20 ANALYSIS: SOLITARY PULMONARY NODULE
Solitary pulmonary nodule (SPN):
“to qualify as a nodule or cyst, a pulmonary lesion must present a reasonably sharp outline. Hence, a focal infiltrate with ill-defined borders is excluded…. I have set no upper limit of size for a pulmonary nodule, though I usually call the big ones a mass”1.
“a focal round or oval area of increased opacity in the lung that measures less than 3.0 cm in diameter”2.
A COMMON SCENARIO
An otherwise generally well patient has a CXR (e.g. for high blood pressure). A SPN is an unexpected finding.
Frequently, the clinical history will make a particular diagnosis highly likely. Examples: a man of 65 who has smoked two packs a day for 40 years—the default diagnosis will be a primary bronchial carcinoma. A history of carcinoma of the breast/kidney/colon some years previously will make a secondary deposit likely.
On the other hand there may be no clue from the history. In this case there are three steps:
| Most common | ||
| Less common | ||
| Much less common | ||
| Very rare | ||
Table 20.3 SPN: benign characteristics.
| CXR feature | Comment |
|---|---|
| Size |
2. A nodule of less than 1 cm in diameter is very difficult to visualise7. Apply this maxim: “this nodule is less than 1 cm in diameter but I can see it very well indeed. This means that it is almost certainly calcified and thus it will be benign.”
|
| Shrinking | Rapid reduction in size in days or weeks on interval CXRs — the lesion is benign (often a resolving infection). |
| Calcification | Benign if central, shaggy, laminated, popcorn, or stippled. |
| Presence of Branching | Tubular branching leading up to the nodule suggests: |
| Stable | No change over two years is a strong feature suggesting a benign lesion8. Not an absolute guarantor5,6 but indicates a high probability. |
CAUSES OF A SPN
A solitary pulmonary nodule is a very common finding on a CXR in adults. The vast majority are benign lesions (Table 20.1), usually old granulomas2-4.
CLINICAL ASSESSMENT
CLINICAL DETAILS ARE CRUCIAL
 Is the clinical history helpful? Sometimes a recent low grade chest infection may result in a residual area of pneumonia. A history of asthma will raise the possibility of mucoid impaction. Perhaps there has been a recent injury to the chest, e.g. a haematoma. Is the clinical examination abnormal? Is there a mole or skin tag on the chest wall? A breast lump, an abdominal mass or an enlarged liver would raise the likelihood of malignancy.
Is the clinical history helpful? Sometimes a recent low grade chest infection may result in a residual area of pneumonia. A history of asthma will raise the possibility of mucoid impaction. Perhaps there has been a recent injury to the chest, e.g. a haematoma. Is the clinical examination abnormal? Is there a mole or skin tag on the chest wall? A breast lump, an abdominal mass or an enlarged liver would raise the likelihood of malignancy.Table 20.2 Traps: simulated pulmonary nodules.
STEP-BY-STEP CXR ANALYSIS
| Step 1: | Exclude any of the common traps (Table 20.2). A nodule may not be in the lung. A lateral CXR will confirm (or exclude) the lesion as intrapulmonary. |
| Step 2: | Apply this rule: “the best next step is comparison with a previous CXR”. This will often remove the need for any further investigation.
If a CXR two or more years prior shows that the lesion has not changed in size…the SPN can be assumed to be benign, usually a benign granuloma. This is not a 100% guarantee5,6. Nevertheless, it is a highly reliable rule of thumb. Lack of growth implies a long doubling time (see opposite) which generally indicates a benign histology. This criterion has even greater power if earlier images (i.e. beyond two years) are also available for comparison. |
| Step 3: | No previous CXR available: look for benign features (Table 20.3). |
| Step 4: | No previous CXR available: look for malignant features (Table 20.4). |
| Step 5: | Is CT of the thorax necessary? Table 20.6 provides guidelines. |
The growth rate of a lesion is often expressed in terms of doubling time (i.e. the time in which a nodule doubles in volume12). It has been estimated that a nodule goes through some 30 doublings before it reaches 1 cm in diameter and becomes readily detectable on a CXR13. Bronchial carcinomas usually take 1–18 months to double in size.
Table 20.4 SPN: malignant characteristics.
| CXR feature | Comment |
|---|---|
| Size | Diameter of more than 3 cm is very suggestive of malignancy. |
| Margin | Ill-defined or spiculated border is a strong pointer towards malignancy. |
| Strands | Radiating strands at the margin — strong probability of a primary carcinoma… but not an absolute certainty. |
| Calcification position9,10 | Eccentric calcification raises the suspicion of a scar carcinoma. |
Rule of thumb: A doubling time of less than one month, or alternatively more than 18 months, suggests benign disease. This maxim is a helpful guideline, but there are occasional exceptions.
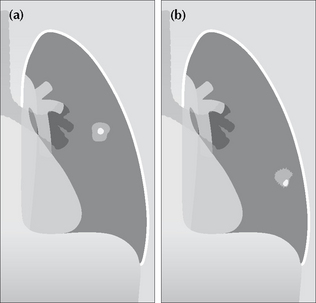
Figure 20.2 (a) Central calcification in a SPN is usually a benign feature. (b) Eccentric calcification raises the suspicion of a carcinoma arising in an old scar.
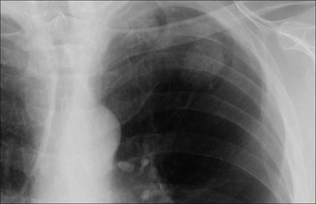
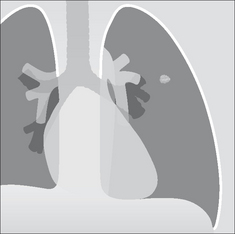
Figure 20.3 SPN at the apex of the left lung. The margin is slightly irregular and ill-defined. These two features are suggestive of a primary bronchial carcinoma.
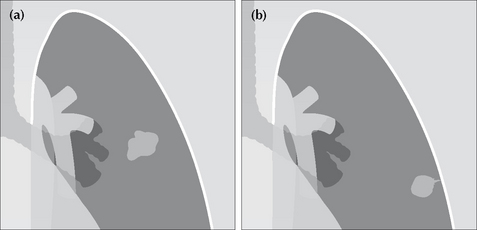
Figure 20.4 SPNs. In (a) the margin is irregular. In (b) a tail sign is present. A “tail” is a strand-like or linear projection of tissue extending outwards from the margin of a nodule. Either (a) or (b) should raise the strong suspicion of malignancy.
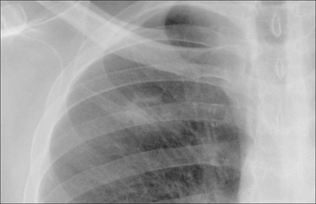
Figure 20.5 The right upper zone nodule has a cavity within it. Some benign lesions do cavitate, e.g. abscess or rheumatoid nodule. All the same, in the appropriate clinical setting, cavitation should always suggest the probability of a squamous carcinoma. Subsequently confirmed squamous carcinoma of the bronchus.
Table 20.5 SPN: unreliable characteristics… the indeterminate nodule.
| CXR feature | Comment |
|---|---|
| Smooth margin | |
| Lobulated outline | May be present in benign as well as in malignant lesions. |
| The tail sign | Can occur in benign and malignant lesions11 (Fig. 20.4). |
| Cavitation | Abscesses cavitate. Squamous cell carcinomas cavitate. |
| Doubling time/rate of growth |
| CXR analysis | Feature | CT indicated? |
|---|---|---|
| Step 1 | An artefact is confirmed (Table 20.2) | No |
| Step 2 | Lesion unchanged over the previous two years | No (very occasionally, the clinical context—age, smoking history— will justify CT) |
| Lesion has increased in size over the previous two years | Yes | |
| Step 3 | Classic benign features (Table 20.3) | No |
| Step 4 | Yes | |
| Yes |
AN INTERESTING LESION—PULMONARY HAMARTOMA2,10
Pathology
Hamartomas are benign tumours found in various organs. All hamartomas contain cells of some of the tissues within the organ of origin. A pulmonary hamartoma invariably contains cartilage and bronchial epithelium; it often contains fat.
Clinical features
Usually an incidental, asymptomatic finding. Tuberous sclerosis is a rare association.
The CXR
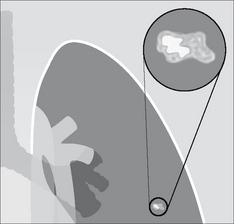
Figure 20.6 Some hamartomas contain visible calcification. It is often stippled or popcorn shaped. This figure shows the appearance of popcorn calcification. Note the similarity to a popped kernel of corn1.
1. Felson B. Chest Roentgenology. Philadelphia, PA: WB Saunders, 1973;314-329.
2. Erasmus JJ, McAdams HP, Connolly JE. Solitary pulmonary nodules: Part I. Morphologic evaluation for differentiation of benign and malignant lesions. Radiographics. 2000;20:43-58.
3. Gurney JW. Determining the likelihood of malignancy in solitary pulmonary nodules with Bayesian analysis. Radiology. 1993;186:405-413.
4. Lillington GA, Caskey CI. Evaluation and management of solitary and multiple pulmonary nodules. Clin Chest Med. 1993;14:111-119.
5. Sherrier RH, Chiles C, Johnson GA, et al. Differentation of benign from malignant pulmonary nodules with digitized chest radiographs. Radiology. 1987;162:645-649.
6. Yankelevitz DF, Henschke CJ. Does 2-year stability imply that pulmonary nodules are benign? AJR. 1997;168:325-328.
7. Kundel HL. Predictive value and threshold detectability of lung tumours. Radiology. 1981;139:25-29.
8. Good CA. Roentgenologic appraisal of solitary pulmonary nodules. Minn Med. 1962;45:157-160.
9. Hansell DM, Armstrong P, Lynch DA, McAdams HP. Imaging of Diseases of the Chest, 4th ed. St Louis, MO: Mosby, 2005.
10. Collins J, Stern EJ. Chest Radiology: The Essentials. Philadelphia, PA: Lippincott Williams & Wilkins, 1999.
11. Webb WR. The pleural tail sign. Radiology. 1978;127:309-313.
12. Reed JC. Chest Radiology: Plain Film Patterns and Differential Diagnoses, 5th Edition. Philadelphia, PA: Mosby, 2003.
13. Collins VP, Loeffler RK, Tivey H. Observations on growth rates of human tumors. Am J Roentgenol. 1956;76:988-1000.
14. Erasmus JJ, McAdams HP, Connolly JE. Solitary pulmonary nodules: Part II. Evaluation of the indeterminate nodule. Radiographics. 2000;20:59-66.
15. Dewan NA, Shehan CJ, Reeb SD, et al. Likelihood of malignancy in a solitary pulmonary nodule: comparison of Bayesian analysis and FDG–PET scan. Chest. 1997;112:416-422.
16. Woodring JH, Fried AM. Significance of wall thickness in solitary cavities of the lung: a follow-up study. AJR. 1983;140:473-474.