CHAPTER 57 Conditioning of the Shoulder Complex for Specific Sports
Function of the shoulder complex in the athlete, and more specifically the overhead athlete, requires synchrony of multiple neuromuscular components. The precise timing of shoulder neurodynamics, osteodynamics, and neuromuscular dynamics depends on function of the entire kinetic chain. In-depth understanding of how the shoulder complex functions in relation to the torso and lower extremities (kinetic chain) allows adequate conditioning in preparation for competitive sports or rehabilitation from injury.
The specific movements of the overhead athlete create numerous adaptations throughout the kinetic chain. Adaptation and compensation are the processes that athletes use to respond to many demands of their given sport. As clinicians and sports trainers we can aid in this adaptation through proper conditioning methods. Specific exercises to promote healthy adaptation are paramount to the success of any program.
Injury prevention is the primary objective of a properly applied conditioning program; performance enhancement and return from injury are secondary objectives. This chapter gives the practitioner a solid foundation for creating a program that fits the needs of each athlete.
KINETIC CHAIN CONCEPTS AND CONNECTIONS
An athlete’s body may be required to move or react in various ways to accomplish sport-specific movements. A perfectly executed movement is the result of several body parts working in synchrony. This synergy is accomplished by precise function of the neuromuscular system. The movement in the overhead athlete begins in the foot, is transferred through the torso, and ends with a force being applied by the hand. As clinicians and sports trainers we must understand how function in one part of the neuromuscular system can affect function in others. The function of the entire kinetic chain is paramount in injury prevention, performance enhancement, and return from injury. The sum of the whole may be more important than the individual components, although each individual component must be evaluated for proper function.
If a component of the kinetic chain is dysfunctional, then deficiencies must be identified and corrected. This can require specific soft tissue manipulation (flexibility, manual therapy) and activation of specific musculature (strengthening exercises). Isolation for activation of specific musculature should be accomplished before sports-specific movements for synchrony. If not, the neuromuscular system will find a means of compensation around the deficient components.
When looking at sport-specific motions, the range of motion, the speed of movement, the muscles activated, and how they are activated (concentrically, eccentrically, isometrically) all must be understood to create a proper conditioning program. Because all movements have an optimal biomechanical position, it is imperative to aim to achieve biomechanical efficiency, which eases stress on tissues and improves function. It is important to emphasize quality of effort and proper intensity to gain optimum results from exercises in any conditioning program.
ADAPTATION
All athletes develop physiologic adaptations to their given sports, some more drastically than others. Influences from daily living habits can also modify the way an athlete functions, for good or ill. Repetitive stresses, which are all too common in sports, can compromise tissues that are shortened or weakened from environmental influences. An in-depth understanding of interaction and adaptation from psychosocial, biochemical, and biomechanical demands allows proper program design.
Understanding the sport and the position-specific demand is critical to good program design. A feel for the tissue stresses that the athlete is being exposed to will help prevent overuse injuries. Misuse or abuse of tissue from sport-specific skill work may be helped or hindered by exercise regimens; therefore, the conditioning program must be carefully selected. The balancing act of loading the tissue to maximize the training response without overloading the adaptive potentials must be constantly monitored.
Selye’s1 specific adaptation to imposed demand (SAID) principle describes the changes that occur throughout the body in response to training or athletic demands. Wilk2 demonstrated that the baseball player has a specific adaptation about the throwing shoulder. As different researchers have tried to determine the exact cause of this adaptation,3-6 it has become apparent that each athlete adapts in a similar pattern depending on the sport and the position within the sport. Although similar patterns of adaptation do occur, each athlete responds in his or her own unique way. Evaluating each athlete allows a path to preventive exercise programs that have a more specific approach.
How much to incorporate in an attempt to prevent the adaptation process is an intriguing question. The adaptation might help the athlete to meet the demands of the game or prevent injury, and clinicians and sports trainers must carefully select their therapeutic interventions. A look specifically at the overhead throwing athlete shows adaptation occurring throughout the kinetic chain. Scapular, torso, and hip adaptations all appear to play roles in the athlete’s success from a performance and well-being standpoint. Because more distal adaptation can ultimately affect the shoulder or elbow, it is necessary to look at all aspects of the body. Promoting a healthy adaptation can require attention to exercise, flexibility, soft tissue therapy, recovery, and proper nutrition.
EVALUATION
The idea that connectivity exists between the shoulder and the rest of the kinetic chain requires a look at proper length-tension relationships. This in turn allows the best chance for optimal movement patterns. An evaluation of the entire body is imperative because it can identify and help correct any problems before implementing a conditioning program. A misguided program can actually promote dysfunction or necessitate new adaptation patterns, either of which could result in injury. The evaluation should take into account overall gross movement dysfunction, postural abnormalities, flexibility, bilateral symmetry, and muscle and joint function. This evaluation should give the practitioner a reasonable picture of an athlete’s current state of function and direction for program design.
It is very common for athletes to develop muscle imbalances that are often overlooked until the athlete has an injury. A thorough evaluation of posture (static, dynamic), muscle tension, and functional movement will help identify abnormalities, which will allow a corrective exercise strategy that can offset any associated muscle imbalances. The corrective exercise program should strive to obtain optimal posture and alignment, which will lead to functional efficiency.
Optimal posture can be viewed as alignment of each component of the kinetic chain. This alignment allows optimal length-tension relationships and force couples from the myofascial components. Adequate joint kinematics will also be optimized. Optimal static posture (viewed in the coronal plane) should reveal a line of gravity passing from the earlobe through the glenohumeral joint and the greater trochanter of the hip and finishing just anterior to the lateral malleolus of the ankle. Dynamic posture is the ability to maintain optimal force couples and length-tension relationships regardless of body position.
In the presence of poor posture, dysfunctional muscle patterns can develop. These dysfunctions may be responses to overuse, misuse, abuse, or disuse.7 A normal response of muscle to any stress is to increase tightness. A chain reaction then occurs whereby the stressed muscles tighten and their antagonists weaken, which creates altered movement patterns.8 Many times these chain reactions create predictable patterns of dysfunction. Vladimir Janda has described them as upper and lower crossed syndromes. These syndromes can have detrimental effects on the shoulder of any athlete.
Sherrington’s law of reciprocal innervation indicates that tight muscles act in an inhibitory fashion to their antagonists.9 Therefore, it is prudent to stretch the tightened muscles before strengthening the weakened muscles.
It is important to evaluate all athletes for postural abnormalities, proper length-tension relationships, and proper muscle-firing patterns. A program to correct flexibility deficits, activate neuromuscular isolation, and integrate exercises can then be developed for each athlete depending on the athlete’s individual needs.
PROGRAM COMPONENTS
To design a specific program for conditioning the shoulder complex, several components must be developed. These components require different degrees of emphasis and specificity depending on the athlete and his or her adaptational patterns, evaluation results, demands of the sport, and goals of the program (injury prevention, improved performance, rehabilitation). Each component depends on the others, on skill development, and on health status.
Strength
Strength is the ability of a muscle or group of muscles to generate muscular force under specific resistive conditions.10 Although there are many types of strength, this chapter only discusses strength in a general sense as it relates to conditioning the shoulder complex.
Some sports depend on strength more than others. Because developing power critically depends on maximal strength, most athletes need some type of strength training to help improve this quality. Strength development can increase the use of muscular motor units through increased intensity. Intensities must be carefully planned (periodized) to gain optimal training effects. Shoulder complex exercises many times use very small and specific musculature; therefore, using maximum strength training exercises might not be advantageous.
Power
Power can be explained as the ability to produce force in a short period of time, which is vital to most sport skills.11 Power is highly related to strength and more specifically at the higher levels of force. Power depends on the stretch-shortening cycle of muscular contraction. Power (plyometric) development can be done in a specific component that is developed in conjunction with the other components or simply intertwined into the strength development component.
The ability to maintain power output is critical to sport success and represents a portion of one’s work capacity. The combination of strength, speed, and endurance yields the most productive use of power. To create an effective power-plyometric program, the exercises should exhibit patterns of movement, speed, and frequency similar to the actual sport movement. These exercises help make the neuromuscular system more efficient at storing and releasing energy. In essence, plyometric training improves the relation between maximum strength and power. The exercises also improve the ability of the tissues to tolerate the higher forces that are common in sports. Many times, less is more with this component of training. An adequate strength base is essential before initiating plyometric exercises.
Endurance (Work Capacity)
This component may be defined as the capacity to resist fatigue. This may be a cumulative process from one repetition to another, from exercise to exercise, or from day to day. The ability to recover and allow more work of higher quality is the goal. Obviously, recovery is a critical variable in this process. Understanding the requirements of the sport and the position of the athlete within the sport determines the importance of training for endurance and more specifically what type of endurance. It is the opinion of many strength and conditioning professionals that endurance work for an anaerobic athlete must be carefully selected because it can prevent the conversion of transitional or intermediate muscle fiber to red endurance fibers.12 Hence, if improved aerobic endurance damages the athlete’s power, then volume and intensity might need to be manipulated. Therefore, when designing a program, make sure it fits the athlete’s needs.
Flexibility and Mobility
This component can be seen as the extensibility of all connective tissues that allow joint range of motion while still maintaining joint integrity. Mobility can refer to the extensibility of a group of muscles and joints rather than a single muscle or joint.
The goal of flexibility training is to correct specific muscle tightness that can inhibit optimum neuromuscular function and to improve extensibility of specific soft tissues.13 A thorough evaluation will help determine specifically which myofascial or neural components need improved flexibility. This will minimize the chance of a hit or miss approach by a general overall body flexibility program. Optimum performance and injury prevention depend on proper length-tension relationships of muscles, and therefore the flexibility and mobility component must address any deficiencies.
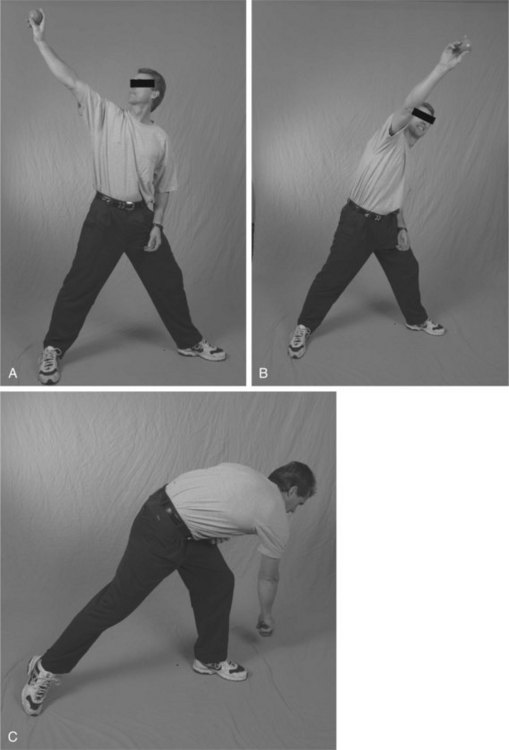
Flexibility and mobility can be achieved by many different methods such as static stretching, myofascial release, muscle energy techniques, proprioceptive neuromuscular facilitation (PNF) stretching, dynamic stretching, and functional movement stretching. A thorough understanding of each type of stretching allows the trainer to integrate the proper method into the overall conditioning program.
Athletes are master compensators. They devise compensation patterns, muscle imbalances, and postural abnormalities that can in turn create joint dysfunction and decreased neuromuscular control. A properly designed flexibility and mobility program can be the determining factor in the health or illness of the athlete.
Stabilization and Neuromuscular Control
It is our view that stabilization is fundamental to injury prevention and proper neuromuscular function. Stabilization is the ability of the neuromuscular system to allow agonists, antagonists, synergists, stabilizers, and neutralizers to work synergistically.
Core stabilization allows proximal stability, which in turn allows a stable fulcrum for efficient extremity motion. It also provides force reduction capabilities and hence injury prevention.
The shoulder girdle has very little static or ligamentous stability. Therefore, the stability required is dynamic and requires specific synergism of all neuromuscular components. It is essential to understand the difference between muscles that provide power for shoulder motion (deltoid, latissimus dorsi, and pectoral muscles) and those that provide shoulder stability (subscapularis, infraspinatus, teres minor, and supraspinatus).14 Stabilization of the shoulder complex is critical to the overall conditioning program. When reactivity is added to the stabilization exercises, the shoulder complex becomes more adept at handling the forces that sporting activities cause. Improved stabilization, neuromuscular control, and reactivity enhance performance and prevent injury.
Coordination or Skill Movements
Coordination or skill movements show how well neuromuscular firing patterns are working. It also shows motor unit recruitment for producing force and for timing of movement qualities. In essence, a specific movement with a specific force with the proper timing is the byproduct of properly executed skill movements. It is neuromuscular control and proprioception that allow these movements to happen efficiently. It is very important to improve all physical conditioning components of the shoulder complex, but ultimately it is the skill movements that are required for success. Skill movements should be classified as exercise in themselves; for example, a throwing or hitting program designed by the skills coach must be considered an exercise. Skill movements are normally practiced repetitiously for maximum biomechanical efficiency. With this in mind, the skills coach is vital to the success of any athlete. A properly designed conditioning program must take into account the volume, frequency, and intensity of skills training and implement the conditioning program around these variables for best results.
Recovery
The most overlooked area of training is recovery. As in any sport, it is not the amount of work the athlete does that determines good health and improved performance, instead it is the recovery that takes place between bouts of exercise and between athletic competitions. The process of recovery, or more specifically regeneration, is a complex biologic reaction influenced by both external and internal environments. Unfortunately, at present there is a greater emphasis on stressing the body than on recovery. There are many methods that can be used to promote recovery. Proper nutrition and hydration, hot and cold hydrotherapies, sports massage, relaxation techniques, and rest and sleep can be used to aid an athlete’s recovery.15 Lymphatic drainage techniques may also be beneficial. Planning recovery is a critical component to maximizing the overall conditioning effect.
GUIDELINES FOR SPECIFIC EXERCISES
Several basic guidelines should be followed when designing an exercise program for the shoulder complex.
Selection
Age
In our opinion, it is important for the prepubescent athlete to be able to control body weight before performing a resistance program involving weights. The neuromuscular control that is required to perform push-ups, press-ups, pull-ups, body squats, lunges, and lateral lunges needs to be developed. This allows the adolescent the opportunity to develop intramuscular coordination that may be overlooked if the training only consists of traditional stabilized weight training that occurs when using benches and machines. Another aspect of age is the effect of overtraining on bone growth plates. Any exercise or sports participation that causes abnormal responses from the epiphysis or apophysis of bone should be discontinued until the symptoms resolve, and return to that activity should be gradual.
Evaluation of Range of Motion
An exercise program should strive to increase the desired response from the targeted muscle group. Before embarking on a designed program, an evaluation to assess posture, scapulothoracic motion, scapulohumeral motion, and muscular strength should be performed by a trained professional. For example, in annual physicals in professional baseball before spring training, each player is evaluated by an orthopedic physician, deficits in strength and range of motion are brought to the attention of the athletic training and strength and conditioning staffs, and individual programs are established for players who have specific needs.
Previous Injuries and Surgeries
An athlete who is returning from a recent injury or surgery must be cleared to participate by the team physician. Any deficits must be corrected before the player embarks on more sport-specific activity. Two common shoulder adaptations that are encountered in the throwing athlete are changes in glenohumeral internal rotation (measured with the scapula stabilized) and weakness or deficits in the rotator cuff. When a decrease in internal rotation is accompanied by a decrease in the total range of motion of the glenohumeral joint it would be advantageous to stretch the involved extremity. Isokinetic testing devices are helpful in providing objective numbers that can be used to motivate an athlete to improve strength deficits. Completion of a properly designed physical therapy program (isotonic through plyometric exercises) should also be completed before beginning a throwing progression.
Training Age
Before a program is designed for an athlete, the athlete’s athletic history and level of training should be determined. Proficiency in tasks (body control exercises) should be determined and a functional screening (posture and functional strength) should be carried out to address any potential weaknesses.
Exercise Selection
The goal of any exercise program should be to increase performance and reduce the probability of injury. An understanding of risk versus reward should be considered when evaluating any exercise. In our experience, athletes are exposed to many training philosophies and might have performed exercises in their training routines that can be considered risk-versus-reward exercises. Over the course of a long career, the cumulative effects of repetitive motion (overhand throwing of an implement or ball) and the added effects of some exercises can place undue stress on the joints and soft tissue. In our opinion, certain exercises can have undesirable effects.
Knee Extension.
The patellofemoral joint is subjected to very high forces when performing open-chain knee-extension exercises. In addition, training the quadriceps with knee extension eliminates recruitment of other muscle groups that occurs in athletic activity.
Military Press.
The act of overhead pressing can decrease the amount of space in the subacromial area. A throwing athlete might already have some chronic changes in the subacromial space. Adding the stress of the overhead press can cause further irritation.
Bench Press.
Performing the bench press with a bar (as opposed to using dumbbells) places the arms in essentially the same working plane, which can cause some acromioclavicular joint stress with time. Using dumbbells, an athlete can vary the angles at which the exercise is performed, and the arms work as individual units. It is also recommended that the athlete not lower the upper arms below the level of the trunk to place less stress on the anterior shoulder capsule and ligaments, preserving the static stabilizers of the anterior shoulder.
Latissimus Pull-downs.
Performing the latissimus pulldown exercise by pulling the bar behind the head can place the anterior structures of the glenohumeral joint in a stretched position at 90 degrees of flexion and 90 degrees of abduction. Performing the exercise with the bar in front of the head trains the targeted muscle groups with less anterior stresses.
Olympic Lift.
Olympic lifts can place a significant demand on the glenohumeral, elbow, and wrist joints. The technical demands of these lifts require extensive coaching and supervision. The potential for incorrect mechanics, combined with heavy loads, necessitates a decision regarding the benefits of the exercises.
Design of an Exercise Program
Periodized training is the gradual cycling (allocation of a specific period of time, whether days, weeks, or months) of specificity, intensity, and volume of training to achieve peak levels of fitness for the most important competitions.16 Before beginning a periodized program it is important to look at two factors: the athlete’s training experience and body mechanics and the specific demands of the sport.
Training needs for an athlete are different from the training needs for a person who is training for aesthetics (bodybuilding) or Olympic lifting. Aesthetic lifters train body parts in stabilized environments to exhaustion to stimulate growth. Olympic lifters train to perform specific one-repetition maximum lifts for competition. The goal for an athlete needs to be specific to the demands of the sport. Athletes should strive to stimulate not only the prime movers or agonists but also the antagonists, synergists, stabilizers, and neutralizers by performing exercises that stimulate the nervous system to fire stabilizing muscle groups. Anecdotal evidence of the inability of exercises to protect athletes from injuries are numerous. Hamstring curls are not the panacea for hamstring injuries, four-way hip machines do not prevent groin strains, and the list can go on and on. An athlete training for a sport needs a good base of general strength and also needs sportspecific training to ensure training the body for the desired response.
Periodization
The training cycle is divided into mesocycles.16 These cycles revolve around the dates that the athlete wants to be at his or her peak, such as major competition dates. The training cycle as a whole, generally 1 year, is a macrocycle. The mesocycles are the preparatory period and the competitive period. The preparatory period (the off-season or noncompetition season) includes the hypertrophy phase, the strength phase, and the power phase.
Preparatory Period.
The hypertrophy phase lasts from 1 to 6 weeks. It begins at a low intensity (weights, running intensity) and a high volume (repetitions per set). This allows the muscles and soft tissues to adapt to the stresses of training that will be increased in the next phase. The exercises can be general or can be specific to the sport. Continued work to improve deficits addressed in the corrective exercises phase can be beneficial (Table 57-1).
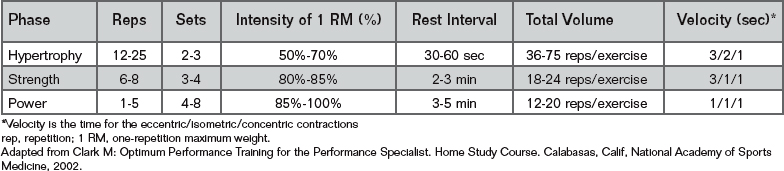
In the strength phase, running progresses to interval sprints at moderate distances, weight training becomes more specific, and intensity level increases. Loads of more than 80% of the athlete’s one-repetition maximum (1 RM) are used, and the volume is reduced from the hypertrophy phase (see Table 57-1).
In the power phase, loads increase to more than 90% of 1 RM and running speedwork is at a near-contest pace. Plyometric exercises can be implemented to take advantage of increased strength gains made in the strength phase. Plyometrics uses the stretch reflex and the accompanying stretch-shortening cycle to elicit more powerful concentric contractions. This type of training includes bounding, hopping, jumping, and throwing. Plyometric training requires sufficient recovery and should be used 1 to 3 days per week for 15- to 20-minute sessions (see Table 57-1)
Competitive Period.
The competitive period is often preceded by a transition period, at which time the athlete usually performs all activities at a low level of intensity and volume. This allows some physical recuperation before competition. The competition period is characterized by very high intensity and low volume training, in essence a maintenance of strength and power, with a minimum of energy expended in the weight room. Periodization or cycling is more complex when the competitive season is long, as in professional sports, or when there are two or more competitive seasons, as in college baseball, which has fall, spring, and summer competitions.
Corrective Exercises
Before starting a comprehensive periodized conditioning program, it might be beneficial to correct any postural deficits in the athlete. When attempting to correct what may be seen as a structural abnormality, remember that the neuromuscular system is an unknown variable. The neuromuscular system can adapt significantly to limit dysfunction.17
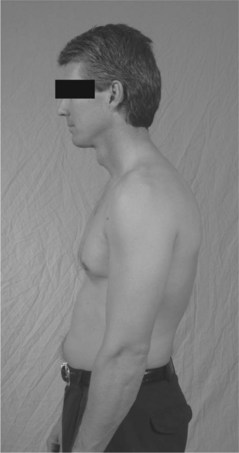
A common postural fault is what is commonly known as upper cross syndrome,8 which is characterized by rounded shoulders (protracted scapula) and a forward head. Lower cross syndrome is characterized by lumbar lordosis and an anterior pelvic tilt. Contributing factors are a group of muscles that are prone to be tight and a group of muscles prone to be weak and inhibited (Fig. 57-1 and Box 57-1). If these postural deficits are not addressed then some common injury patterns, such as rotator cuff impingement and thoracic outlet syndrome can emerge. Some corrective strategies for these syndromes are shown in Box 57-2:
Another postural fault is pronation syndrome, in which subtalar pronation can lead to tibial internal rotation, knee flexion, and femoral internal rotation. Because the tibia does not sufficiently externally rotate during knee extension (with excessive subtalar pronation), the femur must accommodate by internal rotation. Correction of foot biomechanics can greatly enhance the proper function of the kinetic chain.
Injury Prevention, Performance, and Rehabilitation
Factors include work, rest, and weight work. Training sessions should not exceed 90 minutes.18 The number of training sessions per week is influenced by training goals, training age, general health, work capacity, nutritional status, recoverability, lifestyle, and other stressors. Other factors to consider are mechanics (poor vs. perfect), work load (learning a new skill, such as pitches, arm angle) and rehabilitation. It is important not to move too quickly through the rehabilitation process for throwing athletes. The athlete may begin a strengthening program when cleared to do so by the physician.
Resistance and Endurance
Working with the scapular muscle groups is extremely important during the rehabilitation process. Endurance is trained by strengthening using isometric exercises with a 5- to 6-second hold for 10 repetitions using fatigue as a guideline. These exercises are performed for forward flexion, abduction, extension, internal rotation, and external rotation below the level of discomfort (Box 57-3).
If the throwing athlete is allowed in an aquatic environment (no risk of infection), performing isotonic exercises in chest-deep water eliminates the weight of the arm. Exercising in chest-deep water allows the athlete to begin forward flexion, scapular plane, empty can and full can, abduction, and extension exercises. The athlete can also perform range-of-motion exercises such as writing the alphabet and using PNF patterns. The speed of the exercise or the addition of aquatic dumbbells can increase the amount of resistance (Box 57-4).
Note: Use time instead of number of repetitions.
ER, external rotation; GH, glenohumeral; IR, internal rotation; PNF, proprioceptive neuromuscular facilitation.
Isotonic exercises with dumbbells can be initiated when the athlete is able to perform the exercises with proper form and without substituting synergistic muscles (Box 57-5). We have found it useful to start with the weight of the arm for 1 set of 30 repetitions to develop endurance. Once all the exercises can be completed for 30 consecutive repetitions, then 1 pound is added and the athlete is required to complete 30 consecutive repetitions for all exercises before increasing by 1 pound. We have found that using this method, the athlete is less likely to increase resistance than when doing 3 sets of 10 to 15 repetitions. Performing each exercise correctly with 5 pounds for 30 repetitions is a good indicator that the athlete is ready to move on to more sport-specific strengthening.





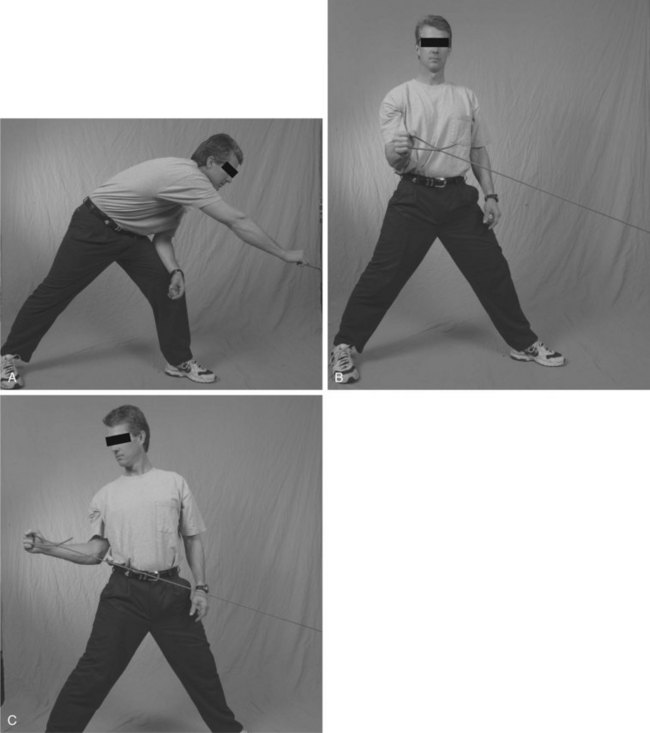
Neuromuscular Control and Stabilization Exercises
Neuromuscular control exercises allow the body to produce force and dynamically stabilize and reduce external forces, essentially to maintain balance during movement. Traditional machine-based strength training eliminates the need for neuromuscular control. The antagonists, stabilizers, and neutralizers are not called on to balance the movement produced by the prime movers (agonists and synergists). Machine-based training also generally exercises prime movers in only one plane instead of in the multiplane mode that sports activities are performed in.
Injuries cause altered sensory afferent feedback to the central nervous system. This alters neuromuscular control, which can lead to tissue overload and further injury.
Neuromuscular control training may be done in functional movement patterns and in a multisensory environment. Exercise progression should occur from slow to fast, from using one extremity to using both, from performing simple movements to performing complex ones, and from performing movements with eyes open to performing them with eyes closed.
Skill Development as an Exercise
One of the most critical components of success for a throwing athlete is performing the throwing motion as efficiently and stress free as possible. Proper mechanics decrease the probability of injury more than all other aspects of the conditioning program. The ability to repeat the correct mechanics is essential to successful overhead throwing. Evaluation by a skilled coach or biomechanist can help correct mechanical flaws that can predispose an athlete to injury. Throwing a baseball is an extremely fast motion, and the ability to watch for certain body positions at different points in the delivery is crucial.
Several skills are important to develop in the throwing athlete. The throwing athlete must develop the ability to balance over the back leg during the wind-up phase. Hand separation should take place at the same time as the lead leg begins moving toward the plate. The hand should be on top of the ball during the windup phase and the planted leg should be pointed toward home plate. The front arm (glove hand) must remain in front of the body during delivery. The elbow position of the throwing arm should remain above the shoulder. The whole body must be used during follow-through.
1 Selye H. The Stress of Life. New York: McGraw Hill, 1956.
2 Wilk KE: Rehabilitation guidelines for the thrower with internal impingement. Presented at the American Sports Medicine Institute Injuries in Baseball Course, January 23, 2004.
3 Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the gleno-humeral joint in professional baseball pitchers. Am J Sports Med. 2002;30(1):20-26.
4 Reagan KM, Meister K, Horodyski MB, et al. Humeral retroversion and its relationship to gleno-humeral rotation in the shoulder of college baseball players. Am J Sports Med. 2002;30(3):354-360.
5 Osbahr DC, Cannon DL, Speer KP. Retroversion of the humerus in the throwing shoulder of college baseball pitchers. The Am J Sports Med. 2002;30(3):347-353.
6 Borsa PA, Wilk KE, Jacobson JA, et al. Correlation of range of motion and glenohumeral translation in professional baseball pitchers. Am J Sports Med. 2005;33:1392-1399.
7 Chaitow L. Muscle energy techniques, 2nd ed. Edinburgh: Churchill Livingstone, 2001.
8 Janda V. Muscles central nervous regulation and back problems. In: Korr I, editor. Neurobiological mechanisms in manipulative therapy. New York: Plenum Press, 1978.
9 Chaitow L, Delany JW. Clinical Application of Neuromuscular Techniques, vol 1: The Upper Body. Edinburgh: Churchill Livingstone, 2001.
10 Siff MC. Supertraining, 6th ed. Denver: Mel C Siff, 2004.
11 Kraemer WJ, Gomez AL. Establishing a solid-fitness base. In: Foran B, editor. High-Performance Sports Conditioning. Champaign, Ill: Human Kinetics, 2001.
12 Francis C. Training for Speed. Canberra: Canadian Faccioni Speed & Conditioning Consultants, 1997.
13 Jull G, Janda V. Muscles and motor control in low back pain: assessment and management. In: Twomey L, editor. Physical Therapy of the Low Back. New York: Churchill Livingstone, 1987.
14 Hammer WI. Functional Soft Tissue Examination and Treatment by Manual Methods: New Perspectives, 2nd ed. Gaithersburg, Md: Aspen Publishers, 1999.
15 Calder A. Recovery: Restoration and regeneration as essential components within training programs. Excel. 1990;6(3):15-19.
16 Baechle TR. Essentials of Strength Training and Conditioning. Champaign, Ill: Human Kinetics, 1994.
17 Brownstein B, Bonner S. Functional Movement in Orthopedic and Sports Physical Therapy. New York: Churchill Livingston, 1997.
18 Clark M. Optimum Performance Training for the Performance Specialist. In Home Study Course. Calabasas, Calif: National Academy of Sports Medicine; 2002.
Anderson JE. Grant’s Atlas of Anatomy, 8th ed. Baltimore: Williams & Wilkins, 1983.
Anderson MK, Hall SJ. Sports Injury Management. Baltimore: Williams & Wilkins, 1995.
Andrews JR, Harrelson GL, Wilk KE. Physical Rehabilitation of the Injured Athlete, 3rd ed. Philadelphia: WB Saunders, 2004.
Apostolopoulos N. Performance flexibility. In: Foran B, editor. High Performance Sports Conditioning. Champaign, Ill: Human Kinetics; 2001:49-61.
Bandy WD, Irion JM, Briggler M. The effect of static stretch and dynamic range of motion training on the flexibility of hamstring muscles. J Orthop Sports Phys Ther. 1998;27(4):295-300.
Barlow W. Anxiety and muscle tension pain. Br J Clin Pract. 1959;13(5):339-350.
Basmajian JV, DeLuca CJ. Muscles Alive, 5th ed. Baltimore: Williams & Wilkins, 1985.
Brotzman SB, Wilk KE. Clinical Orthopaedic Rehabilitation. Philadelphia: Mosby, 2003.
Chaitow L. Integrated neuromuscular inhibition technique. Br J Osteop. 1994;13:17-20.
Chaitow L, Delany JW. Clinical Application of Neuromuscular Techniques. The Lower Body, Vol 2. Edinburgh: Churchill Livingstone. 2002.
Chaitow L. Positional Release Techniques, 2nd ed. Edinburgh: Churchill Livingstone, 2002.
Chaitow L. Palpation and assessment skills, 2nd ed. Edinburgh: Churchill Livingstone, 2003.
Church JB, Wiggins MS, Moode FM, et al. Effect of warm-up and flexibility treatments on vertical jump performance. J Strength Cond Res. 2001;15(3):332-336.
Cramer JT, Housh TJ, Johnson GO, et al. Acute effects of static stretching on peak torque in women. J Strength Cond Res. 2001;18(2):236-241.
Ellenbecker TS. Restoring performance after injury. In: Foran B, editor. High Performance Sports Conditioning. Champaign, Ill: Human Kinetics; 2001:327-344.
Farfan HF. Biomechanics of the spine in sports. In: Watkins RG, editor. The Spine in Sports. St Louis: Mosby; 1996:13-20.
Frederick GA, Syzmanski DJ. Baseball (part I): Dynamic flexibility. Strength Cond J. 2001;23(1):21-30.
Fritz S, Grosenbach JM. Mosby’s Essential Sciences for Therapeutic Massage, 2nd ed. St Louis: Mosby, 2004.
Fritz S. Mosby’s Fundamentals of Therapeutic Massage, 2nd ed. St Louis: Mosby, 2000.
Gleim GW, McHugh MP. Flexibility and its effects on sports injury and performance. Sports Med. 1997;24(5):289-299.
Gracovetsky SA. The Spinal Engine. New York: Springer-Verlag, 1998.
Greenfield B, Catlin PA, Coats PW, et al. Posture in patients with shoulder overuse injuries and healthy individuals. J Orthop Sports Phys Ther. 1995;21(5):287-295.
Greenman P. Principles of Manual Medicine. Baltimore: Williams & Wilkins, 1991.
Hodges PW, Richardson CA, Jull G. Evaluation of the relationship between laboratory and clinical tests of transverse abdominus function. Physiother Res Int. 1996;1:30-40.
Janda V. Janda Compendium, 2 vols. Minneapolis: OPTP. 1997.
Jones LH, Kusunose R, Goering E. Jones strain-counterstrain. Boise, Idaho: Jones Strain-Counterstrain, Inc., 1995.
Kendall FP, McCreary EK. Muscle testing and function, 3rd ed. Baltimore: Williams & Wilkins, 1983.
Knudson DV, Noffal GJ, Bahamonde RE, et al. Stretching has no effect on tennis serve performance. J Strength Cond Res. 2004;18(3):654-656.
Korr I. Neurobiological mechanisms in manipulation. New York: Plenum Press, 1980.
Kurz T. Stretching Scientifically: A Guide to Flexibility Training, 4th rev ed. Island Pond, Vt: Stadion Publishing, 2003.
Lacote M, Chevalier AM, Miranda A, et al. Clinical Evaluation of Muscle Function. Edinburgh: Churchill Livingstone, 1987.
Lee D. The Pelvic Girdle, 2nd ed. Edinburgh: Churchill Livingstone, 1999.
Lewit K. Manipulative Therapy in Rehabilitation of the Motor System, 3rd ed. London: Butterworths, 1999.
Liebenson C. Muscular relaxation techniques. J Manip Physiol Ther. 1990;12(6):446-454.
Liebenson C. Active muscular relaxation techniques (Part 2). J Manip Physiol Ther. 1990;13(1):2-6.
Liebenson C, editor. Rehabilitation of the Spine. Baltimore: Williams & Wilkins, 1996.
Liebenson C. Sensory motor training. Journal of Bodywork and Movement Therapies. 2001;5(1):21-27.
Lukasiewiscz AC, McClure P, Michener L, et al. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29(10):574-586.
Magee D. Orthopedic Physical Assessment, 3rd ed. Philadelphia: WB Saunders, 1997.
Mangine B, Nuzzo G, Harrelson GL. Physiologic factors of rehabilitation. In: Andrews JR, Harrelson GL, Wilk KE, editors. Physical Rehabilitation of the Injured Athlete. 3rd ed. Philadelphia: WB Saunders; 2004:13-33.
McAtee RE. Facilitated Stretching. Champaign, Ill: Human Kinetics, 1993.
McGill S. Ultimate Back Fitness and Performance. Waterloo, Ont: Wabbuno Publishers, 2004.
McGill S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation. Champaign, Ill: Human Kinetics, 2002.
Merrick MA. Therapeutic modalities as an adjunct to rehabilitation. In: Andrews JR, Harrelson GL, Wilk KE, editors. Physical Rehabilitation of the Injured Athlete. 3rd ed. Philadelphia: WB Saunders; 2004:51-98.
Myers T. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists. Edinburgh: Churchill Livingstone, 2002.
Norris CM. Sports Injuries: Diagnosis and Management, 3rd ed. London: Butterworth-Heinemann, 2004.
Norris C. Back Stability. Champaign, Ill: Human Kinetics, 2000.
O’Sullivan PB, Twomey LT, Allison GT. Altered abdominal muscle recruitment in patients with chronic back pain following a specific exercise intervention. J Orthop Sports Phys Ther. 1998;27(2):114-124.
Porterfield JA, Derosa C. Mechanical Low Back Pain: Perspectives in Functional Anatomy, 2nd ed. Philadelphia: WB Saunders, 1998.
Richardson C, Jull G, Hodges P, Hides J. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain. Edinburgh: Churchill Livingstone, 1999.
Rothbart BA. Medial column foot systems: An innovative tool for improving posture. Journal of Bodywork and Movement Therapies. 2002;6(1):37-46.
Sahrmann SA. Diagnosis and treatment of movement impairment syndromes. Baltimore: Williams & Wilkins, 2002.
Shrier I. Stretching before exercise does not reduce the risk of local muscle injury: A critical review of the clinical and basic science literature. Clin J Sports Med. 1999;9(4):221-227.
Simons D, Travell J, Simons L. Myofascial Pain and Dysfunction: The Trigger Point Manual, vol 1: Upper Half of Body, 2nd ed. Baltimore: Williams & Wilkins, 1999.
Solem-Bertott E, Thuomas KA, Westerberg CE. The influence of scapular retraction and protraction on the width of the subacromial space: An MRI study. Clin Orthop Relat Res. 1993;296:99-103.
Thacker SB, Gilchrist J, Stroup DF, et al. The impact of stretching on sports injury risk: A systematic review of the literature. Med Sci Sports Exerc. 2004;36(3):371-378.
Thompson B. Ankle pain (chronic) with associated low back pain. In: Chaitow L, DeLany J, editors. Clinical Application of Neuromuscular Techniques: Practical Case Study Exercises. Edinburgh: Churchill Livingstone, 2005.
Travell J, Simons D. Myofascial Pain and Dysfunction: The Trigger Point Manual, vol 2: The Lower Extremities. Baltimore: Williams & Wilkins, 1993.
Warner JJ, Micheli LJ, Arslanian LE, et al. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement: A study using Moiré topographic anaylsis. Clin Orthop Relat Res. 1992;285:191-199.
Wenos DL, Konin JG. Controlled warm up intensity enhances hip range of motion. J Strength Cond Res. 2004;18(3):529-533.
Watkins RG, editor. The Spine in Sports. St Louis: Mosby, 1996.
Young WB, Behm DG. Should static stretching be used during a warm up for strength and power activities? Strength Cond J. 2002;24(6):33-37.