9
The Transthoracic Examination, View by View
Bernard E. Bulwer
Introduction
This chapter presents the views acquired during the normal two-dimensional (2D) adult comprehensive transthoracic echocardiography (TTE) examination. These views are based on the standards recommended by the American Society of Echocardiography (see Chapter 8).1 Optimal image acquisition is a prerequisite for optimal interpretation and reporting of the adult transthoracic echocardiogram by the echocardiographer/cardiologist expert. This involves competency in cardiac sonographer skills and training,2 as well as optimizing patient and instrument settings (see Chapter 11).
The comprehensive adult 2D TTE examination (TTE) begins at the left parasternal window, followed by the apical, subcostal, and suprasternal notch windows (Tables 9.1–9.6). Each standard echocardiographic view is described using three components (see Table 9.1; see also Chapter 8): (1) transducer position or window, namely the parasternal (P), apical (A), subcostal (SC), and suprasternal notch (SSN) windows; (2) echocardiographic imaging plane, namely long-axis (LAX), short-axis (SAX), or four-chamber (4C) planes; and (3) cardiac structures or regions of interest.
At each window, each echocardiographic view must be optimized and recorded. This includes video loops, still frames, and recommended pertinent measurement (Figs. 9.1–9.10 and corresponding  Videos 9.1–9.28).1–10 The typical sequence of the modalities employed are as follows:
Videos 9.1–9.28).1–10 The typical sequence of the modalities employed are as follows:
Videos 9.1–9.28).1–10 The typical sequence of the modalities employed are as follows:1. 2D examination for cross-sectional anatomy of the cardiac structures
2. M-mode examination for timing of cardiac events and linear measurements
3. Color flow Doppler examination for the initial visual assessment of normal and abnormal flows, and a guide to quantitative assessment of velocities using spectral Doppler
4. Spectral Doppler examination—namely continuous-wave (CW) Doppler to measure maximum transvalvular velocities and gradients, followed by pulsed-wave (PW) Doppler to detect flows at specific anatomical sites when indicated
5. Tissue Doppler imaging (TDI) to assess myocardial velocities
6. Three-dimensional (3D) echocardiography incorporated when available and as indicated (see Chapter 10)
Left Parasternal Views
The left parasternal window (P) or transducer position is where the adult TTE examination begins. Here a family of left parasternal long-axis (PLAX) and left parasternal short-axis (PSAX) views are acquired and assessed (see Tables 9.1 and 9.2; see also Figs. 9.1–9.4). All four cardiac chambers, the four cardiac valves, and the juxtacardiac portions of the great vessels are examined. Complementary views from the A, SC, and SSN windows are necessary for the comprehensive assessment of cardiac structure and function (see Figs. 9.5–9.10).
The PLAX view of the left ventricle (LV) inflow-outflow tract, or simply PLAX, is the starting point for the adult TTE echo exam (see Tables 9.1 and 9.2; see also Fig. 9.1). The PLAX view sets the stage for the assessment of several important parameters of global and regional cardiac structure and function. Important L-sided structures are optimally aligned and measured: LV walls and cavity, mitral and aortic valves (MV, AV). The initial assessment of right ventricle (RV) function and the pericardium also begins with the PLAX view.
The RV Inflow view is used to evaluate right ventricular inflow, from right atrium (RA) to RV via the tricuspid valve (TV; see Tables 9.1 and 9.2; see also Fig. 9.2). It can be used to assess the inferior two-thirds of RV, TV, RA, and the inferior vena cava (IVC) and coronary sinus as they empty into the RA. This view is useful for the evaluation of right heart pressures, specifically the RV systolic (RVSP) and pulmonary artery systolic (PASP) pressures. The RV outflow view is often used to examine the RV outflow tract (RVOT), pulmonary valve (PV), and proximal pulmonary artery (PA; see Table 9.1; see also Fig. 9.2).
The PSAX views are aligned orthogonal to the long-axis of the LV or aorta (see Tables 9.1 and 9.3; see also Figs. 9.3 and 9.4). The PSAX views are important for examination of all four cardiac valves: AV, MV, PV, and TV; both ventricles, LV, RV; both atria (LA, RA); and both septae, interatrial septum (IAS) and the interventricular septum (IVS). The PSAX views are acquired at multiple levels (see Figs. 9.3 and 9.4; see also Table 9.3)—namely at levels of (1) the aortic valve (AVL); (2) pulmonary artery bifurcation (PAB); (3) the MV; (4) papillary muscle (PML) or mid-LV; and (5) LV apical level and apical cap (apex).
Apical Views
The apical views (see Figs. 9.5–9.8; see also Tables 9.1 and 9.4) are the most important views in the TTE exam (along with the parasternal views). They play a central role in the assessment of ventricular systolic and diastolic function, as well as atrioventricular valve structure and function. The apical views transect the true cardiac apex and are aligned parallel to the cardiac long-axis. The typical order of examination of the apical views are (1) the apical four-chamber (A4C) view, (2) the apical five-chamber (A5C) view, (3) the apical two-chamber (A2C) view, and (4) the apical three-chamber (A3C) or apical long-axis (ALAX) view.
Subcostal Views
In adult echocardiography, the SC views complement the examination of the parasternal and apical views—specifically, both atria, LA, RA; both ventricles, LV, RV; the interatrial and interventricular septae; the mitral and tricuspid valves; the IVC and hepatic veins; and the proximal abdominal aorta (AA; see Fig. 9.9; see also Tables 9.1 and 9.5).
In patients with advanced chronic obstructive pulmonary disease (COPD) and chest trauma/postchest surgery patients, in whom the parasternal and apical windows are often obliterated or unavailable, the SC window can be used as a substitute. Here, a family of short-axis and long-axis views can be acquired that correspond to those normally obtained from the left parasternal and apical windows.
Suprasternal Notch Views
In the comprehensive 2D TTE adult examination, the suprasternal notch views are typically the final views acquired in the adult TTE examination. Here, the aortic arch and branches, the vena cave (SVC, IVC) en route to the RA, and proximal branches of the main pulmonary artery are examined (see Fig. 9.10; see also Tables 9.1 and 9.6).
TABLE 9.1
Standard Two-Dimensional Adult Transthoracic Echocardiography Views
| Window | Cardiac imaging plane | Region-Structures of Interest |
| Parasternal Views (see Figs. 9.1–9.4) | ||
| Parasternal (P) | Long-axis (LAX) | LV inflow-outflow, LA, MV, LV, LVOT, RVOT, IVS, Aortic root, descending thoracic aorta |
| P | LAX | RV inflow, TV, RV, coronary sinus, IVC |
| P | LAX | RV outflow: RVOT, PV, PA |
| P | Short-axis (SAX) | Aortic valve level: AV, TV, PV, IAS, LA, IAS, coronary arteries; IVC |
| P | SAX | PA bifurcation: main PA, PV, RPA, LPA, coronary arteries |
| P | SAX | Mitral valve level: MV, basal LV walls, LVOT, IAS |
| P | SAX | Papillary muscle level: LV walls, papillary muscles; IAS |
| P | SAX | Apical level: apical LV walls; LV apex (apical tip) |
| Apical Views (see Figs. 9.5–9.8) | ||
| Apical (A) | Four-chamber (4C) | LV, RV, LA, RA, MV, TV, pulmonary veins |
| A | Five-chamber (5C) | AV, LV, LVOT |
| A | Two-chamber (2C) | LV walls, LV, LA, LAA, MV |
| A | Three-chamber (3C); or long-axis (LAX) | LV walls, LV inflow-outflow, LA, MV, LV, LVOT, RVOT, IVS |
| Subcostal Views (see Fig. 9.9) | ||
| Subcostal (SC) | Four-chamber | IAS, LV, RV, LA, RA, MV, TV |
| SC | Long-axis (LAX) | Inferior vena cava (IVC), hepatic veins |
| SC | LAX | Abdominal aorta (AA) |
| SC | Optional views | Family of SAX and LAX views of the heart when transthoracic windows unavailable, or in the pediatric examination SAX views of IVC and AA |
| Suprasternal Notch Views (see Fig. 9.10) | ||
| Suprasternal notch | Long-axis | Aortic arch and branches, distal ascending aorta, proximal descending thoracic aorta |
| Suprasternal notch | Optional views | Short-axis views of the aortic arch with “crab” view of the LA and pulmonary veins, frontal view of the ascending aorta |
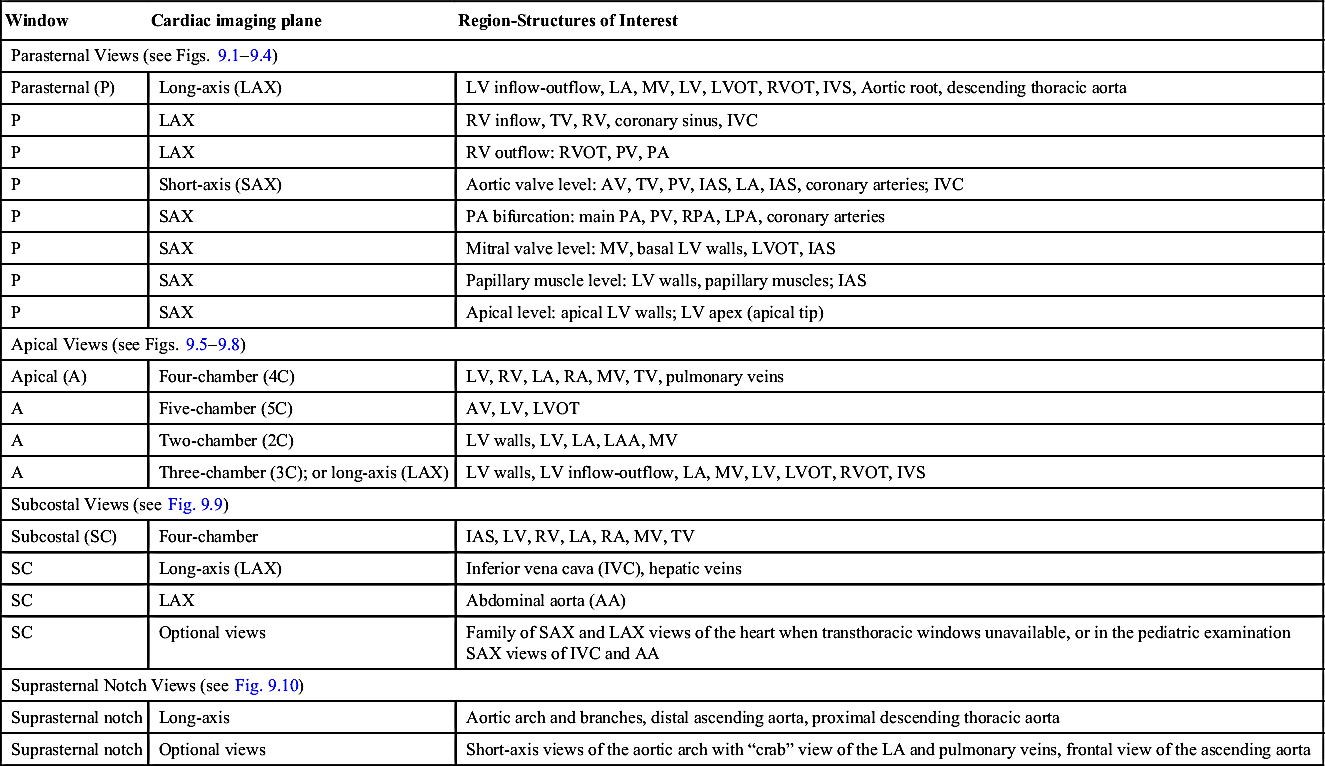
TABLE 9.2
Parasternal Long-Axis Views: Normal Examination (see Figs. 9.1 and 9.2)
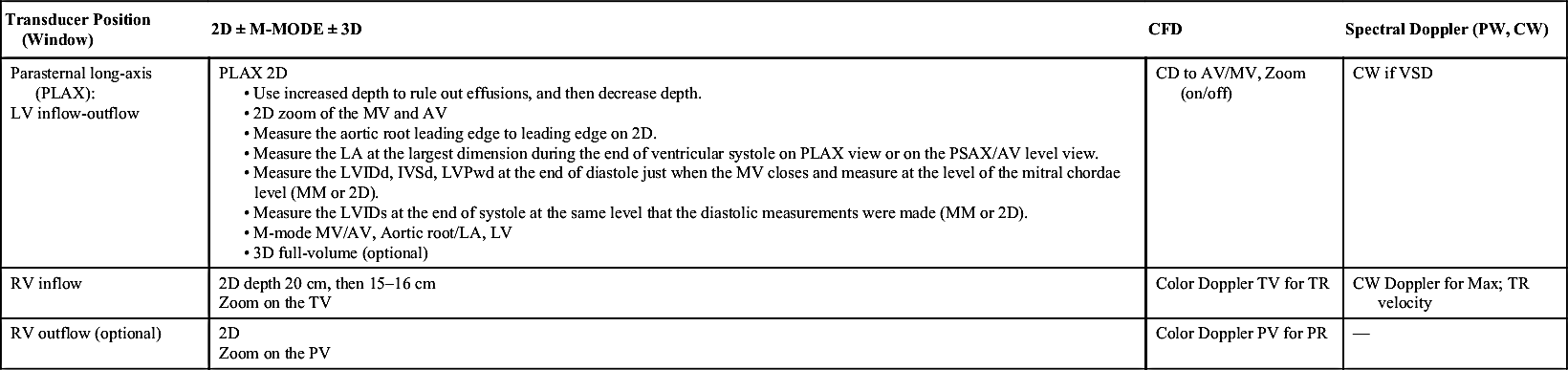
TABLE 9.3
Parasternal Short-Axis Views: Normal Examination (see Figs. 9.3 and 9.4)
| Transducer Position (Window) | 2D ± M-MODE ± 3D | CFD | Spectral Doppler PW, CW |
| Parasternal short-axis (PSAX): aortic valve level (AVL) | 2D to PV M-mode (optional) 3D full-volume (optional) | CFD to AV CFD to TV for TR CFD to PV for PR | CW to TR max velocity |
| PSAX: pulmonary artery bifurcation (PAB) | 2D image of PAB | CFD for PR and PDA | PW-CW of PV |
| PSAX: Mitral valve level (MVL) | 2D image at the MV and basal LV walls | CFD to MV | — |
| PSAX: papillary muscle level (PML) | 2D image at PML, mild LV walls | — | — |
| PSAX: apical level | 2D image at LV apical walls and LV apical segment | — | — |
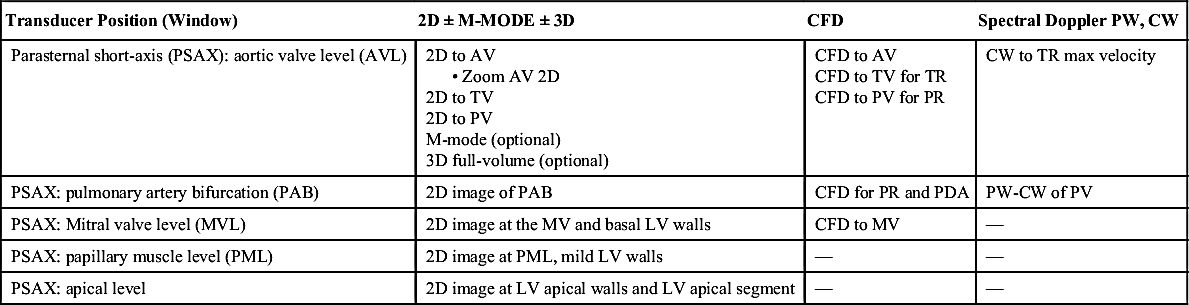
TABLE 9.4
Apical Views (see Figs. 9.5–9.8)
| Transducer Position (Window) | 2d ± M-Mode ± 3d | CFD | Spectral Doppler Pw, Cw | Tissue Doppler Imaging (Tdi) |
| Apical four-chamber (A4C) | 2D image; depth 15–16 cm. 2D Measurement of LA volume- measure LA volume at the end of systole and the shorter length of the LA 3D full-volume (optional) Evaluate RV function on 2D focus RV image. TAPSE (tricuspid annular plane systolic excursion) | CFD to MV for MR, MS CFD the Pulmonary veins, PW of right upper or lower pulmonary vein Color M-Mode flow propagation velocity CFD to TV and CW for TR max velocity. | PW Doppler at the tips of the mitral leaflets for MV inflow CW Doppler of the MV | TDI (PW) of MV annulus (lateral and septal) Color TDI to LV walls TDI of TV annulus |
| Apical five-chamber view (A5C) | 2D visualization of the AV-Zoom on the valve | CFD to the AV | PW Doppler of the LVOT (1–2 cm) from the valve leaflets, closing AV click CW for transaortic velocities | |
| Apical two-chamber view (A2C) | 2D image | CFD to MV | TDI (PW) of MV annulus (anterior and inferior) Color TDI to LV walls | |
Apical three-chamber view (A3C) or apical long-axis (ALAX) view | 2D image for wall motion evaluation | CFD to AV and MV | — | — |
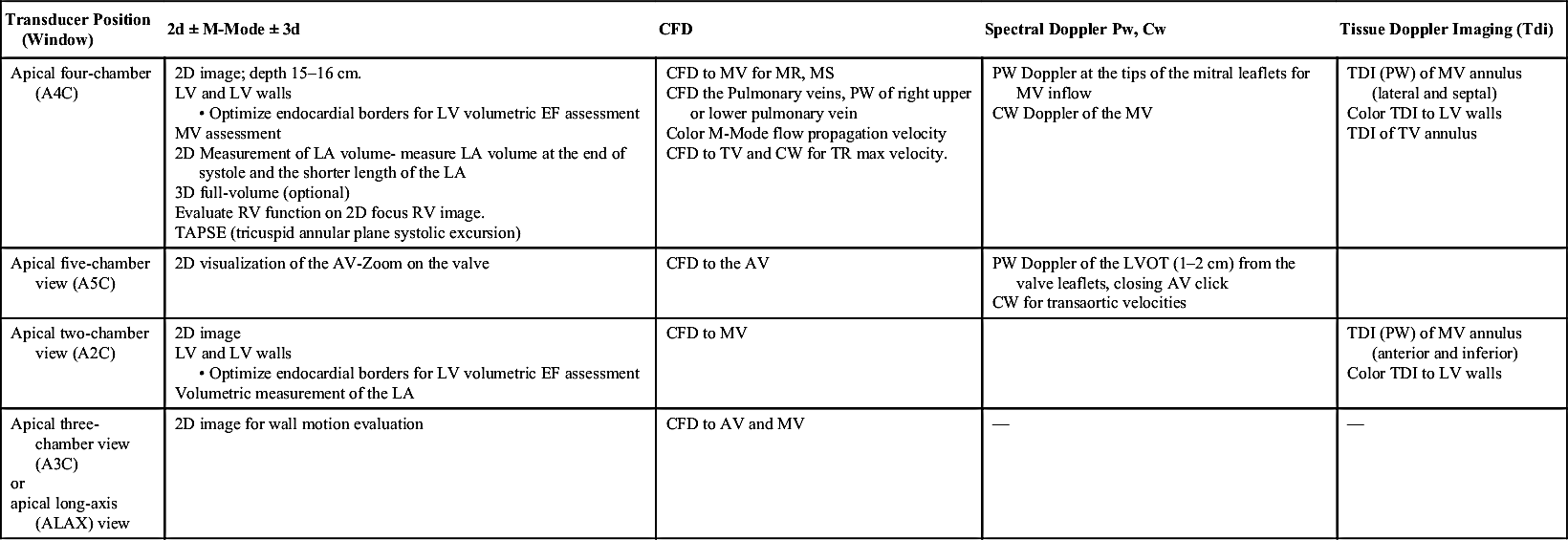
TABLE 9.5
Subcostal Views (see Fig. 9.9)
TABLE 9.6
Suprasternal Notch Views (see Fig. 9.9)
| Transducer Position (Window) | 2D | Color Flow Doppler | Spectral Doppler PW, CW | Tissue Doppler | 3D |
| SSN | 2D image Aortic arch, distal ascending aorta, proximal descending aorta | CFD | PW/CW | — | — |

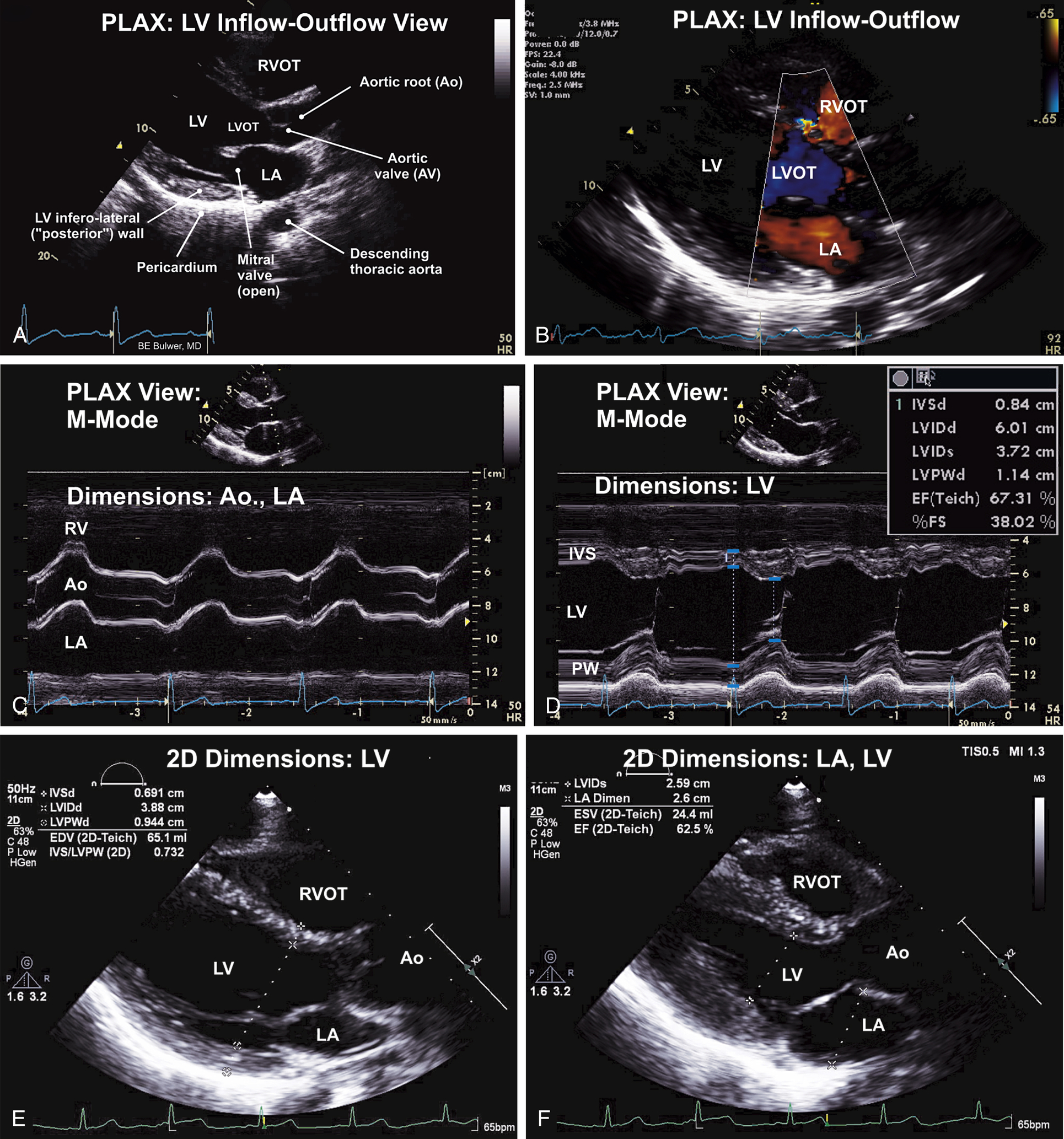
FIG. 9.1 Parasternal long-axis (PLAX) view—left ventricular (LV) inflow-outflow.
(A) PLAX of the heart showing the LV inflow, and outflow (LVOT), the outflow portion of the right ventricle (RV), and related structures. This view is usually the first view obtained in the transthoracic examination, and can provide a quick overview of several aspects of cardiac structure and function. Significant findings should be sought using subsequent echocardiographic windows and views. Quantitative measures of cardiac chamber size and dimensions should also obtained on this view. (B) PLAX showing color flow Doppler (CFD) interrogation of the mitral and aortic valves. The examination may reveal flow patterns indicative of valvular stenosis or regurgitation. Ventricular septal defects involving the interventricular septum may also be detected on CFD. (C) M (motion) of the PLAX at the level of the aortic valve (AV). These measurements are useful when LV geometry is normal. (D) M-mode along the PLAX at the level of the LV. These measurements are useful when LV geometry is normal. (E) Linear LV dimensions measured using the parasternal long-axis (PLAX) view. These are preferred over M-mode linear measures which are prone to off-axis measurements, made worse in the presence of remodeled LV geometry. (F) End-systolic frame showing measurement of the LV internal diameter during systole (LVIDs) and the left atrial.
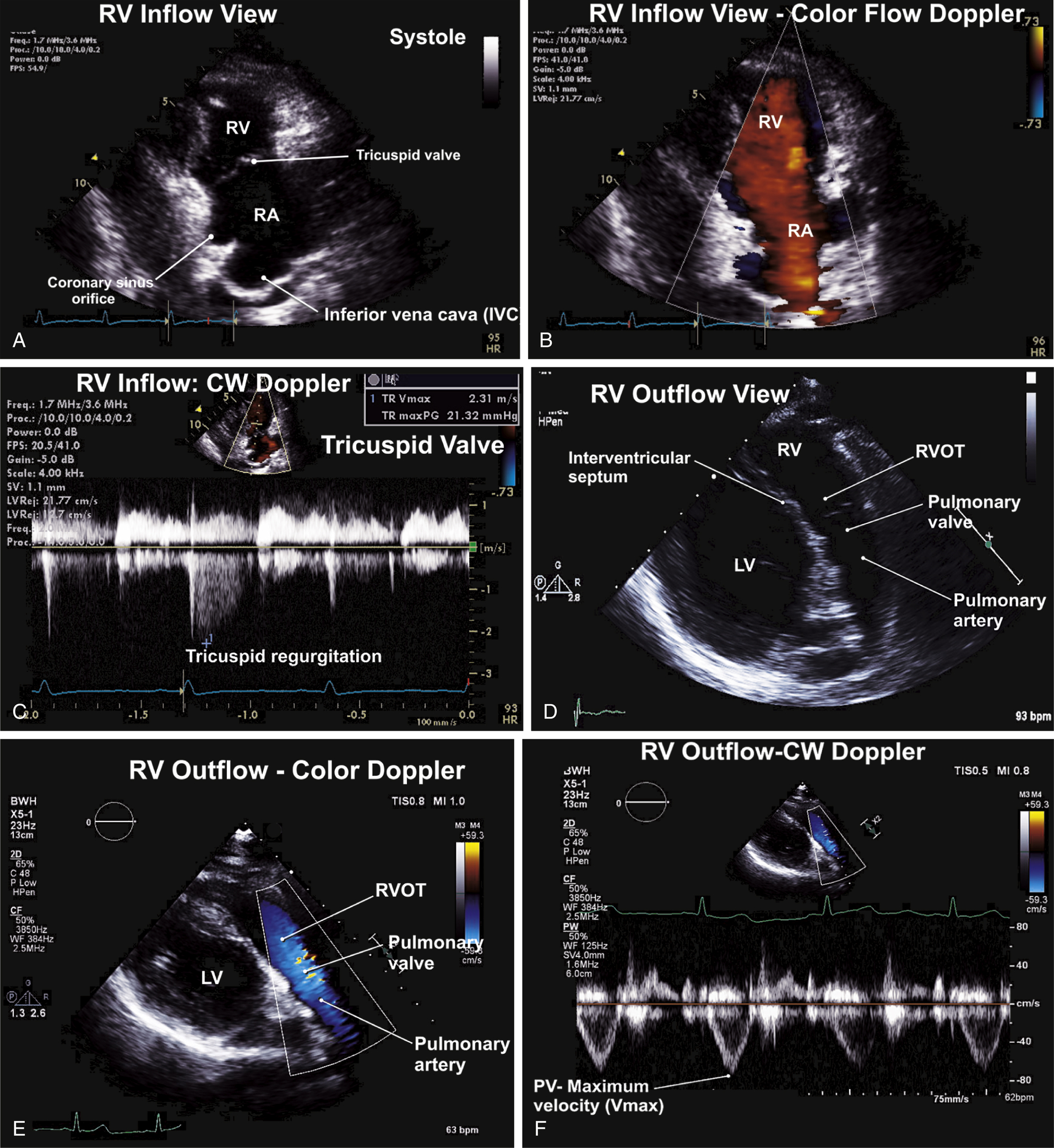
FIG. 9.2 Right ventricular inflow and outflow views.
Right ventricular (RV) inflow view. This view is useful for Doppler interrogation of the tricuspid valve. (A) RV Doppler interrogation of the tricuspid valve on the RV inflow view. Diastolic flow from the right atrium (RA) into the RV moves in a direction toward the transducer—hence appearing red (by convention). Flow away from the transducer (e.g., tricuspid regurgitation) would appear blue. (B) Continuous-wave (CW) Doppler to the tricuspid valve showing spectral profile predominantly below the baseline. This finding represents mild tricuspid regurgitant flow away from the transducer. (C) The long-axis view of the RV outflow track and main pulmonary artery (MPA) is often performed in the initial assessment of flow across the RV outflow tract (RVOT), the pulmonary valve, and the MPA. (D) Color flow Doppler showing the normal systolic flow velocities across the pulmonary valve. Blue flow is indicative of flow away from the transducer. (E) Pulsed-wave (PW) Doppler assessment of flow at the level of the pulmonary valve. Velocities below the baseline are indicative of forward flow away from the transducer.
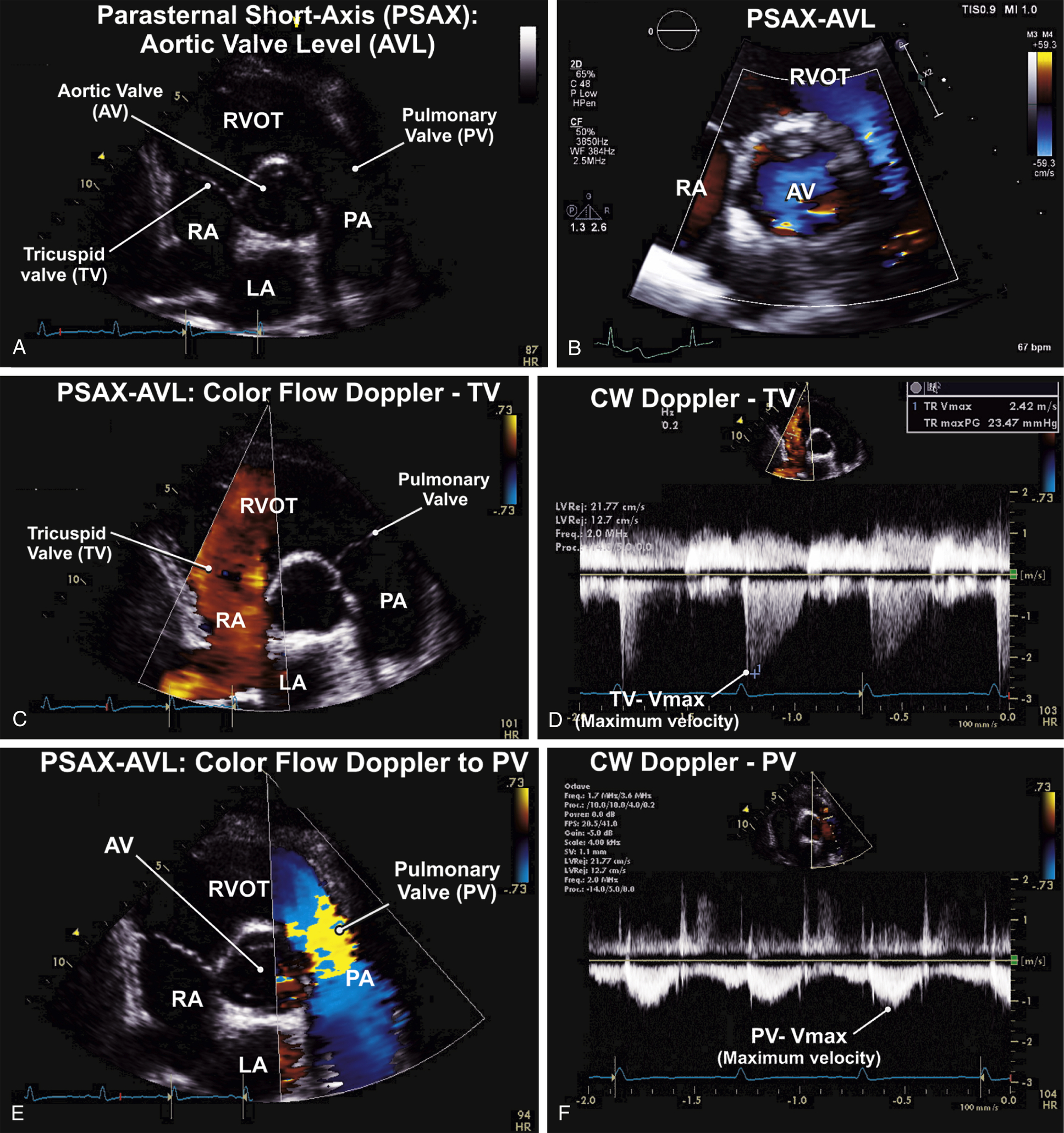
FIG. 9.3 Parasternal short-axis (PSAX) view—aortic valve level (AVL).
(A) The PSAX-AVL view at the base of the heart is important in the assessment of the three cardiac valves: the aortic, tricuspid, and pulmonary valves. (B) Zoomed view of the aortic valve showing flow across the aortic valve on color flow Doppler. (C) The routine assessment of flows across the tricuspid valve, including tricuspid regurgitant (TR) flows is performed on the PSAX-AVL view on color flow Doppler. (D) Maximum velocities (Vmax) of TR flows is routinely measured using continuous-wave (CW) Doppler. This is used to estimate RV systolic pressures/pulmonary artery systolic pressures (PASP) using the Bernoulli equation. (E) Color flow Doppler assessment is the important first step in the evaluation of flows across the pulmonary valve. (F) The Vmax across the pulmonary valve is routinely measured using the CW Doppler.
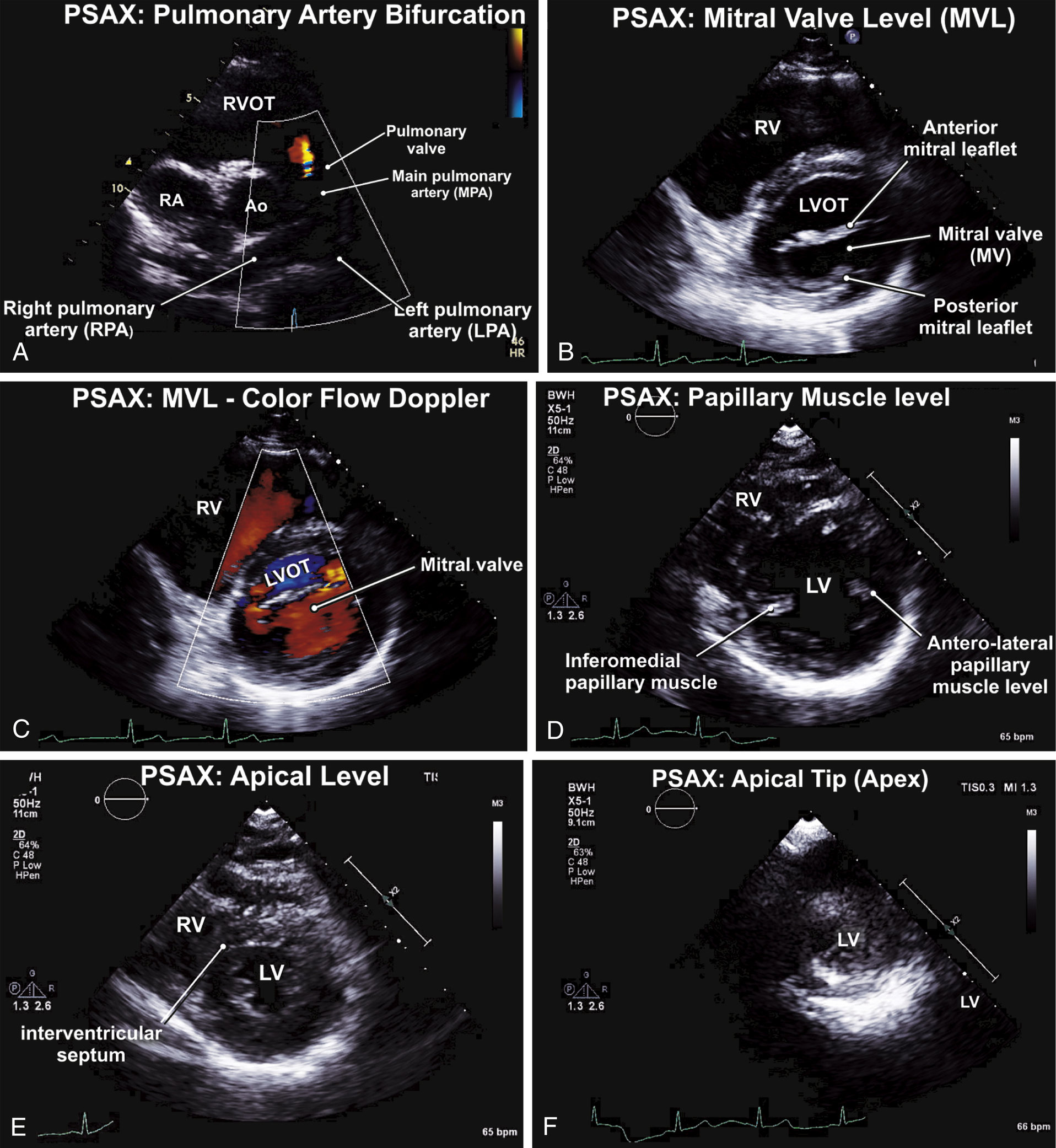
FIG. 9.4 Parasternal short-axis (PSAX) views—at the levels of the pulmonary artery bifurcation (PSAX-PAB), mitral valve (PSAX-MVL), papillary muscle (PSAX-PML), and left ventricular apex.
(A) Diastolic frame of the PSAX-PAB is shown, along with a small pulmonary regurgitant jet. The ostia of the coronary arteries can be examined using this view. (B) A diastolic frame on the PSAX-MVL view is shown, with the mitral leaflets in their open position. Polarimetry of the mitral valve orifice on both two-dimensional and three-dimensional echocardiography is measured on this view. (C) Color flow Doppler is useful to assess abnormal flow patterns across the MV on the PSAX-MVL view. Localization of the affected MV scallops can be identified on color flow Doppler. (D) Assessment of ventricles, the LV walls, and the interventricular septum is routinely performed using the PSAX-PML view. This complements the regional wall motion assessment of the LV segments performed. (E) More distally, assessment of the regional walls of the LV is also routinely performed on the PSAX view at the level of the LV apical segments. (F) LV torsion can be routinely observed by PSAX views at the apical tip of the LV. This can be quantified on speckle-tracking echocardiography.
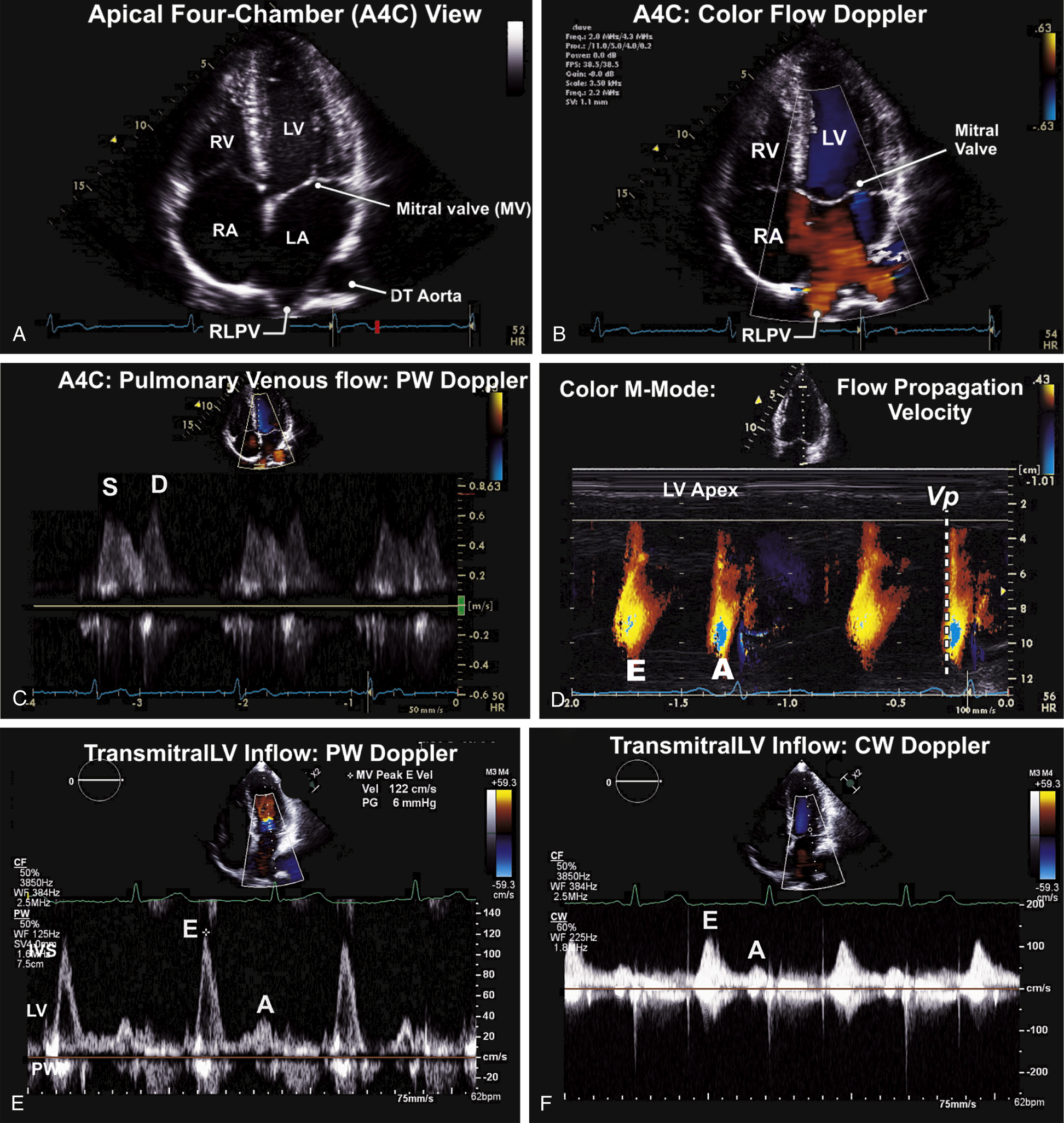
FIG. 9.5 Apical four-chamber (A4C) view—left atrial and left ventricular filling.
(A) The A4C showing the four cardiac chambers and the atrioventricular valves. This view plays a critical role in the assessment of ventricular systolic and diastolic function, and is optimally aligned to assess left atrial and left ventricular filling. (B) Color flow Doppler assessment is initially used to assess flows within the cardiac chambers and across the mitral and tricuspid valves. (C) Left atrial filling is assessed using PW Doppler interrogation of pulmonary venous flow. This is used as a composite measure of LV diastolic function assessment. (D) Color Doppler M-mode of flow propagation of velocities within the LV is routinely measured. The slope (Vp) of the early rapid diastolic flow of LV filling is also used as a composite measure in the assessment of LV diastolic function. (E) Left ventricular transmitral filling is routinely assessed as a composite measure of LV diastolic function. Flow at the tip of the mitral leaflets is measured using PW Doppler. (F) Peak flows and gradients across the mitral valve is assessed using CW Doppler.
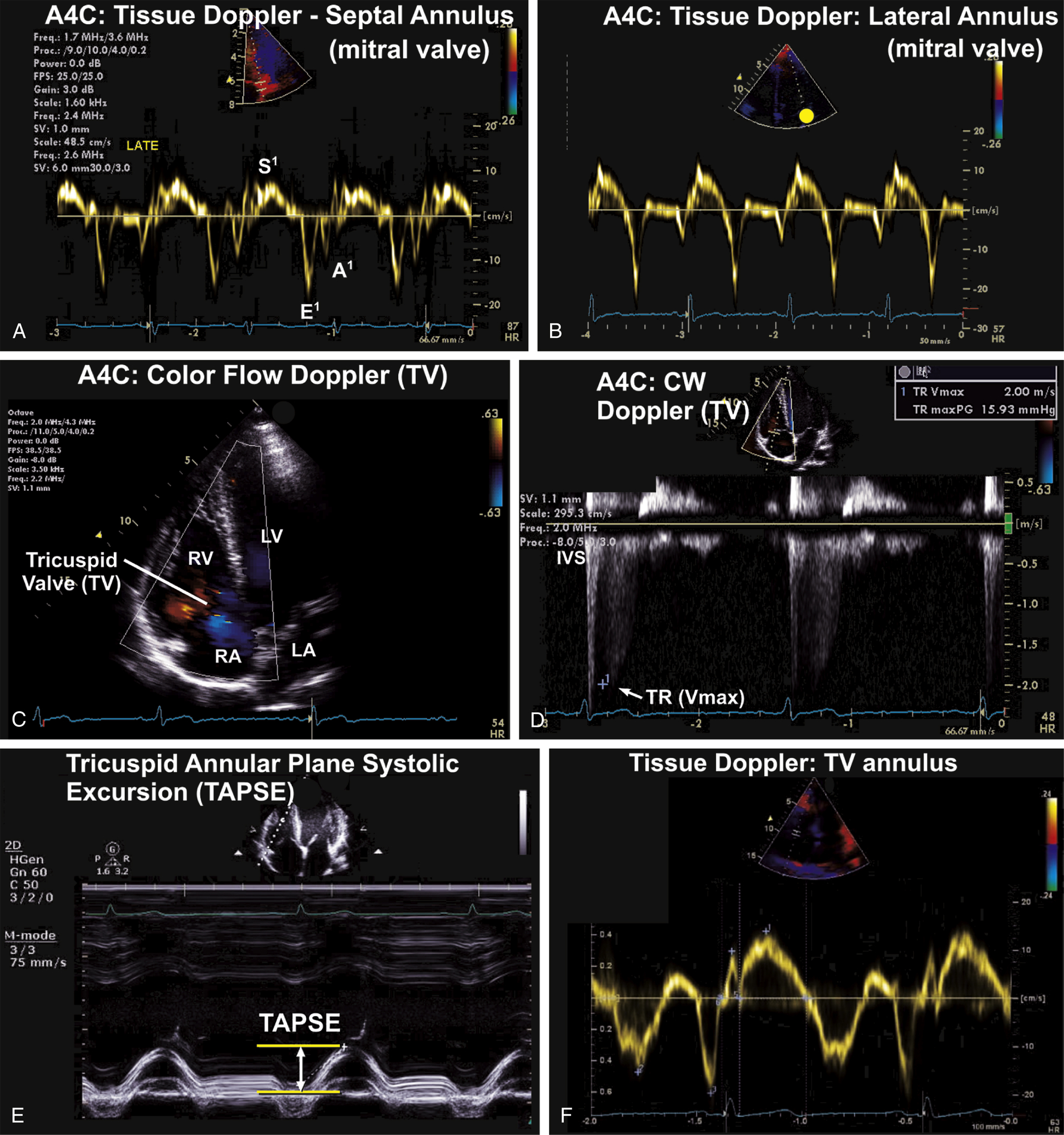
FIG. 9.6 Apical four-chamber (A4C) view—tissue Doppler imaging at the mitral annulus and right ventricular function assessment.
(A) Tissue Doppler imaging (TDI) of the mitral valve annulus on the A4C views. TDI is useful in the assessment of longitudinal diastolic and systolic myocardial mechanics. (B) Both the septal and mitral annulus are routinely assessed during the comprehensive adult transthoracic echocardiography examination. (C) Assessment of flow across the tricuspid valve (TV) on the A4C view. This complements the assessment of tricuspid regurgitation that initially begins on the PSAX view at the level of the aortic valve. (D) Continuous-wave (CW) Doppler assessment of tricuspid regurgitation (TR) across the TV. From this, right atrial systolic pressure and pulmonary artery systolic pressure can be assessed using the maximum velocity (Vmax) of the TR jet. (E) Complementary measures of right ventricular systolic function includes the measurement of the tricuspid annular plane systolic excursion (TAPSE) on M-mode and RV fractional area change. (F) Tissue Doppler imaging (TDI) of the RV myocardial velocities is now routinely performed on the A4C view.
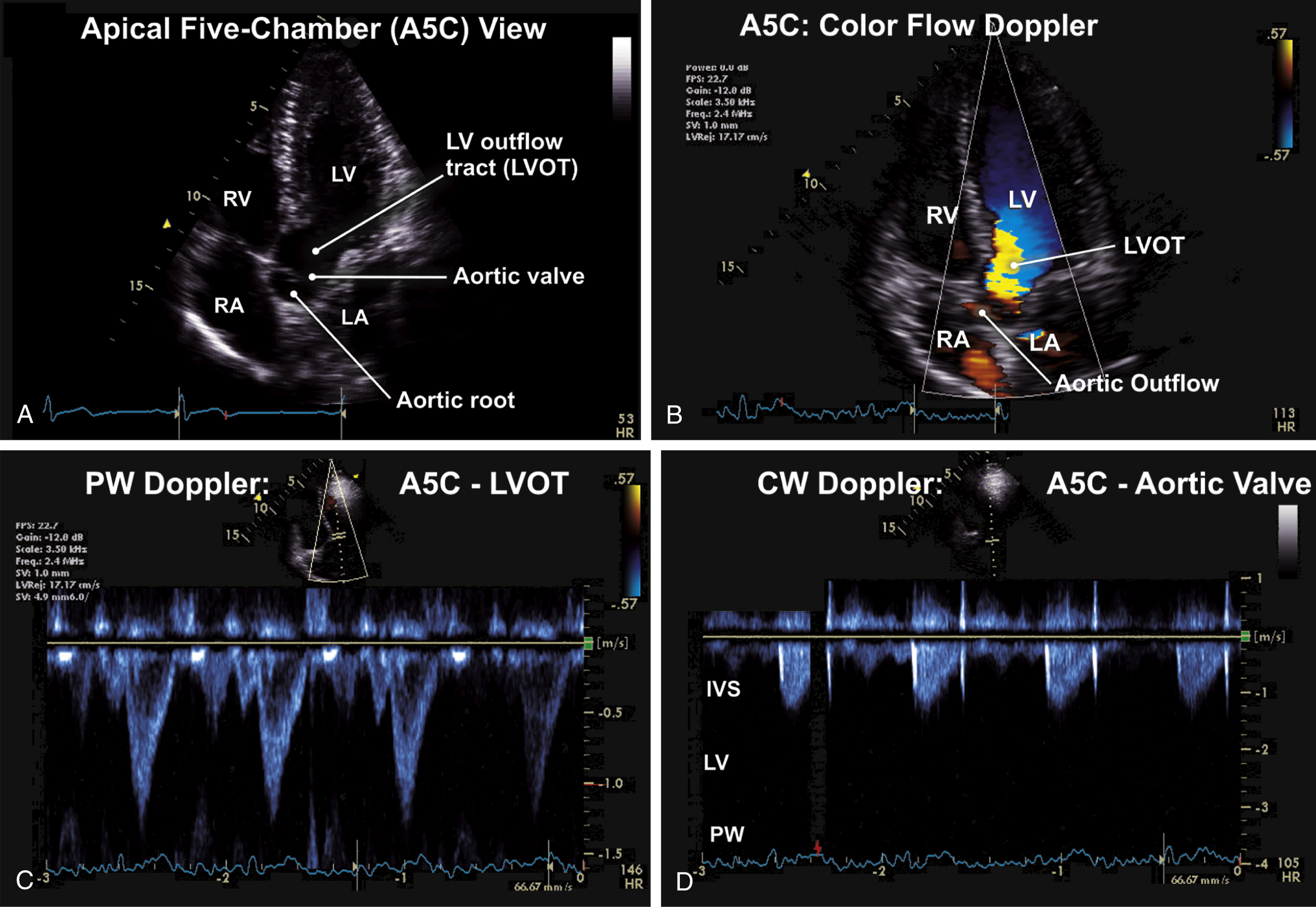
FIG. 9.7 Apical five-chamber (A5C) view.
(A) Apical five-chamber (A5C) view showing the aortic root and LV outflow tract. The A5C view also complements the evaluation of the four cardiac chambers, intervening, and atrioventricular valves. (B) Color flow Doppler interrogation of flow velocities across left ventricular outflow tract (LVOT) and the aortic valve on the A5C view. This view is important for evaluating pathology of the aortic valve and LVOT. (C) The A5C view is ideal for evaluation of flows across the LV outflow tract and the aortic valve. Frame showing PW Doppler assessment of velocities and gradients across the left ventricular outflow tract. This is useful for evaluation of LVOT obstruction in hypertrophic cardiomyopathy and subvalvular aortic stenosis. (D) Continuous-wave (CW) Doppler is useful for evaluation of the transaortic velocities and pressure gradient. This measurement is used for calculation of peak velocities and gradients across the aortic valve in aortic stenosis.
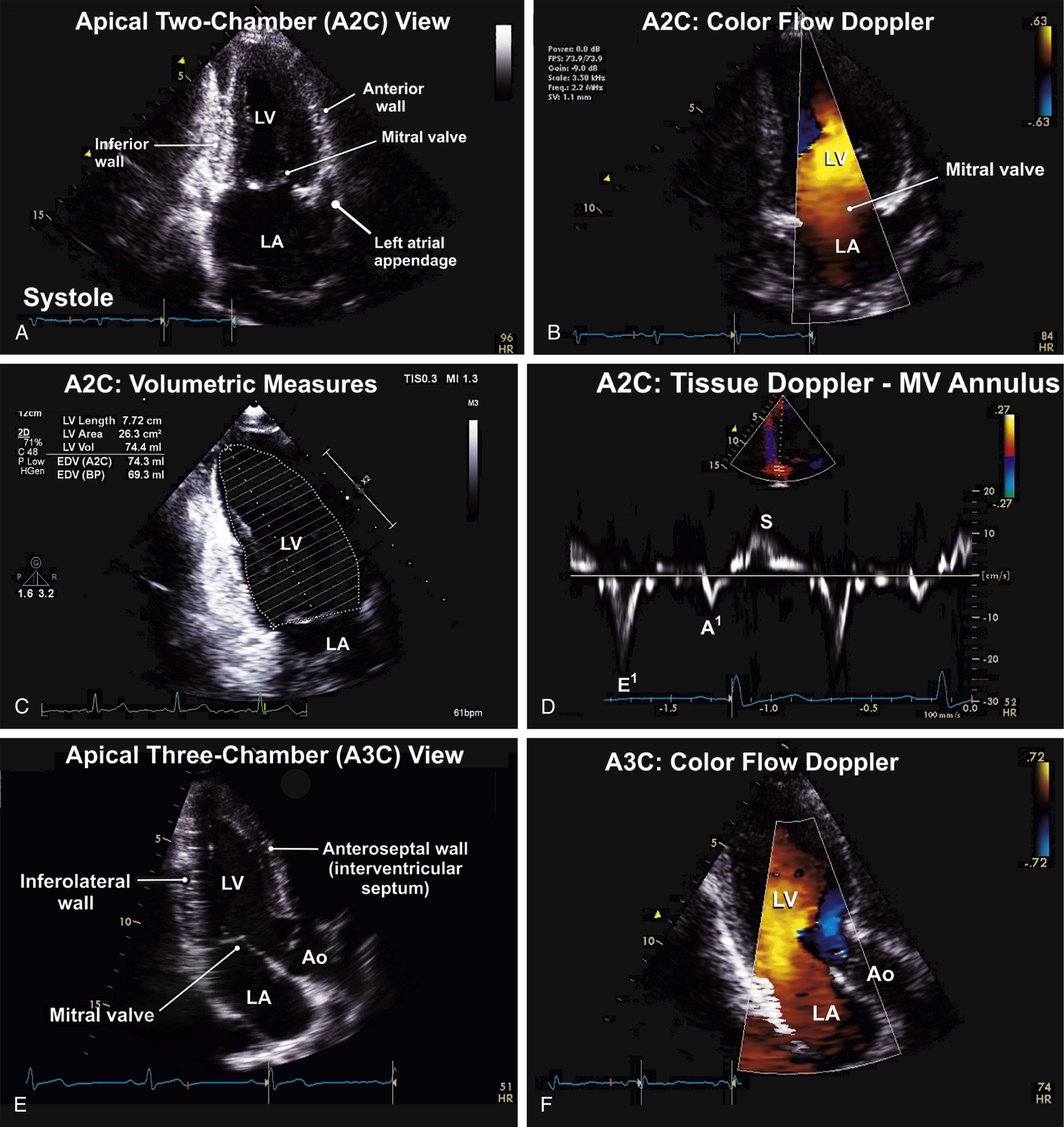
FIG. 9.8 Apical two-chamber (A2C) and apical three-chamber (A3C) views.
(A) The A2C view showing the left-sided cardiac chambers and the intervening mitral valve. Measures of cardiac chamber size and dimensions should also obtained on this view. (B) Color flow Doppler evaluation of the mitral valve on the A2C) view. (C) Diastolic frame showing the measurement of left ventricular area, as part of the assessment of LV volumes using the biplane method of disks (Simpson’s rule). This method is used to measure left atrial areas and volumes on the A2C view. (D) Tissue Doppler assessment of the left ventricular annulus is also performed on the A2C view. Here, measurement of the inferior mitral annulus is shown. (E) The A3C or the apical long-axis (ALAX) view is aligned along the LV long-axis like the PLAX view. However, it enables visualization of the LV apex. Measures and assessments conducted on the PLAX and A5C views can be performed and corroborated using the A3C view. (F) Color flow Doppler assessment of LV inflow and outflow across the mitral and aortic valves on the A3C view.
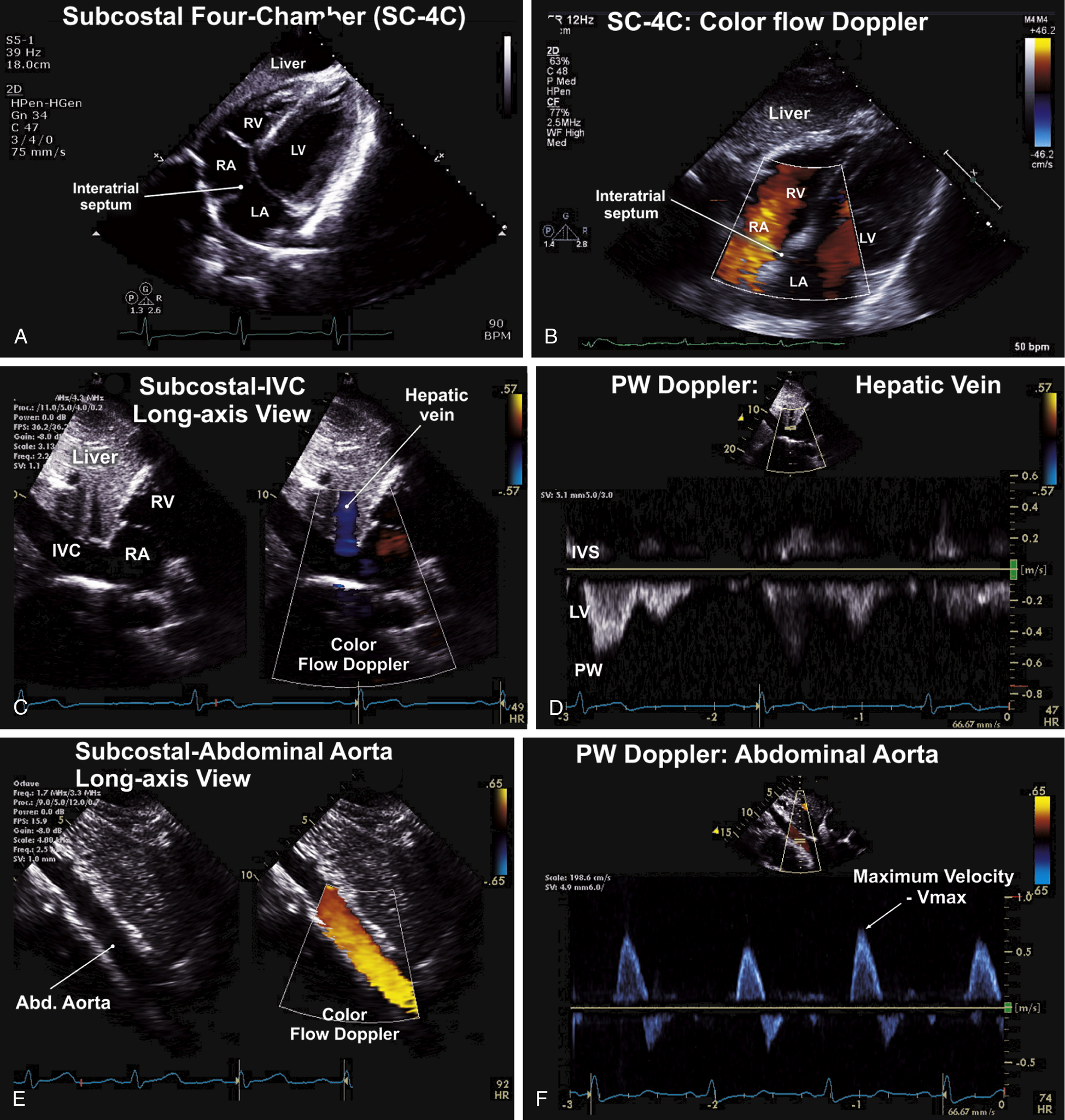
FIG. 9.9 Subcostal views.
(A) The subcostal four-chamber (SC-4C) view permits optimal viewing of the interatrial septum and atrial septal defects. It complements the assessment of the parasternal and apical views of the four-cardiac chambers and atrioventricular valves. (B) Color flow Doppler interrogation of the interatrial septum on the subcostal four-chamber (SC-4C) view shows an intact interatrial septum. (C) The subcostal-IVC view permits evaluation of inferior vena cava (IVC) dimensions, respirophasic behavior, and Doppler evaluation of IVC and hepatic vein flow. (D) On the subcostal-IVC view, pulsed (PW) Doppler evaluation of the hepatic veins normally shows a spectral velocity profile of flow (below baseline), mostly during systole. This pattern is reversed in severe tricuspid regurgitation due to flow reversal. (E) Subcostal long-axis views of the proximal abdominal aorta (left). Color flow Doppler examination of the abdominal aorta shows laminar red flow velocities toward the transducer. (F) PW Doppler examination of the aortic valve shows the characteristic biphasic velocity profiles, with forward flow above the baseline and peak velocities below 1 m/s.
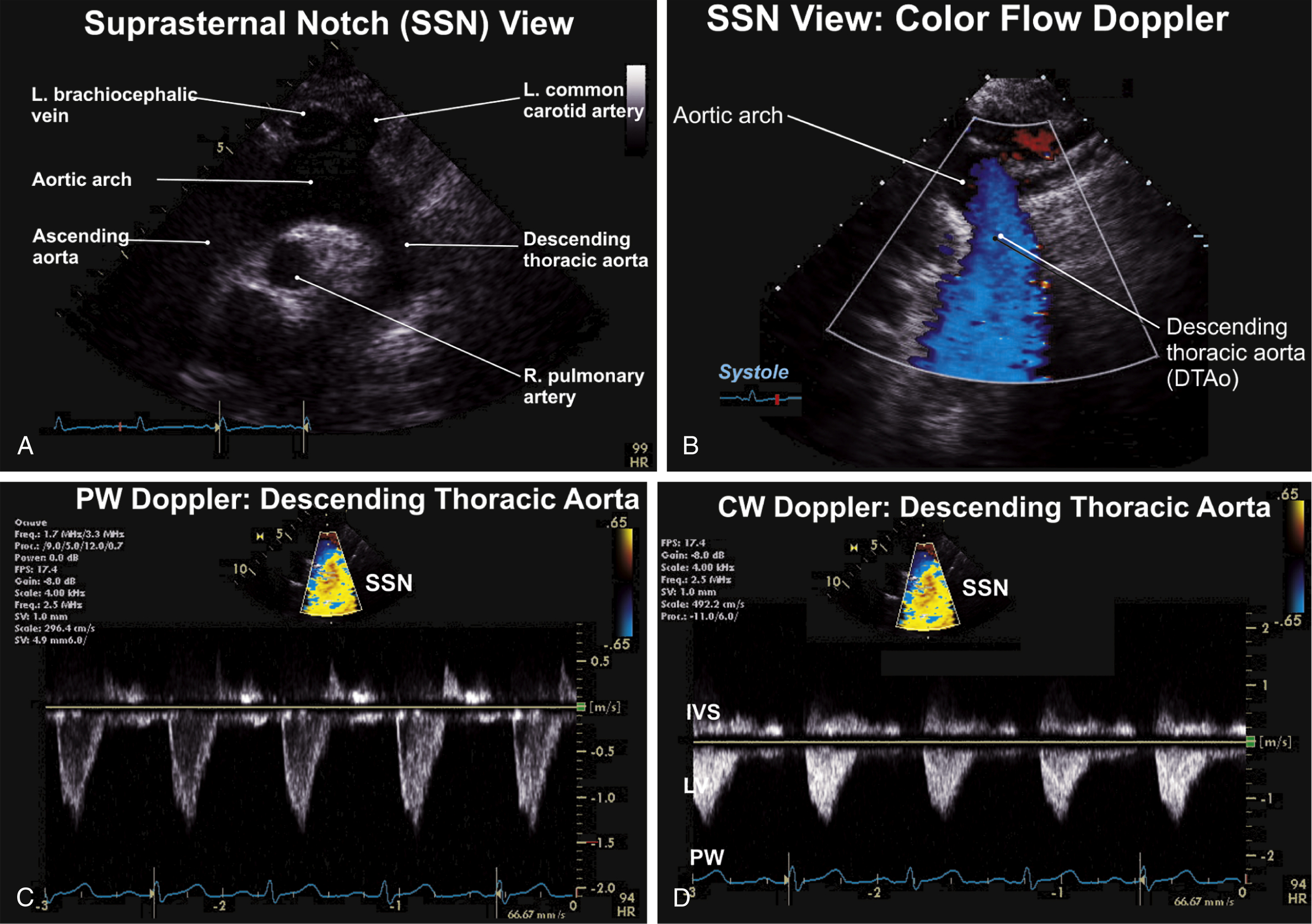
FIG. 9.10 Apical two-chamber (A2C) and apical three-chamber (A3C) views.
(A) The suprasternal notch (SSN) view is best for visualization of the aortic arch and branches and for evaluation of coarctation of the aorta. (B) Color flow Doppler evaluation of the proximal descending thoracic aorta shows normal (blue) flow away from the transducer. (C) Evaluation of flow in the descending thoracic aorta is best visualized and assessed on the suprasternal notch (SSN) view. Coarctation of the aorta, which classically affects the postductal portion distal to the left subclavian artery origin, requires pulsed (PW) and continuous-wave Doppler assessment. (D) Continuous-wave (CW) Doppler assessment of flow in the descending thoracic aorta. This is used to evaluate peak flows across the descending thoracic aorta.