Atrial Fibrillation
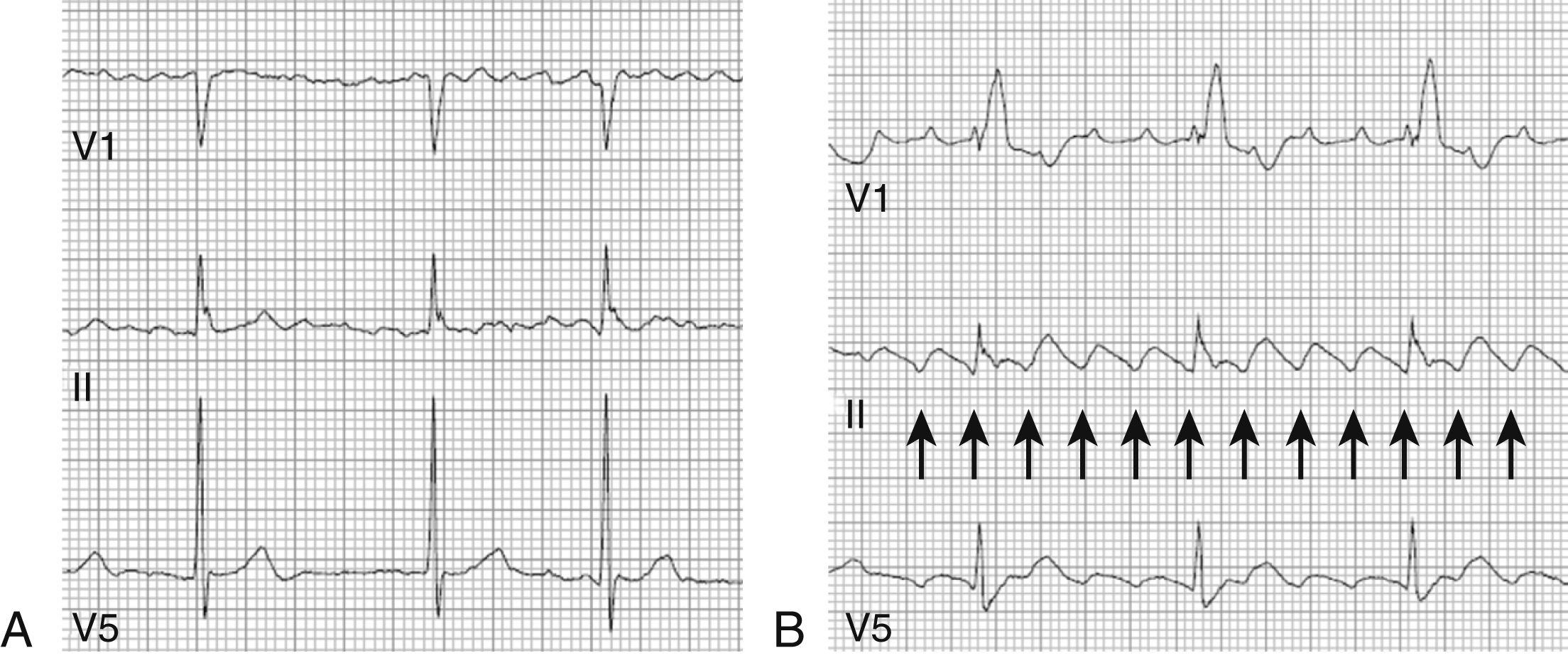
1. What is the difference between atrial fibrillation and atrial flutter?
2. How common is atrial fibrillation?
3. What are the primary goals of atrial fibrillation management?
4. What is the current classification of atrial fibrillation?
5. What are the most common etiologic factors contributing to atrial fibrillation?
6. What is the CHA2DS2-VASc score, and how is it used?
7. What can be used to assess a patient’s bleeding risk on anticoagulation?
8. What are the different medication alternatives to warfarin?
Table 35.2
The CHA2DS2-VASc Scoring System
| CHA2DS2-VASc | Event Rate at 1 Year |
| 0 | 0.78 |
| 1 | 2.01 |
| 2 | 3.71 |
| 3 | 5.92 |
| 4 | 9.27 |
| 5 | 15.26 |
| 6 | 19.74 |
| 7 | 21.50 |
| 8 | 22.38 |
| 9 | 23.64 |
Table 35.3
Anticoagulation Recommendation for Atrial Fibrillation Based on Patients’ CHA2DS2-VASc Score
| CHA2DS2-VASc SCORE | Recommendation |
| ≥2 | Oral anticoagulants are recommended |
| 1 | Either anticoagulation, no therapy, aspirin |
| 0 | No antithrombotic therapy |
Modified from January, C. T., Wann, L. S., Alpert, J. S., Calkins, H., Cleveland, J. C. Jr., Cigarroa, J. E., et al. (2014). 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Journal of the American College of Cardiology, 64(21), e1–e76.
Table 35.4
Modified from Pisters, R., Lane, D. A., Nieuwlaat, R., de Vos, C. B., Crijns, H. J., & Lip, G. Y. (2010). A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest, 138, 1093–1100.
Table 35.5
| Score | Bleeding Risk (%) |
| 0 | 1 |
| 1 | 2 |
| 2 | 3 |
| 3 | 4 |
| 4 | 9 |
| >5 | 13 |
Modified from Pisters, R., Lane, D. A., Nieuwlaat, R., de Vos, C. B., Crijns, H. J., & Lip, G. Y. (2010). A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest, 138, 1093–1100.

9. What are the alternatives to anticoagulation for the prevention of stroke and systemic embolism with atrial fibrillation?
10. What options exist for rate control of atrial fibrillation?
11. What is the optimal target heart rate for rate control in atrial fibrillation?
12. What are the reasons to pursue maintenance of sinus rhythm in patients with atrial fibrillation?
13. Are anticoagulation recommendations different for patients with paroxysmal versus persistent atrial fibrillation?
14. When is anticoagulation indicated around the time of cardioversion?
15. What can be done if cardioversion for atrial fibrillation is unsuccessful?
16. What are some common side effects with amiodarone?
17. Why do some patients taking propafenone have a pronounced beta-blocking effect?
18. What are some risk factors for torsades de pointes associated with antiarrhythmic drug therapy?
19. What is the target of atrial fibrillation catheter ablation?
20. What are the indications for atrial fibrillation catheter ablation?
21. When is it appropriate to stop anticoagulation after atrial fibrillation catheter ablation?
22. What are some complications of atrial fibrillation catheter ablation?
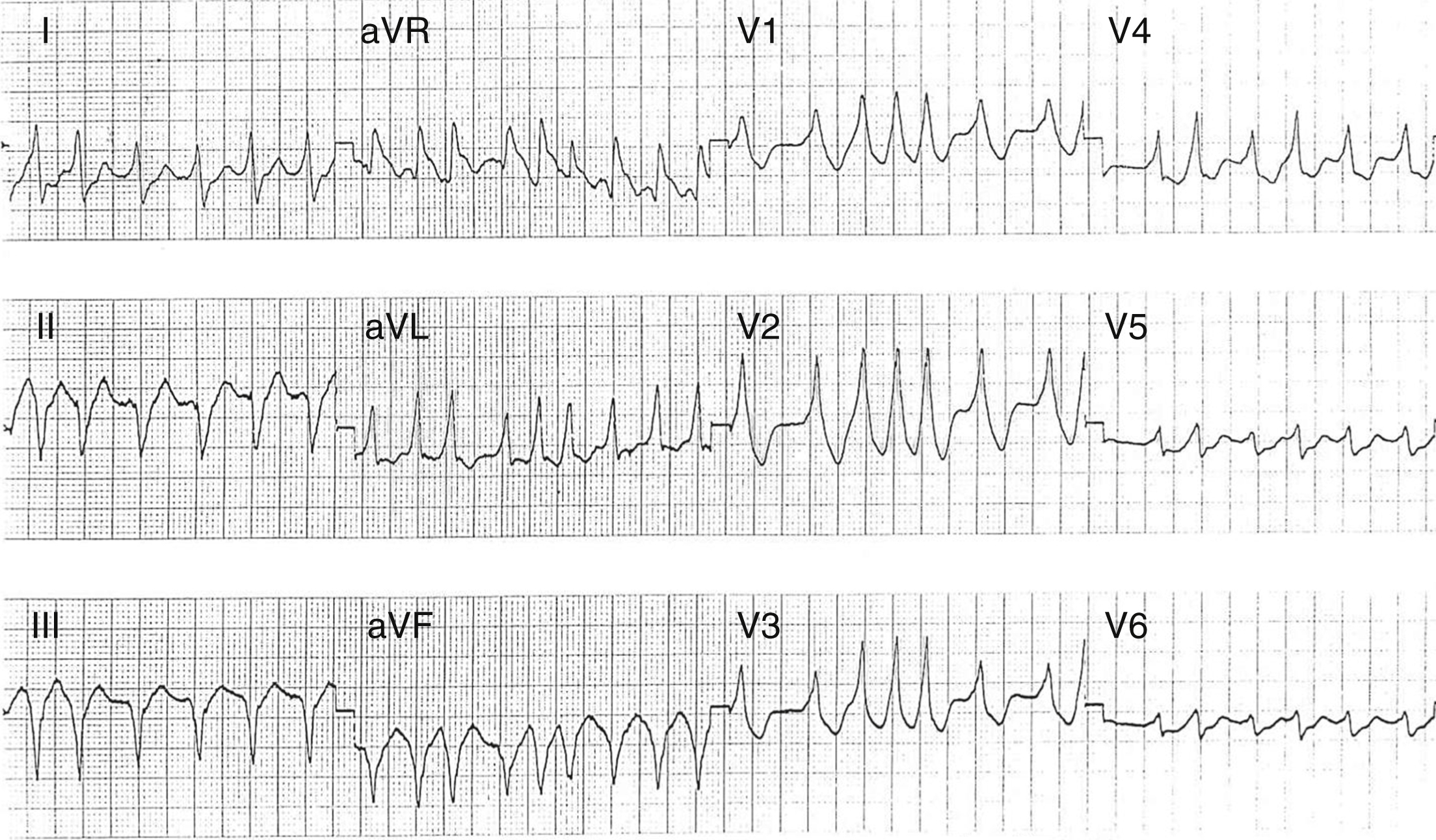
23. What is “pre-excited” atrial fibrillation?