21 ANALYSIS: MULTIPLE PULMONARY NODULES
“The term is generally accepted as indicating several or many separate and rounded lung densities varying in size up to 30 mm in diameter.”
“miliary pattern (nodules)…a collection of tiny discrete pulmonary opacities that are generally uniform in size, widespread in distribution, and each of which is 2 mm or less in diameter.”1
TWO SCENARIOS
Scenario 1: A CXR shows multiple nodules. It is highly likely that the patient’s clinical history will suggest the likely diagnosis. Examples:

Scenario 2: The clinical presentation does not provide an obvious clue to the likely diagnosis. We need to remind ourselves of:
Table 21.1 Causes of multiple pulmonary nodules2–6.
| Inflammatory/Infective | |
| Neoplastic | |
| Autoimmune disease | |
| Vascular | |
| Other |

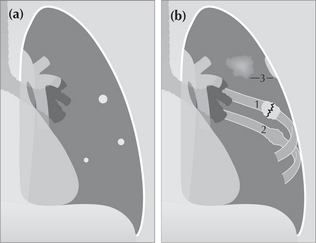
Figure 21.1 (a) Multiple pulmonary nodules. The size of the nodules usually vary. Strictly speaking, a nodule has a maximum diameter of 30 mm. Above 30 mm an opacity is conventionally referred to as a mass. Some descriptive flexibility is accepted, particularly if most of the lesions are less than 30 mm in diameter. (b) Opacities outside the lung can simulate pulmonary nodules. These include healing rib fractures (1), old rib fractures (2), and pleural plaques (3).
CAUSES OF MULTIPLE NODULES
A CXR showing clinically unexpected nodules is unusual. The default diagnosis is metastatic disease. In most instances the clinical history and examination will indicate whether an alternative diagnosis is likely.
Table 21.2 Traps10: simulated pulmonary nodules.
NODULES—CXR FEATURES
Particular appearances will suggest a fairly limited differential diagnosis(Table 21.3).
Table 21.3 Features and potential diagnoses.
| Morphology | The possibilities |
|---|---|
| Calcified nodules | |
| Cavitating nodules | |
| Beware |
NODULES—A RULE OR TWO
Several useful rules of thumb can be applied (Table 21.4).
Table 21.4 Particular pathologies — CXR features.
| Pathology | Features |
|---|---|
| Metastases | |
| Abscesses | |
| Rheumatoid nodules |

Figure 21.2 Multiple nodules. Metastases from a renal cell carcinoma. The appearances are typical of metastases–rounded lesions with fairly well-defined margins.
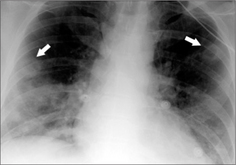
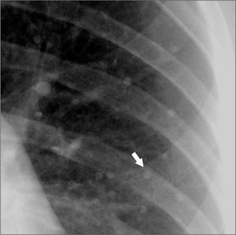
Figure 21.3 Multiple nodules. Male. Age 38. Intravenous drug user. Endocarditis. Lung abscesses. Two of the nodules are cavitating (arrows).
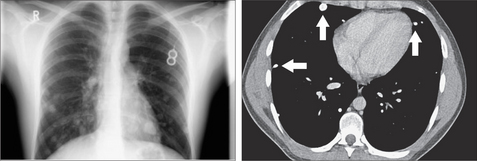
Figure 21.4 Multiple small nodules. Some are much smaller than 10 mm but are readily visible. This suggests that they are calcified. Indeed, they do contain calcification as shown on the CT section (arrows). Secondary tumours from a primary osteogenic sarcoma.
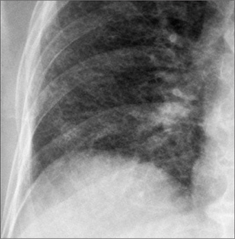
Figure 21.5 Multiple miliary nodules. Tuberculosis. These very small densities (2 mm diameter) are visible because the lung interstitium has hundreds/thousands of exceptionally tiny lesions superimposed one in front of another.

Figure 21.6 Male. Cavitating nodules. Metastatic lesions from a primary tumour of the larynx. Metastases that cavitate are usually squamous cell lesions: in men, frequently a head and neck primary tumour; in women, often carcinoma of the cervix.
INTERESTING NODULES—CHICKENPOX INFECTION11
Aetiology/pathology
Highly infectious viral infection (varicella). Spread by droplet infection/ruptured skin lesions/contact with herpes zoster.
Clinical features
Children are most commonly affected and it is then a relatively mild illness. Infected adults can be very ill. Characteristic rash appears centrally starting on the trunk and spreads centrifugally. In adults, chickenpox pneumonia may occur; it is a very rare complication in children. Pneumonia can be debilitating and occasionally fatal, particularly in immunocompromised individuals.
1. Glossary of terms for thoracic radiology: recommendations of the Nomenclature Committee of the Fleischner Society. AJR. 1984;143:509-517.
2. Zitting AJ. Prevalence of Radiographic small lung opacities and pleural abnormalities in a representative adult population sample. Chest. 1995;107:126-131.
3. Reed JC. Chest Radiology: Plain Film Patterns and Differential Diagnosis, 5th ed., Philadelphia, PA: Mosby; 2003:259-286.
4. Collins SJ, Stern EJ. Chest Radiology: The Essentials. Philadelphia, PA: Lippincott Williams & Wilkins, 1999;96-105.
5. Felson B. Chest Roentgenology. Philadelphia, PA: WB Saunders, 1973.
6. Fraser RG, Muller NL, Colman NC, Pare PD. Fraser and Pare’s Diagnosis of Diseases of the Chest, 4th ed. Philadelphia, PA: WB Saunders, 1999.
7. Huang RM, Naidich DP, Lubat E, et al. Septic pulmonary emboli: CT–radiographic correlation. AJR. 1989;153:41-45.
8. Seo JB, Im JG, Goo JM, et al. Atypical pulmonary metastases; spectrum of radiologic findings. Radiographics. 2001;21:403-417.
9. Frazier AA, Rosado-de-Christenson ML, Galvin JR, et al. Pulmonary angiitis and granulomatosis: radiologic–pathologic correlation. Radiographics. 1998;18:687-710.
10. Gronner AT, Ominsky SH. Plain film radiography of the chest: findings that simulate pulmonary disease. AJR. 1994;163:1343-1348.
11. Sargent EN, Carson MJ, Reilly ED. Roentgenographic manifestations of varicella pneumonia with post mortem correlation. AJR. 1966;98:305-317.