer: the next generation. Cell. 2011;144:646–674.
2. Vogelstein B., Kinzler K.W. Cancer genes and the pathways they control. Nat Med. 2004;10:789–799.
3. Kastan M.B., Bartek J. Cell-cycle checkpoints and cancer. Nature. 2004;432:316–323.
4. Sherr C.J. Principles of tumor suppression. Cell. 2004;116:235–246.
5. Hoeijmakers J.H. DNA damage, aging, and cancer. N Engl J Med. 2009;361:1475–1485.
6. Hoeijmakers J.H. Genome maintenance mechanisms for preventing cancer. Nature. 2001;411:366–374.
7. Steele R.J., Lane D.P. P53 in cancer: a paradigm for modern management of cancer. Surgeon. 2005;3:197–205.
8. Berger A.H., Knudson A.G., Pandolfi P.P. A continuum model for tumour suppression. Nature. 2011;476:163–169.
9. Fletcher O., Houlston R.S. Architecture of inherited susceptibility to common cancer. Nat Rev. 2010;10:353–361.
10. Balmain A. Cancer genetics: from Boveri and Mendel to microarrays. Nat Rev. 2001;1:77–82.
11. Harris H., Miller O.J., Klein G., Worst P., Tachibana T. Suppression of malignancy by cell fusion. Nature. 1969;223:363–368.
12. Allderdice P.W., Miller O.J., Miller D.A. et al. Chromosome analysis of two related heteroploid mouse cell lines by quinacrine fluorescence. J Cell Sci. 1973;12:263–274.
13. Klein G., Bregula U., Wiener F., Harris H. The analysis of malignancy by cell fusion. I. Hybrids between tumour cells and L cell derivatives. J Cell Sci. 1971;8:659–672.
14. Fearon E.R. Human cancer syndromes: clues to the origin and nature of cancer. Science. 1997;278:1043–1050.
15. Knudson A.G. Two genetic hits (more or less) to cancer. Nat Rev. 2001;1:157–162.
16. Cavenee W.K., Dryja T.P., Phillips R.A. et al. Expression of recessive alleles by chromosomal mechanisms in retinoblastoma. Nature. 1983;305:779–784.
17. Knudson Jr. A.G., Meadows A.T., Nichols W.W., Hill R. Chromosomal deletion and retinoblastoma. N Engl J Med. 1976;295:1120–1123.
18. Friend S.H., Bernards R., Rogelj S. et al. A human DNA segment with properties of the gene that predisposes to retinoblastoma and osteosarcoma. Nature. 1986;323:643–646.
19. Burkhart D.L., Sage J. Cellular mechanisms of tumour suppression by the retinoblastoma gene. Nat Rev. 2008;8:671–682.
20. Knudsen E.S., Knudsen K.E. Tailoring to RB: tumour suppressor status and therapeutic response. Nat Rev. 2008;8:714–724.
21. Levine A.J., Oren M. The first 30 years of p53: growing ever more complex. Nat Rev. 2009;9:749–758.
22. Goh A.M., Coffill C.R., Lane D.P. The role of mutant p53 in human cancer. J Pathol. 2011;223:116–126.
23. Meijers-Heijboer H., van den Ouweland A., Klijn J. et al. Low-penetrance susceptibility to breast cancer due to CHEK2(∗)1100delC in noncarriers of BRCA1 or BRCA2 mutations. Nat Genet. 2002;31:55–59.
24. Rahman N., Seal S., Thompson D. et al. PALB2, which encodes a BRCA2-interacting protein, is a breast cancer susceptibility gene. Nat Genet. 2007;39:165–167.
25. Anderson C.A., Pettersson F.H., Barrett J.C. et al. Evaluating the effects of imputation on the power, coverage, and cost efficiency of genome-wide SNP platforms. Am J Hum Genet. 2008;83:112–119.
26. Hao K., Schadt E.E., Storey J.D. Calibrating the performance of SNP arrays for whole-genome association studies. PLoS Genet. 2008;4:e1000109.
27. Chen Z., Trotman L.C., Shaffer D. et al. Crucial role of p53-dependent cellular senescence in suppression of Pten-deficient tumorigenesis. Nature. 2005;436:725–730.
28. Alimonti A., Carracedo A., Clohessy J.G. et al. Subtle variations in Pten dose determine cancer susceptibility. Nat Genet. 2010;42:454–458.
29. Bellacosa A., Godwin A.K., Peri S. et al. Altered gene expression in morphologically normal epithelial cells from heterozygous carriers of BRCA1 or BRCA2 mutations. Cancer Prev Res (Phila). 2010;3:48–61.
30. Venkatachalam S., Shi Y.P., Jones S.N. et al. Retention of wild-type p53 in tumors from p53 heterozygous mice: reduction of p53 dosage can promote cancer formation. EMBO J. 1998;17:4657–4667.
31. Malumbres M., Barbacid M. To cycle or not to cycle: a critical decision in cancer. Nat Rev. 2001;1:222–231.
32. Massague J. G1 cell-cycle control and cancer. Nature. 2004;432:298–306.
33. Malumbres M., Barbacid M. Cell cycle, CDKs and cancer: a changing paradigm. Nat Rev. 2009;9:153–166.
34. Ruas M., Peters G. The p16INK4a/CDKN2A tumor suppressor and its relatives. Biochim Biophys Acta. 1998;1378:F115–F177.
35. Lowe S.W., Sherr C.J. Tumor suppression by Ink4a-Arf: progress and puzzles. Curr Opin Genet Dev. 2003;13:77–83.
36. Larsson L.G. Oncogene- and tumor suppressor gene-mediated suppression of cellular senescence. Semin Cancer Biol. 2011;21(6):367–376.
37. Polager S., Ginsberg D. p53 and E2f: partners in life and death. Nat Rev. 2009;9:738–748.
38. Kuilman T., Michaloglou C., Mooi W.J., Peeper D.S. The essence of senescence. Genes Dev. 2010;24:2463–2479.
39. Feldser D.M., Greider C.W. Short telomeres limit tumor progression in vivo by inducing senescence. Cancer Cell. 2007;11:461–469.
40. Nardella C., Clohessy J.G., Alimonti A., Pandolfi P.P. Pro-senescence therapy for cancer treatment. Nat Rev. 2011;11:503–511.
41. Collado M., Serrano M. The power and the promise of oncogene-induced senescence markers. Nat Rev. 2006;6:472–476.
42. Michaloglou C., Vredeveld L.C., Mooi W.J., Peeper D.S. BRAF(E600) in benign and malignant human tumours. Oncogene. 2008;27:877–895.
43. Michaloglou C., Vredeveld L.C., Soengas M.S. et al. BRAFE600-associated senescence-like cell cycle arrest of human naevi. Nature. 2005;436:720–724.
44. Jones R.G., Thompson C.B. Tumor suppressors and cell metabolism: a recipe for cancer growth. Genes Dev. 2009;23:537–548.
45. Sabatini D.M. mTOR and cancer: insights into a complex relationship. Nat Rev. 2006;6:729–734.
46. Engelman J.A. Targeting PI3K signalling in cancer: opportunities, challenges and limitations. Nat Rev. 2009;9:550–562.
47. Cairns R.A., Harris I.S., Mak T.W. Regulation of cancer cell metabolism. Nat Rev. 2011;11:85–95.
48. Vousden K.H., Ryan K.M. p53 and metabolism. Nat Rev. 2009;9:691–700.
49. Taby R., Issa J.P. Cancer epigenetics. CA Cancer J Clin. 2010;60:376–392.
50. Feinberg A.P., Tycko B. The history of cancer epigenetics. Nat Rev. 2004;4:143–153.
51. Rodriguez-Paredes M., Esteller M. Cancer epigenetics reaches mainstream oncology. Nat Med. 2011;17:330–339.
52. Calin G.A., Croce C.M. MicroRNA signatures in human cancers. Nat Rev. 2006;6:857–866.
53. Lujambio A., Lowe S.W. The microcosmos of cancer. Nature. 2012;482:347–355.
54. Kasinski A.L., Slack F.J. Epigenetics and genetics. MicroRNAs en route to the clinic: progress in validating and targeting microRNAs for cancer therapy. Nat Rev. 2011;11:849–864.