CHAPTER 31 Biomechanics of the Shoulder During Sports
Before studying prevention and treatment of shoulder injuries, it is vital to understand the anatomy of the shoulder complex and shoulder biomechanics during various athletic motions. Shoulder biomechanics are particularly important for chronic and overuse injuries, because the cumulative effect of repetitive motions and forces may be paramount in the pathology. The vast majority of overuse shoulder injuries treated in sports medicine result from overhead throwing or striking. An especially large portion of the patient population comes from baseball pitchers.
In this chapter, the biomechanics of overhand throwing and striking will be explained. The rapid, forceful biomechanics of baseball pitching are described first and serve as a basis for the general understanding of all overhand throws. Specific characteristics of other types of overhand throws are then described, followed by the biomechanics of various striking and swinging motions in sports. The overall biomechanics of these activities are quantified and described, but shoulder biomechanics are emphasized. For the sake of brevity, approximate values for the kinematic and kinetic parameters are often included in this text without standard deviation or ranges.
BASEBALL PITCHING
Normal Biomechanics
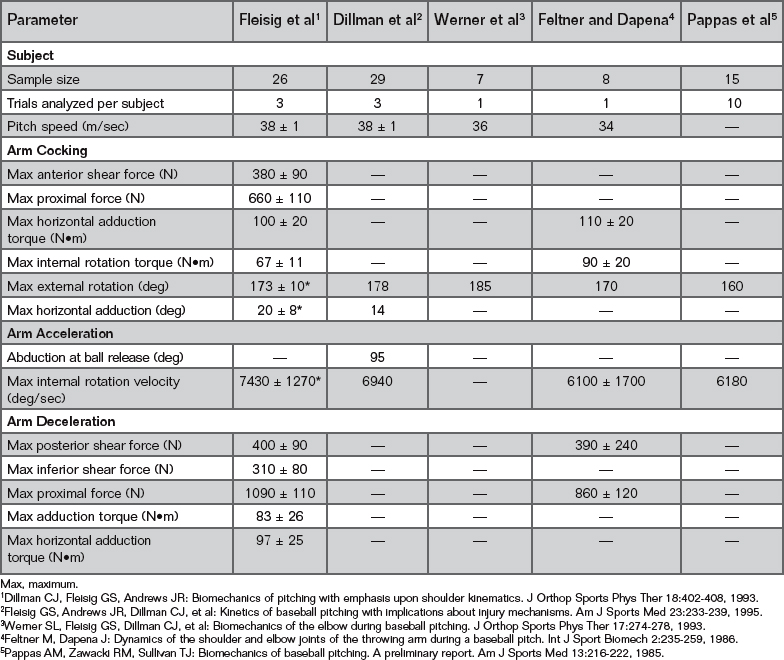
Of all sports motions, the greatest shoulder angular velocity and greatest incidence of shoulder injuries occur during baseball pitching. Even though a baseball pitch is a continuous motion, it can be divided into different phases to help understand the mechanics involved.1-4 A summary of shoulder kinematics (motions) and shoulder kinetics (forces and torques) during these phases is presented in Table 31-1 and in the text. A pitch is broken into six phases:
Wind-up
The purpose of the wind-up phase is to put the athlete in a good starting position to pitch. The wind-up begins as the pitcher plants the back foot against the rubber in preparation for raising the lead leg (Fig. 31-1A). The lead leg is lifted by concentric contractions of the hip flexors (rectus femoris, iliopsoas, sartorius, pectineus).5 When the knee has reached its maximum height, the pitcher should be in a balanced position with the lead side (left side for right-handed pitcher) facing toward home plate and the left knee and both hands anterior to the chest (see Fig. 31-1B). The stance leg bends, slightly controlled by eccentric contractions from the quadriceps muscle, and remains in a fairly fixed position due to isometric contractions of the quadriceps until a balanced position is achieved.5 The hip abductors (gluteus medius, gluteus minimis, and tensor fascia latae) of the stance leg must also contract isometrically to prevent a downward tilting of the opposite side pelvis, and the hip extensors of the stance leg contract both eccentrically and isometrically to control and stabilize hip flexion.5
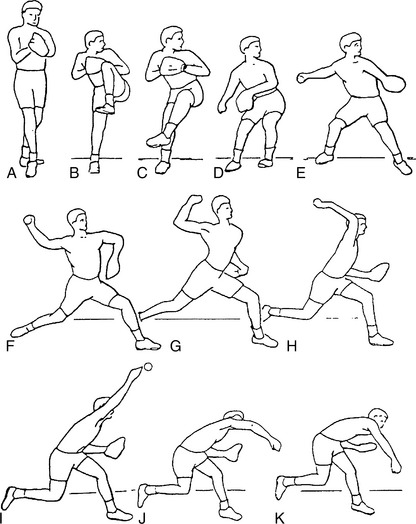
Figure 31-1 The six phases of pitching. A to C, Wind-up. C to F, Stride. F to H, Arm cocking. H to I, Arm acceleration. I to J, Arm deceleration. J to K, Follow-through.
(From Dillman CJ, Fleisig GS, Andrews JR: Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther 18:402, 1993. Reprinted with permission of the Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association.)
The shoulders are partially flexed and abducted, and they are held in this position by the anterior and medial deltoids, supraspinatus, and the clavicular portion of the pectoralis major.6,7 In addition, elbow flexion is maintained by isometric contraction8 of the elbow flexors (biceps brachii, brachialis, and brachioradialis).7,8
Wind-up ends with the pitcher in a good balanced position. Except for the potential energy from lifting the lead leg, very little energy is generated in the wind-up phase. Electromyographic (EMG) studies have shown that upper extremity muscle activity during this phase is minimal.6-12
Stride
The stride phase begins at the end of the wind-up, when the lead leg begins to fall and move toward the target and the hands separate. The stride ends when the lead foot first contacts the ground (see Fig. 31-1C to F). Eccentric contraction of the hip flexors controls the lowering of the lead leg, and concentric contraction from the hip abductors of the stance leg help lengthen the stride.5 In pitching, the forward movement is probably initiated to some degree by hip abduction, followed by knee and hip extension from the stance leg. As the lead leg falls downward and forward, the lead hip begins to externally rotate, while the stance hip begins to internally rotate.3 The stance hip also extends due to concentric contractions from the hip extensors.13 Throughout the stride phase the trunk is tilted slightly sideways, away from the target.
These motions cause the upper and lower body to stretch out, creating elastic energy to be used to drive the upper body forward. The stride of the body from the high leg position toward the plate also creates kinetic energy. The lead foot lands almost directly in front of the stance foot or a few centimeters closer. The stride length from the rubber to the lead foot should be slightly less than the pitcher’s height. At foot contact, the pitching arm abducts 91 ± 11 degrees, externally rotates 58 ± 25 degrees, and horizontally abducts 22 ± 10 degrees behind the trunk.
Arm Cocking
The arm cocking phase begins at foot contact and ends at maximum shoulder external rotation. During the stride and arm cocking phases, the pelvis rotates open to face home plate. Shortly after the pelvis begins to rotate, the torso begins transverse rotation about the spinal column. As the trunk rotates toward the target, the forearm and hand segments lag behind the rapidly rotating trunk and shoulder, producing a maximum external rotation (MER) of 165 to 180 degrees.2,4,5,14-16 The pitching shoulder horizontally adducts, moving from a position of horizontal abduction at foot contact to a position of 15 to 20 degrees of horizontal adduction at MER.2 A maximum shoulder horizontal adduction velocity of 581 deg/sec is reached during this period.5 The shoulder remains abducted 80 to 100 degrees throughout the arm cocking phase.5
Great amounts of shoulder forces and torques are generated throughout arm cocking (Figs. 31-2 and 31-3). As the pelvis and upper torso rapidly rotate, a centrifugal force is created to distract the shoulder. To balance these actions, a peak force of 550 to 770 N is generated at the shoulder mainly by the rotator cuff muscles.14,15 Furthermore, the internal rotator muscles are eccentrically loaded and elastically stretched to decelerate shoulder external rotation. An 80-N•m shoulder internal rotation torque is generated just before MER. A maximum shoulder anterior shear force of 380 ± 90 N and a shoulder horizontal adduction torque of 100 ± 20 N•m are produced to resist posterior translation of the arm and keep the arm moving forward with the trunk.14,15 High forces and torques are also generated at the elbow joint throughout the arm cocking phase (see Table 31-1).4,14,15
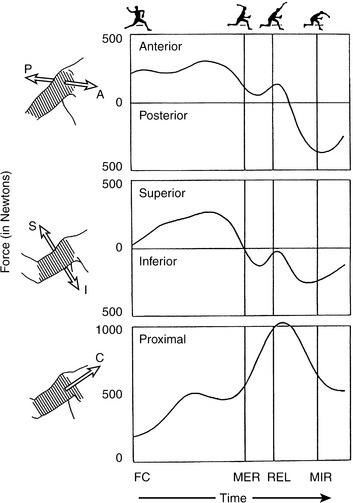
Figure 31-2 Forces generated at the shoulder in pitching: anterior to posterior (top), superior to inferior (middle), and proximal to distal (bottom). FC, front foot contact; MER, maximum external rotation; MIR, maximum internal rotation; REL, ball release.
(From Fleisig GS, Dillman CJ, Escamilla RF, Andrews JR: Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 23:233, 1995. Reprinted with permission.)
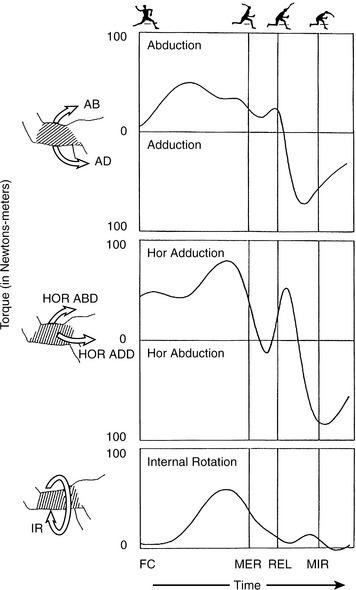
Figure 31-3 Torques experienced by the shoulder in pitching: abduction (AB) and adduction (AD) (top), horizontal adduction (HOR ADD) and horizontal abduction (HOR ABD) (middle), and internal rotation (IR) (bottom). FC, front foot contact; MER, maximum external rotation; MIR, maximum internal rotation; REL, ball release.
(From Fleisig GS, Dillman CJ, Escamilla RF, Andrews JR: Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 23:233, 1995. Reprinted with permission.)
Arm Acceleration
The arm acceleration phase begins at MER and ends at ball release. As the arm reaches the point of MER, the elbow begins to extend. Elbow extension is followed immediately by the onset of shoulder internal rotation. There is a short delay between the onset of elbow extension and shoulder internal rotation. This crucial delay allows the thrower to reduce the arm’s rotational resistance about its longitudinal axis, thereby allowing greater internal rotation velocity to be generated. The shoulder internal rotators contract concentrically to help produce a peak maximal internal rotation velocity of 6000 to 8000 deg/sec near ball release.2,14,16,17 The pitching shoulder is abducted approximately 80 to 100 degrees throughout the arm acceleration phase.2
Biomechanical analysis suggests that approximately 90 degrees of abduction is the strongest angle for the shoulder during a throw, as well as the angle with minimum chance of impingement or other shoulder injury.2,18 A peak shoulder horizontal adduction of 18 ± 6 degrees is reached at the time of MER, positioning the elbow slightly in front of the trunk. As the shoulder internally rotates, the hand moves forward and the elbow moves backward. Shoulder horizontal adduction at ball release is reduced to 9 ± 7 degrees.
Arm Deceleration
The arm deceleration phase begins at ball release and ends at maximum shoulder internal rotation (MIR) (see Fig. 31-1I to J). At the end of arm deceleration, the shoulder rotation is approximately neutral (0 degrees of internal rotation).5 Large eccentric loads are needed at both the shoulder and elbow joints to decelerate the arm. Interestingly, some studies showed minimal external rotation torque generated about the shoulder after ball release.14,15 The reason is that after ball release the arm is extended at the elbow, abducted at the shoulder, and directed toward home plate. In this position, the rotator cuff and related musculature decelerate the arm primarily by resisting distraction. A maximum proximal force of approximately body weight (1000-1200 N) is generated at the shoulder during arm deceleration.14,15 The posterior muscles of the shoulder have been identified as having a paramount role in resisting shoulder distraction force and anterior subluxation force.2,6,9 A maximum shoulder posterior force of 400 ± 90 N and a maximum shoulder horizontal abduction torque of 97 ± 25 N•m are applied to the arm in order to decelerate shoulder horizontal adduction and resist anterior humeral head translation, respectively.15 Moreover, a maximum shoulder inferior force of 310 ± 80 N and a maximum shoulder adduction torque of 83 ± 26 N•m are produced to resist shoulder abduction and superior humeral head translation, respectively.15
Follow-Through
A good follow-through is critical in minimizing the risk of injury. Most overuse injuries to the posterior side of the arm or trunk occur during arm deceleration and follow-through. This is because all of the energy generated in the body to accelerate the ball forward must be dissipated after ball release. The key to a good follow-through is to let the larger body parts help dissipate the energy in the pitching arm. The trunk should flex forward and the upper trunk should continue to rotate (see Fig. 31-1K). As in the arm deceleration phase, the posterior shoulder muscles continue to be eccentrically active throughout the follow-through, thus continuing to decelerate the horizontally adducting shoulder. Shoulder joint forces and torques generated during the follow-through are generally lower than those generated during the arm deceleration phase.5
Biomechanical Comparison Among Various Levels of Development
Although pitching biomechanics of adult pitchers have been extensively studied, information on younger pitchers and the difference between adult and younger pitchers is limited. Cosgarea and colleagues19 compared pitching kinematics among levels of competition (9-12 years, 13-16 years, collegiate, and professional). They showed that a younger pitcher generated significantly less shoulder internal rotation velocity. Fleisig and colleagues17 also compared youth, high school, college, and professional baseball pitchers, measuring both the kinematics and kinetics. They found that no position and temporal shoulder parameters showed significant differences among the four competition levels, whereas all the velocity and kinetic shoulder parameters displayed significant differences (Table 31-2). In an earlier study where pitching kinetics were compared between 10 youth and 10 professional pitchers,20 the researchers found that the adult pitcher produced greater shoulder anterior force and shoulder internal rotation torque during the arm cocking phase. The adult pitcher also generated greater shoulder posterior force during the follow-through.
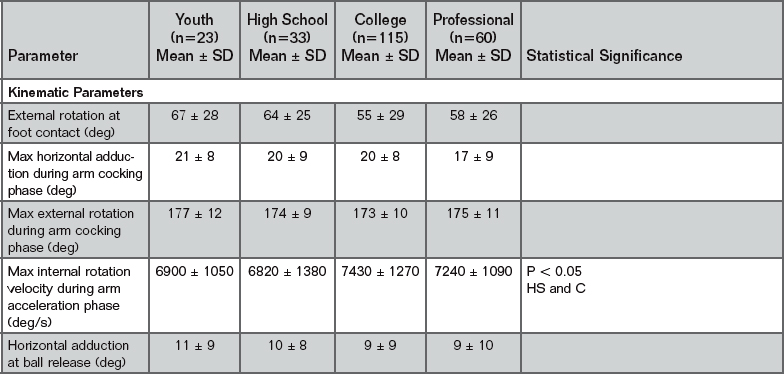
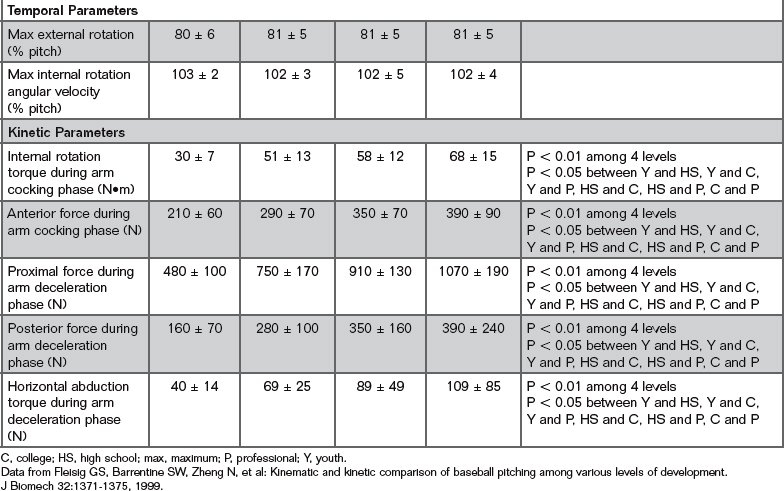
The kinematic data from these studies suggest that pitching mechanics did not change significantly with level. They also supported the common coaching philosophy that a child should be taught proper pitching mechanics that could be used throughout a career. The increases of shoulder joint forces and torques with competition levels were most likely due to greater muscle strength at higher levels. The greater shoulder angular velocities produced by higher-level pitchers were most likely due to the greater joint forces and torques generated during the arm cocking and arm acceleration phases (see Table 31-2).
In another study by the American Sports Medicine Institute (ASMI), Dun’s group21 compared the baseball pitching kinematics between a group of younger professional pitchers (mean age, 19.7 years) and a group of older professional pitchers (mean age, 29.5 years). They showed that the older group produced less shoulder external rotation during the arm cocking phase. However, this difference was not associated with ball velocity. Their results implied that both biologic changes and technique adaptations occur during the career of a professional baseball pitcher.
Biomechanical Comparison Among Pitch Types
Fleisig and colleagues conducted two studies to compare the biomechanics of four common pitch types—fastball, change-up, curveball, and slider—in collegiate pitchers.22,23 Compared with fastball kinematics, the kinematics of the slider were similar, whereas the change-up and curveball demonstrated decreased range of motion and decreased joint velocities.22 Shoulder internal rotation torque, horizontal adduction torque, abduction torque, and proximal force were significantly less in the change-up than in the other three pitch types.23 Shoulder horizontal adduction torque was greater in the fastball than in the curveball and slider. Shoulder proximal force was greater in the slider than in the curveball (Table 31-3). Both studies showed that the curveball and change-up displayed kinematic differences from the fastball (Table 31-4). Therefore, there were significant (but few) kinematic differences between the fastball and curveball. The change-up had lower joint kinetics, lower angular velocities, and different body positions than the other three pitch types.
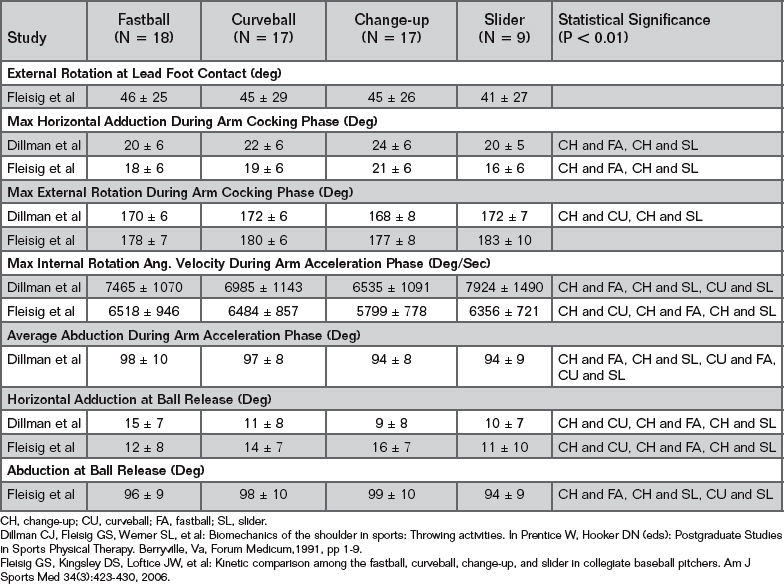
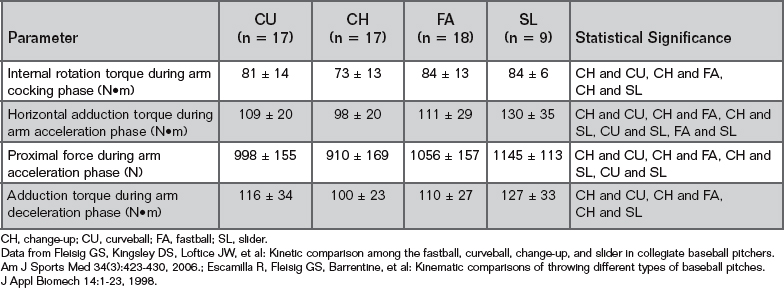
The low kinetics in the change-up suggests that it is the safest pitch for college-level pitchers. Because the resultant joint loads were similar among the fastball, curveball, and slider, this study did not imply that any of these pitches was most dangerous for the collegiate pitcher. Future studies comparing pitches at different levels, especially younger levels, are needed.
Flat Ground Throwing
Flat ground throwing is used in training and rehabilitation for baseball pitchers. The Interval Throwing Program was developed to assist in the rehabilitation of baseball athletes. In the Interval Throwing Program, a pitcher is instructed to throw from flat ground with a crow-hop and with normal pitching mechanics. The pitcher throws to a prescribed distance anywhere from 45 to 180 feet away. The idea is that throwing from flat ground is less harmful to the shoulder than throwing from the mound. By gradually increasing applied loads to the shoulder, the pitcher can return to full strength without putting the shoulder at risk too soon.24
To determine differences between pitching from a mound and throwing from flat ground, Fleisig and colleagues25 tested 27 college pitchers. Each subject threw in different conditions that included pitching with full effort from a standard mound and three flat ground throws: 180-foot crow-hop throw, 120-foot crow-hop throw, and 60-foot crow-hop throw. Reflective markers were placed on anatomic landmarks, and their motion was analyzed using an automatic digitizing system.
The analysis revealed that there were some significant differences between flat ground throwing and pitching from a mound. Stride length was 71% ± 4% of the body height when throwing from the mound and about 66% of the body height when throwing from flat ground. With the shorter stride, a pitcher achieves less external rotation at foot contact when throwing from flat ground (about 28 degrees) than when pitching from the mound (42 ± 26 degrees). However, maximum external rotation was approximately 170 degrees for all of the throws. There was no significant difference in shoulder internal rotation torque, shoulder anterior force, or shoulder internal rotation velocity produced to accelerate the ball between pitching from the mound and throwing from flat ground.25
One key variable that might be related to overuse injuries in pitchers is shoulder proximal force. Shoulder proximal force was 910 ± 110 N when pitching from the mound and approximately 850 N when throwing from flat ground for the three throwing-distance conditions.25 Less force required to resist distraction in flat ground throws may be related to the low injury rate during throwing for nonpitchers.
Pathomechanics
With improper mechanics, force in shoulder muscles may be unusually large. It has been demonstrated that muscle activity of the infraspinatus, teres minor, supraspinatus, and biceps was two to three times higher in amateur pitchers than in professional pitchers.12 These findings imply that professional pitchers better coordinate the movements of their body segments to increase pitching efficiency.
During the wind-up phase of a pitching motion, the tendency of many pitchers, especially young pitchers, is to rush their motion by moving their lead leg toward home plate as it is lifted. By rushing, a pitcher does not have the proper coordination between the arms and lower body, which can limit the amount of energy passed from the legs to the arm. A pitcher who rushes can therefore place too great a demand on the pitching arm and increase the chance of shoulder injury.
Because of the large magnitudes and rapid changes of the forces experienced by the shoulder during baseball pitching, maintaining a stable shoulder joint may be difficult. Forces in the shoulder during pitching that shift the humeral head to the rim of the glenoid fossa, coupled with glenohumeral distraction, cause the humeral head to be reseated off-center and place the labrum in jeopardy for injury.26 Specifically, translation and subluxation of the humeral head in the anterior or posterior direction can cause forceful entrapment of the labrum between the humeral head and the glenoid rim, resulting in labral tearing.27 Capsular laxity, as well as muscle weakness or fatigue, makes maintaining shoulder stability even more difficult, further increasing the chance of injury.
Rotator Cuff Injuries
Most rotator cuff tears in throwers are located from the mid supraspinatus posterior to the mid infraspinatus area.28 These tears are presumably caused by tensile failure, as the rotator cuff muscles tried to resist distraction, horizontal adduction, and internal rotation at the shoulder during arm deceleration. Proximal force and horizontal adduction torque are produced and the posterior shoulder muscles are very active during the arm deceleration phase10; this supports the belief that the posterior shoulder muscles are susceptible to injury during arm deceleration.
Baseball pitchers at the professional level,29-32 college level,33,34 and youth level35 have all been found to demonstrate significantly greater shoulder external rotation in the dominant arm. Similar results have been found in position players, too.30 In maximum external rotation at the end of the arm cocking phase, the posterior rotator cuff can become impinged between the glenoid labrum and the humeral head.36 This over-rotation injury can lead to degeneration of the superior labrum and the rotator cuff.36
Shoulder-Grinding Factor
The shoulder-grinding factor proposed by McLeod and Andrews states that if the humeral head translates anteriorly or posteriorly, rapid internal rotation and proximal force can cause the humerus to grind on the labrum.26 The shoulder-grinding factor can increase the degeneration of the labrum resulting from humeral translation.
Subacromial Impingement
Subacromial impingement is another shoulder injury associated with baseball pitching.28 It can cause inflammation of the supraspinatus, infraspinatus, or bicipital tendon, and it can cause abrasion wears. During the arm deceleration phase, 310 N of inferior force is required to keep the humerus in a balanced position (Fig. 31-2). The inability to generate this amount of force could result in superior translation of the humerus. Because the arm is abducted, horizontally adducted, and internally rotated, the superior translation of the humerus can cause impingement of the greater tuberosity, rotator cuff muscles, or biceps against the inferior surface of the acromion or coracoacromial ligament.
SLAP Lesions
A SLAP lesion is a tear to the superior labrum, anterior and posterior.37 Andrews and colleagues reported a tear to the anterosuperior labrum in a series of 73 baseball pitchers and other throwing athletes.38 The injury was believed to result from repetitive overuse throwing, because a traumatic episode was not present for most of these patients. It was proposed that the injuries were caused by forces imparted by the long head of the biceps brachii, particularly during arm deceleration, which peel the labrum away from the glenoid.37,38
The primary function of the biceps brachii is to supply elbow flexion torque. Eccentric flexion torque, found during the arm acceleration and the arm deceleration phases, reaches a maximum value of 61 N•m right before ball release. Because the long head of the biceps brachii originates on the anterosuperior aspect of the glenoid labrum, contraction of the muscle produces tension on the biceps tendon–labrum complex. Another important function of the biceps brachii is to resist humeral distraction. Contraction of the biceps is particularly efficient in applying a proximal force to the arm at the instant of maximum proximal force, because reduced external rotation at this time allows the long head of the biceps to be closely aligned with the proximal direction. Total force generated by the biceps is a combination of its contribution to elbow flexion torque and shoulder proximal force.
With proper pitching mechanics, maximum elbow flexion torque occurs before maximum shoulder proximal force. With improper timing between these two loads or other mechanical faults, greater total force by the biceps may be required. Laxity in the shoulder joint can also result in increased shoulder proximal force needed, further increasing the demand on the biceps tendon–labrum complex. This is supported by the findings that the EMG activity level in the biceps is larger in shoulders with chronic anterior instability.11 Bey and colleagues39 showed that a SLAP lesion could be reliably produced with traction on the long head of the biceps tendon with the shoulder inferiorly subluxated. This study supports the belief that SLAP lesions can occur at or shortly after the instant of ball release.
Morgan and colleagues40 and Burkhart and Morgan41 proposed a peel-back mechanism. During the arm cocking phase of pitching, the abduction and external rotation of the pitching arm cause the biceps tendon to assume a more vertical and posterior angle. The dynamic angle change produces a twist at the base of the biceps, transmitting a torsional force to the posterosuperior labrum. This torsion force causes the posterosuperior labrum and biceps anchor to rotate medially over the corner of the glenoid onto the scapular neck, which can eventually result in a SLAP lesion.
To determine if SLAP lesions are more likely to occur with the in-line mechanism (McLeod and Andrews theory) or the peel-back mechanism (Morgan and Burkhart theory), it would be helpful to compare the force on the biceps tendon during pitching with the force the biceps can handle without tearing. Near the time of ball release, the long head of the biceps tendon is aligned approximately in the distal direction of the glenoid as the arm is abducted about 90 degrees and internally rotates from a cocked-back position to a neutral position. At this time, the biceps contributes to the roughly 1000-N shoulder proximal force shown in Table 31-1. The force contribution of the biceps has not been quantified. When the arm is cocked back into external rotation, force in the biceps contributes toward the 380-N anterior shear force and 67-N•m internal rotation torque shown in Table 31-1. Again, the force contribution of the biceps has not been quantified.
A cadaver study,42 found that the biceps anchor demonstrated significantly greater ultimate strength with in-line loading (group A, 508 N) as opposed to peel-back posterior loading (group B, 262 N). All group B specimens failed at the biceps anchor, resulting in a type II SLAP lesion. If biceps tendon forces during pitching could be calculated, then these strengths during cadaveric testing could be compared. It is likely that SLAP lesions actually occur from a combination of the proposed in-line and peel-back mechanisms.
A weed-pull theory has been proposed as the cause of SLAP lesions in the overhead athlete.43 This theory states that repetition of the rapid, forceful motion from the peel-back position to the in-line position pulls the biceps tendon away from the glenoid rim.
Humeral Retroversion
During a baseball pitching motion, a torque about the long axis of the humerus reaches a peak value of 67 ± 11 N•m for adult pitchers15 right before maximum shoulder external rotation. The direction of this torque tends to rotate the distal end of the humerus externally relative to the proximal end. This high torque could lead to deformation of the weak proximal humeral epiphyseal cartilage, causing humeral retroversion over time.44 Humeral retroversion has been found in professional pitchers,31 college pitchers,31,34 and youth baseball pitchers.45 Greater retroversion has been demonstrated to be significantly associated with an increased maximum shoulder external rotation.34,46,47
It is believed that humeral retroversion may be beneficial for baseball pitchers in two respects. First, with greater retroversion of the humerus there is the potential for increased shoulder external rotation, which increases the range of shoulder motion to generate energy and therefore greater ball velocity. Secondly, the shoulder may be more stable to resist anterior force with greater humeral retroversion. This is because the anterior soft tissue structures would have to stretch less for a given amount of external rotation. If the soft tissues are able to stay within their elastic range, they will be better shoulder stabilizers.47 On the other hand, proximal humeral epiphysiolysis is a pathologic response to the shear stress arising from the high torque that causes humeral retroversion.44
FOOTBALL THROWING
An understanding of shoulder biomechanics in baseball pitching serves as a foundation for understanding, preventing, and treating shoulder injuries in other throwing motions. Fleisig and colleagues48 compared throwing kinematics and kinetics between 26 baseball pitchers and 26 football quarterbacks from high schools and colleges. Reflective markers were placed on bony landmarks of subjects, and their motion was analyzed using a three-dimensional automatic digitizing system.
Seven of the eight shoulder kinematic variables that were analyzed showed significant differences (Table 31-5). Compared with pitchers, quarterbacks had greater external rotation at the instant of foot contact. Quarterbacks externally rotated the shoulder 90 ± 33 degrees at foot contact to reach a maximum of 164 ± 12 degrees through the passing motion. Quarterbacks also exhibited a greater degree of shoulder horizontal adduction through ball release than pitchers. Shoulder horizontal adduction of quarterbacks was approximately 7 ± 15 degrees at foot contact, reached a maximum of 32 ± 9 degrees during the arm cocking phase, and decreased to 26 ± 9 degrees at ball release. Quarterbacks also exhibited 96 ± 13 degrees of shoulder abduction at foot contact and reached a maximum of 108 ± 8 degrees during the arm acceleration phase.48
TABLE 31-5 Differences of Shoulder Kinematics Between Baseball Pitching and Football Passing
| Parameter | Pitching (n = 26) Mean ± SD | Passing (n = 26) Mean ± SD |
|---|---|---|
| Lead Foot Contact | ||
| Shoulder abduction (deg) | 93 ± 12 | 96 ± 13 |
| Shoulder horizontal adduction (deg) (P < 0.001) | 17 ± 12 | 7 ± 15 |
| Shoulder external rotation (deg) (P < 0.01) | 67 ± 24 | 90 ± 33 |
| Arm Cocking Phase | ||
| Max shoulder horizontal adduction (deg) (P < 0.001) | 18 ± 8 | 32 ± 9 |
| Max shoulder external rotation (deg) (P < 0.01) | 173 ± 10 | 164 ± 12 |
| Arm Deceleration Phase | ||
| Average shoulder abduction (deg) (P < 0.001) | 93 ± 9 | 108 ± 8 |
| Max shoulder internal rotation velocity (deg/sec) (P < 0.001) | 7 ± 7 | 26 ± 9 |
| Ball Release | ||
| Shoulder horizontal adduction (deg) (P < 0.001) | 7550 ± 1360 | 4950 ± 1080 |
Max, maximum.
Data from Fleisig GS, Escamilla R, Andrews J, et al: Kinematic and kinetic comparison between baseball pitching and football passing. J Appl Biomech 12:207-224, 1996.
Although quarterbacks had greater shoulder external rotation than pitchers at the time of front foot contact, pitchers had greater maximum shoulder external rotation and greater maximum shoulder internal rotation angular velocity. The maximum shoulder internal rotation angular velocity of quarterbacks was 4950 ± 1080 deg/sec compared with 7550 ± 1360 deg/sec for pitchers. The lack of higher angular velocities might be due to the weight of the football, which is three times more than a baseball (0.42 kg and 0.14 kg, respectively). This is also perhaps why quarterbacks rotate their shoulders sooner and farther back, to give them more time to accelerate the arm.48
Of seven shoulder kinetic variables compared between baseball pitching and football passing, only two showed significant differences (Table 31-6). McLeod and Andrews26 proposed that forces about the shoulder could shift the humerus to the rim of the glenoid fossa, causing injury to the anterior glenoid labrum in pitchers. However, no difference in shoulder anterior force between quarterbacks and pitchers was discovered in the current study. The low incidence of anterior glenoid labrum injuries in quarterbacks might be due to their greater horizontal abduction, which helps stabilize the glenohumeral joint. Quarterbacks are also less prone to rotator cuff injury because they have less shoulder proximal force than pitchers (660 ± 120 N compared with 850 ± 140 N). The risk of subacromial impingement is also less in quarterbacks, because they do not externally rotate their shoulders as much as pitchers during the arm-cocking stage.48
TABLE 31-6 Differences of Shoulder Kinetics Between Baseball Pitching and Football Passing
| Parameter | Pitching (n = 26) Mean ± SD | Passing (n = 26) Mean ± SD |
|---|---|---|
| Arm Cocking Phase | ||
| Max shoulder anterior force (N) | 310 ± 50 | 350 ± 80 |
| Max shoulder horizontal adduction torque (N•m) | 82 ± 13 | 78 ± 19 |
| Max shoulder internal rotation torque (N•m) | 54 ± 10 | 54 ± 13 |
| Arm Deceleration Phase | ||
| Max shoulder compressive force (N)* | 850 ± 140 | 660 ± 120 |
| Max shoulder adduction torque (N•m)* | 79 ± 23 | 58 ± 34 |
| Follow-Through Phase | ||
| Max shoulder posterior force(N) | 310 ± 110 | 240 ± 120 |
| Max shoulder horizontal abduction torque (N•m) | 85 ± 51 | 80 ± 34 |
Max, maximum.
Data from Fleisig GS, Escamilla R, Andrews J, et al: Kinematic and kinetic comparison between baseball pitching and football passing. J Appl Biomech 12:207-224, 1996.
The analysis of the kinetic data showed that football passing did not produce higher forces or torques compared with baseball pitching. The incidence of shoulder injuries is also much lower for quarterbacks than for pitchers. The fundamental explanation for this is that quarterbacks limit their trunk kinematic parameters. Quarterbacks had less motion in their legs, pelvis, and upper torso compared with pitchers, and thus quarterbacks were able to limit the amount of forces and torques normally experienced at the shoulder by pitchers. Another explanation for the lower incidence of injury in quarterbacks is that quarterbacks throw much less than pitchers, play in fewer games, and have a greater rest period between games. The quarterbacks thus have less fatigue and instability in the shoulder, with a decreased chance of injury.48
WINDMILL THROWING
Underhand pitching has received little attention in sports medicine due to the perception that the windmill throwing motion produces less stress on the arm and thus injuries to the shoulder are less common; however, this might not be true. In one study of eight collegiate softball teams with 24 pitchers in total, the incidence of upper extremity injuries accounted for 17 of the 26 injuries reported.49
In a study conducted by Barrentine and colleagues,49 the pitching motion of eight female pitchers was analyzed using a three-dimensional automatic digitizing system. The torque values in this study were normalized as percentages of the body weight times body height, and the forces values were normalized as percentages of the body weight. The results, as presented in Table 31-7, showed that the kinematic and kinetic variables were generally low during the wind-up and stride phases. However, during the delivery phase where the arm accelerated quickly to generate ball velocity, the kinematic and kinetic variable magnitudes were quite high and comparable with or higher than those of male overhand baseball pitchers. Compared with overhand-pitching athletes, the shoulder horizontal abduction torque was lower in windmill pitchers (5.3%-7.2% for overhand compared with 3.3% ± 1.4% for windmill), whereas the shoulder internal rotation torque was comparable with overhand athletes (3.7%-5.9% for overhand compared with 4.4% ± 1.5% for windmill). The high shoulder internal rotation torque was probably generated as a result of the shoulder flexion velocity exceeding 5000 deg/sec. The maximum shoulder medial force was 74% ± 14% and the maximum shoulder anterior force was 38% ± 14%, which was comparable with overhand pitchers (39%-44%). All of these variables occurred from 0% to 55% of the delivery phase.49
TABLE 31-7 Differences of Shoulder Kinematics and Kinetics Between Female Windmill Softball Pitchers and Male Overhead Baseball Pitchers
| Parameter | Windmill (n = 8) Mean ± SDa | Overhead Range |
|---|---|---|
| Shoulder flexion velocity 0%-50% of delivery (deg/sec) | 5260 ± 2390 | — |
| Shoulder internal rotation velocity 75%-100% of delivery (deg/sec) | 4650 ± 1200 | 6073–7550b-e |
| Shoulder horizontal adduction torque 0%-50% of delivery (%bw × ht) | 3.3 ± 1.4 | 5.3-7.2b,d,e,f |
| Shoulder internal rotation torque 0%-50% of delivery (%bw × ht) | 4.4 ± 1.5 | 3.7-5.9b,d,e,f |
| Shoulder medial force 0%-50% of delivery (%bw) | 74 ± 14 | — |
| Shoulder anterior force 50%-75% of delivery (%bw) | 38 ± 14 | 39-44b,e |
| Shoulder superior and compressive force 75%-100% of delivery (%bw) | 98 ± 12 | — |
| Shoulder abduction torque 75%-100% of delivery (%bw × ht) | 9.4 ± 4.0 | — |
| Shoulder lateral force 75%-100% of delivery (%bw) | 50 ± 26 | — |
| Shoulder extension torque 75%-100% of delivery (%bw × ht) | 9.8 ± 3.4 | — |
| Shoulder extension/horizontal abduction torque during arm deceleration (%bw × ht) | 9.0 ± 2.7 | 5.3-6.0b,e |
| Shoulder posterior force during arm deceleration (%bw) | 59 ± 13 | 39-46b,e |
| Shoulder superior and compressive force during arm deceleration (%bw) | — | 104-126b,d,e |
bw, body weight; ht = body height.
a Barrentine SW, Fleisig GS, Whiteside JA, et al: Biomechanics of windmill softball pitching with implications about injury mechanisms at the shoulder and elbow. J Orthop Sports Phys Ther 28:405-415, 1998.
b Campbell KR, Hagood SS, Takagi Y, et al: Kinetic analysis of the elbow and shoulder in professional and little league pitchers. Med Sci Sports Exerc 26: S175, 1994.
c Dillman CJ, Fleisig GS, Andrews JR: Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther 18:402-408, 1993.
d Feltner M, Dapena J: Dynamics of the shoulder and elbow joints of the throwing arm during a baseball pitch. Int J Sport Biomech 2:235-259, 1986.
e Fleisig GS, Andrews JR, Dillman CJ, et al: Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 23:233-239, 1995.
f Werner SL, Fleisig GS, Dillman CJ, et al: Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther 17:274-278, 1993.
During the latter part of the delivery phase, 75% to 100%, the shoulder of the windmill pitcher experienced a maximum superior force of 98% ± 12% and a maximum lateral force of 50% ± 26%. The shoulder then internally rotated quickly at 4650 ± 1200 deg/sec. The torques at the shoulder were quite high at this point: 9.4% ± 4.0% shoulder abduction torque, and 9.8% ± 3.4% shoulder extension torque. Peak horizontal abduction torque, which was much higher than that for overhand pitchers, occurred after ball release (5.3%-6.0% for overhand compared with 9.0% ± 2.7% for windmill). A shoulder posterior force of 59% ± 13% was also experienced at this time, which was higher than the shoulder posterior force of overhand pitchers (39%-46%).49
Glenohumeral joint stability is of question during windmill pitching, much as in overhand pitching. Unlike with overhand pitching, where the humerus is held in an abducted position during the pitch, leading to shoulder joint instability, the shoulder instability in windmill pitching comes from resistance to distraction and the shoulder’s controlling internal rotation and elbow extension. The arm rotates a total of 485 degrees around the shoulder with the arm fully extended, and this increases shoulder distraction force. Another difference between overhand and windmill pitching is that the maximum resistance to distraction occurs during the arm acceleration phase in overhand pitching, but the maximum resistance to distraction occurs during the arm deceleration phase in windmill pitching. The magnitude of distraction in windmill pitching was approximately 80% to 95% of the magnitude of distraction measured in overhand pitching, so the magnitudes were quite similar.49
Anterior shoulder discomfort near the origin of the long head of the biceps tendon is a problem that many windmill pitchers experience. Usually this discomfort is treated with injections of a steroid or analgesic into the bicipital tendon area. However, the discomfort could actually be subscapularis or pectoralis strain due to increased shoulder extension followed by large forces and torques during the delivery motion. In addition, the long head of the biceps acts as a humeral head depressor. The biceps brachii undergoes a lot of strain as it prevents humeral distraction during the delivery phase, and it provides elbow flexion torque to control elbow extension and initiate elbow flexion. This can lead to overuse injury.49
Because both genders were compared in the study, the musculoskeletal differences between the two groups must also be accounted for. Comparisons between windmill and overhand pitching showed similar joint speeds and joint loads. In addition to experiencing high forces and torques, the demands on a female windmill pitcher are much higher than those on a male overhand pitcher. An overhand pitcher might get 3 or 4 days of rest between games, but windmill pitchers might pitch two days in a row and possibly even twice in the same day.49 Thus, the risk of overuse injury is quite high, and it can be speculated that windmill pitching can be quite hard on the pitcher and comparable with overhand pitching.
JAVELIN THROWING
Like other types of throws, javelin throwing requires an efficient kinetic chain to generate energy to achieve maximum results. A good indicator of performance in overhead throwing sports is increased external rotation. In a study by Herrington,50 javelin throwers were tested to determine their external rotation and internal rotation angles. Shoulder range of motion was measured with the subject in a supine position with the arm abducted and elbow flexed approximately 90 degrees. Shoulder external rotation was significantly greater in the throwing arm (approximately 90 degrees) than in the nonthrowing arm (approximately 70 degrees), and internal rotation was approximately 50 degrees for both arms.
Javelin throwers may be susceptible to over-rotation injuries, much like baseball pitchers. As discussed in the section on shoulder pathomechanics during baseball pitching, higher external rotation of the throwing shoulder could increase the chance of injury to the shoulder. Impingement of the rotator cuff can become an issue because it is impinged between the glenoid labrum and the humeral head. This weakens the rotator cuff muscles, which are then less effective to resist anterior humeral head displacement. The end result is increased strain on the glenohumeral joint. Both of these factors can lead to pathologic changes in the shoulder, resulting in an increased chance of injury.36
The weight, size, inertia, and vibration properties of a javelin can also cause problems to the shoulder. A javelin can be 0.4 to 0.8 m long (1.3 to 2.6 feet) and weigh as much as 0.8 kg (28 oz.).51 This is more than five times the weight of a baseball. However, no research has been performed on these subjects, so no definitive statements can be made on how the physical properties of the javelin affect forces and torques on the shoulder.
CRICKET THROWING AND BOWLING
The mass of a cricket ball is slightly greater than the mass of a baseball, 5.50 to 5.75 oz for a cricket ball compared with 5.00 to 5.75 oz for a baseball. Although the throwing motion in cricket is quite comparable with the throwing motion in baseball, the cricket bowling motion is quite different from baseball pitching. The demands placed on the shoulder to generate velocity in bowling and throwing in cricket can eventually lead to injury. Fielding in cricket and baseball involves picking up a ball and throwing it to a particular location quickly and accurately. This is especially important in cricket, where the thrower might have to be extremely accurate in throwing out a runner by hitting three small stationary sticks. As in any kind of throwing, a kinematic series of events must occur to throw efficiently.
There are quite a few differences in the sport of cricket compared with baseball that could affect athletes. In cricket, the entire field of play is a circle or oval approximately 375 to 525 feet in diameter, whereas the field of play in baseball ranges from 290 to 410 feet from the batter’s box. When in play, cricket batters have to run approximately 60 feet to be safe, and baseball hitters have to run 90 feet to reach a safe base.52 The temporal differences associated with these sports can have a big impact on the athlete.
The bowler’s role in cricket is similar to a baseball pitcher’s role. However, unlike baseball pitching, where the pitcher is static on the mound before throwing, the cricket bowler runs up to the bowling location, gradually increasing speed, and leaps into the air to a predelivery phase. This provides additional energy to the kinetic chain of the cricket delivery. The bowler then lands with the back foot down and the upper trunk tilted away from the batter. The hands part, and between the times of rear foot contact and lead foot contact, the arm is rotated and then quickly counter-rotated around the glenohumeral joint. The elbow is barely flexed, if it is flexed at all, during this counterrotation, and the arm is accelerated as it circumducts the glenohumeral joint.53
There have been no biomechanical studies that have determined kinematic or kinetic magnitudes of this action. These variables could have been used to determine injury mechanisms associated with cricket bowling such as rotator cuff sprain and subacromial impingement. The bowler’s lead foot has to land behind a marked line. If that line is passed, the throw is deemed illegal. The ball is released a little later in the rotation compared with baseball pitching, as it is usually meant to bounce before reaching the batter. Pitch speeds can exceed 90 mph, as in baseball pitching.53 The bowler has to bowl six legal throws before one over (comparable with an inning in baseball) is complete, after which he is replaced by another bowler. The bowlers may then alternate bowling if they wish to do so.
Most bowling injuries are related to the lower back, but many injuries occur at the throwing shoulder as well.54 The injuries to the shoulder in cricket include rotator cuff sprain and subacromial impingement.55 How the shoulder is angled toward the batter is also a key indicator of throwing technique. When the bowler’s shoulders are perpendicular to the batter at rear foot contact, the bowler is said to be a side-on bowler. When the bowler’s shoulders are more rotated toward the batter at rear foot contact (rotated approximately 20 degrees or more toward the pitcher), the bowler is said to be a front-on bowler. A third type of bowler, a mixed bowler, possesses characteristics of both the other types of bowlers, where initially the bowler has a front-on technique at rear foot contact and then changes to a side-on technique during the delivery stride.53
As in baseball, the shoulder externally rotates and prepares for the arm acceleration phase during the arm cocking phase or preparation phase in cricket, as referred to by Cook and Strike.56 In baseball pitching and throwing, the shoulder externally rotates to about 170 degrees.4,15 In cricket throwing, the external rotation is only about 150 degrees.56 Because the elbow is not flexed in the cricket throwing motion, as it is in baseball pitching, the athlete might not be able to externally rotate the shoulder as much. This may be due to the greater inertia of the forearm when the elbow is flexed closer to 90 degrees. On the other hand, the decreased external rotation in cricket bowling might simply be because maximizing external rotation when the elbow is not flexed does not give a biomechanical advantage. This could be due to time limitation placed on a thrower to throw out a runner. In baseball, the pitcher and fielder have more time to externally rotate their shoulders and generate more ball velocity. Cricket throwers only averaged about 68 mph when throwing from the outfield. Once maximum external rotation has been reached, the shoulder quickly internally rotates to accelerate the arm, much as in baseball.56
HANDBALL
Handball places heavy demands on the thrower’s shoulder. This sport is popular mainly in Europe. As in other sports, the thrower activates a kinetic chain of body movements to develop the energy to throw with velocity. One study found that 53% of the resultant ball velocity was due to arm action, and the remaining 47% was due to lower and upper trunk angular velocity.58 This shows the importance of using the entire body to generate ball velocity as opposed to throwing only with the arm. Increased or high range of motion and stability of the shoulder allow the ball to be thrown with higher velocity because the internal and external rotator muscles are more efficient.58 Strengthening these muscles could also help generate higher ball velocity.
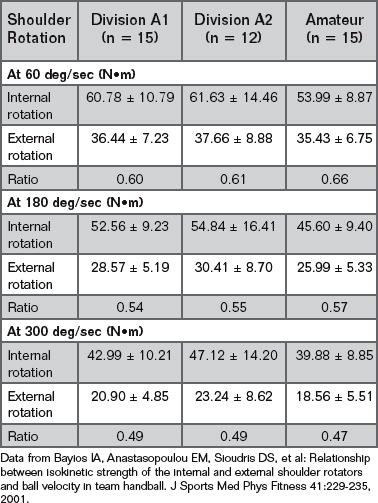
Bayios and colleagues59 studied the relation between ball velocity in handball and isokinetic strength of the shoulder rotator muscles. Forty-two subjects at three different levels were studied: Division A1, Division A2, and amateur. Shoulder strength during concentric internal and external rotation was measured using an isokinetic dynamometer at three rates: 60 deg/sec, 180 deg/sec, and 300 deg/sec. Shoulder external rotation was measured with the shoulder abducted at 90 degrees and the elbow flexed at 90 degrees. There were no significant differences in any of the variables among the three skill levels (Table 31-8). The shoulder external rotation strength was always less than the shoulder internal rotation strength, ranging anywhere from 47% to 66% of the internal rotation strength. The measured strength of both internal and external rotation decreased as the isokinetic rate of testing was increased.
TABLE 31-8 Peak Torque Values of Concentric Internal and External Rotational Shoulder Strength of Three Levels of Skill
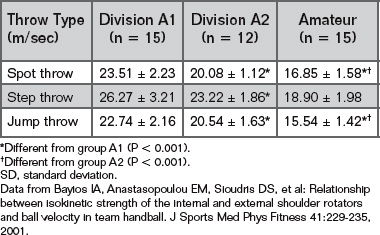
Ball velocity was also measured for each skill level for three different throws: on the spot, crossover step, and vertical jump (Table 31-9). There were significant differences between skill levels for each type of throw. Specifically, as skill level decreased, the throwing velocity decreased regardless of throw type.59
In general, there was no relationship between ball velocity and isokinetic strength of the internal and external rotators regardless of the type of throw or experience level. This was quite surprising because even though ball velocity increased between the groups, no increase in internal or external rotation torque was noticed. The few significant relationships that were discovered occurred during the jump throw for levels A1 and A2. However, these relationships were not very clear and no conclusion could be obtained from the data.59 In a previous study, Fleck and colleagues60 found that there was a relationship between internal rotation strength and ball velocity for the jump shot. This implies that the upper extremity rotation is more important when making a jump shot. The explanation could be that because the feet are off the ground, the lower body is not as able to generate torque to provide energy to increase ball velocity.
There appears to be some fundamental difference between handball throwing and the throwing motion seen in baseball. Furthermore, no relationship between range of motion of the shoulder and ball velocity was discovered in handball athletes. Other factors, like lower extremity rotation, perhaps play a bigger role in generating ball velocity, especially when throwing from flat ground.
TENNIS SERVE
The tennis serve, much like the other throwing sports, uses a kinetic chain to develop energy to generate ball velocity. However, there are two main differences in the tennis serving motion. In addition to the human kinetic chain involved in the serve, there is another kinetic contribution from the racquet. Furthermore, instead of throwing or releasing the ball, the athlete strikes the ball. These two differences could have varying effects on the shoulder when compared with a typical throwing motion.
The tennis serve requires the athlete to repetitively strike the tennis ball in a manner that makes the shoulder susceptible to overuse injury. Hill61 reported injury rates as high as 56% in competitive tennis players. They suffered from various injuries, including rotator cuff and shoulder impingement injuries. According to Elliott and colleagues62 up to 50% of the resultant linear racquet head velocity was related to shoulder internal rotation. The forces experienced by the shoulder during the tennis serve can thus cause distraction of the shoulder. Understanding the kinematic and kinetic parameters of the serve motion can lead to a better understanding of the injury mechanism and how to reduce the chance of injury.
Fleisig and colleagues63 and Elliott and colleagues62 described kinematic and kinetic variables of the tennis serve. Using two high-speed, electronically synchronized video cameras at the XXVII Olympic Games, data from 20 elite tennis athletes, both male and female, were collected. Using manual digitizing and a computer program that calculated angles, velocities, forces, and torques, the magnitudes of kinematic and kinetic variables were calculated. The shoulder kinematic and temporal values from the study are displayed in Table 31-10. Tennis athletes exhibited a high value of maximum external rotation, 172 ± 12 degrees, which was similar to that of elite baseball pitchers. As in baseball pitching, this large value of external rotation can be attributed to a combination of glenohumeral rotation, scapulothoracic motion, and trunk extension. Maximum external rotation occurred 95 ± 14 msec before ball impact with the racquet. The shoulder was abducted approximately 100 degrees and horizontally abducted about 6 degrees at both maximum external rotation and ball impact.63 The abduction angle of 100 degrees supported the hypothesis made by Atwater and colleagues64 that the arm is usually abducted about 90 degrees in overhand sports. The angle’s magnitude is also similar to that proposed by Matsuo and colleagues65 for maximizing ball velocity and minimizing loading of the shoulder.
TABLE 31-10 Kinematic and Temporal Parameters Measured in Olympic Tennis Athletes
| Parameter | Mean ± SD (n = 20) |
|---|---|
| Shoulder external rotation at maximum shoulder external rotation (deg) | 172 ± 12 |
| Shoulder abduction at maximum shoulder external rotation (deg) | 101 ± 13 |
| Shoulder horizontal adduction at maximum shoulder external rotation (deg) | 7 ± 9 |
| Male shoulder internal rotation at maximum angular velocity (deg/sec) | 2420 ± 590 |
| Female shoulder internal rotation at maximum angular velocity (deg/sec) | 1370 ± 730 |
| Shoulder abduction at instant of ball impact (deg) | 101 ± 11 |
| Shoulder horizontal adduction at instant of ball impact (deg) | 5 ± 10 |
| Maximum shoulder external rotation as time before ball impact (ms) | 95 ± 14 |
| Maximum shoulder internal rotation velocity as time before ball impact (ms) | 10 ± 18 |
SD, standard deviation.
Data from Elliott B, Fleisig GS, Nicholls R, et al: Technique effects on upper limb loading in the tennis serve. J Sci Med Sport 6:76-87, 2003.
After maximum shoulder external rotation, the shoulder internally rotates quickly to generate the energy needed to accelerate the arm and racquet. In Fleisig’s study, shoulder internal rotation angular velocity reached a maximum of 2420 ± 590 deg/sec for men and 1370 ± 730 deg/sec for women approximately 10 msec before ball impact.63 Although the angular velocities were quite high, they were much less than the maximum shoulder internal rotation angular velocity of baseball pitchers (7400 deg/sec).17 This could be attributed to the mass, moment of inertia, and air resistance of the racquet, which slowed down the internal rotation.63 The large difference in internal rotation angular velocity of the two genders is the greater internal rotation strength of male tennis players.62
Because men generate more ball velocity, they are also subjected to larger forces and torques. In the study by Elliott and associates62 shoulder forces and torques in male and female tennis athletes were compared (Table 31-11). The normalized and absolute internal rotation torques of men were found to be significantly greater than those of women when the arm was externally rotated to its maximum position (4.6% ± 0.9% and 64.9 ± 15.8 N•m for men compared with 3.5% ± 1.2% and 37.5 ± 15.0 N•m for women). Peak values for normalized horizontal abduction torque (7.6% ± 0.8% for men compared with 6.5% ± 0.9% for women), normalized shoulder proximal force (79.6% ± 5.3% for men compared with 59.1% ± 8.4% for women), and absolute proximal force (608.3 ± 109.5 N for men compared with 363.7 ± 87.8 N for women) were also higher in the male tennis players.62
TABLE 31-11 Differences of Shoulder Kinetics Between Male and Female Tennis Athletes
| Parameter | Male (n = 8) Mean ± SD | Female (n = 12) Mean ± SD |
|---|---|---|
| Internal Rotation Torque at Maximum External Rotation | ||
| As a percentage of body weight times height* | 4.6 ± 0.9 | 3.5 ± 1.2 |
| In Newton meters* | 64.9 ± 15.8 | 37.5 ± 15.0 |
| Horizontal Adduction Torque at Maximum External Rotation | ||
| As a percentage of body weight times height | 4.2 ± 1.7 | 3.5 ± 1.4 |
| In Newton meters | 61.7 ± 31.0 | 36.8 ± 16.3 |
| Peak Internal Rotation Torque | ||
| As a percentage of body weight times height | 5.1 ± 0.9 | 4.5 ± 1.3 |
| In Newton meters | 71.2 ± 15.1 | 47.8 ± 16.3 |
| Peak Horizontal Adduction Torque | ||
| As a percentage of body weight times height* | 7.6 ± 0.8 | 6.5 ± 0.9 |
| In Newton meters | 107.8 ± 24.9 | 68.8 ± 14.3 |
| Peak Anterior Force | ||
| As a percentage of body weight | 38.5 ± 14.0 | 30.5 ± 10.2 |
| In Newtons | 291.7 ± 119.8 | 185.1 ± 60.9 |
| Peak Proximal Force | ||
| As a percentage of body weight* | 79.6 ± 5.3 | 59.1 ± 8.4 |
| In Newtons* | 608.3 ± 109.5 | 363.7 ± 87.8 |
SD, standard deviation.
* Significant difference between male and female subjects (P < 0.01).
Data from Fleisig GS, Nicholls R, Elliott B, et al: Kinematics used by world class tennis players to produce high-velocity serves. Sports Biomech 2:51-64, 2003.
The higher forces and torques experienced by the male tennis players were a result of men exerting themselves to a greater degree to generate higher service velocities. The magnitude of shoulder internal rotation torque and shoulder horizontal adduction torque both exceeded Dillman and coworkers’66 implication that any torque greater than 50 N•m was loading the shoulder excessively. According to this assertion, the shoulder is subject to excessive loading, and because of the repetitive nature of the tennis serve, the shoulder could be susceptible to overuse injury.
Another issue that must be considered is the effect of muscle imbalance. Chandler and colleagues67 found this phenomenon in the college tennis players they tested. In this study, the tennis players had stronger internal rotator muscles compared with external rotator muscles. Specifically, when isokinetic strength testing was performed at a rate of 60 deg/sec, the external rotation peak torque was approximately 60% of the internal rotation peak torque in the dominant arm. When handball athletes performed the same isokinetic exercise, the external rotation peak torque was approximately 60% of the internal rotation peak torque in the dominant arm as well.59 In the nondominant arm of the tennis player, the ratio of external to internal rotation torque was 70%.67 The idea is that the internal rotators increased in strength as serving power increased, but the external rotators that decelerate the arm did not increase in strength enough. This strength difference or imbalance can cause a problem with how the repetitive arm motion is decelerated.
BASEBALL SWING
The baseball swing requires the shoulders to accelerate quickly in coordination with the hips and arms to generate energy to hit a baseball. Although the swing is not as hard on the shoulder as a pitch or throw is, there are still numerous problems associated with the swinging mechanism. One such problem is posterior instability of the lead shoulder.
To discuss the injury pathology related to the baseball swing, it is important to understand how the baseball swing can be hard on the shoulder. One study by Welch and colleagues68 focused on quantifying the kinematics of the baseball swing. Seven subjects were included in the study. Each batter hit off a tee to minimize the effects of reaction time, pitch type, and pitch speed. The investigators identified three events in the baseball swing: foot off, foot down, and ball contact. The time between the foot off and foot down was the stride phase. Between foot down and ball contact was the swing phase. The follow-through phase was the part of the swing after ball contact. Welch’s group also defined the shoulders, hips, and arms as segments rotating around the spine. They modeled the hips as a vector from the back hip to the leading hip, the shoulders as a vector from the back shoulder to the leading shoulder, and the arms as a vector from the mid shoulders to mid wrists. The rotations of the segments were calculated as rotations around a common spine axis, which was defined as the mid shoulders to the mid hips. For the sake of discussion, clockwise and counterclockwise refer to the direction of rotation of a segment about the common spine axis as viewed from above for a right-handed batter.
During the foot-off phase, the batter shifts the weight from the lead leg to the back leg and rotates the upper body (shoulders and arms) clockwise away from the mound. The hips then rotate clockwise as well. This is referred to as the coiling process. The batter then shifts the weight forward, planting the lead leg in the ground to provide an axis of rotation during the foot-down phase. During this phase, the hips rotate counterclockwise, and shortly after this, the shoulders and arms rotate counterclockwise as well. The bat is then swung around as the arms rotate counterclockwise.68
The shoulders undergo different motions during batting. During the foot-off phase, when the batter shifts the weight to the back leg, the shoulder vector rotates clockwise about 30 degrees from the initial starting point facing the mound. The batter strides forward, further rotating the shoulders clockwise to increase the coiling effect. At this point, the shoulders are 52 degrees back from the initial starting point. The batter then plants the lead leg, and the shoulders now rotate counterclockwise toward the mound. At foot contact, the shoulders are rotated about 29 degrees clockwise from the initial starting point. The batter then explodes toward the ball by quickly whipping the pelvis and then the upper trunk counterclockwise toward the mound. The shoulder vector reaches a maximum rotational velocity of 937 deg/sec about 65 msec before ball contact. The batter then follows through until the shoulders come to rest at a position −66 degrees from the starting position.68
Posterior instability of the leading shoulder could develop in batters due to the repetitive extreme range of motion while swinging. This effect might be increased when a batter faces an outside pitch where the batter has to extend, having increased horizontal flexion to hit the baseball. This means that there is more shear force acting across the glenohumeral joint. In an unpublished study of two baseball hitters with complaints of posterior instability, the players described a feeling of subluxation after ball contact. Biomechanical data showed that the lead shoulder had 83 degrees and 98 degrees of horizontal flexion when hitting an inside pitch and 98 degrees and 110 degrees of horizontal flexion when hitting an outside pitch. When the batter pulled the ball, horizontal flexion increased to 100 degrees and 115 degrees. In this study of two batters, it was hypothesized that higher horizontal flexion correlated with increased posterior glenoid shear force because of the way the shoulder horizontally flexed. The higher force could cause trauma to the posterior capsular restraints. Additionally, the mass of the bat factors in as a variable and contributes to the increased forces experienced in the glenohumeral joint. Both variables combine to present a condition where the shoulder is subject to laxity that allows periodic subluxation.69
GOLF SWING
The golf swing seems harmless, but this is hardly the case. Both shoulders are susceptible to injury either from overuse or from poor technique, especially the lead shoulder. Studies show that almost 90% of shoulder injuries in golf are injuries to the leading shoulder. Younger golfers tend to develop shoulder instability, middle-aged golfers are more likely to suffer subacromial impingement, and older golfers are susceptible to arthrosis of the glenohumeral joint.70,71
The golf swing is generally broken up into four phases: set-up, backswing, downswing, and follow-through.72 The chance of injury and injury type vary with each phase. During the set-up phase, where the golfer lines up with the ball, the back shoulder tilts from the combination of spine flexion and the downward rotation of the back arm and scapula. The golfer then initiates the swinging motion by shifting weight to the back foot. When this happens, the right shoulder picks up and the hips rotate as the shoulders rotate. At the top of the back swing, shoulder rotation ranges from 78 to 102 degrees depending on skill level. The left shoulder then rotates internally and adducts horizontally. It is at this position that the left rotator cuff and scapular muscles are stretched, potentially placing the glenohumeral joint in an impinged position.72,73 This stretch also gives a golfer the X-factor, which is the lag of the hips compared with the shoulders. With this lag, energy is transferred from the legs up to the hips, shoulders, arms, and wrists.72
During the downswing, the shoulder accelerates quickly, following the hips to generate energy to drive the ball. In one study, the shoulder angular velocity for professional golfers was 723 deg/sec.74 Hume and colleagues72 found that the shoulders were responsible for about 20% of the club-head speed. The primary contribution came from the wrists (70%). In the follow-through, the lead shoulder externally rotates and abducts while the back shoulder adducts and internally rotates. The motion of the lead shoulder here could lead to anterior instability or biceps tendinitis.73
Golfers work hard to increase shoulder flexibility to maximize their ability to rotate their shoulders to produce maximum club speed. Jobe and colleagues75 found that rotator cuff disease and subacromial impingement were the most common shoulder injuries and accounted for 93% of shoulder injuries. The mechanism for impingement as discussed earlier was the internal rotation and horizontal adduction of the left shoulder across the chest that occurs at the top of the backswing. Sometimes, the capsular and labral structures become injured, and hyperlaxity of the shoulder can also become a problem.76 Instability could also arise due to the adduction across the body in the backswing phase. Anterior instability can occur at the end of the follow-through when the arm experiences maximum abduction and external rotation. Arthritis in old age is another problem. Glenohumeral arthroplasty is usually the treatment, and golfers return to playing within a few months.73 The best way to prevent some of these injuries is to practice proper technique and refrain from playing excessively.
SWIMMING
Swimming is considered to be an overhead sport much like the others sports previously discussed. The shoulder is put through a great deal of stress as the internal rotators fire and the arm abducts during the acceleration phase, and then firing of the external rotators occurs to decelerate the arm.67,77 This can be especially problematic for swimmers who repetitively execute this motion under water, making their shoulders susceptible to injury.
The most common ailment of swimmers is impingement associated with glenohumeral instability or too much laxity.77,78 Injury to the shoulder could also be related to an imbalance of external and internal rotator muscles. When compared with nonswimmers, swimmers had a lower external rotation to internal rotation strength ratio (0.75 ratio for nonswimmers and 0.64 in swimmers). This was because the swimmers exhibited higher internal rotation strength.79 This same phenomenon is also measured in people who have impinged shoulders. It has also been noted in numerous studies that overhead athletes have greater external rotation range of motion at the cost of internal rotation range of motion (Table 31-12).79,80
TABLE 31-12 Mean and SD Differences of Shoulder Range of Motion Between Swimmers and Nonswimmers
| RIGHT SHOULDER RANGE OF MOTION (DEGREES) | ||
|---|---|---|
| Parameter | Swimmer | Nonswimmer |
| External Rotation | ||
| Arm adducted | 69 ± 14 | 59 ± 14 |
| Arm adducted 90 deg | 115 ± 14 | 80 ± 12 |
| Internal Rotation | ||
| Arm adducted | 96 ± 4 | 92 ± 5 |
| Arm adducted 90 deg | 74 ± 14 | 63 ± 12 |
SD, standard deviation.
Data from Rupp S, Berninger K, Hopf T: Shoulder problems in high level swimmers—impingement, anterior instability, muscular imbalance? Int J Sports Med 16:557-562,1995.
In a study of elite swimmers and nonswimmers, Rupp and colleagues81 measured the shoulder range of motion of swimmers and nonswimmers and compared the values. There was no difference in range of motion between the left and right shoulders for the swimming or nonswimming athlete. However, when the swimming and nonswimming athletes’ shoulder range of motion was compared, significant differences were found. Because differences between the left and right shoulders were insignificant, only measurements for the right shoulder are discussed here (see Table 31-12). When looking at shoulder external rotation with the arm adducted 90 degrees, the swimmers had 115 ± 14 degrees of external rotation, whereas the nonswimmers only had 80 ± 12 degrees of external rotation. When looking at shoulder internal rotation with the arm adducted 90 degrees, the swimmers had 74 ± 14 degrees of internal rotation, whereas the nonswimmers only had 63 ± 12 degrees of internal rotation.
Rupp and colleagues81 also reported isokinetic strength testing to measure the peak internal and external rotation torques (Table 31-13). There was no difference in external rotation peak torque values. However, the swimmers did have higher internal rotation peak torque values. In general, there appeared to be a 12-N•m difference of strength between the external and internal rotator muscles. Thus, the ratio of external to internal rotator strength was less for swimmers than for nonswimmers. Furthermore, the external to internal ratio of strength in swimming, 0.64,81 was comparable with the external to internal ratio of strength in handball, 0.66 to 0.60,59 and tennis, 0.60.67
TABLE 31-13 Mean and SD Isokinetic Peak Torque Values for External and Internal Rotation for Male Swimmers and Nonswimmers
| Parameter | Male Swimmer | Male Nonswimmer |
|---|---|---|
| External Rotation Peak Torque at 60 deg/sec (N•m) | ||
| Right | 33.16 ± 9.27 | 32.77 ± 11.84 |
| Left | 29.18 ± 6.54 | 28.99 ± 10.50 |
| External Rotation Peak Torque 180 deg/sec (N•m) | ||
| Right | 32.62 ± 13.49 | 29.35 ± 9.73 |
| Left | 31.04 ± 8.25 | 29.11 ± 9.21 |
| Internal Rotation Peak Torque 60 deg/sec (N•m) | ||
| Right | 45.43 ± 9.76* | 31.17 ± 11.18 |
| Left | 45.70 ± 8.70* | 33.31 ± 11.13 |
| Internal Rotation Peak Torque 180 deg/sec (N•m) | ||
| Right | 44.34 ± 12.04 | 34.04 ± 13.32 |
| Left | 45.50 ± 10.85* | 30.52 ± 11.87 |
SD, standard deviation.
* Significantly different from male nonswimmers (P < 0.05).
Data from Rupp S, Berninger K, Hopf T: Shoulder problems in high level swimmers—impingement, anterior instability, muscular imbalance? Int J Sports Med 16:557-562,1995.
SUMMARY
Athletic injuries are a serious problem for the shoulder joint. Throwing injuries are of particular concern, because these injuries are common, disabling, and to some extent preventable. During the baseball pitch and other overhand throwing motions, the shoulder is abducted, rotated into maximum external rotation, and then rapidly internally rotated. Large forces and torques are produced to terminate external rotation, initiate internal rotation, prevent distraction, and control abduction and horizontal adduction. These forces and torques may be even larger and more dangerous if the athlete uses improper mechanics. The shoulder also goes through significant range of motion during underhand and striking motions in sports.
An understanding of the kinematics and kinetics of the shoulder during athletic activity is essential for good treatment of shoulder injury. The physician, physical therapist, athletic trainer, or other health care professional must design treatment and rehabilitation appropriate for the demands that will be placed on the shoulder. An understanding of biomechanics is just as critical for the strength coach, technique coach, and others who work with the athlete to optimize performance and minimize the risk of injury. Shoulder biomechanics presented in this chapter serve as a foundation to the sports medicine clinician for reading the rest of this book.
1 Dillman CJ. Proper mechanics of pitching. Sports Med Update. 1990;5:15-18.
2 Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther. 1993;18:402-408.
3 Fleisig GS, Dillman CJ, Andrews JR. Proper mechanics for baseball pitching. Clin Sports Med. 1989;1:151-170.
4 Werner SL, Fleisig GS, Dillman CJ, et al. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17:274-278.
5 Fleisig GS, Escamilla RF, Barrentine SW. Biomechanics of pitching: Mechanism and motion analysis. In: Andrews JR, Zarins B, Wilk KE, editors. Injuries in Baseball. Philadelphia: Lippincott–Raven; 1998:3-22.
6 Jobe FW, Tibone JE, Perry J, et al. An EMG analysis of the shoulder in throwing and pitching. A preliminary report. Am J Sports Med. 1983;11:3-5.
7 Jobe FW, Moynes DR, Tibone JE, et al. An EMG analysis of the shoulder in pitching. A second report. Am J Sports Med. 1984;12:218-220.
8 Sisto DJ, Jobe FW, Moynes DR. An electromyographic analysis of the elbow in pitching. Am J Sports Med. 1987;15:260-263.
9 Bradley JP, Tibone JE. Electromyographic analysis of muscle action about the shoulder. Clin Sports Med. 1991;10:789-805.
10 DiGiovine NM. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg. 1992;1:15-25.
11 Glousman R, Jobe F, Tibone J, et al. Dynamic electromyographic analysis of the throwing shoulder with glenohumeral instability. J Bone Joint Surg Am. 1988;70:220-226.
12 Gowan ID, Jobe FW, Tibone JE, et al. A comparative electromyographic analysis of the shoulder during pitching. Professional versus amateur pitchers. Am J Sports Med. 1987;15:586-590.
13 Jacobs P. The overhand baseball pitch: A kinesiological analysis and related strength-conditioning programming. NCSA J. 1987;9:5-13.
14 Feltner M, Dapena J. Dynamics of the shoulder and elbow joints of the throwing arm during a baseball pitch. Int J Sport Biomech. 1986;2:235-259.
15 Fleisig GS, Andrews JR, Dillman CJ, et al. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239.
16 Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseball pitching. A preliminary report. Am J Sports Med. 1985;13:216-222.
17 Fleisig GS, Barrentine SW, Zheng N, et al. Kinematic and kinetic comparison of baseball pitching among various levels of development. J Biomech. 1999;32:1371-1375.
18 Dillman CJ, Fleisig GS, Werner SL, et al. Biomechanics of the shoulder in sports: Throwing activities. In: Prentice W, Hooker DN, editors. Postgraduate Studies in Sports Physical Therapy. Berryville, Va: Forum Medicum; 1991:1-9.
19 Cosgarea AJ, Campbell KR, Hagood SS, et al. Comparative analysis of throwing kinematics from little league to professional baseball pitchers. Med Sci Sports Exerc. 1993;25:S131.
20 Campbell KR, Hagood SS, Takagi Y, et al. Kinetic analysis of the elbow and shoulder in professional and little league pitchers. Med Sci Sports Exerc. 1994;26:S175.
21 Dun S, Fleisig GS, Loftice JW, et al. The relationship between age and baseball pitching kinematics in professional baseball pitchers. J Biomech. 2007;40:265-270.
22 Escamilla R, Fleisig G, Barrentine S, et al. Kinematic comparisons of throwing different types of baseball pitches. J Appl Biomech. 1998;14:1-23.
23 Fleisig GS, Kingsley DS, Loftice JW, et al. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am J Sports Med. 2006;34(3):423-430.
24 Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30:136-151.
25 Fleisig GS, Escamilla RF, Barrentine SW, et al: Kinematic and kinetic comparison of baseball pitching from a mound and throwing from flat ground. American Society of Biomechanics Conference Proceedings of the 20th Annual Meeting, Atlanta, Ga, 1996, pp 153-154.
26 McLeod WD, Andrews JR. Mechanisms of shoulder injuries. Phys Ther. 1986;66:1901-1904.
27 Andrews JR, Kupferman SP, Dillman CJ. Labral tears in throwing and racquet sports. Clin Sports Med. 1991;10:901-911.
28 Andrews JR, Angelo RL. Shoulder arthroscopy for the throwing athlete. Tech Orthop. 1988;3:75-81.
29 Bigliani LU, Codd TP, Connor PM, et al. Shoulder motion and laxity in the professional baseball player. Am J Sports Med. 1997;25:609-613.
30 Brown LP, Niehues SL, Harrah A, et al. Upper extremity range of motion and isokinetic strength of the internal and external shoulder rotators in major league baseball players. Am J Sports Med. 1988;16:577-585.
31 Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002;30:20-26.
32 Ellenbecker TS, Roetert EP, Bailie DS, et al. Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers. Med Sci Sports Exerc. 2002;34:2052-2056.
33 Baltaci G, Johnson R, Kohl HIII. Shoulder range of motion characteristics in collegiate baseball players. J Sports Med Phys Fitness. 2001;41:236-242.
34 Reagan KM, Meister K, Horodyski MB, et al. Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players. Am J Sports Med. 2002;30:354-360.
35 Meister K, Day T, Horodyski M, et al. Rotational motion changes in the glenohumeral joint of the adolescent/Little League baseball player. Am J Sports Med. 2005;33:693-698.
36 Zheng N, Fleisig GS, Andrews JR. Biomechanics and injuries of the shoulder during throwing. Athletic Therapy Today. 1999;4:4-10.
37 Snyder SJ, Karzel RP, Del Pizzo W, et al. SLAP lesions of the shoulder. Arthroscopy. 1990;6:274-279.
38 Andrews JR, Carson WGJr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13:337-341.
39 Bey MJ, Elders GJ, Huston LJ, et al. The mechanism of creation of superior labrum, anterior, and posterior lesions in a dynamic biomechanical model of the shoulder: The role of inferior subluxation. J Shoulder Elbow Surg. 1998;7:397-401.
40 Morgan CD, Burkhart SS, Palmeri M, et al. Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14:553-565.
41 Burkhart SS, Morgan CD. The peel-back mechanism: Its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy. 1998;14:637-640.
42 Shepard MF, Dugas JR, Zeng N, et al. Differences in the ultimate strength of the biceps anchor and the generation of type II superior labral anterior posterior lesions in a cadaveric model. Am J Sports Med. 2004;32:1197-1201.
43 Jazrawi LM, McCluskey GMIII, Andrews JR. Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. AAOS Instr Course Lect. 2003;52:43-63.
44 Sabick MB, Kim YK, Torry MR, et al. Biomechanics of the shoulder in youth baseball pitchers: Implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med. 2005;33:1716-1722.
45 Mair SD, Uhl TL, Robbe RG, et al. Physeal changes and range-of-motion differences in the dominant shoulders of skeletally immature baseball players. J Shoulder Elbow Surg. 2004;13:487-491.
46 Kronberg M, Brostrom LA, Soderlund V. Retroversion of the humeral head in the normal shoulder and its relationship to the normal range of motion. Clin Orthop Relat Res. 1990;253:113-117.
47 Osbahr DC, Cannon DL, Speer KP. Retroversion of the humerus in the throwing shoulder of college baseball pitchers. Am J Sports Med. 2002;30:347-353.
48 Fleisig G, Escamilla R, Andrews J, et al. Kinematic and kinetic comparison between baseball pitching and football passing. J Appl Biomech. 1996;12:207-224.
49 Barrentine SW, Fleisig GS, Whiteside JA, et al. Biomechanics of windmill softball pitching with implications about injury mechanisms at the shoulder and elbow. J Orthop Sports Phys Ther. 1998;28:405-415.
50 Herrington L. Glenohumeral joint: Internal and external rotation range of motion in javelin throwers. Br J Sports Med. 1998;32:226-228.
51 Morriss C, Bartlett R. Biomechanical factors critical for performance in the men’s javelin throw. Sports Med. 1996;21:438-446.
52 Melville T. Cricket (game). In Microsoft Encarta Online Encyclopedia. Redmond, Wash: Microsoft Corporation; 2006.
53 Bartlett RM, Stockill NP, Elliott BC, et al. The biomechanics of fast bowling in men’s cricket: A review. J Sports Sci. 1996;14:403-424.
54 Elliott BC. Back injuries and the fast bowler in cricket. J Sports Sci. 2000;18:983-991.
55 Crisp T, King JB. Cricket. In: Fu FH, Stone DA, editors. Sports Injuries: Mechanisms, Prevention, Treatment. Baltimore: Williams & Wilkins; 1994:283-290.
56 Cook DP, Strike SC. Throwing in cricket. J Sports Sci. 2000;18:965-973.
57 Toyoshima S, Hoshikawa T, Miyashita M, et al. Contribution of the body parts to throwing performance. In: Nelson RC, Morehouse CA, editors. Biomechanics IV. Baltimore: University Park Press; 1974:169-174.
58 Tullos HS, Erwin WD. Throwing mechanism in sports. Orthop Clin North Am. 1973;4:709-720.
59 Bayios IA, Anastasopoulou EM, Sioudris DS, et al. Relationship between isokinetic strength of the internal and external shoulder rotators and ball velocity in team handball. J Sports Med Phys Fitness. 2001;41:229-235.
60 Fleck SJ, Smith SL, Craib MW, et al. Upper extremity isokinetic torque and throwing velocity in team handball. J Appl Sports Sci Res. 1992;6:120-124.
61 Hill JA. Epidemiologic perspective on shoulder injuries. Clin Sports Med. 1983;2:241-246.
62 Elliott B, Fleisig G, Nicholls R, et al. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6:76-87.
63 Fleisig G, Nicholls R, Elliott B, et al. Kinematics used by world class tennis players to produce high-velocity serves. Sports Biomech. 2003;2:51-64.
64 Atwater AE. Biomechanics of overarm throwing movements and of throwing injuries. Exerc Sport Sci Rev. 1979;7:43-85.
65 Matsuo T, Matsumoto T, Takada Y, Mochizuki Y: Influence of different shoulder abduction angles during baseball pitching on throwing performance and joint kinetics. Presented at the 23rd annual meeting of the International Society of Biomechanics, 17th Congress, Calgary, Alberta, August 8-13, 1999.
66 Dillman CJ, Schultheis JM, Hintermeister RA, et al. What do we know about body mechanics involved in tennis skills. In: Krahl H, Pieper H, Kibler B, et al, editors. Tennis: Sports Medicine and Science. Düsseldorf: Germany, Society for Tennis Medicine and Science; 1995:6-11.
67 Chandler TJ, Kibler WB, Stracener EC, et al. Shoulder strength, power, and endurance in college tennis players. Am J Sports Med. 1992;20:455-458.
68 Welch CM, Banks SA, Cook FF, et al. Hitting a baseball: A biomechanical description. J Orthop Sports Phys Ther. 1995;22:193-201.
69 Philips BB, Andrews JR, Fleisig GS. Batter’s shoulder: Posterior instability of the lead shoulder, a biomechanical evaluation. Birmingham: Alabama Sports Medicine and Orthopaedic Center, 2000.
70 Mallon WJ. Golf. In: Hawkins RJ, Misamore GW, editors. Shoulder Injuries in the Athlete: Surgical Repair and Rehabilitation. New York: Churchill Livingstone; 1996:427-433.
71 Pink M, Jobe FW, Perry J. Electromyographic analysis of the shoulder during the golf swing. Am J Sports Med. 1990;18:137-140.
72 Hume PA, Keogh J, Reid D. The role of biomechanics in maximising distance and accuracy of golf shots. Sports Med. 2005;35:429-449.
73 Kim DH, Millett PJ, Warner JJ, et al. Shoulder injuries in golf. Am J Sports Med. 2004;32:1324-1330.
74 Geisler PR. Golf. In: Shamus E, Shamus J, editors. Sports Injury Prevention and Rehabilitation. New York: McGraw-Hill; 2001:185-225.
75 Jobe FW, Moynes DR, Antonelli DJ. Rotator cuff function during a golf swing. Am J Sports Med. 1986;14:388-392.
76 Jobe FW, Pink MM. Shoulder pain in golf. Clin Sports Med. 1996;15:55-63.
77 Jobe FW, Jobe CM. Painful athletic injuries of the shoulder. Clin Orthop Relat Res. 1983;173:117-124.
78 Kennedy JC, Hawkins R, Krissoff WB. Orthopaedic manifestations of swimming. Am J Sports Med. 1978;6:309-322.
79 McMaster WC, Long SC, Caiozzo VJ. Shoulder torque changes in the swimming athlete. Am J Sports Med. 1992;20:323-327.
80 Kibler WB, Chandler TJ, Livingston BP, et al. Shoulder range of motion in elite tennis players. Effect of age and years of tournament play. Am J Sports Med. 1996;24:279-285.
81 Rupp S, Berninger K, Hopf T. Shoulder problems in high level swimmers’impingement, anterior instability, muscular imbalance? Int J Sports Med. 1995;16:557-562.