Small Animal Vertebral Column
Marg Brown RVT, BEd Ad Ed
The best lightning rod for your protection is your own spine.
—Ralph Waldo Emerson, American essayist and poet, 1803–1882
- 1. Describe the common positions and principles used to radiograph the small-animal vertebral column.
- 2. Properly and safely position a dog or cat for the various common positions of the vertebral column with an emphasis on nonmanual restraint.
- 3. Correctly measure and center the patient to include the peripheral borders.
- 4. Ensure that the body part is parallel to the image receptor and the central ray is perpendicular to both the field of view (FOV) and receptor.
- 5. Identify other views that may need to be completed as an alternative.
- 6. Identify normal spinal anatomy found on a radiograph.
Key Terms
Key terms are defined in the Glossary on the Evolve website.
Coned-down view
Diverge
Dynamic
Flexed lateral
Hyperextension
Hyperflexion
Kyphosis
Orthogonal
Positioning terminology
Survey
Vertebral formula

Technical Note:
To preserve space, the radiographs presented in this chapter do not show collimation. For safety, always collimate so that the beam is limited within the image receptor edges. In film radiography, you should see a clear border of collimation (frame) on every radiograph. In some jurisdictions, evidence of collimation is required by law.
Survey axial skeletal imaging does have limited diagnostic value in neurological disease and may be insufficient in conditions of the vertebral column, such as trauma. Definitive evidence may need to be obtained by myelography, computerized tomography (CT), or magnetic resonance imaging (MRI).1,2 When these modalities are available, they have largely replaced radiography for spinal disease/trauma diagnosis in referral practices.
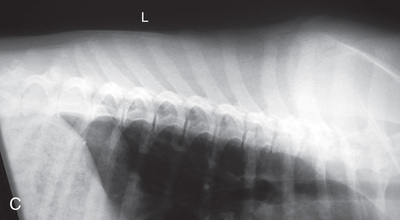
However, in spite of the limitations, proper survey vertebral radiographs are a valuable tool for those patients who have suffered spinal injuries and present with paresis or paralysis, either partial or complete. In addition, survey radiographs can demonstrate many of the signs consistent with intervertebral disk protrusion. Common intervertebral disk protrusion sites are T12 to T13, T13 to L1, C2 to C3, and C3 to C4.1
High-quality images are needed to see subtle changes in bone opacity, shape, and angulation of the vertebrae or vertebral column1,2 (Table 20.1). The common views of this portion of the axial skeleton are the lateral (L) and ventrodorsal (VD) views of the cervical, thoracic, thoracolumbar, lumbar, lumbosacral, sacral, and caudal vertebrae. Depending on the size of the patient, a full survey study is either four or five images of each orthogonal view.
TABLE 20.1
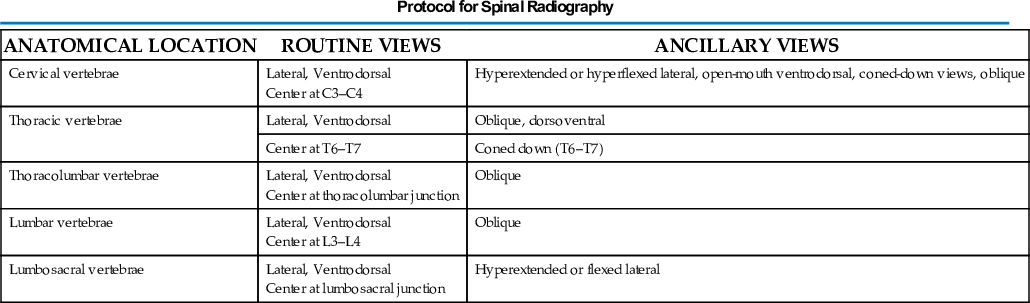
- • Survey radiographs of a large dog center at C3 to C4, T6 to T7, thoracolumbar, L4, and lumbosacral
- • Small dog survey radiographs center at C3 to C4, T6 to T7, L4, and lumbosacral
Cat survey studies of the vertebrae are often part of the whole-body view. For both the dog and the cat, coned-down views are important for areas of interest. Dynamic views of the vertebrae are not common in cats but can be completed.
See Appendix D on the Evolve website for information on the vertebral number and characteristics of the vertebrae of some common species.
Radiographic Concerns
- • Each of the vertebral segments and adjacent intervertebral disks generally need to be examined, so correct positioning and attention to detail are essential to produce images of diagnostic value. This means centering the primary beam on the particular area of interest and tightly collimating immediately adjacent to the spine to increase the detail and contrast.
- • Remember that the x-ray beam diverges from the central ray, so it is important to use smaller cassettes and take multiple views. Limit the number of vertebrae examined so that the intervertebral disk spaces are more perpendicular to the central beam. The farther away the area of interest is from the central beam, the greater the geometrical variation and the more inaccurate the interpretation of that area. Intervertebral spaces at the periphery of radiographs often appear falsely narrowed.3 Coned-down views give further high-quality images.
- • Having the anatomy parallel to the image receptor and perpendicular to the center of the beam is also essential for accurate diagnosis.
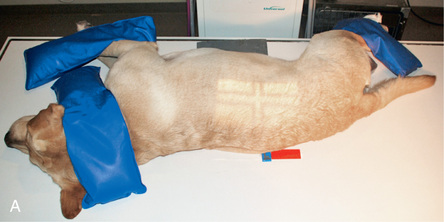
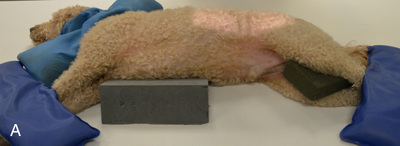
- • Tape placed along the spine may assist in proper alignment4 (Fig. 20.1).
 FIG. 20.1 Placing tape along the vertebrae helps maintain correct alignment and position. A small foam pad under the nose may be required. A line drawn between the greater trochanters should be perpendicular to the table.
FIG. 20.1 Placing tape along the vertebrae helps maintain correct alignment and position. A small foam pad under the nose may be required. A line drawn between the greater trochanters should be perpendicular to the table. - • Use sponges or cotton padding between the limbs and under the sternum to keep the spine parallel to the tabletop, avoid any sagging, and prevent axial rotation.
- • Sandbags can also be used for positioning on areas that will not be in the field of view.
- • For patients without spinal cord injuries, pulling and supporting the front and hind limbs in opposite directions keeps the thoracolumbar vertebral column extended to a near-parallel position, as well as opening the intervertebral spaces.1-3
- • Tape placed along the spine may assist in proper alignment4 (Fig. 20.1).
- • Choose a high-detail cassette/film combination if film is used. Low kilovoltage (kV) and high milliampere-seconds (mAs) provide better radiographic contrast, and the use of a grid further increases the contrast. Ensure there is enough kV for penetration and mAs for film darkening or signal (digital film).
- • If using digital imaging, utilize appropriate algorithms to process raw data to prevent a sudden transition between bone and soft tissue that can create an artificial dark halo around the vertebrae.2
- • The directional and identification labels should be in the field of view, but be conscious of overlapping the label on important anatomy, especially in VD views.
- • The hair coat should be clean and dry. Remove the collar for any cranial and cervical views. The bladder and colon should be emptied, as material within the colon or a distended bladder can create multiple superimposed shadows that might interfere with diagnosis.
- • Generally it is more comfortable for right-handed radiographers to place the dog or cat in right lateral recumbency, but either side can be dependent.
- • General anesthesia should be used to achieve accurate positioning with muscle relaxation; otherwise false narrowing of the intervertebral disk spaces due to muscle spasm may occur.1,2,5
- • Because most feline patients requiring vertebral radiography likely present with spinal injury, sedation or general anesthesia and gentle handling are needed.
- • If trauma is suspected, ensure that any concurrent issues such as thoracic pathology are addressed before obtaining the radiography.
- • If the patient is compromised, VD views can also be made using the horizontal cross-table beam with the patient in lateral recumbency. This is especially useful if vertebral body fractures are suspected.
- • Dorsoventral (DV) views (ancillary view) are not as accurate because of the increase in object-film distance (OFD). Also, it may be more difficult to obtain a parallel technique if the animal is in the DV position.
- • Hyperflexion and hyperextension views (ancillary views) can further evaluate the caudal aspect of the lateral cervical and the lumbosacral vertebrae if the patient is chemically restrained and will not be traumatized by such handling. Be extremely gentle with handling.
 Technician Notes
Technician Notes
To understand the importance of and to demonstrate the optical illusion of variation in spacing that occurs farther from the central beam, evenly place a row of pennies on a 5-cm sponge about half an inch (1.5 mm) apart along the center length of the image receptor. Take an x-ray (suggested technique of 50 kV and 2 mAs) and look at the image. On the resulting image notice how the spacing between the pennies appears to distort as they progress toward the outside edges of the film.
Technician Notes
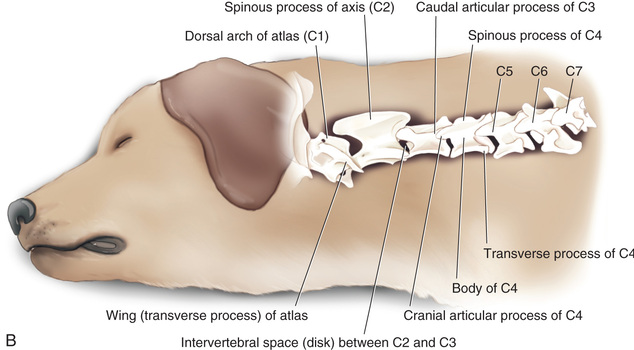
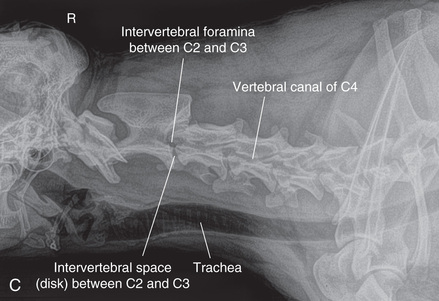
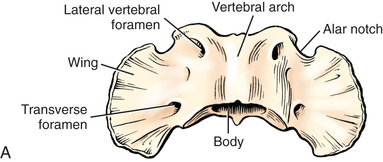
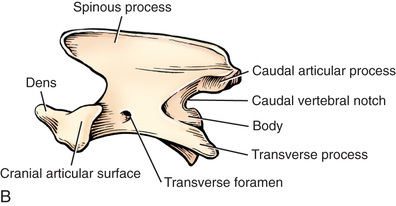
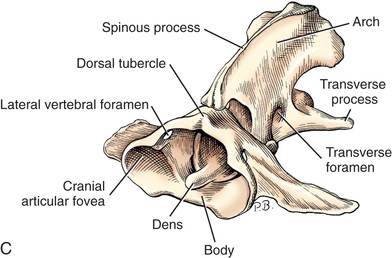
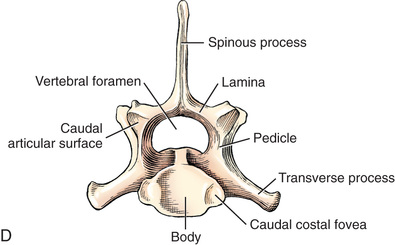
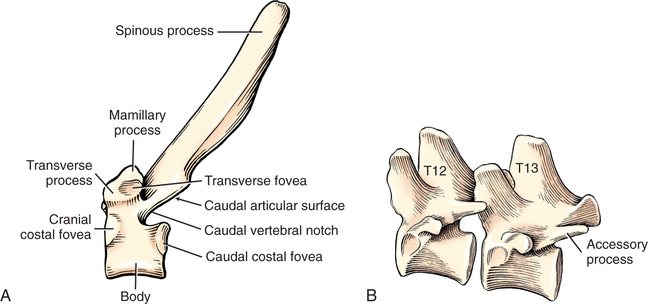
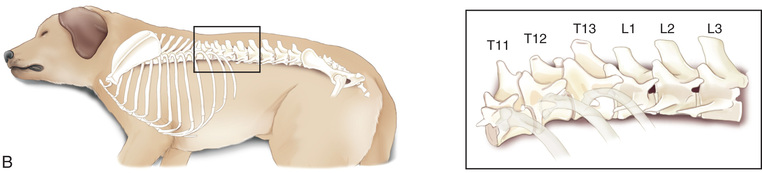
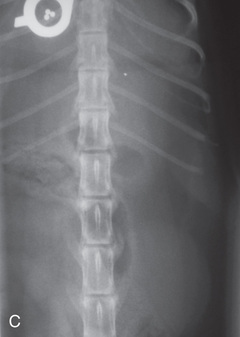
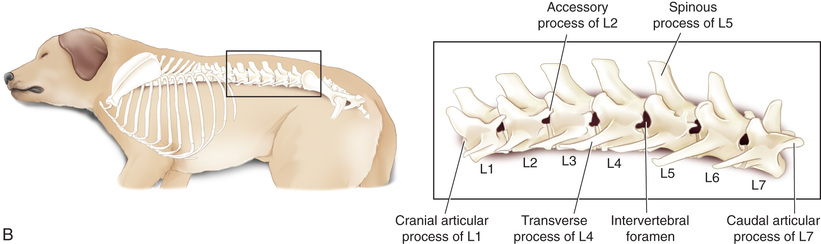
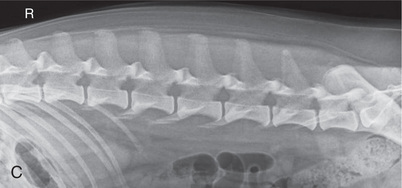
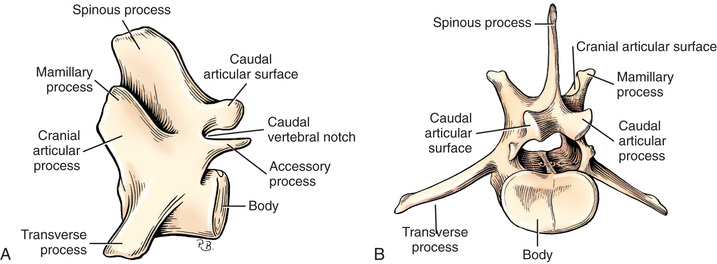
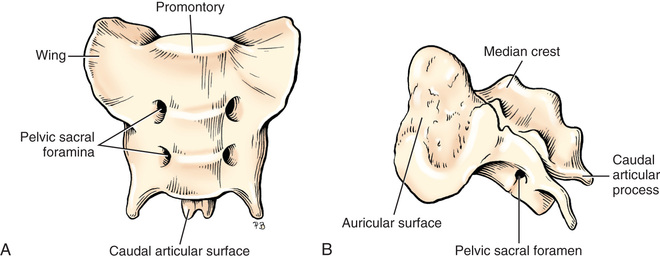
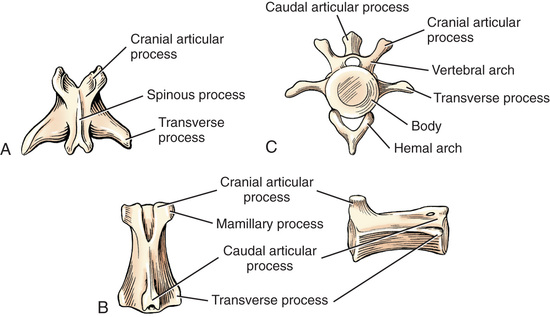
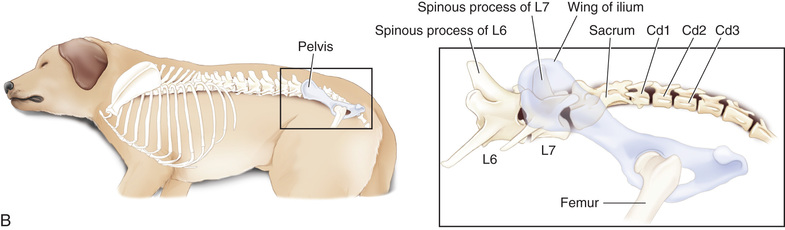
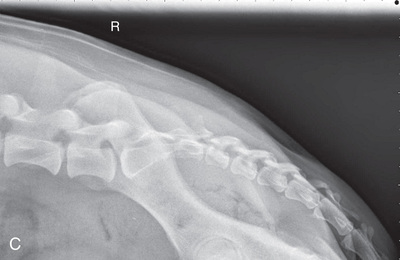
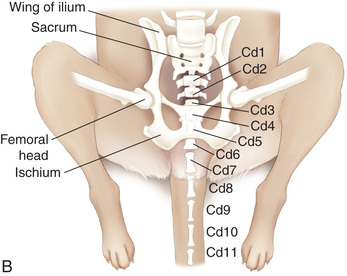
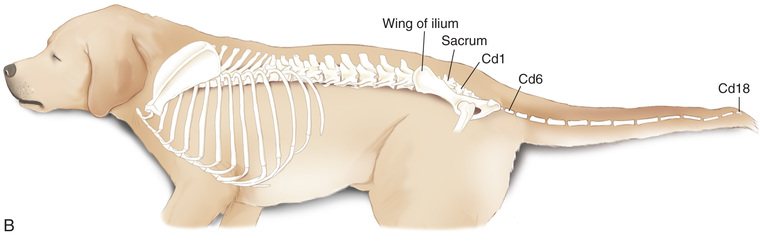
In general, each vertebra is made up of a body (the denser ventral portion, which is separated from the bodies of adjacent vertebra by intervertebral disks), vertebral arch (located dorsal to the body), and various processes (the cranial and caudal articular processes, the dorsal spinous process, and the lateral transverse process) (see Figs. 20.3, 20.9, 20.16, and 20.17).
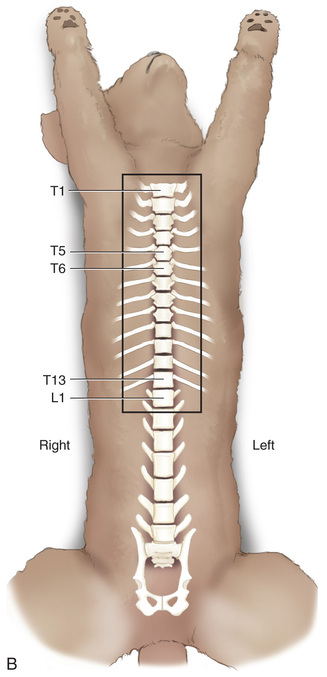
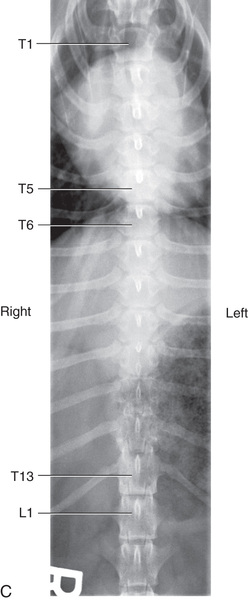
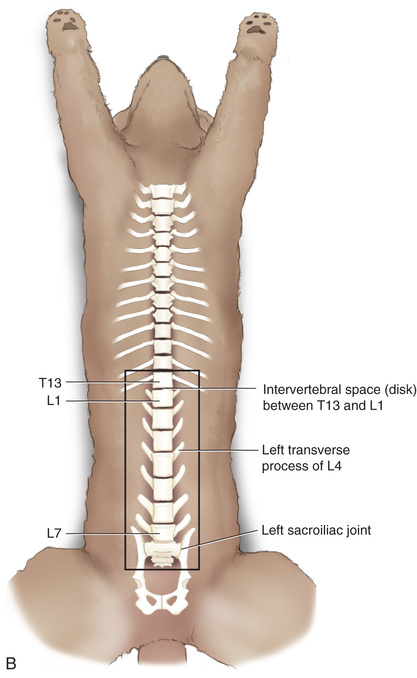
The first letter designating each group, followed by the number of vertebrae in each group, is the vertebral formula. The vertebral formula for a dog and cat is C7T13L7S3Cd6-20.
Technician Notes
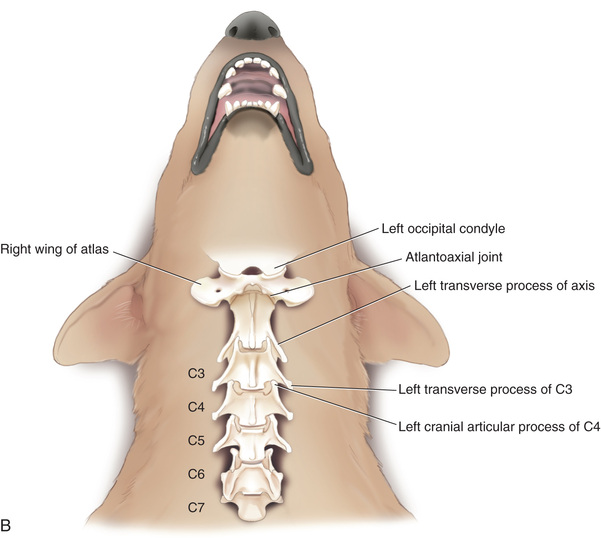
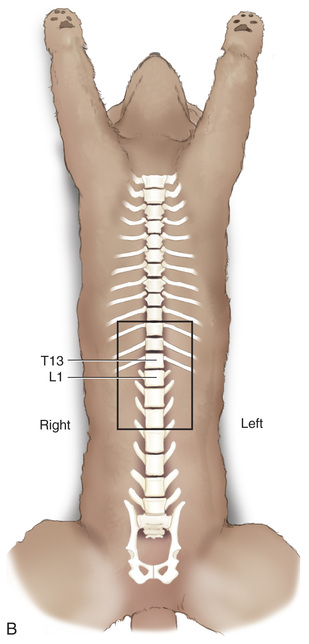
The vertebral column is divided into five regions: cervical (neck), thoracic (chest), lumbar (abdomen), sacral (pelvis), and caudal (tail). To refer to a particular vertebra, use abbreviations for the region followed by the number within the region, beginning at the cranial end. For example, T12 is the twelfth thoracic vertebra. The abbreviation for caudal vertebrae is Cd (although sometimes the tail vertebrae are referred to as coccygeal and the abbreviation is Cy).
Technician Notes
Note that the positioning itself is fairly similar for most of the lateral and ventrodorsal views of the vertebrae. Keep important principles in mind.
Technician Notes
Remember to collimate tightly to the vertebrae. Place the label/marker on the dorsal aspect for the lateral views. For VD views, tape the marker on the body or place it on the table in an area that will not obscure important anatomy.
Cervical Vertebrae
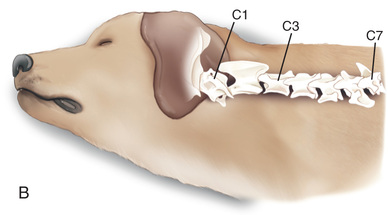
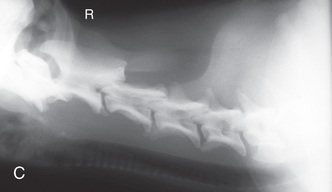
Lateral View of the Cervical Vertebrae—Routine
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and place the pelvic limbs caudally; secure with a sandbag.
- Forelimbs: Position and superimpose the forelimbs caudally; secure with a sandbag.
- A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: Extend the head and elevate the nose using a sponge. Keep the head in a true lateral position. To see if the head is in a true lateral, draw an imaginary line between the medial canthi, and make sure this line is perpendicular to the table. Place a flat positioning device under the midcervical area if it is sagging. Support the cranial area of the head with a sandbag, or secure it with tape/Velcro strapping. Place sponges under the sternum to achieve true alignment with the vertebrae.
- Vertebrae: Use foam pads or cotton beneath the cervical vertebrae to keep them parallel to the table.
Comments and Tips
- • Keep the spine parallel to the table—the transverse processes of each vertebra should be superimposed on the image.
- • A separate image of the cervicothoracic junction may be required to better evaluate this region.1
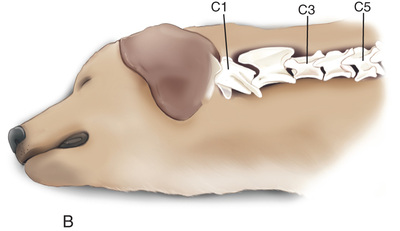
- • The head must be in a true lateral position because any obliquity of the head can change the position of the cranial cervical vertebrae.
- • Try to keep true lateral positioning of the entire body even if radiographing only the cervical area.
- • Do not overextend the limbs because doing so might cause rotation of the spine.
- • Do not flex or extend the head.
- • To help align the cervical vertebrae with the long axis of the image receptor, position the pelvis region dorsally in a line with the head.
- • Larger canine patients may have to be radiographed in two sections for the lateral and ventrodorsal cervical vertebrae:
Examples
MEASURE: Across the shoulder at the level of C6 to ensure adequate penetration of the caudal cervical vertebrae. Overexposure may occur with the cranial cervical vertebrae. Coned-down views can be made of these areas.
CENTRAL RAY: C3 to C4.
BORDERS: Base of the skull to the spine of the scapula (just past the shoulder joint, about T2, to include the cervical vertebrae). Collimate tightly to the edge of the wings of the atlas and the center of the spine of the scapula.
Technician Notes
Strategically used positioning aids give the patient the illusion that it is being held.
Technician Notes
Pulling the front limbs caudally prevents shoulder soft tissue from overlapping the spine.
Technician Notes
Be extra careful when manipulating small-breed dogs that present with apparent neck pain.
Technician Notes
Quickly go through your mental checklist before pushing the exposure button: settings correct; image receptor/machine/grid in position; proper location of markers and ID (if using at this stage); correct body part and view; properly centered; borders correct and collimated; patient properly prepared, positioned, and restrained so the vertebrae are in the same horizontal plane as the sternum for the lateral and superimposed for the VD, and parallel to the image receptor. The central ray is perpendicular to the field of view and the receptor.
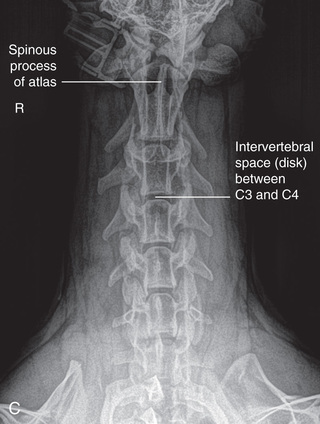
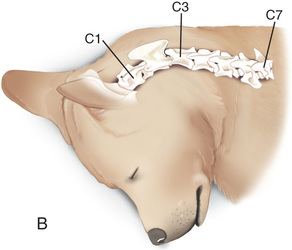
Ventrodorsal View of the Cervical Vertebrae
Positioning

- Place In: Dorsal recumbency in a V-trough or supported by tape/Velcro strapping or sandbag if needed.
- Hind Limbs: Place the pelvic limbs in a neutral position and secure with sandbags.
- Forelimbs: Evenly position the forelimbs caudally and secure with a sandbag.
- Head/Neck/Sternum: Keep the head in a natural position with the nose slightly up to minimize the curvature of the cervical spine. Secure with padding lateral to the head and neck. Keep the sternum superimposed over the vertebrae.
- Vertebrae: Use padding beneath the rostral neck to keep the cervical vertebrae parallel to the table.
Comments and Tips
- • If possible, angle the beam in a slight caudocranial direction (20 degrees) between the intervertebral spaces to improve visualization of the disk spaces because they slope caudally in the VD position.
- • Make sure that the sternum and vertebrae are superimposed and perpendicular to the image receptor to minimize rotation.
- • The nose should be in line with the base of the tail with the limbs positioned evenly.
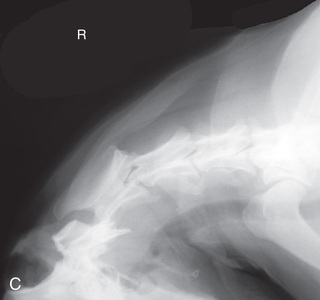
- • If there is an interest in the occipital bone, point the nose upward and secure with sandbags lateral to the head and neck so that there is no bone superimposition of C1 to C2 with the occipital bone.
- • As this is often the last view made, the endotracheal tube may need to be removed before the image is taken to avoid artifacts that might interfere with diagnosis.
- • An open-mouth view of the odontoid process can be made as described in Chapter 21.
Examples
MEASURE: Level of C6 near the manubrium.
CENTRAL RAY: C3 to C4.
BORDERS: Base of the skull to just past the shoulder joint to about T2, with tight collimation laterally.
Hyperextended Lateral View of the Cervical Vertebrae—Ancillary
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and place the pelvic limbs caudally; secure with a sandbag.
- Forelimbs: Position and superimpose the forelimbs caudally; secure with a sandbag. A small foam pad may be placed between the limbs.
- Head/Neck/Sternum: Elevate and keep the nose level to the table, using a foam pad. To see if the head is in a true lateral, draw an imaginary line between the medial canthi, and make sure this line is perpendicular to the table. Hyperextend the neck and head dorsally and caudally until resistance is met. Support the cranial area of the head with a sandbag, or secure with tape/Velcro strapping. Place foam pads under the sternum to achieve true alignment with the vertebrae.
- Vertebrae: Use a foam pad or cotton beneath the cervical vertebrae as needed to keep each vertebra parallel to the table.
Comments and Tips
- • For true hyperextension, all cervical vertebrae need to be extended dorsally.
- • As with other cervical laterals, the head must be in a true lateral position; keep true lateral positioning of the entire body using proper padding, and do not overextend the limbs.
- • Collimate tightly so that a coned-down view is obtained.
- • If an endotracheal tube is present, be careful that the patient's breathing is not restricted at any point.
- • The hyperextended view is usually completed before the flexion to determine if the latter is required.
- • The hyperextended and hyperflexed views are referred to as dynamic views and are usually completed after myelography to note any spinal cord impingement due to extradural changes associated with vertebral instability.2 Be very cautious with the procedures to prevent further injury.
Examples
MEASURE: C3 to C4 intervertebral space across the neck.
CENTRAL RAY: C3 to C4 intervertebral space.
BORDERS: Base of the skull to the spine of the scapula (just past the shoulder joint). Collimate tightly to the edge of the wings of the atlas and the center of the spine of the scapula.
Flexed Lateral View of the Cervical Vertebrae—Ancillary
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and position the pelvic limbs caudally; secure with sandbags.
- Forelimbs: Position and superimpose the forelimbs ventrally and caudally, and secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: Place tape or thin rope around the nose or canine teeth, and gently apply traction on the end so the neck and head are flexed. Pull the tape caudally between the forelimbs close to the body, and secure to a sandbag. If needed, elevate the nose using a sponge so the head is in true lateral. Draw an imaginary line between the medial canthi, and make sure this line is perpendicular to the table. A sandbag can be placed dorsal to the nose to maintain the hyperflexed position. Place sponges under the sternum to achieve true alignment with the vertebrae.
- Vertebrae: If needed, use sponges beneath the cervical vertebrae to keep the spine parallel to the table and at the same plane as the thoracic vertebrae.
Comments and Tips
- • For true flexion, all cervical vertebrae need to be flexed.
- • As with other cervical laterals, the head must be in a true lateral position; keep true lateral positioning of the entire body using proper padding, and do not overextend the limbs.
- • The flexed lateral dynamic view is generally used to assess small-breed dogs with suspected subluxation.2
- • Begin with the mildest extension that will demonstrate instability, as marked flexion may further damage the spinal cord.
- • Collimate tightly so that a coned-down view is obtained for less distortion and better contrast.
- • The radiographs should only be taken with the patient under general anesthesia and placement of an endotracheal tube. Be careful with hyperflexing the neck so as not to cause tracheal trauma or constriction of the endotracheal tube.
Examples
MEASURE: C3 to C4 intervertebral space across the neck.
CENTRAL RAY: C3 to C4 intervertebral space.
BORDERS: Base of the skull to the spine of the scapula (just past the shoulder joint). Collimate tightly to the edge of the wings of the atlas and the center of the scapular spine.
Lateral Oblique View for the Odontoid Process—Ancillary
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and place the pelvic limbs caudally; secure with a sandbag.
- Forelimbs: Position and superimpose the forelimbs caudally; secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: Use tape/Velcro strapping to keep the head in its natural oblique position.6 Place sponges under the sternum so it is on the same plane as the thoracic vertebrae.
- Vertebrae: Use padding to keep the cervical vertebrae lateral and the head and C1 oblique.
Examples
MEASURE: C1 (for odontoid process).
CENTRAL RAY: C1 (for odontoid process).
BORDERS: Midskull to C4.
Thoracic Vertebrae
Lateral View of the Thoracic Vertebrae—Routine
Positioning

- Place In: Lateral recumbency with pelvis moved ventrally to straighten the thoracic spine.
- Hind Limbs: Superimpose and place the pelvic limbs caudally; secure with a sandbag. A small foam pad can be placed between the limbs.
- Forelimbs: Superimpose and cranially position the forelimbs slightly; secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: Keep the head in a natural position, and support the neck with a sandbag. If needed, use sponges under the sternum and between the limbs to achieve true alignment of the sternum and vertebrae.
- Vertebrae: Use padding if needed to keep each thoracic vertebra on the same horizontal plane as the sternum. Using tape as in Fig. 20.1 can assist with proper alignment.
Comments and Tips
- • Try to keep lateral positioning of the entire body even if radiographing only the thoracic area.
- • Collimate tightly laterally.
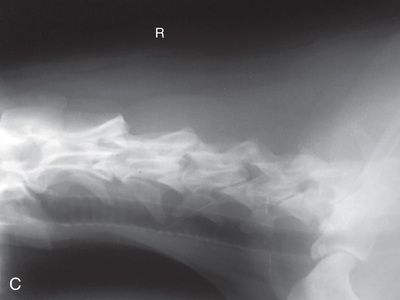
- • The pelvis should be positioned ventrally so that the thoracic vertebrae are aligned with the long axis of the image receptor. In the mid-to-caudal thoracic vertebrae region, dogs and cats have a natural area of kyphosis.1
- • The ribs should be superimposed over each other so that the intervertebral spaces are better viewed, and the sternum should be on the same plane as the vertebrae. Use foam pads appropriately.
- • Large dogs may require two separate views.
- • Placing a lead mask or saline bag dorsal to the thoracic spine helps prevent scattered/secondary radiation from darkening the spinous processes in large dogs.
Examples
MEASURE: Highest point of the midthorax.
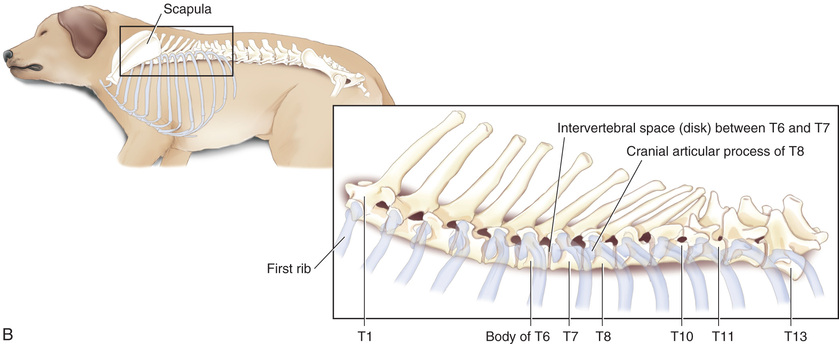
CENTRAL RAY: T6 to T7 or the caudal border of the scapula.
BORDERS: From C7 to L1 inclusive (shoulder joint to past the origin of the last rib).
Technician Notes
Placing padding under the nose and the natural curvatures of the spine (neck and lumbar regions) and between the limbs for all lateral positions will keep the spine parallel and horizontal with the table/image receptor and perpendicular to the center ray.
Keep a true lateral position of the entire body for each view, and keep the sternum and vertebrae on the same plane, parallel to the table and perpendicular to the x-y beam and receptor.
Ventrodorsal View of the Thoracic Vertebrae—Routine
Positioning

- Place In: Dorsal recumbency in a V-trough or use sandbags, if needed, to prevent rotation.
- Hind Limbs: Equally place the pelvic limbs in a neutral position; secure with sandbags.
- Forelimbs: Equally position the forelimbs cranially and tie or secure with sandbags.
- Head/Neck/Sternum: The head and neck are best positioned with the nose parallel to the table and equidistant between the limbs. Support with ties or a sandbag, being careful not to restrict breathing.
- Vertebrae: Superimpose the sternum and vertebrae to minimize any rotation.
Comments and Tips
- • Ensure that there is a straight line from the tip of the nose to the base of the tail to achieve rib symmetry on the image.
- • Large dogs may require two separate views.
- • The symmetry of the normal patient is noted on an image when the spinous processes are evident on the midvertebral body and the sternum is superimposed over the vertebrae.
Thoracolumbar Vertebrae
Lateral View of the Thoracolumbar Vertebrae—Routine
Positioning
- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and place the pelvic limbs caudally; secure with a sandbag.
- A small foam pad can be placed between the limbs.
- Forelimbs: Superimpose and cranially position the forelimbs slightly; secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: If needed, use foam pads under the sternum to achieve true alignment with the vertebrae. Keep the head in a natural position and support the neck with a sandbag, being careful not to restrict breathing.
- Vertebrae: Keep the thoracolumbar vertebrae on the same plane as the sternum. Using tape as in Fig. 20.1 can assist with proper alignment.
Comments and Tips
- • Try to maintain true lateral positioning of the entire body even if radiographing only the thoracolumbar area.
- • Collimate tightly. The vertebrae should be limited to four on either side of the thoracolumbar junction. If interested in both the thoracic and lumbar vertebrae, each area should be radiographed separately so that the number of vertebrae are limited.
- • The ribs should be superimposed over each other so that the intervertebral spaces are better viewed, and the sternum should be at the same distance from the table as the vertebrae.
- • On the image the intervertebral foramina should be superimposed, and they should be of equal sizes from the thoracolumbar junction toward the sacrum.
Ventrodorsal View of the Thoracolumbar Vertebrae—Routine
Positioning

- Place In: Dorsal recumbency in a V-trough or use sandbags, if needed, to prevent rotation.
- Hind Limbs: Place the pelvic limbs in a neutral position; secure with sandbags if needed.
- Forelimbs: Position the forelimbs cranially; tie or secure with sandbags.
- Head/Neck/Sternum: The head and neck can be in a natural position. If needed, support with a sandbag, being careful not to restrict breathing. The nose should be equidistant between both front limbs.
- Vertebrae: Have the sternum and vertebrae superimposed to minimize any rotation.
Comments and Tips
- • Ensure that there is a straight line from the tip of the nose to the base of the tail.
- • Collimate tightly. If interested in both the thoracic and lumbar vertebrae, each area should be radiographed separately so that the number of vertebrae are limited. See Box 20.1 to ensure you have proper symmetry on the image.
Examples
MEASURE: Highest point of the midthorax.
CENTRAL RAY: T13 to L1 intervertebral space.
BORDERS: Xiphoid to the caudal portion of last rib (about T10–L3).
Technician Notes
Provide enough support with a V- trough, foam pads, or sandbags to prevent any axial rotation. The spine and sternum must be superimposed perpendicular to the table and plate for the ventrodorsal view; and on the same horizontal plane, parallel to the table and plate, for the lateral views.
Technician Notes
Collimate tightly to include the transverse process and muscle mass, but do not include the fat and skin.
Lumbar Vertebrae
Lateral View of the Lumbar Vertebrae—Routine
Positioning
- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and place the pelvic limbs slightly caudally; secure with a sandbag. A small foam pad can be placed between the limbs.
- Forelimbs: Superimpose and position the forelimbs slightly cranially; secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: If needed, use foam pads under the sternum to achieve true alignment with the vertebrae. Keep the head in a natural position; support the neck with a sandbag, being careful not to restrict breathing.
- Vertebrae: Keep each lumbar vertebra parallel to the table and image receptor and on the same horizontal plane as the sternum. Using tape as in Fig. 20.1 can assist with proper alignment.
Comments and Tips
- • Try to maintain true lateral positioning of the entire body even if radiographing only the lumbar area.
- • Collimate tightly.
- • See Box 20.1 to ensure you have proper symmetry on the image.
Examples
MEASURE: Level of L1.
CENTRAL RAY: L3 to L4 (palpate).
BORDERS: T12 to S1 (Just cranial to origin of last rib to just before the greater trochanter).
Ventrodorsal View of the Lumbar Vertebrae—Routine
Positioning


- Place In: Dorsal recumbency in a V-trough or use sandbags, if needed, to prevent rotation.
- Hind Limbs: Place the pelvic limbs in a neutral position; secure with sandbags if needed.
- Forelimbs: Position the forelimbs cranially and secure with a sandbag if needed.
- Head/Neck/Sternum: The head can be in a natural position.
- Support with a sandbag, being careful not to restrict breathing.
- Position the nose equidistant between the forelimbs.
- Vertebrae: Superimpose the sternum and vertebrae to prevent any rotation.
Examples
MEASURE: Level of L1.
CENTRAL RAY: Level of L4 (palpate).
BORDERS: T12 to S1 (Just cranial to both the origin of the last rib and acetabulum).
Technician Notes
Extending the forelimbs and hind limbs and securing them provide further support to help avoid rotation of the spine in the VD position.
Lumbosacral Vertebrae
Lateral View of the Lumbosacral Vertebrae—Natural Positioning—Routine
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and position the pelvic limbs slightly caudally, with a foam pad between them; secure with sandbags. Ensure that the wings of the ilia are superimposed and parallel to the image receptor by placing padding under the upper limb.
- Forelimbs: Superimpose and cranially position the forelimbs slightly; secure with a sandbag. A small foam pad can be placed between the limbs.
- Head/Neck/Sternum: Use foam pads under the sternum to achieve true alignment with the vertebrae. Keep the head in a natural position; support the neck with a sandbag, being careful not to restrict breathing.
- Vertebrae: Use padding to keep each lumbar vertebra parallel to the table and the image receptor.
Comments and Tips
- • Use the pelvis technique chart to ensure adequate penetration.
- • See Box 20.1 to ensure you have proper symmetry on the image.
- • Ancillary views of the lumbosacral include hyperextended and hyperflexed views of the vertebrae.
Examples
MEASURE: Level of the lumbosacral junction or the highest point of the wings of the ilia.
CENTRAL RAY: Level of the lumbosacral junction (just caudal to the wings of the ilia).
BORDERS: L4 to the most cranial caudal vertebra (just cranial to the wings of the ilia to the femoral head).
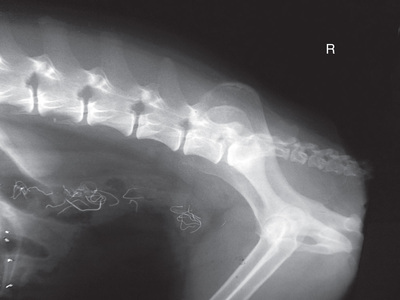
Lateral View of the Lumbosacral Vertebrae—Ancillary
Comments and Tips
- • These views are used to demonstrate lumbosacral instability.
- • The measuring, centering, borders, and positioning is exactly the same as for the lateral view except for positioning of the hind limbs:
- • For the hyperextended view (Fig. 20.19A): hyperextend the superimposed hind limbs as far caudally as possible, placing a sandbag over them to hold in position.
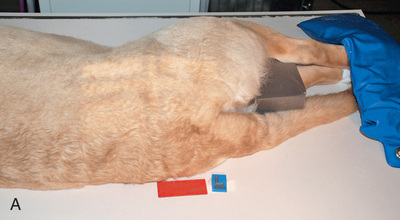
 FIG. 20.19 A, Positioning for the lateral view of the lumbosacral vertebrae—hyperextended view. B, Positioning for the lateral view of the lumbosacral vertebrae—hyperflexed view.
FIG. 20.19 A, Positioning for the lateral view of the lumbosacral vertebrae—hyperextended view. B, Positioning for the lateral view of the lumbosacral vertebrae—hyperflexed view. - • For the hyperflexed view (Fig. 20.19B): position the superimposed hind limbs as far cranially as possible, placing a sandbag over them to hold in position.
- • For the hyperextended view (Fig. 20.19A): hyperextend the superimposed hind limbs as far caudally as possible, placing a sandbag over them to hold in position.
Technician Notes
Collimate, ensuring that labels/markers are included and that borders are visible for every image.
Ventrodorsal View of the Lumbosacral Vertebrae—Routine
Positioning


- Place In: Dorsal recumbency in a V-trough or use sandbags if needed.
- Hind Limbs: Partially extend the pelvic limbs equally in a normal position, and secure with sandbags if needed. The pelvic limbs may be externally rotated.
- Forelimbs: Position the forelimbs cranially and secure with a sandbag.
- Head/Neck/Sternum: The head can be in a natural position. Support with a sandbag, being careful not to restrict breathing.
- Vertebrae: Maintain the sternum and vertebrae in the same vertical plane.
Examples
MEASURE: Wings of the ilia.
CENTRAL RAY: On the lumbosacral junction, caudal to the wings of the ilia, at an angle of 20 to 30 degrees in a caudocranial direction.
BORDERS: L4 to the most cranial-caudal vertebra (from just cranial to the wings of the ilia to the femoral head).
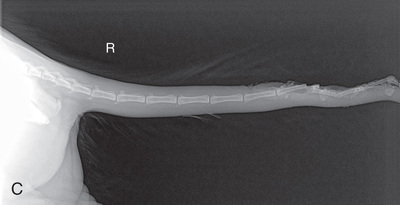
Caudal Vertebrae
Lateral View of the Caudal Vertebrae—Routine
Positioning

- Place In: Lateral recumbency.
- Hind Limbs: Superimpose and pull the pelvic limbs in a neutral position; secure with a sandbag.
- Forelimbs: Superimpose and cranially position the forelimbs slightly; secure with a sandbag if needed.
- Head and Neck: Keep the head in a natural position; support with a sandbag if needed.
- Vertebrae: Place a foam pad to keep the vertebrae parallel to the table. A film cassette can be placed on the foam pad under the tail. Secure the tail to the cassette if needed.
Examples
MEASURE: Thickest part of the tail.
CENTRAL RAY: Area of interest.
BORDERS: Four or five vertebrae on either side of the area of interest, or the full tail.
Ventrodorsal View of the Caudal Vertebrae—Routine
Positioning
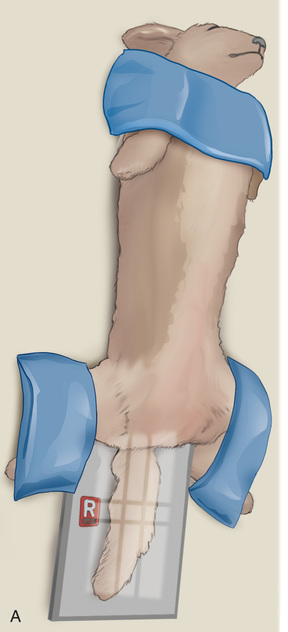

- Place In: Dorsal recumbency in a V-trough or supported by tape/Velcro strapping or sandbag if needed.
- Hind Limbs: Extend the pelvic limbs; secure with sandbags if needed.
- Forelimbs: Position the forelimbs cranially; secure with sandbags if needed.
- Head/Neck/Sternum: The head can be in a natural position. Secure if needed.
- Vertebrae: Secure the tail with tape, if required, and keep it in a straight line with the body.
Examples
MEASURE: Thickest part of the tail.
CENTRAL RAY: Area of interest.
BORDERS: Four or five vertebrae on either side of the area of interest, or the full tail.
Further Ancillary Views
- • A VD view of the spinal column with a vertical beam may not always be feasible because of patient injury or other concerns.
- • Alternatives include a lateral decubitus view, an oblique view, and a DV view (Fig. 20.23).

 FIG. 20.23 A, Positioning for ventrodorsal views of the vertebrae with a horizontal beam. Tightly collimate the beam on the area of interest. B, A dorsoventral view can be obtained if it is difficult to obtain a ventrodorsal view. Object-film distance and magnification will be increased with the dorsoventral view, and the vertebrae are more difficult to keep parallel. Collimate the beam in tightly for spinal radiographs.
FIG. 20.23 A, Positioning for ventrodorsal views of the vertebrae with a horizontal beam. Tightly collimate the beam on the area of interest. B, A dorsoventral view can be obtained if it is difficult to obtain a ventrodorsal view. Object-film distance and magnification will be increased with the dorsoventral view, and the vertebrae are more difficult to keep parallel. Collimate the beam in tightly for spinal radiographs. - • Keep the principles of measuring, centering, and borders in mind for each of the positions described here.
- • Center the beam on the area of interest and collimate.
Lateral Decubitus View of the Vertebrae (Ventrodorsal View With a Horizontal Beam)—Ancillary
- • The VD view can also be achieved using a horizontal beam with the dog in lateral recumbency as described for the thoracic and abdominal views in Chapters 16 and 17.
Oblique View of the Vertebrae—Ancillary
- • To help localize a lesion identified on the lateral or VD views that requires further examination, an oblique view may be requested.
- • Place the patient in dorsal recumbency and rotate the body either to the right or to the left.
- • Use padding under the mandible, cranial sternum, and pelvis to obtain a 30- to 45-degree oblique projection.
- • Both the right and left oblique views should be compared.
Dorsoventral View of the Vertebrae—Ancillary
- • A DV view with the dog in sternal recumbency can also be completed if an orthogonal view is required but the patient would be compromised in VD position or if the machine does not allow a lateral decubitus view. It is more difficult to maintain the vertebrae parallel to the table for a DV, and OFD—and thus magnification—will be increased.
- • For completion of this view, keep a pad under the head so that all the vertebrae are parallel to the table (Fig. 20.23B).
Fig. 20.24 is a mystery radiograph. Review it and answer the question presented with it.
 Key Points
Key Points
- 1. General anesthesia or sedation should be considered for accurate positioning.
- 2. The common views are lateral and VD views of each spinal area. Ancillary views may further assist diagnosis.
- 3. It is essential that each vertebra being imaged is parallel to the table/image receptor and the central ray is perpendicular to both. This minimizes distortion that could lead to misdiagnosis.
- 4. Measure at the thickest part of the area of interest.
- 5. Collimate tightly to the vertebrae, being conscious of the placement of the labels and markers.
- 6. Multiple views are recommended. Limit the number of vertebrae on an image due to the divergence of the x-ray beam.
- 7. If the patient has a spinal column injury, manipulation of the limbs and spine may be contraindicated.
Review Questions
1. The ventrodorsal cervical vertebrae of a Doberman are to be radiographed. It is best to measure:
2. For a radiograph of the lateral cervical vertebrae of the Doberman, sponges can be used to help ensure proper patient positioning. A sponge is not likely needed:
b. Beneath the cervical vertebrae
3. The front limbs of the Doberman for the lateral cervical vertebrae should be:
a. Superimposed and positioned slightly caudally
b. Superimposed and positioned slightly cranially
c. Scissored and positioned slightly caudally
d. Scissored and positioned slightly cranially
4. A flexed lateral view is required for the cervical vertebrae of this Doberman. The cervical vertebrae should be flexed, and:
a. The head should be in a natural oblique position
b. The head should be in a true lateral position
c. The limbs should be extended as far cranial as possible
d. No padding is required under the cervical vertebrae
5. A lateral view of the thoracolumbar vertebrae is required of a Dachshund. You should measure at the:
a. T13 to L1 intervertebral space
b. Cranial border of the scapula
6. The borders for this lateral view of the Dachshund thoracolumbar vertebrae should be at:
a. The xiphoid to the most caudal portion of the last rib
b. The cranial portion of C1 to T6
c. T13 to caudal portion of L1
7. To ensure proper positioning for a ventrodorsal thoracolumbar view:
a. Superimpose the ribs so that the intervertebral spaces are better viewed
b. Place padding under the cervical vertebrae and sternum
c. Place the pelvic limbs over each other in a neutral position, and secure with sandbags
d. Superimpose the sternum over the vertebrae
8. In the lateral view of the TL junction, the label and positional markers should be placed:
a. Ventral to the vertebrae being imaged
b. Dorsal to the vertebrae being imaged
c. At the cranial aspect of the vertebrae being imaged
d. At the caudal aspect of the vertebrae being imaged
9. An Irish Setter is paralyzed. After it is stabilized and appropriate medication administered, the veterinarian wants you to take accurate orthogonal x-rays of the thoracic and lumbar vertebrae, as the veterinarian suspects compression fracture but is concerned about causing further injury. With film radiography you should complete a:
a. Right lateral and right lateral decubitus view
d. Right and left lateral and DV view
10. In radiographing an Irish Wolfhound’s thoracic and lumbar vertebrae for lateral and orthogonal views, you should measure and center at:
a. T6/T7 and L4 to obtain four radiographs total
b. T6/T7, TL junction, and L4 to obtain six radiographs total
c. T6/T7 and L4 to obtain two radiographs total
d. T6/T7, TL junction, and L4 to obtain three radiographs total
11. In radiographing the Irish Wolfhound’s thoracolumbar vertebrae, you should include from:
12. You are checking the lateral lumbar radiographs of the Irish Wolfhound vertebrae to ensure that you are giving the veterinarian properly positioned radiographs. On the lateral image you are looking for:
a. Superimposed intervertebral foramina and transverse processes
b. Equal symmetry of the transverse processes
c. A colon that does not contain any stool
d. Spinous processes that are evident on the midvertebral body
13. To note symmetry on the VD lumbar radiograph of the Irish Wolfhound, you are looking for:
a. Superimposed intervertebral foramina that are of equal size
b. Superimposed pelvic limbs that are slightly positioned caudally
c. Spinous processes that are evident on the midvertebral body
d. A “Nike” swoosh created by the superimposition of transfer processes
14. A cleansing enema performed 1 to 2 hours before exposure is recommended for:
a. The ventrodorsal lumbar and lumbosacral views
b. Lateral and ventrodorsal lumbar and lumbosacral vertebrae views
c. All ventrodorsal vertebrae views
d. All ventrodorsal and lateral vertebrae views
15. Lumbosacral instability is suspected in a Greyhound. Along with the regular lateral the veterinarian will complete dynamic studies after a myelography study. The dynamic study is in reference to:
d. Both hyperextended and hyperflexed views
16. For a hyperextended lumbosacral view, a German Shepherd will be positioned in:
a. Ventral recumbency with a horizontal beam aimed at the lumbosacral junction
b. Lateral recumbency with the hind limbs superimposed and extended quite caudally
c. Lateral recumbency with the hind limbs superimposed and extended quite cranially
d. Dorsal recumbency with the hind limbs superimposed and extended quite cranially
17. Which chart should be used to determine the exposure factors for the lateral lumbosacral vertebrae?
18. If oblique views are to be taken of the vertebrae, the patient should be placed in:
a. Lateral recumbency with 30 to 45 degrees rotation
b. Sternal recumbency with 30 to 45 degrees rotation
c. Dorsal recumbency with 30 to 45 degrees rotation
d. Dorsal recumbency with 15 to 25 degrees rotation
19. A stabilized and paralyzed feline patient had been HBC (hit by car). The veterinarian suspects a complete fracture in the thoracic and lumbar region but wishes to take an initial radiograph to assist the owners to determine if treatment is an option. The veterinarian suggests that for now she would like you to obtain:
a. Right and left lateral radiographs from C1 to S1
b. Right lateral and VD radiographs from C1 to S1
c. Three right lateral radiographs: C1 to L1, T10 to L3, and T12 to S1
d. A right lateral radiograph from the shoulder joint to the pelvis
Chapter Review Question answers are located in the Instructor Resources on Evolve and can be provided to students at the discretion of the Instructor.