CHAPTER 55 Dropsical Conditions Affecting Pregnancy
Hydrallantois and hydramnios, hydrops of the allantois and the amnion, respectively, are the two most common causes of dropsy of the fetal membranes and fetus in cattle. Other, less common causes include edema of the chorioallantois, fetal anasarca, and fetal edema with ascites and hydrothorax.1 In the largest published retrospective study of hydrops to date, Vandeplassche and associates documented that of a total of 60 cases, hydroallantois accounted for 88%, 5% of the cases were hydramnios, and 7% involved both compartments.2
HYDRALLANTOIS
Hydrallantois is the single pathologic factor present in 85% to 90% of dropsical conditions in the bovine.1,2 Placental dysfunction is thought to be the cause of hydrallantois, although this condition is observed with both uterine and placental disease. Adventitious placentation commonly is present (Fig. 55-1), and the number of caruncles also may be deficient. This deficiency may be due to a congenital lack of development or to uterine disease acquired later in life. A reduction in the number of caruncles also has been noted with hydrallantois, and those that are present tend to be hypertrophied.3 The condition is seen sporadically in both dairy and beef cows, and dams carrying multiple fetuses are at greater risk for hydrallantois. An increased prevalence of hydrallantois has been noted in recipient cattle carrying fetuses produced by in vitro fertilization and by transgenic and cloning technologies.4,5
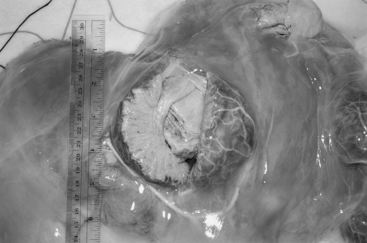
Fig. 55-1 Abnormal cotyledon from the placenta of a cow with hydrallantois (8 months of gestation). The cotyledon, measuring 5 inches in diameter, has been sectioned; note the excessive edema within the intercotyledonary placenta.
The structural and functional changes in the chorioallantois that lead to hydrallantois result in the excessive production of a transudative fluid that resembles plasma.1 In severe hydrallantois, the accumulated fluid volume may reach 150 to 250 L, and the combined weight of the dropsical fluids, membranes, and fetus can exceed 225 kg.3 Fluid composition studies comparing allantoic fluid from normal cows in late gestation and from those suffering from hydrallantois have demonstrated marked differences in sodium, potassium, chloride, and creatinine levels.2,6,7 In hydrallantois, the levels of these electrolytes are much higher, more closely resembling plasma levels.8 In addition, lower peripheral plasma concentrations of estradiol have been observed in cows suffering from hydrallantois.7 The exact role of estrogen deficiency in the maintenance of fetal membrane permeability and its effect on allantoic and amniotic fluid volume in the cow remains uncertain. Studies in pigs and ovariectomized sheep, however, point to a link between the estrogen-to-progesterone ratio and fetal fluid volume.8,9
The clinical signs associated with hydrallantois vary with the volume of fluid at presentation. Abdominal distention rarely has been noted as early as the fifth month of gestation.3 The typical case of hydrallantois, however, is characterized by a larger than normal accumulation of allantoic fluid during a 5- to 20-day period in the last trimester of pregnancy3 (Fig. 55-2). Mild cases may remain undiagnosed or may be suspected only at parturition when an abnormally large volume of fetal fluids is expelled. In such instances, the producer may have assumed that the dam was carrying twins. In the more severe cases, progressive abdominal distention during the last 4 to 6 weeks of pregnancy worsens to such an extent as to decrease appetite and cause difficulty moving or rising.10 Progressive maternal tachycardia, anxiety, reduced appetite, and dehydration should be anticipated with untreated hydrallantois. Recumbency and metabolic problems, particularly ketosis, are therefore potential complications associated with advanced cases of hydrallantois, and these will be even more likely should the condition be associated with multiple fetuses. The combined weight of the fetus(es) and allantoic fluid also may result in either prepubic tendon rupture or secondary ventral abdominal muscle herniation.
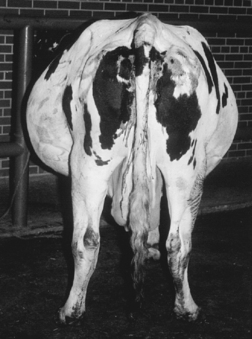
Fig. 55-2 Severe bilateral abdominal distention secondary to hydrallantois is evident when this adult Holstein cow is viewed from the rear.
(Courtesy of Dr. W. C. Rebhun.)
A definitive diagnosis of hydrallantois can be obtained by rectal palpation. The external appearance of the cow may suggest the presence of vagal indigestion, but rectal palpation will quickly distinguish between the two conditions. In hydrallantois, the abdominal cavity will be dominated by the fluid-filled uterus, frequently precluding palpation of other structures, whereas vagal indigestion will be characterized by a prominent, enlarged L- or V-shaped rumen. The fetus and placentomes usually are not palpable in cases of hydrallantois, and it is therefore difficult to ascertain the viability of the fetus without fetal heart rate measurement. Evaluation of fetal number and viability is best performed by transabdominal ultrasound examination with a 2.5- or 5-MHz sector scanner.
HYDRAMNIOS
Hydramnios causes approximately 10% of the cases of hydrops of the fetal membranes in cows.1 The condition is characterized by gradual accumulation of excessive amniotic fluid, with progressive abdominal enlargement in the dam during the last trimester of pregnancy. The abdominal distention typically is slower to develop than in hydrallantois.3 Hydrops of the amnion usually is the result of an abnormal fetus and is therefore considered a fetal problem, whereas hydrallantois is due to maternal abnormalities of placentation. From midgestation to term, amniotic fluid normally is swallowed or inhaled into the large bronchi of the fetus and subsequently absorbed.11 Hydramnios results from fetal abnormalities that prevent swallowing or intestinal transport of amniotic fluids.1 During late gestation, the volume of normal amniotic fluid reaches between 3.8 and 7.6 L; however, in hydramnios, the volume will increase to 19 to 114 L. The fluid is viscous and syrupy in consistency.1
Hydramnios can be associated with both genetic and nongenetic fetal abnormalities. Certain fetal anomalies inherited as autosomal recessive traits have been associated with hydramnios in specific breeds of cattle:
The nongenetic causes of hydramnios in cattle include those anomalies that impair the ability of the fetus to swallow amniotic fluid, such as schistosomus reflexus. Hydramnios also has been reported in hybrid crosses between American bison and domestic cattle.11
TREATMENT OF HYDRALLANTOIS AND HYDRAMNIOS
The decision whether to treat a cow suffering from hydrallantois or hydramnios should always be tempered by practical considerations regarding the likelihood of success and the etiology of the specific condition. Salvaging the cow for slaughter should be considered in all cases of hydrops in the cow.1,3,11 The cause of hydrallantois is uterine or placental disease, or both, so the likelihood of recurrence should be considered.3 In cases of hydramnios, an inherited etiology should be considered and the fact that the fetus most likely will be anomalous should be borne in mind. If the fetal anomaly is due to an established autosomal recessive disorder, both the dam and the sire will be carriers.1,3
The severity of the condition at presentation also should play an important role in decision making. In severe cases of hydrallantois in which the patient is already recumbent and unable to rise, or prepubic tendon or abdominal wall rupture has already occurred, the prognosis becomes increasingly grave, and immediate slaughter should be considered. In dairy cattle, because individual animals are in negative energy balance and often within the last trimester at the time of diagnosis, they may never obtain projected production levels despite successful termination of a pathologic pregnancy. For the aforementioned reasons, salvage usually is considered unless the cow or the fetus is particularly valuable and the pregnancy is within 2 to 3 weeks of term.10
If the decision is made to treat the condition, several options exist. Most clinicians agree that elective cesarean section is rarely as successful as induced parturition.3,10,11 Uterine atony due to overdistention, retained fetal membranes, and severe metritis are complications that should always be anticipated after either induced parturition or elective surgery. Debate exists among different authors about whether hydrops patients are markedly dehydrated or not; some sources support the hypothesis,1,10 whereas others refute it.11 The induction of parturition, however, will result in a slower release of uterine fluids than the rapid decompression that occurs after surgery. The rapid release of up to 250 L of allantoic fluid would certainly seem to predispose the patient to hypovolemic shock subsequent to compartmental shifting into the splanchnic pool.11 Some clinicians advocate the use of a trocar or plastic tube inserted percutaneously through the abdominal and uterine walls to draw off fluid gradually during a 24-hour period before elective cesarean.6 This procedure will predispose the cow to the development of peritonitis and/or metritis, however, and whether this maneuver actually allows a significant volume of fluid to drain is uncertain.3 Drainage also can be attempted transcervically if the cervix is relaxed enough to permit passage of a suitable catheter. In cases of hydrallantois treated by cesarean section, some authors have observed that the uterus may continue to fill with a significant volume of transudative fluid for up to 48 hours after surgery.1
To induce either abortion or calving, 25 to 35 mg of prostaglandin F2α can be injected intramuscularly either alone or in combination with dexamethasone.3 An alternative regimen involves the administration of 10 to 20 mg of flumethasone intramuscularly. Some clinicians advocate the use of 6 to 8 mg of estradiol cypionate intramuscularly once daily until parturition to relax the cervix and caudal reproductive tract. The combination of a prostaglandin and an abortifacient steroid reliably induces parturition in late gestation in a normal cow within 24 to 48 hours, but the response can be rather more unpredictable in cases of hydrops.
After induction of parturition, the cow should be carefully monitored and regularly examined for signs of labor. Periodic vaginal examination is important to ascertain the progress of cervical dilation and to rupture the fetal membranes as soon as possible.3 Once the fetus can be palpated per vagina, it should be assessed for size, position, and the presence of any anomalies that may hinder vaginal delivery. In many cases of hydrallantois, parturition may not progress beyond this point as a result of uterine atony, and assistance will be required to complete delivery.
After induction, the cow should be kept in a deeply bedded stall with good footing, to limit the chances of catastrophic musculoskeletal injury associated with parturition. If dehydration is suspected or if the cow has evidence of other metabolic complications (ketosis, hypocalcemia), then supportive polyionic intravenous fluids augmented with dextrose and calcium are indicated. In a field situation, acute hypovolemic shock can be addressed with smaller volumes of hypertonic saline (2–3 L of 7% sodium chloride given intravenously, followed by access to water and electrolyte solutions). In dairy cows, milking should be initiated as soon as the calf is delivered, although it often can be challenging to achieve projected production levels in cows that have experienced a dropsical pregnancy. A majority of fetuses will be small, nonviable, or anomalous, but in the rare case of an apparently viable calf, colostrum must be provided from an alternative source, because the dam rarely has normal colostrum. With exceptionally valuable calves it is wise to consider plasma administration, because colostrum absorption may be compromised by precocious gut closure induced by chronic in utero swallowing of excessive fetal fluid.
The prognosis for individual animals suffering from hydrallantois, particularly if the condition is advanced at the time of diagnosis, is much poorer for life and future fertility than is the case with hydramnios. Retained fetal membranes and potentially severe metritis should be anticipated with both conditions, but especially with hydrallantois, particularly if parturition is induced or the cervix is still significantly closed at the time of elective cesarean section. Prophylactic antibiotics should be instituted if the cow is not being sold for slaughter.
OTHER DROPSICAL CONDITIONS OF CATTLE
Dropsical conditions other than hydrallantois and hydramnios are very rare but include the following:
In all of these conditions, with the possible exception of edema of the chorioallantois, abdominal enlargement usually is not noted.1
1 Roberts SJ. Disease and accidents of gestation. In Veterinary obstetrics and genital diseases, 3rd ed., Woodstock, VT: published by the author; 1986:223.
2 Vandeplassche M, Oyaert W, Bouters R, et al. Uber die Einhautwassersucht beim Rind. Wiener Tieraztl Monatsschr. 1965;5:461.
3 Elmore R, Morris D, Brinsko S, et al. Bovine hydrallantois and hydramnios. In: Theriogenology Handbook. Hastings, NE: Society for Theriogenology; 1988:B-2.
4 Hill JR, Roussel AJ, Cibelli JB, et al. Clinical and pathologic features of cloned transgenic calves and fetuses (13 case studies). Theriogenology. 1999;51:1451.
5 Van Wagtendonk-de Leeuw AM, Aerts BJ, den Daas JH. Abnormal offspring following in vitro production of bovine preimplantation embryos: a field study. Theriogenology. 1998;49:883.
6 Skydsgaard JM. The pathogenesis of hydrallantois bovis. Acta Vet Scand. 1965;6:193.
7 Spencer J, Cox J, Dobson H. Electrolytes and reproductive hormone concentrations in maternal plasma and fetal fluids of dairy cows with hydrops. Vet Rec. 1989;124:159.
8 Dalton D, Knight J. Effects of exogenous progesterone and estrone on conceptus development in swine. J Anim Sci. 1980;56:1354.
9 Alexander G, Williams D. Hormonal control of amniotic and allantoic fluid volume in ovariectomized sheep. J Endocrinol. 1968;41:477.
10 Rebhun WC. Reproductive disorders. In: Diseases of dairy cattle. Philadelphia: Lea & Febiger; 1995:323.
11 Elmore R. Focus on bovine reproductive disorders: managing cases of placental hydrops. Vet Med. 1992;87:73.
12 Donald H, Deas D, Wilson L. Genetic analysis of the incidence of dropsical calves in herds of Ayrshire cattle. Br Vet J. 1952;108:227.