Microbial Conjunctivitis
Scott D. Barnes, Nalin M. Kumar, Deborah Pavan-Langston, Dimitri T. Azar
Conjunctivitis
Conjunctivitis affects people of all ages and is seen in all geographic locations; it is the most common inflammation of the eye and ocular adnexa.1,2 The economic impact for prevention, diagnosis, and treatment of microbial conjunctivitis is immense.3 The various forms of conjunctivitis caused by viruses, chlamydia, bacteria, parasites, fungi, and antigens tend to share a number of signs and symptoms, but there are some clinical differences that suggest the appropriate identification and treatment. The patient's history often provides the diagnosis, which may then be confirmed through clinical examination and possibly laboratory evaluation. Different agents cause acute versus chronic conjunctivitis. Onset within 4 to 6 weeks before presentation is classified as acute disease. In this chapter we describe the anatomy and physiology of the conjunctiva and the clinical presentation and laboratory testing of microbial conjunctivitis, and we discuss viral conjunctivitis, bacterial conjunctivitis, and neonatal conjunctivitis. We end with descriptions of fungal and parasitic conjunctivitis.
Anatomy and Physiology
The inner surface of the eyelid is covered by a mucous membrane called the conjunctiva. This membrane lining the lids (palpebral conjunctiva) is reflected on itself, forming an inferior and superior cul-de-sac, or fornix, as it then covers the surface of the globe (bulbar conjunctiva) and extends to the edge of the cornea (limbus). These fornices form a physical barrier that prevents a foreign body (e.g., contact lens) from getting into the orbital space. In addition to connecting the lids to the globe, the conjunctiva produces mucus as part of the tear film. The conjunctiva and tear film provide protection of the ocular surface from pathogens accomplished via mechanical means and via the resident immune tissue.
The conjunctiva is made up of a superficial epithelial layer overlying the substantia propria. The conjunctival epithelium possesses goblet cells, unique among stratified, nonkeratinized epithelia. These goblet cells contribute to the production of mucins in the tear film. Corneal stem cells are known to exist at the limbus and peripheral cornea. A similar search for conjunctival stem cells has produced interesting results. Conjunctival cells with stemlike activity have been identified in rabbits, and subdermal injection of clonal cultures of conjunctival epithelium in nude mice has produced cysts with goblet cells and stratified epithelium, suggesting pluripotency that seems to give rise to both cell types.4,5 The connective tissue of the substantia propria is loose and highly vascularized, properties that allow for the rather dramatic clinical appearances of significant edema and injection. Abundant numbers of lymphocytes, mast cells, plasma cells, and neutrophils are found throughout the connective tissue.6 This lymphoid tissue does not form actual lymph nodes; however, its abundance, combined with the phagocytic properties of the conjunctival epithelium, demonstrates the nature of this tissue in dealing with infectious organisms.7
Clinical Presentation
History and Physical Examination
Particular attention should be paid to the time course of the condition, any inciting events, prior and current medication use, and the patient's own report of the associated symptoms. The physical examination focuses on the appearance of the periorbital skin and other mucous membranes (e.g., nasal, oral); unilaterality/bilaterality; the appearance of the conjunctiva; the associated discharge; and any specific facial, lid, and corneal involvement.
Eye Pain
In contrast to keratitis, ocular pain is not common with most forms of conjunctivitis. There is usually some degree of irritation, most commonly described as a foreign body sensation. Although uncommon in most forms of conjunctivitis, the presence of ulcerated lesions in the eyelid and conjunctiva in herpetic, smallpox, and vaccinia conjunctivitis may be quite painful. If the conjunctival process secondarily affects the cornea, eye pain may also become more prominent. Therefore, the presence of significant eye pain should prompt a more thorough search for lid/corneal involvement or intraocular inflammation.
Itching
Almost all patients with conjunctivitis complain of variable ocular burning and itching. However, severe itching tends to be a hallmark of the allergic and toxic causes of conjunctivitis. In addition to the resident lymphoid tissue, the conjunctiva has plentiful immunoglobulin E and mast cells. Degranulation of mast cells and histamine released in response to an inciting antigen are responsible for the significant itching.
Recent studies have focused on whether itching can be regarded as a top clinical sign and symptom for conjunctivitis. Using a logistic regression model, Rietveld and colleagues8 report itching as one of the three indicators that provided optimal discrimination between patients with and without a positive culture. They reported that infectious conjunctivitis history and itch both made the probability of current bacterial involvement less likely. This has now been incorporated into the practice guidelines of the Dutch College of General Practitioners (NHG).9
Visual Acuity
Visual acuity is usually normal or mildly decreased with conjunctivitis. Unless the cornea has become secondarily involved, vision is preserved. The ocular irritation and discharge may affect the ability to read an eye chart; a topical anesthetic agent and surface irrigation may improve the office examination of vision. A reduction in vision should prompt a search for an associated cause other than the conjunctivitis.
Periocular and Periorbital Skin
Some cases of conjunctivitis have associated skin changes. Skin lesions typical in poxviruses, immune-mediated diseases (Stevens-Johnson syndrome), and herpetic conditions are usually not difficult to recognize; however, a close examination may help identify causes that produce less obvious skin findings. Subtle vesicular changes on the lid margin may be the only sign of an otherwise unimpressive herpetic conjunctivitis. Numerous lesions in molluscum contagiosum provide an easy diagnosis, but small, isolated lesions may be missed if they are buried near the eyelid margin or obscured by the eyelashes. Ocular rosacea is quite common and usually bilateral. Caution must be used when diagnosing rosacea in unilateral cases because sebaceous gland carcinoma can manifest in such a fashion. Allergic conjunctivitis incited by antigens such as cosmetics, soaps, lotions, and some medications often has a typical periocular dermal manifestation.
Sweet's syndrome (acute febrile neutrophilic dermatosis) is commonly associated with conjunctivitis.8 The ocular manifestations of Sweet's syndrome include periorbital and orbital inflammation, dacryoadenitis, conjunctivitis, episcleritis, scleritis, limbal nodules, peripheral ulcerative keratitis, iritis, glaucoma, and choroiditis. The ocular inflammation appears concurrently with skin lesions. In addition, the syndrome can present itself with optic nerve involvement.10 Treatment of the ocular complications of Sweet's syndrome includes systemic administration of corticosteroid or cyclosporine.11
Conjunctival Hyperemia
The rich network of subepithelial vessels that runs throughout the conjunctiva becomes markedly dilated and congested. Against the background of the relatively avascular sclera, this hyperemia appears quite impressive. On closer examination, the hyperemia appears greater near the conjunctival periphery than in the limbal region (near the corneal border). Saccular aneurysms, petechiae, and subconjunctival or intraconjunctival hemorrhages may be present.
Discharge
Ocular secretion is almost universal in conjunctivitis. Excessive tearing results from either increased lacrimation or impaired lacrimal outflow. Increased mucin production, especially relative to the aqueous component of the tear film, is a common finding. Exudation from the conjunctival surface contains varying proportions of protein and cellular debris. A serous exudation is mainly proteinaceous; a purulent exudate is more cellular (e.g., leukocytes, fibrin). The combination of proteins, fibrin, mucin, and sloughed epithelial cells can be copious depending on the cause of the inflammation. Significant matting and “sticking together” of the eyelids and eyelashes are common.
Conjunctival Edema (Chemosis) and Conjunctivochalasis
The loosely adherent subepithelial connective tissue allows the conjunctiva a rather impressive degree of edema. Hemodynamic changes and altered vascular integrity allow transudation through fenestrated capillaries, resulting in chemosis. This edema can be so prominent that the conjunctiva appears to be “bulging” out from between the eyelids, and it may indeed cause exposure of the ocular surface if the eyelids cannot adequately close. Depending on the inciting agent, the chemosis may become hemorrhagic. Acute chemosis is often self-limited, but chronic chemosis can lead to conjunctivochalasis, or laxity of the conjunctiva, with resultant redundancy sometimes draping over the lower lid margin.
Conjunctival Papillae
The palpebral conjunctiva contains connective tissue septa that provide anchorage for the tarsus (dense connective tissue providing strength to eyelids). Conjunctival inflammation may result in dilated subepithelial blood vessels that become surrounded by an infiltrate of mixed inflammatory cells (e.g., neutrophils, lymphocytes). This edema produces elevated mounds of conjunctival epithelium, with the septa restricting diffusion beyond the fibrovascular core. The mounds, or “papillae,” have a central red dot corresponding to the dilated capillary viewed from above. A mild papillary reaction has a velvety appearance; increasing severity or chronicity may lead to enlarged, cobblestone-like papillae. Mucus and purulent material may collect within the furrows between adjacent papillae. The conjunctiva beyond the tarsus is less likely to reveal papillae because the septal connections decrease toward the fornices. With prolonged or recurrent inflammation, the septal anchors may weaken to the point at which the papillae appear reduced because of confluence. Although papillae are fairly nonspecific, they appear more commonly in cases of bacterial and allergic conjunctivitis. They are usually much less than 1 mm in diameter, but giant papillae of 1- to 3-mm diameters may be seen in association with contact lenses, ocular prostheses, or exposed corneal sutures.
Large cobblestone papillae on the superior tarsal conjunctiva and limbal conjunctiva are common with vernal conjunctivitis. The cobblestone papillae characteristically are easily visible with eversion of the upper lid. On slit-lamp examination, they are 1 to 8 mm in diameter, have a central core of blood vessels, and stain with fluorescein at their apices from erosion during active inflammation. Laced between and on top of the giant papillae is a ropy mucoid discharge that can form a pseudomembrane. The papillae in the upper lid may become so severe as to cause a mechanical ptosis from their weight. White dots (Horner's points or Trantas' dots) can occur in the corneal limbus and persist for 2 days to 1 week. Follicles are not a feature of this disease. Vernal conjunctivitis can cause a reticular subepithelial fibrosis but does not cause keratoconjunctivitis sicca and only rarely causes cicatrization of the conjunctiva.12
Conjunctival Follicles
Lymphoid tissue is normally present within the substantia propria of the conjunctiva except in neonates, in whom follicles are not visible. Conjunctival follicles are small, elevated clusters of lymphocytes. Small follicles can be observed in the noninflamed conjunctiva, especially in the lower fornix, and clusters of noninflamed follicles have been observed in children and adolescents in a condition called benign lymphoid folliculosis.13 Follicles associated with conjunctivitis are usually of recent onset, inflamed, and enlarged. Follicles used to be distinguished from papillae. Follicles have a similar elevated appearance to conjunctival papillae; however, there is no central vascular core in conjunctival follicles. The vessels surround and peripherally encroach on the raised follicle, with the central lymphocytes and other mononuclear cells often obscuring the vessels. Except in giant papillary conjunctivitis, papillae are smaller than follicles. Follicles often have a smooth, glistening surface and are most commonly seen near the tarsus, although their presence has been described on the bulbar and limbal conjunctiva.14 As with papillae, the presence of follicles is a nonspecific sign, but follicles are most commonly associated with viral, chlamydial, and toxic conjunctivitis.
Membranes and Pseudomembranes
Membrane formation results from intertwining of the conjunctiva with coalescence of an inflammatory coagulum, forming a yellowish-white membrane overlying the palpebral conjunctiva. If the fibrinous layer is intertwined with the conjunctiva via granulation tissue, it is a true membrane and will cause bleeding when removed.
Pseudomembranes have a similar appearance but are not as adherent and do not bleed when removed. Viral and bacterial causes of conjunctivitis have an increased likelihood of membrane formation, although the presence of a membrane does not rule out other causes.
Conjunctival Phlyctenules and Granulomas
A phlyctenule is a whitish, nodular collection of chronic inflammatory cells located at or near the limbus, often in the center of a hyperemic area. This represents a delayed hypersensitivity reaction generally associated with Staphylococcus species or tuberculosis. However, it can also be associated with coccidioidomycosis, candidiasis, lymphogranuloma venereum, or parasitic conjunctivitis.
Although a granulomatous nodule of chronic inflammatory cells with a fibrovascular proliferation is a classic finding in Parinaud's oculoglandular conjunctivitis, it is not common with most types of conjunctivitis. A conjunctival granuloma is more indicative of an embedded foreign body or a granulomatous disease (e.g., sarcoidosis, tuberculosis), but it may be seen with chlamydial and fungal conjunctivitis.
Corneal Involvement
Because of the close proximity of the conjunctiva to the cornea, it is not surprising to see extension of the conjunctival inflammation. Corneal involvement can be as mild as punctate epithelial erosions or as severe as frank ulceration that may lead to perforation. A number of bacterial agents that can cause conjunctivitis may penetrate an intact corneal epithelium. Foreign body sensation, pain, decreased vision, and photophobia are all signs of corneal involvement; however, many of these signs are present with the inciting conjunctivitis alone. The corneal involvement, especially with viral causes, may quickly improve with the resolution of the conjunctivitis; however, some associations can lead to undesired sequelae. Continued vigilance, a high index of suspicion, and appropriate treatment of corneal involvement are necessary.
Preauricular Adenopathy
The lymphatic vessels of the eyelids drain primarily to the preauricular lymph node. The medial third of the eyelids and the conjunctiva drain to the submandibular and submental lymph nodes. Preauricular adenopathy is also a nonspecific finding, but it is often present with viral, chlamydial, herpetic, and gonococcal causes of conjunctivitis and may be absent in toxic, allergic, and nongonococcal bacterial conjunctivitis. Submandibular and submental lymphadenopathy are uncommon but are usually present in Parinaud's oculoglandular conjunctivitis.
Laboratory Evaluation
Routine laboratory evaluation is probably not performed in most cases of conjunctivitis. Although there is agreement that all cases of suspected ophthalmia neonatorum (conjunctivitis in first month of life) should have laboratory evaluation with cultures and smears for bacterial, chlamydial, and herpetic causes, there is not universal agreement regarding which other cases require laboratory evaluation and which types of evaluation are most appropriate. Because most cases of conjunctivitis are viral, it is expected that most patients will go through a self-limited course, with spontaneous resolution after nothing but supportive therapy. The patient's history and physical examination can often predict the need for laboratory evaluation. Clear cases of viral conjunctivitis may not require conjunctival scraping for stains and cultures, but if bacterial conjunctivitis is suspected, such scrapings are recommended to guide appropriate antibiotic therapy. Indiscriminate use of antibiotics without laboratory identification of a bacterial cause may lead to the emergence of resistant organisms or may aggravate the condition as the result of a toxic or immune-mediated reaction associated with the medication.
The most common procedure involves the use of a calcium alginate swab or culturette device to collect material from the conjunctiva. Material is transferred to slides for appropriate Gram and Giemsa stains and to culture plates (e.g., blood/chocolate agar, fungal media) for further identification and sensitivity testing. Diagnosis of bacterial conjunctivitis has been recently reviewed by Golde and Gardiner.15 Smears from bacterial infections reveal numerous neutrophils along with the standard epithelial and goblet cells. Lymphocytes and monocytes are predominant in viral infections. Herpetic conjunctivitis may reveal multinucleated epithelial cells and eosinophilic, intranuclear inclusion bodies. Chlamydial conjunctivitis often reveals leukocytes, lymphocytes, and epithelial cells with basophilic, intracytoplasmic inclusion bodies; these findings are noted more frequently in children than in adults. The most common agents for bacterial conjunctivitis in children are Haemophilus influenzae and Streptococcus pneumoniae,15 whereas in adults they are Staphylococcus aureus and Haemophilus influenzae.16 Identification of inclusion bodies can be difficult, and suspected cases of herpetic and viral conjunctivitis may be diagnosed with the use of immunofluorescent techniques.
Viral Conjunctivitis
As a group, viral organisms are probably the most common cause of conjunctivitis. Viral conjunctivitis, often called “pink eye,” is one of the most frequent reasons for a visit to the emergency department or physician's office. Because the diagnosis can usually be made clinically, viral cultures and laboratory evaluations are not commonly performed.8 The viral organisms typically produce an acute, unilateral conjunctivitis with involvement of the second eye occurring often within 1 week. The watery discharge and conjunctival hyperemia can be quite impressive. Preauricular adenopathy is often noted on the involved side. Although many health care providers prescribe antibiotics in the mistaken notion that such discharge and hyperemia have a bacterial cause, most cases of viral conjunctivitis spontaneously resolve within days to weeks, usually without adverse sequelae. Numerous viruses can cause conjunctivitis, and many can be identified by slightly differing features of the disease course.
Adenoviral Conjunctivitis
Adenoviruses are responsible for two of the most common types of conjunctivitis. These infections are spread through respiratory fomites or by direct contact with conjunctival secretions. The incubation period varies from 5 to 10 days, with the clinical process lasting 5 to 15 days.17 Nineteen different serotypes of adenovirus have been reported to cause conjunctivitis.18 Once the disease course passes, immunocompetent patients are protected from a recurrent adenoviral infection caused by the same serotype.
The advent of new laboratory techniques such as the real-time polymerase chain reaction (PCR), which can identify more pathogens than routine virus isolation, have led to more accurate diagnosis of adenoviral conjunctivitis.19 Recently, a review of the available methods for identifying adenoviruses has suggested that a commercially available immunoassay kit (RPS Adeno Detector; Rapid Pathogen Screening Inc., Sarasota, FL), using antibodies to the hexon protein may be as sensitive and ideally suited for analysis in a clinical environment.2,20
Pharyngoconjunctival Fever
Pharyngoconjunctival fever (PCF) has been reported to be the most common ocular adenoviral infection.21 The most commonly implicated serotypes in PCF are 3, 4, and 7, but it has been associated with types 1, 5, 6, and 14 as well, having been isolated from conjunctiva, nasopharynx, and feces. The incubation period after exposure is 5 to 12 days (most commonly 8 days).22 The triad of pharyngitis, fever, and subsequent conjunctivitis is the classic clinical presentation. The conjunctivitis is marked by a follicular reaction accompanied by a mild watery discharge, hyperemia, and chemosis (edema of the conjunctiva). The cornea may have fine, punctate erosions, and preauricular adenopathy is present in about 90% of cases. The condition usually resolves spontaneously within 2 weeks. Supportive treatment with cold compresses and artificial tears is usually sufficient.
Epidemic Keratoconjunctivitis
Epidemic keratoconjunctivitis (EKC) is associated most often with adenovirus serotypes 8 and 19, but it has also been reported with multiple serotypes including types 2 to 4, 7 to 11, 14, 16, and 29. Serotypes other than 8 and 19 may produce a similar clinical picture to the latter but do not have the tendency to widespread epidemic.22 EKC is more severe than PCF; it lasts 7 to 21 days, with possible corneal sequelae persisting for weeks or months.23 The mixed papillary and follicular response in the conjunctiva is accompanied by a watery discharge, chemosis, significant hyperemia, and preauricular adenopathy.17,24 Subconjunctival hemorrhages and conjunctival membranes are found in approximately one third of patients with EKC, especially in the more severe cases.25 These membranes (and pseudomembranes) are made up primarily of fibrin, leukocytes, and fibroblasts. Removal of the membrane leaves a bleeding conjunctival surface; removal of pseudomembranes is not associated with such bleeding. The presence of either type of membrane can be associated with formation of conjunctival scarring and symblepharon (adhesion of conjunctival surfaces). Corneal involvement varies from the almost ubiquitous diffuse, punctate epithelial elevations to the subepithelial infiltrates, seen in 20% to 50% of cases, which may persist for months or longer but usually resolve without scarring or neovascularization.24 Treatment of EKC focuses on relieving the symptoms and minimizing the spread of this highly contagious disease. Patients are usually infectious for 10 to 14 days after onset. Cold compresses, artificial tears, and possibly decongestant eye drops constitute the main treatment. Reduced visual acuity or disabling glare from the subepithelial infiltrates often responds to topical corticosteroids.26 Removal of the membranes and pseudomembranes, along with administration of topical steroids, often has a significant effect on patient comfort. Meyer-Rüsenburg and colleagues27 have recently reviewed the prevention and treatment of epidemic keratoconjunctivitis. They recommended the application of rigorous hygenic conditions in medical facilities to reduce viral transmission.
The structural changes occurring during the course of adenovirus EKC from the onset of the disease up to 24 weeks of follow-up have been recently evaluated by confocal microscopy.28 Hyperreflective cells in the basal epithelial cell layer were found 1 week after infection. Subepithelial accumulations of dendritic cells, located mainly at the level of the Bowman layer, were also observed at 1 week. Underneath the anterior stroma, clusters of highly reflective, irregularly shaped cells were detected. At 2 weeks, follicular conjunctivitis, focal keratitis, and subepithelial infiltrates were present. Confocal microscopy revealed persistent clusters of hyperreflective basal epithelial cells intermingled with roundish cells that probably represent leukocytes. Dendritic cells had formed an intricate network and, in the anterior stroma, a hyperreflective cellular plaque that corresponded to the subepithelial infiltrate was detected. At 24 weeks after onset of the symptoms, density and dimension of dendritic cell clusters were decreased, but stromal hyperreflectivity in the midstroma was detected.28
Acute Hemorrhagic Conjunctivitis
Also known as Apollo disease, acute hemorrhagic conjunctivitis was initially described in Ghana during the time of the first lunar landing mission in 1969.29 The disease is associated with coxsackievirus A24 and enterovirus 70.30 The classic presentation is rapid onset of severe, painful papillary conjunctivitis marked by chemosis, tearing, and small subconjunctival hemorrhages. Although individual hemorrhages are noted at first, these rapidly coalesce to become confluent. The resultant hemorrhagic chemosis can reach alarming proportions. The cornea may have punctate elevations or erosions, but these rarely progress to subepithelial opacities as seen with EKC. The conjunctivitis tends to clear in 4 to 6 days, but the hemorrhages may persist. Epidemics are quite common, especially in developing countries, where up to 50% of the population may be involved. Treatment again is mainly supportive.
Recent reports have documented several outbreaks of hemorrhagic conjunctivitis with coxsackievirus A24 variant.31,32,33,34,35,36 Molecular serotyping methods have been reported to be a good alternative to the “gold standard” cell culture-neutralization method for diagnosis in view of its easy accessibility and expected sensitivity.
Herpes Simplex Conjunctivitis
Primary ocular involvement by herpes simplex virus (HSV) may manifest as an acute follicular conjunctivitis or keratoconjunctivitis with preauricular adenopathy and often with notable vesiculating periocular skin involvement. Pseudomembranes may be present in the fornices. In 1% to 5% of all HSV cases, skin lesions may be absent.2 In the absence of frank skin vesiculation, differentiation from adenoviral infection is aided by a careful search of the lid margins for signs of herpetic blistering. In contrast to primary disease, recurrent blepharoconjunctivitis is a much more localized infection. Vesicles are localized rather than diffuse, starting as red papules, which form clear vesicles, break, and scab over to heal without scarring. Virus is present for about 3 days in the lesions, although the lesions themselves take about 1 week to heal. Conjunctivitis is usually diffuse and watery. Occasionally, rose bengal or fluorescein staining reveals a conjunctival dendritic ulcer. As opposed to the host of treatment regimens used when herpetic disease affects the cornea and other ocular components, herpetic manifestations limited to the conjunctiva require minimal supportive treatment. There is no role for antiviral agents or corticosteroids; however, an antibiotic ointment such as erythromycin may be used to prevent a bacterial superinfection. Close monitoring for corneal or adnexa involvement is necessary because this complication would necessitate a change in the treatment regimen.
Research into HSV has resulted in mechanistic insights in how this virus gains entry into ocular cells and how it spreads.37 This includes the involvement of receptors such as nectin1, HVEM, heparin sulfate, and paired immunoglobulin-like 2, as well as the participation of Toll-like receptors and nuclear factor kappa B.38,39 The involvement of filopedia and endocytic pathways in the initiation and progression of the disease has also been suggested.37
Varicella and Herpes Zoster Conjunctivitis
Although the follicular conjunctivitis and preauricular adenopathy of herpes zoster virus are rarely seen, approximately 4% of patients with chickenpox have conjunctival or corneal findings, or both.40 Papules may be seen on the lids, conjunctiva, and limbus. Vesicles may be found on the semilunar fold and throughout the conjunctiva. The papules form pustules, which then ulcerate as the disease progresses. Again, there is no indication for antivirals or corticosteroids in this herpetic conjunctivitis. Supportive care, with the possibility of prophylactic antibacterial ointment, is usually sufficient. However, herpes zoster ophthalmicus may lead to substantial disability if left untreated.41,42 These complications may involve the anterior segment, optic nerve, and the retina, resulting in a number of ocular pathologies including optic neuritis, glaucoma, retinal vasculitis, and uveitis.43
Variola (Smallpox) Conjunctivitis
Between 10% and 20% of individuals affected with smallpox develop severe ocular complications.44 Additionally, about 7% of unvaccinated patients develop corneal lesions.45 About 5 days after the onset of clinical disease, an exanthematous, watery conjunctivitis may develop. It frequently clears without complication. However, in some patients, pustules then appear on the bulbar conjunctiva. These painful lesions are associated with a great inflammatory reaction and purulent discharge. The lesions often extend to the cornea, leading to inflammation, scarring, and possible perforation with loss of the eye. Specific treatment is currently not established. A promising but unproven treatment is systemic and topical cidofovir; this agent has some activity against variola in vitro and against poxviruses in animal model systems.46,47 A recently developed drug, ST-246 (tecovirimat [Arestvyr]), may prove to be useful in treating smallpox and is being stockpiled by the U.S. government for use in a bioterrorist smallpox attack (see Chapter 135). Penicillinase-resistant antimicrobial agents should be used if the skin lesions are secondarily infected or if infection is near or involves the eyes. Daily rinsing of the eyes is important in severe cases. There are no data showing that prophylaxis or treatment of variola conjunctivitis with vaccinia immune globulin (VIG) has any effect, but many experts would use it to reduce the likelihood of spread.
Vaccinia Conjunctivitis
The attention to smallpox as a bioterror hazard has also brought attention to the complications of smallpox vaccine (vaccinia). Lid and conjunctival involvement is the most common form of ocular vaccinia and is similar to that seen on the arm at the site of the intentional vaccination. Initial formation of vesicles progresses to indurated pustules, which then umbilicate to open sores. The resultant scab formation may occasionally scar and leave depigmented marks in the skin. Vaccinia conjunctivitis is characterized by an acute papillary reaction and serous or mucopurulent discharge. Multifocal ulceration of the palpebral and bulbar conjunctiva occurs commonly. Conjunctival ulcers have a whitish center with surrounding injection and edema; they may be covered by a thick, yellowish-gray membrane and may lead to symblepharon formation. Preauricular and submandibular adenopathy commonly accompanies vaccinia conjunctivitis.48,49 The differential diagnoses of vaccinia lesions of the eyelid or ocular adnexa include molluscum contagiosum, keratoacanthoma, bacterial blepharitis, and herpes simplex or varicella-zoster virus infection.50
Clinicians must maintain a high index of suspicion for ocular smallpox vaccine–associated adverse reactions in vaccine recipients and their close contacts. A 26-year-old woman developed right preseptal cellulitis and blepharoconjunctivitis after contact with a vaccinated member of the military was reported by Hu and colleagues.51 The preseptal cellulitis resolved with antibacterial therapy, and the conjunctival infection was treated successfully with a 14-day course of topical trifluridine and a single dose of intravenous VIG.51
When compared with historical data on the ocular complications of smallpox vaccination, the incidence of ocular complications during the Department of Defense Smallpox Vaccination program in the United States has been low. In addition, the severity of disease seems to be less than during other vaccination periods. Perhaps these findings are the result of improved screening of vaccinees, prevaccination counseling, postvaccination wound care, and the suggested efficacy of trifluridine in the treatment of ocular vaccinia.52
No topical antiviral agents have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of ocular vaccinia, but topical trifluridine, cidofovir, and vidarabine have been shown to be effective in animal and uncontrolled human reports. In addition, use of antiviral ophthalmic medication and vaccinia-immune globulin medication has been suggested.53 VIG has been demonstrated to be effective in treatment of lid and conjunctival lesions.54,55 A 2002 panel convened by the Centers for Disease Control and Prevention in Atlanta recommended the treatments shown in Table 114-1 for vaccinia conjunctivitis.56
TABLE 114-1
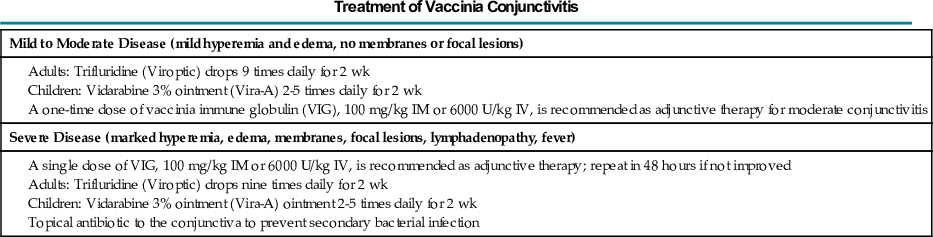
From Centers for Disease Control and Prevention. Smallpox: Summary of October 2002 Advisory Committee on Immunization Practices Smallpox Vaccination Recommendations. Atlanta: Centers for Disease Control and Prevention; 2002.
Other Viral Etiologies
Rubella, rubeola, mumps, influenza, Epstein-Barr virus, papillomavirus, molluscum contagiosum, and Newcastle disease virus have all been implicated in conjunctivitis. Rubella produces a catarrhal and/or follicular reaction along with the typical disease findings. Influenza viruses have also been associated with a catarrhal and/or follicular conjunctivitis. Rubeola (measles) produces a catarrhal and/or papillary reaction, often with significant discomfort and photophobia. Pale, avascular spots, similar in appearance to the oral Koplik spots, can be found in the conjunctiva.57 Patients with mumps may develop a catarrhal conjunctivitis and punctate epithelial keratitis with severe photophobia and lacrimation but often little discomfort.58 A follicular conjunctivitis is present in about 5% of patients with Epstein-Barr–induced mononucleosis.59 Human papillomavirus can produce lesions on the lid margin and the conjunctiva; a catarrhal conjunctivitis may follow. Molluscum contagiosum lesions on the lid margin may cause an irritating chronic follicular conjunctivitis with punctate keratitis, superior corneal vascular pannus, and cicatricial punctal occlusion. Lesions may also occur several millimeters away from the lid margins yet still cause a follicular conjunctivitis culture positive for virus.60 Lesions confined only to the cornea or conjunctiva are rare but not unknown. They are usually seen in patients with immune dysfunction.61 Newcastle disease, seen primarily in poultry workers, veterinarians, and laboratory technicians, typically produces a unilateral, follicular, and papillary conjunctivitis with hyperemia, edema, and chemosis usually in the lower fornix, mild tearing, and preauricular adenopathy.62
In all of these cases, there is no specific therapy directed toward the conjunctivitis because it is almost always self-limited. Therapy directed toward the causative agent (e.g., removal of molluscum lesions) may hasten the resolution of the conjunctivitis.
Chlamydial Conjunctivitis
Chlamydia trachomatis Infection
Chlamydial infections cause several important acute and chronic eye infections.63 Studies using monoclonal antibodies to the chlamydial major outer membrane protein have identified several serotypes of Chlamydia trachomatis. Serotypes B, Ba, and D through K, which are often sexually transmitted, can cause a follicular conjunctivitis in the adult (inclusion conjunctivitis). The same serotypes can lead to neonatal conjunctivitis if an infected mother transmits the pathogen to the newborn during vaginal delivery. Repeated infections with C. trachomatis serotypes A, B, Ba, and C can cause trachoma, a chronic follicular keratoconjunctivitis that remains the most common cause of preventable blindness in the world. C. trachomatis infection can also cause acute reactive arthritis (formerly known as Reiter's syndrome),64 a triad of urethritis, arthritis, and iridocyclitis frequently seen in sexually active young men who are positive for the HLA-B57 histocompatibility allele. In addition, several cases of Parinaud's oculoglandular syndrome have been reported with lymphogranuloma venereum, a sexually transmitted disease characterized by painful inguinal lymphadenopathy and caused by C. trachomatis serotypes L1 through L3. Although vaccines for chlamydial infections have been developed for animals, such vaccines have not yet been generated for humans. Strategies and promising avenues for development of vaccines for chlamydial infections in humans have been recently summarized.65
Chlamydia pneumoniae Infection
Chlamydia pneumoniae shares considerable homology with C. trachomatis and follows a similar life cycle.66 However, it is transmitted by aerosol droplets, can target a spectrum of cell types, and is associated with several chronic inflammatory diseases, most notably atherosclerosis.67 Although C. pneumoniae first was isolated from the conjunctiva, there are few studies on its role in ocular disorders. The organism has been detected in conjunctival swabs collected from patients with conjunctivitis,68 but a clear association with external ocular disease is lacking. Although it has been suggested that there is an association of C. pneumoniae with age-related macular degeneration (AMD),69 most evidence indicates the lack of association of Chlamydia infection with AMD.70
Trachoma
C. trachomatis serotypes A through C are responsible for trachoma. Active trachoma affects an estimated 84 million people; another 7.6 million have end-stage disease, of which about 1.3 million are blind.71 The severely blinding condition is endemic in many developing countries, especially in areas of close overcrowding and poor sanitation. Trachoma is typically the result of multiple untreated infections rather than a one-time event. The initial follicular conjunctivitis begins in the upper palpebral conjunctiva and is followed by limbal follicles. Papillary hypertrophy, mucopurulent discharge, superior corneal pannus (neovascularization), and epithelial keratitis are early features of the disease. Later stages are marked by cicatrization of the conjunctiva, cornea, and eyelids.
Trachoma stands on the brink of extinction thanks to a 1998 initiative launched by the World Health Organization (WHO)—the Global Elimination of Trachoma by 2020. This program advocated control of trachoma at the community level with four interrelated population-health initiatives that form the “SAFE” strategy: surgery for trichiasis, antibiotics for active trachoma, facial cleanliness, and environmental improvement. Evidence supports the effectiveness of this approach, and if current world efforts continue, blinding trachoma will indeed be eliminated by 2020.71,72 In this context, the success of this approach has been recently demonstrated by the elimination of trachoma in Nepal.73
The blinding complications of trachoma are the result of corneal exposure and ulceration caused by conjunctival scarring and lid deformities.74 Two classic findings are Arlt's line and Hebert's pits. Arlt's line is the horizontal line of conjunctival scarring found along the superior palpebral conjunctiva. Hebert's pits are the sharply demarcated erosions near the limbus that are filled with epithelium after the cicatrization of the limbal follicles. Once regression of the superior pannus occurs, a diffuse corneal haze may be seen. Eyelid deformities are the result of conjunctival scarring. Lids can be turned inward (entropion) or outward (ectropion), and lashes can be directed against the cornea (trichiasis), all of which contribute to an irregular ocular surface. Such irregularities can cause corneal scars, ulcers, neovascularization, and even perforation.
Most trachoma programs use the WHO simplified grading system, which was specifically designed to allow rapid assessment of prevalence and severity of disease within a population. The grading system is based on the presence or absence of five clinical signs71:
- • Trachomatous inflammation follicular (TF): five or more follicles of larger than 0.5 mm on upper tarsal conjunctiva
- • Trachomatous inflammation intense (TI): inflammatory thickening obscuring more than half the normal deep tarsal vessels
- • Trachomatous conjunctival scarring (TS): presence of easily visible scars in the tarsal conjunctiva
- • Trachomatous trichiasis (TT): at least one eyelash rubbing on the eyeball or evidence of recent removal of in-turned eyelashes
- • Corneal opacity (CO): corneal opacity blurring part of pupil margin
Although there is no gold test for C. trachomatis, it has been determined that a clustered latent class analysis (LCA) using WHO criteria and PCR may provide a useful method for diagnosis.75
Systemic tetracycline or erythromycin has been given for 3 to 4 weeks. Because the clinical response can often take several months, topical tetracycline or erythromycin is often used twice daily for 5 days each month for 6 months.18 This repeated topical treatment is especially useful in situations in which repeat infection is likely. Loosely based on the smallpox eradication efforts, widespread prophylactic systemic antibiotics have been tried in endemic areas in an attempt to eliminate the disease. A single dose of azithromycin was proposed as a good choice for the eradication theory.76 The use of azithromycin for 3 to 5 days has also been proposed for treatment in patients with bacterial or trachomatous conjunctivitis.77 With the advent of topical azithromycin, there has been support for consideration of using this eye drop as a treatment for the various ocular sequelae of trachoma.78 Evidence has been provided that face washing alone or in combination with treatment with topical tetracycline is ineffective in treatment of active trachoma.79
Consensus has built on the value of mass treatment strategies for both logistic and efficacy reasons. Important unanswered questions remain about the best distribution strategies including timing of repeat mass antibiotic treatment and duration of treatment. Theoretical models suggest that biannual treatment is necessary when the baseline prevalence is greater than 50% in children. Currently, WHO recommends mass treatment for at least 3 years if the prevalence of trachoma in children aged 1 to 9 years is greater than 10% and then reassessment of prevalence. Evidence to guide duration of treatment is scarce; however, trachoma is unlikely to be eliminated until the SAFE strategy has been implemented for at least 3 years. A survey has recently been published on the clinical management, treatment options, and challenging issues facing elimination of this disease.80
Adult Inclusion Conjunctivitis
C. trachomatis can cause a chronic follicular conjunctivitis in adults and neonates. The adult form is usually sexually transmitted, with an estimated 1 in 300 patients with genital chlamydia developing conjunctivitis,81 but it can occur with orogenital or hand-to-eye transmission of secretions.82 The most common presentation is that of a unilateral red eye (although it can be bilateral), preauricular adenopathy, papillary hypertrophy, marked hyperemia, mucopurulent discharge, and a follicular reaction. Men often have a concomitant urethritis; women may have chronic cervicitis. Corneal involvement may quickly follow the conjunctivitis, resulting in punctate keratitis, EKC-like infiltrates, and superior limbal pannus (neovascularization). Corneal scarring and neovascularization are less common with inclusion conjunctivitis than with trachoma, and the upper and lower palpebral conjunctivae are often equally involved, as opposed to the preferentially affected upper conjunctiva in trachoma. However, severe inclusion conjunctivitis may be associated with a chronic, relapsing course leading to characteristics generally seen in trachoma.
Treatment of Adult Inclusion Conjunctivitis
Because of the prominent sexual transmission of this form of conjunctivitis, it is important to simultaneously treat all known partners. Failure to do so often results in more serious sequelae associated with reinfections. Topical antibiotics are relatively ineffective, so systemic therapy is the mainstay of treatment. Tetracycline, doxycycline, or erythromycin is given for 3 weeks, with caution to avoid tetracycline in young children and in pregnant or lactating women. The use of oral azithromycin was found to be effective in the treatment of Chlamydia infection, although often more than one course of treatment was required.83
Lymphogranuloma Venereum
Certain serotypes of C. trachomatis (L1, L2, and L3) have been associated with systemic lymphogranuloma venereum. The associated conjunctivitis is often mild and unilateral, producing a scant, watery discharge. Although the conjunctivitis appears mild, there is rather impressive edema in the upper and lower eyelids. In addition to the usual preauricular lymphadenopathy, the nodes in the parotid and submaxillary region are also involved. There is a report of lymphogranuloma venereum conjunctivitis causing a keratitis leading to a corneal perforation in a patient with acquired immunodeficiency syndrome (AIDS).84 Treatment is similar to that for inclusion conjunctivitis.
Bacterial Conjunctivitis
There is significant disagreement on the actual incidence of bacterial conjunctivitis. Many cases of conjunctivitis are treated as if they were caused by bacterial organisms, but culture-proven bacterial conjunctivitis appears uncommon. The clinical presentation is characterized by a rapid onset of unilateral lid edema, conjunctival injection, and a mucopurulent discharge, followed by involvement of the second eye within 1 to 2 days. Staphylococcus and Corynebacterium species are the most common organisms to colonize the lids and conjunctiva; consequently, they are prominent causes of infectious conjunctivitis.85 Although almost any bacterial organism can cause conjunctivitis given the appropriate set of conditions, the most common ones are Staphylococcus species, S. pneumoniae, Haemophilus species, Moraxella, Corynebacterium diphtheriae, Neisseria species, and enteric gram-negative rods.86
Pathogenesis
The pathogenesis of bacterial conjunctivitis usually involves a compromised epithelial surface. Although intact epithelium is an effective barrier to most organisms, Neisseria gonorrhoeae, C. diphtheriae, Haemophilus aegyptus (Koch-Weeks bacillus), and Listeria monocytogenes can penetrate such a surface through specialized attachments or toxins, or both.87 Injured epithelium or specialized attachments allow adhesion, which may result in the entry of various bacterial products and toxins. Enzymatic components such as proteases, coagulases, collagenases, and fibrinolysins, combined with toxins such as those seen in Staphylococcus and Pseudomonas species, can disrupt underlying tissue, allowing further bacterial entry and possible isolation from host defense mechanisms.88 Bacterial conjunctivitis can be clinically categorized as acute, hyperacute, or chronic on the basis of various features.
Acute (Mucopurulent) Bacterial Conjunctivitis
S. aureus, S. pneumoniae, and H. influenzae are the organisms that most commonly cause bacterial conjunctivitis. The acute conjunctivitis is marked by unilateral hyperemia, tearing, mucopurulent discharge, and matting of the eyelids. S. aureus is the most common agent in adults and children; S. pneumoniae and H. influenzae occur more frequently in children than in adults.89 H. influenzae is often associated with systemic infections, such as upper respiratory tract disease, and its treatment usually requires the administration of systemic antibiotics. Viridans streptococci and Streptococcus pyogenes can produce an acute conjunctivitis, often with an associated membranous reaction. Gram-negative rods, other than Haemophilus species, rarely cause acute conjunctivitis in the immunocompetent patient.
Treatment of Acute Bacterial Conjunctivitis
Appropriate laboratory confirmation of bacterial conjunctivitis should be attained to guide treatment. Although many mild conjunctival infections resolve on their own, topical antibiotic treatment may speed resolution and reduce severity and morbidity.90 Treatment with a broad-spectrum agent such as sulfacetamide, trimethoprim-polymyxin, or a fluoroquinolone is necessary for 7 to 10 days. Recently, topical moxifloxacin has gained FDA approval to treat bacterial conjunctivitis in those as young as 3 years of age and topical azithromycin has been shown to be effective in treating bacterial conjunctivitis with a 3-day course.91 Appropriate agents may be selected or altered on the basis of laboratory results.
In one study it was reported that the upper eyelid may have tarsoconjunctival crypts, and these may be a reservoir for the organisms. It was recommended that marsupialization of the crypts be performed because it obliterates the potential space and was found to be curative.92
Hyperacute (Purulent) Bacterial Conjunctivitis
The most frequent cause of hyperacute conjunctivitis is N. gonorrhoeae; a less severe form can be seen with Neisseria meningitidis.93 This severe disease is most common in neonates, sexually active adolescents, and young adults. The most impressive characteristic is the copious, thick, yellowish-green, purulent discharge. Marked chemosis, painful hyperemia, and eyelid edema are seen. In contrast to most cases of bacterial conjunctivitis, there is often tender preauricular adenopathy. There may be conjunctival membrane formation, and the condition may rapidly progress to corneal ulceration and perforation because Neisseria species can penetrate an intact corneal epithelium in as little as 24 hours.
Treatment of Hyperacute Bacterial Conjunctivitis
Laboratory evaluation via Gram stain and culture is important because the treatment of Neisseria conjunctivitis is different than that of most bacterial entities. Topical antibiotics can augment treatment, but systemic therapy is the mainstay with Neisseria infections. The prevalence of penicillin-resistant organisms has made ceftriaxone the treatment of choice. Gonoccocal conjunctivitis without corneal involvement may be treated with one intramuscular injection of ceftriaxone. Corneal involvement usually requires hospitalization for a 3-day course of intravenous treatment. Topical antibiotic ointments and solutions have been considered, but the most important topical therapy is frequent (every 30 to 60 minutes) saline irrigation of the conjunctival surface and fornices to remove the inflammatory cells, proteolytic enzymes, and debris, which may be toxic to the ocular surfaces. Because up to one third of patients with gonococcal conjunctivitis have been reported to have chlamydia, concurrent treatment with tetracycline, doxycycline, or azithromycin may be indicated. A 1.5% azithromycin solution was found to be well tolerated and effective in patients with purulent bacterial conjunctivitis.77
Chronic Bacterial Conjunctivitis
The most common causes of chronic bacterial conjunctivitis are the Staphylococcus species.94 Such infections can be difficult to eradicate because the eyelid margins and surrounding skin are heavily populated with staphylococci. Associated exotoxins are thought to be responsible for the effect on the conjunctiva, lids, and cornea. A diffuse hyperemia, minimal mucopurulent discharge, and conjunctival thickening with either a follicular or papillary reaction are common. Eyelid involvement may manifest as redness, telangiectasia, loss of lashes, thickening, or recurrent hordeola (“stye”), and ulceration at the base of the eyelashes may be seen. Maceration and ulceration of the inner and outer canthal angles may be seen in chronic blepharoconjunctivitis caused by Moraxella species. Chronic staphylococcal blepharoconjunctivitis may lead to marginal corneal ulceration, most likely as the result of an immune-mediated hypersensitivity reaction. Gram-negative bacteria are more common in chronic than acute conjunctivitis.95 Organisms more often associated with the intestinal flora can be associated with chronic conjunctivitis: Proteus mirabilis is the most common of these, but Klebsiella pneumoniae, Escherichia coli, and Serratia marcescens have also been described.
Treatment of Chronic Bacterial Conjunctivitis
Treatment of this type of bacterial conjunctivitis demands appropriate antibiotic therapy combined with aggressive lid hygiene and possible evaluation of the lacrimal system. Laboratory evaluation may guide appropriate antibiotic treatment, often with erythromycin or bacitracin ointment. Lid hygiene involves the use of warm compresses, eyelid scrubs with nontearing shampoo, and gentle lid massage because the meibomian (sebaceous gland) orifices at the base of the eyelashes may harbor the inciting agents. The lacrimal canaliculus or sac may also serve as a bacterial reservoir requiring antibiotic irrigation and oral antibiotics. The staphylococcal hypersensitivity reaction in the cornea may require mild topical corticosteroid treatment to reduce the associated inflammation. Oral tetracycline or doxycycline may be beneficial in more severe infections.
Neonatal Conjunctivitis
Any conjunctivitis occurring within the first 4 weeks of life is classified as neonatal conjunctivitis (ophthalmia neonatorum).96 Conjunctivitis in the newborn can be bacterial, viral, chlamydial, or toxic (reaction to chemicals). Specific identification of the cause is particularly important because there is often a potentially serious systemic infection associated with the localized ocular condition. Neonatal conjunctivitis is more commonly found if babies are delivered vaginally compared with cesarean, and this may be a risk factor for this disease.97
Neonatal Chemical Conjunctivitis
In 1881 Credé introduced the use of topical silver nitrate as prophylaxis against neonatal gonococcal infection.98 The self-limited conjunctivitis, present in approximately 90% of treated newborns, usually begins a few hours after delivery and resolves in 24 to 36 hours.99 Although quite effective against N. gonorrhoeae, silver nitrate has little effect on bacteria and essentially no effect on chlamydia or viruses.100 Silver nitrate may injure epithelial cells to such a degree that they are more susceptible to the entry of other microbial agents. Silver nitrate may still be used in some countries, but hospitals in the United States have changed to erythromycin or tetracycline ointment. Betadine is markedly inexpensive and quite effective against many microbial agents; it is becoming more widely used as a prophylactic agent for newborns, especially in developing countries. The associated chemical conjunctivitis is similar in nature and course as that seen with silver nitrate.
Liquid detergent capsules have also been associated with ocular conjunctivitis in children in a U.K. study.101
Neonatal Chlamydial Conjunctivitis
The most frequent cause of neonatal conjunctivitis in the United States is C. trachomatis.102 Up to 3 million new cases of chlamydial infection occur annually,103 with 4% to 10% of all pregnant women in the United States being diagnosed with chlamydia.104 The infant of an untreated mother has a 30% to 40% chance of developing conjunctivitis and a 10% to 20% chance of developing pneumonia.98 A unilateral or bilateral discharge begins 5 to 14 days after delivery. PCR has been demonstrated to be more sensitive than other conventional methods in detecting neonatal chlamydial conjunctivitis and may be useful for the routine screening and treatment of genital C. trachomatis infection in pregnant women.105,106,107
Chlamydial conjunctivitis in the neonate differs from that in the adult in a number of ways. No follicular response is seen in the neonate because of the immature immune system's inability to form such a reaction. The amount of mucopurulent discharge is greater in the neonate, as is the propensity to form membranes on the palpebral conjunctiva. The infection in neonates is more responsive to topical medications. Although the typical conjunctivitis is mild and self-limited, severe cases can result in conjunctival scarring with corneal pannus and scarring. If erythromycin or tetracycline ointment is applied to the conjunctival surface within 1 hour after delivery, the chance of developing chlamydial conjunctivitis is reportedly almost zero.108 However, topical medications cannot treat the pneumonitis and otitis media that may accompany the conjunctivitis. Two weeks of oral erythromycin therapy is given to the newborn with laboratory-proven chlamydia conjunctivitis; a second course may be given if adequate resolution is not achieved with the initial treatment. The mother and her sexual partners must also be treated with oral erythromycin or tetracycline (with caution in breast-feeding mothers) for 1 week.
Neonatal Gonococcal Conjunctivitis
The incidence of neonatal gonococcal conjunctivitis has dropped dramatically with effective prenatal screening and use of prophylactic antimicrobial agents in newborns. The clinical presentation begins with a hyperacute bilateral conjunctival discharge that appears within the first 24 to 48 hours after delivery. The associated purulent exudate is often so profuse that it reappears immediately after cleaning of the eye. Conjunctival membrane formation is not uncommon. N. gonorrhoeae can penetrate an intact epithelial surface and quickly invade the cornea, causing ulceration, perforation, and even endophthalmitis if not promptly treated. Other localized gonococcal infections such as rhinitis and proctitis may be present, as well as the rare but more severe disseminated infection with arthritis, meningitis, pneumonia, and septicemia, which could lead to infant death.103 With resistance emerging against penicillin, tetracycline, and even the fluoroquinolones, a single dose of intramuscular or intravenous ceftriaxone, 25 to 50 mg/kg, not to exceed 125 mg, is the preferred treatment.109 Hospitalization and hourly saline irrigation of the conjunctival fornices are recommended; if corneal involvement cannot be ruled out because of the copious exudation, topical antibiotics are applied.110 Povidone-iodine prophylaxis treatment has also been suggested, but its effectiveness compared with tetracycline ointment has been questioned.111,112,113,114 Fusidic acid may prove to be a promising treatment.114
Nongonococcal Neonatal Bacterial Conjunctivitis
Numerous organisms can cause bacterial conjunctivitis in the newborn. The majority of infections are associated with gram-positive organisms such as the Staphylococcus and Streptococcus species. Gram-negative organisms such as the Haemophilus and Enterobacter spp., E. coli, P. mirabilis, K. pneumoniae, and S. marcescens have been less commonly implicated.115 Although Pseudomonas aeruginosa is a rare cause of neonatal conjunctivitis, it deserves special consideration because of its ability to rapidly cause corneal ulceration and possible perforation.116
Although symptoms can manifest at any time within the first month of life, nongonococcal bacterial conjunctivitis usually manifests 2 to 5 days after delivery. The clinical presentation consists of periorbital edema, chemosis, and conjunctival hyperemia and discharge. There is a higher incidence if obstruction of the nasolacrimal system is present. Conjunctival scraping for Gram stain and cultures allows for appropriate treatment—usually erythromycin ointment for gram-positive organisms and either gentamicin or tobramycin ointment for gram-negative organisms.
Neonatal Viral (Herpetic) Conjunctivitis
Herpetic conjunctivitis in the neonate is rare but can be associated with significant morbidity and mortality. HSV types 1 and 2 can be associated with conjunctivitis. In theory, HSV-1 can be transmitted to the infant through oral secretions from an adult or sibling with an active “cold sore,” but the more common source is contact with HSV-2 during passage through an infected birth canal. The edema, conjunctival injection, and tearing usually begin within the first 2 weeks of life and may be followed by keratitis or keratouveitis. Diagnosis is commonly made by Giemsa stain but can be confirmed in 24 to 48 hours by PCR.
If HSV is detected in neonatal conjunctivitis, the baby should be evaluated for extent of HSV infection and intravenous acyclovir should be started immediately per American Academy of Pediatrics guidelines.117
Parinaud's Oculoglandular Conjunctivitis
This condition refers to the association of follicular conjunctivitis and unilateral preauricular lymphadenopathy. This classification describes a type of conjunctivitis that has numerous associated causes including bacterial, viral, parasitic, mycobacterial, syphilitic, leukemic, and fungal agents. The red eye, mucopurulent discharge, and foreign body sensation are accompanied by one or more granulomatous nodules on the palpebral conjunctiva. There is usually a visibly enlarged preauricular or submandibular lymph node on the involved side. This follicular conjunctivitis is associated with a fever and possible skin rash. Bartonella henselae, or cat-scratch disease, is the most common cause, but tularemia, tuberculosis, syphilis, lymphoma, mumps, Epstein-Barr virus, sporotrichosis, and sarcoidosis have all been implicated as potential causes.
Cat-scratch disease often resolves spontaneously, but 1 month of topical and systemic antibiotic therapy has been described. Because of the host of etiologic agents, an extensive workup may be warranted, with the identified cause given the appropriate systemic treatment (see Chapter 236).
Parasitic Conjunctivitis
Leishmaniasis and Microsporidia
A number of parasites may be associated with conjunctivitis, either by primary infection or secondarily as a response to the presence of the parasite. Blepharoconjunctivitis caused by Leishmania may begin as simple edema and hyperemia, with eventual progression to superficial phlyctenules in the conjunctiva and at the corneal limbus.118 These phlyctenules may progress to abscess formation, scarring of the lids and conjunctiva, and even corneal perforation. These parasites are obligate intracellular agents that are transmitted through bites of infected sand flies. Previously uncommon protozoa are now being recovered from the conjunctivae of patients with acquired immunodeficiency syndrome.
Other Parasites and Ectoparasites
The tsetse fly can infect humans with the flagellates responsible for African trypanosomiasis or “sleeping sickness.” Ocular effects manifest as unilateral conjunctivitis, periorbital edema, and preauricular lymphadenopathy.119 Cryptosporidia, fly larvae, and nematodes (e.g., Loa loa) have also been implicated as parasitic causes of conjunctivitis.120,121-124 The lid margin and lashes may be colonized by Phthirus pubis (lice) or Demodex (mites), with conjunctivitis occurring as a reaction to the organism or its waste products. Treatment for the actual conjunctivitis associated with the parasitic agents is mainly supportive; more aggressive treatment may be necessary for the systemic parasitic condition.
Fungal Conjunctivitis
Although various fungal agents can be recovered from the conjunctiva, fungal conjunctivitis is rarely observed clinically. In comparison with fungal keratitis, relatively few organisms have been implicated in fungal conjunctivitis. Candida spp., Blastomyces spp., and Sporothrix schenckii have been associated with a granulomatous conjunctivitis. These mycoses are treated with systemic antifungal agents. Conjunctival Rhinosporidium seeberi infection usually manifests as a fleshy, friable, red, pedunculated mass.1 Excision of the mass with adequate margins is often curative.
Microsporidia are ubiquitous obligate intracellular fungi that are found more often in animal hosts, but the related microsporidium, Encephalitozoon, has been implicated as the cause of a mild conjunctivitis with punctate epithelial keratitis in immunocompromised patients.119 Symptoms may be mild and can easily be mistaken for tear film deficiencies or blepharitis; a high index of suspicion is required to make a clinical diagnosis of microsporidial conjunctivitis. Oral albendazole, 400 mg twice daily, has been reported to be effective (see Chapter 283). Topical fumagillin can be obtained as Fumadil B and formulated for human use but is not approved by the FDA; fumagillin has been used to successfully treat microsporidial keratoconjunctivitis (see Chapter 283).120 In general, medical treatment involves long duration with frequent recurrences after discontinuation of medication.
Noninfectious Vision-Threatening Conditions Associated with “Red Eye”
Care must be taken with any patient who presents with a “red eye” because there are numerous conditions that can simulate conjunctivitis. As with most conditions, a thorough medical history and physical examination are often helpful in the differential diagnosis. Most cases of conjunctivitis are associated with fairly painless discharge and irritation, essentially normal vision, normally reactive pupil, normal intraocular pressure, essentially clear cornea, and generally diffuse conjunctival injection. Three possible sight-threatening conditions—corneal ulcer, uveitis, and angle-closure glaucoma—often have different signs, which may enable a more proper diagnosis.
An attack of angle-closure glaucoma is associated with significant pain, often nausea, usually no discharge, generally markedly decreased vision, mid-dilated nonreactive pupil, markedly elevated intraocular pressure, a cloudy and edematous cornea, and a more localized conjunctival injection in the limbal region.
Uveitis is generally associated with mild to moderate pain with photophobia, essentially normal to mildly reduced vision, no discharge, a small to normal-sized reactive pupil, normal to low intraocular pressure (elevated in herpetic uveitis and Posner-Schlossman syndrome), a generally clear cornea, and a localized conjunctival injection around the limbus.
Corneal ulcers are quite painful and are usually accompanied by moderate to markedly reduced vision, variable mucoid or mucopurulent discharge, normally reactive pupil, normal intraocular pressure, an opaque lesion that is easily visible in the cornea, and usually a generalized conjunctival injection.