Chapter 8
Sphenoidotomy
Alexander G. Chiu, and Jeremy Reed
Introduction
- ▪ There are two ways to approach and perform a sphenoidotomy: transnasal and transethmoid.
- ▪ In the transnasal approach, the sphenoidotomy is performed while sparing the ethmoid cavity. Dissection proceeds medial to the middle turbinate. Common indications for this approach are isolated pathologic processes within the sphenoid sinus (e.g., fungal ball, isolated sphenoid sinusitis). This approach may also be combined with a posterior septectomy for an endoscopic transnasal approach to the pituitary sella (see Chapter 28).
- ▪ In the transethmoid approach, the uncinate process and inferior ethmoid air cells are removed to access the anterior face of the sphenoid sinus. This technique may be used in cases of isolated sphenoid disease, but most commonly is performed as a component of a complete functional endoscopic sinus surgery.
Anatomy
Sphenoid
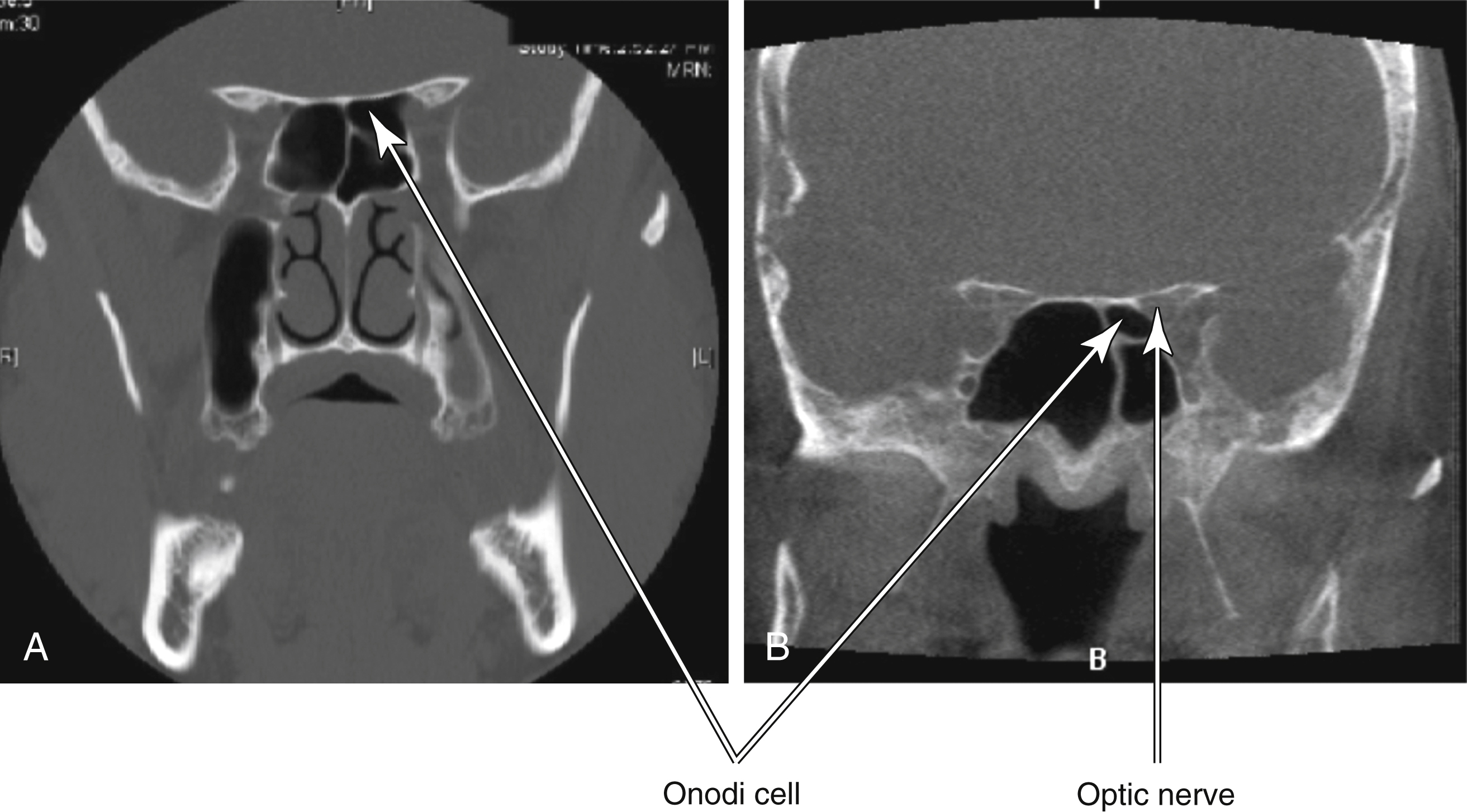
Onodi Cell
- ▪ An Onodi cell is a posterior ethmoid cell that lies superior or lateral to the sphenoid sinus.
- ▪ When a sphenoidotomy is performed, it is crucial not to confuse the posterior wall of an Onodi cell with the anterior face of the sphenoid.
- ▪ A common cause of optic nerve or orbital apex injury in the early days of functional endoscopic sinus surgery was dissection through the posterior wall of an Onodi cell because it was mistaken for the anterior face of the sphenoid sinus (Fig. 8.3).
Vasculature
Preoperative Considerations
- ▪ When a sphenoidotomy is performed, a greater palatine or sphenopalatine artery injection can be helpful in controlling intraoperative bleeding.
- ▪ A greater palatine artery injection is performed through the mouth. The greater palatine canal is in the hard palate, opposite the second molar. Bend the needle at 1.5 to 2 cm from the tip at a 45-degree angle, aspirate, and then inject 1 to 2 mL of 1% lidocaine with 1:100,000 epinephrine.
- ▪ A sphenopalatine artery injection can be performed transnasally. Identify the inferior attachment of the middle turbinate to the lateral nasal wall and inject roughly 1 mL of 1% lidocaine with 1:100,000 epinephrine 1 cm above the inferior border.

Radiographic Considerations
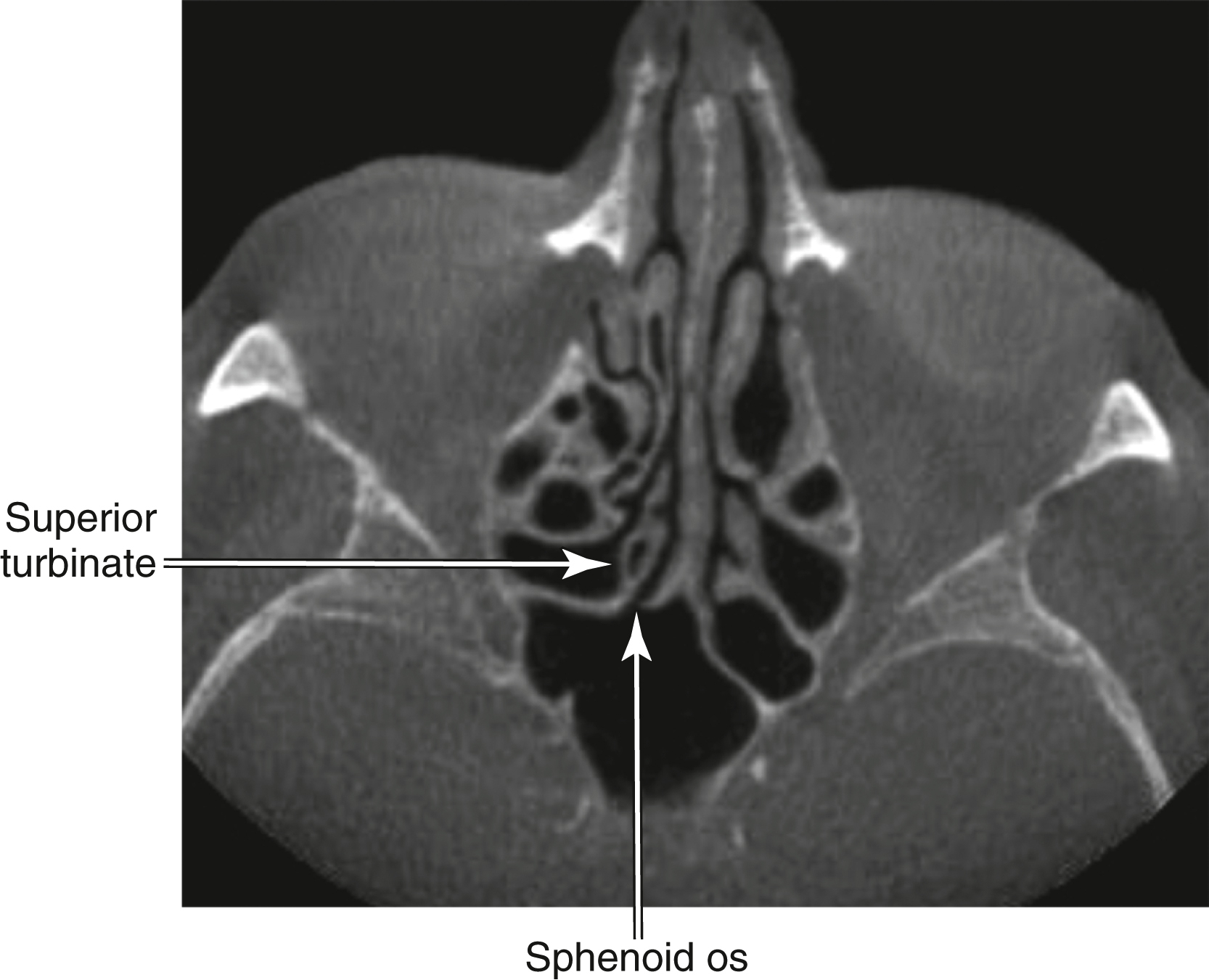
- ▪ The axial, coronal, and sagittal computed tomography (CT) scans are helpful to understand the anatomy.
- ▪ Identify the size and pneumatization of the sphenoid sinus.
- ▪ Look at the nature of the bone of the sphenoid walls. Fungal balls or long-standing inflammatory disease often results in thickened bone of the anterior face (sometimes requiring a drill for sphenoidotomy enlargement).
- ▪ Identify the presence of any Onodi cells.
- ▪ Identify the intersinus septum and track its path back to the posterior wall. Beware of any attachments to the internal carotid artery. If such an attachment is identified, it is advisable to avoid aggressive manipulation of the intersinus septum for fear of injuring the artery (Fig. 8.4).
Instrumentation
Pearls and Potential Pitfalls
- ▪ Avoid operating in a narrow space when entering the sphenoid. Visualization is significantly improved by removing superior ethmoid air cells, which allows greater access to light from the endoscope.
- ▪ A reliable method to identify the natural os of the sphenoid is to truncate the lower half of the superior turbinate. Avoid excising too much of the superior turbinate, because olfactory fibers are located in its most superior portion.
- ▪ Dissect from “known to unknown.” Identify the natural os first and then expand the antrostomy laterally.
- ▪ If image guidance is available, estimate the height of the septal branch of the sphenopalatine artery. This can be done by looking at the axial computed tomography (CT) sections and noting the location of the sphenopalatine foramen.
- ▪ Identify the presence of an Onodi cell preoperatively as well as intraoperatively. Mistaking the anterior surface of an Onodi cell for the sphenoid face can result in inadvertent injury to the orbital apex (Fig. 8.5).
- ▪ Avoid stripping mucosa off the skull base or medial orbital wall. This will often lead to prolonged localized postoperative mucosal edema and long-term neo-osteogenesis.

Surgical Procedures
Transnasal Sphenoidotomy
Step 1
- ▪ With a 0-degree endoscope, gently lateralize the middle turbinate to identify the lower half of the superior turbinate.
- ▪ Use a straight through-cutter to excise the lower half of the superior turbinate. This is done to identify the natural os of the sphenoid sinus (Fig. 8.6).
Step 2



Transethmoid Sphenoidotomy
Dilation of the Natural Os
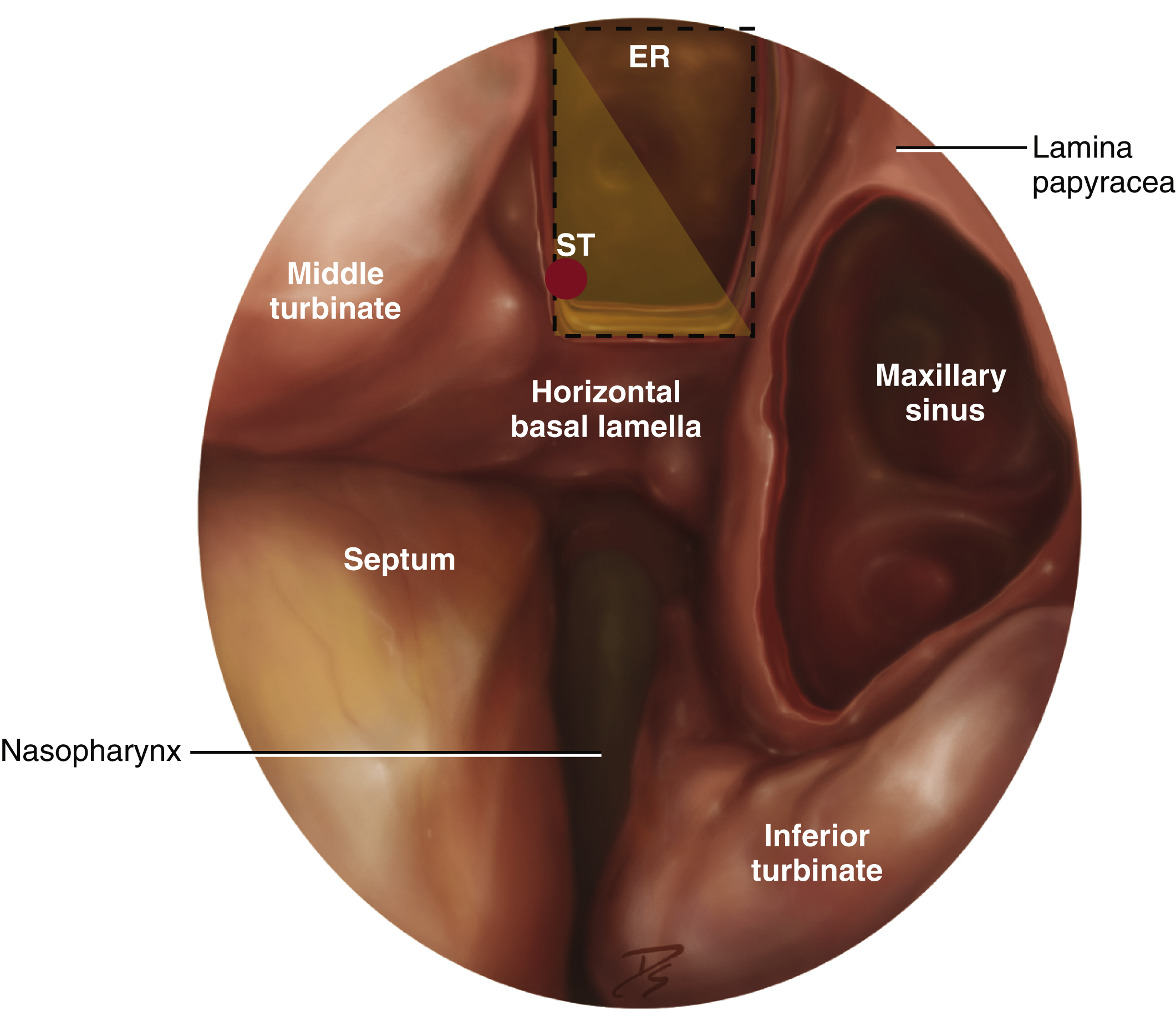
- ▪ After a posterior ethmoidectomy has been performed, identify the superior turbinate and its horizontal lamellae (Fig. 8.7).
- ▪ Remove the lower half of the superior turbinate to identify and then enlarge the natural os (Fig. 8.8). It is safest to find the os in its medial location and then, using a J-curette, fracture the anterior sphenoid face in a lateral direction.
- ▪ Enlarge the antrostomy by using an upbiting through-cutting instrument, Kerrison rongeur, or straight mushroom punch (Fig. 8.9).
- ▪ The final antrostomy is shown in Fig. 8.10.

Bolger Box Method
- ▪ The “Bolger box” method is a technique for performing a sphenoidotomy without finding or resecting the superior turbinate.
- ▪ Draw a rectangular box with the borders being the superior turbinate medially, superior turbinate lamellae inferiorly, skull base superiorly, and orbit laterally. Draw a diagonal line through the box and enter the sphenoid face medial and inferior to the line (Fig. 8.11).
Special Considerations—Onodi Cell
- ▪ An Onodi cell lies superior to the natural os of the sphenoid sinus. Continued dissection through the posterior wall of an Onodi cell results in intracranial or orbital apex injury.
- ▪ The floor of an Onodi cell may be removed to create one continuous sphenoid cavity (Fig. 8.12).