Liver and Spleen
Martha Moon Larson
Radiology of the Liver
The liver is the largest solid organ in the abdomen. Changes in hepatic size, shape, location, and opacity are used to assess the liver for possible abnormality.1-8
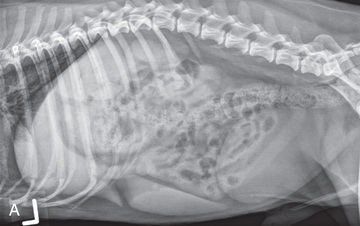
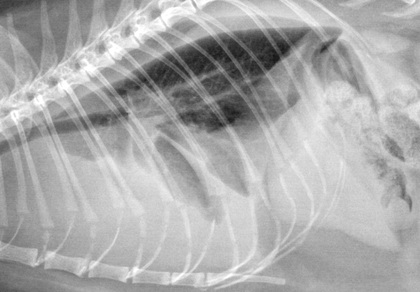
The liver is in the cranial aspect of the abdomen between the diaphragm, which delineates its cranial border, and the stomach, right kidney, and cranial portion of the duodenum, which define the caudal extent. The liver is nearly entirely within the costal arch, with the caudal ventral border, composed of the left lateral liver lobe in the dog, extending just slightly beyond the costal arch (Fig. 40.1). In dogs with a deep thoracic cavity, the liver lies more completely within the costal arch, whereas greater caudal hepatic extension is present in dogs with shallow, wide thoracic conformation. Abundant falciform fat, especially in cats, can result in dorsal displacement of the ventral aspect of the liver on lateral views. On ventrodorsal (VD) views, the liver is distributed symmetrically in dogs, but a larger portion is often right sided in cats (Fig. 40.2).

Hepatic shape may not be visualized without sufficient surrounding omental and falciform fat. The caudoventral hepatic margin protruding slightly from the costal arch should be relatively sharply marginated and triangular. It may protrude farther caudally in right lateral recumbent views, where it may merge with the spleen, blurring exact definition. If lateral views are slightly oblique, the liver can appear to have round margins, which should not be confused with hepatic enlargement.
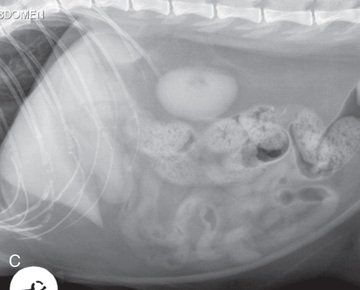
The gallbladder is located just to the right of midline, in the cranioventral portion of the liver, but is not visible normally because of silhouetting with the soft tissue of the liver (Fig. 40.3). In some cats, the gallbladder can be seen on lateral abdominal radiographs as a curved structure protruding from the ventral liver margin (see Fig. 40.3C).9
Hepatomegaly
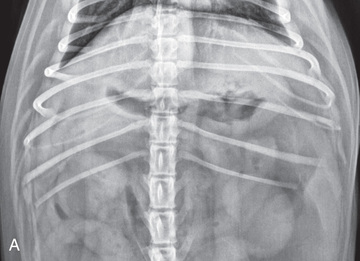
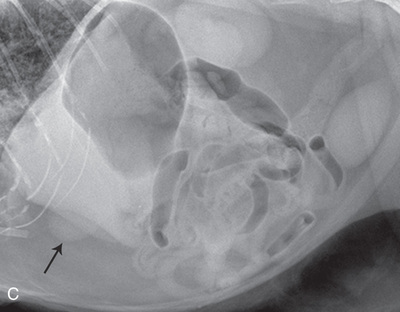
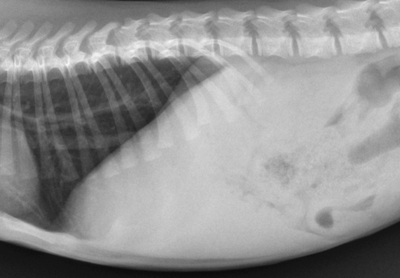
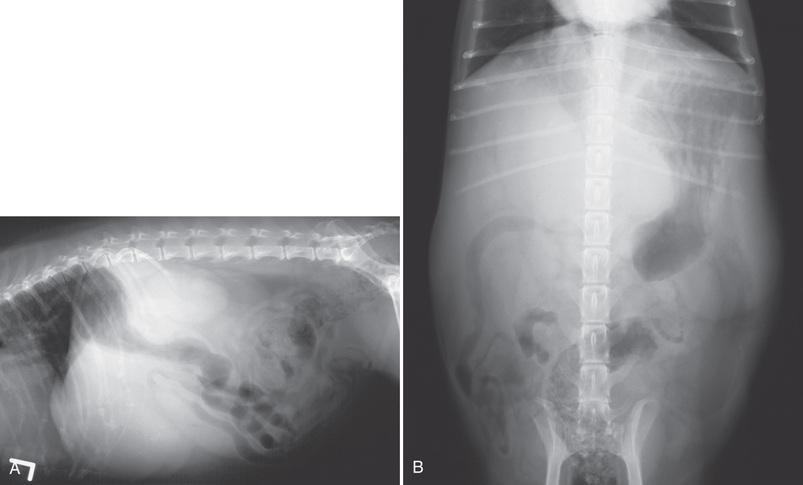
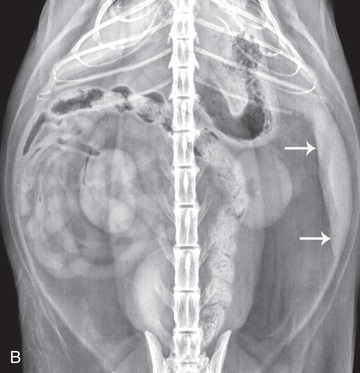
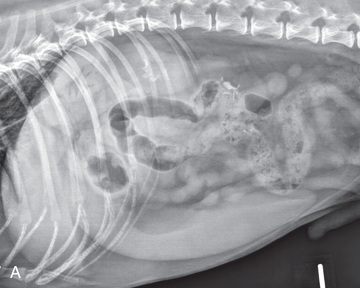
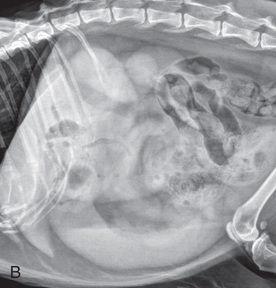
Hepatic enlargement can be detected radiographically, although mild size changes cannot be assessed accurately. An objective means of assessing hepatic size has been reported and uses a ratio of liver length, measured on right lateral images, with a line extending from the caudal most aspect of the caudoventral liver margin, to the ventral aspect of the caudal vena cava just cranial to the diaphragm, and length of the 11th thoracic vertebra.10,11 Normal reported length of the liver using this method has been reported as 5.4 and 5.5 times the length of T1 and 5.16 times the length of T11 in brachycephalic dogs.10,11 Pekingese dogs had smaller liver length ratios, at 4.64.11 The classic radiographic signs of generalized hepatomegaly are rounding or blunting of the caudoventral liver margins, along with extension beyond the costal arch, and caudal, and perhaps medial, displacement of the gastric axis (Figs. 40.4 and 40.5).12-14

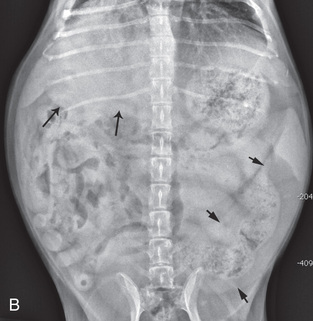
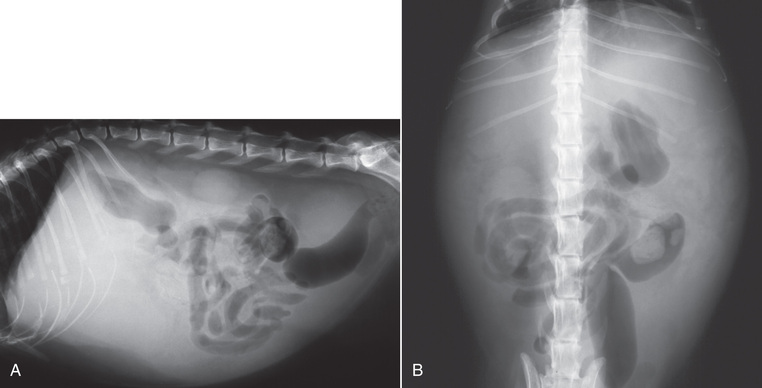
Several nonpathologic conditions can result in extension of hepatic margins beyond the costal arch, including overexpansion of the thorax or deep inspiration (Fig. 40.6). Older dogs and cats can have stretching or elongation of the triangular ligaments attaching the liver to the diaphragm, resulting in sagging and caudal extension of the liver. The same phenomenon can occur in obese dogs with a pendulous abdomen. In the obese dog, the liver does not extend as far dorsally. Some brachycephalic and chondrodystrophic dogs have caudal extension of the liver because of it being aligned more horizontally compared with deep-chested breeds. In addition, neonatal and young dogs and cats have a larger liver size compared with body size, creating the appearance of hepatomegaly without a true hepatic abnormality (Fig. 40.7).1,15 Because of the numerous normal variations that can cause hepatic lobe extension beyond the costal arch, rounding or blunting of these lobes should also be present before hepatomegaly is concluded.
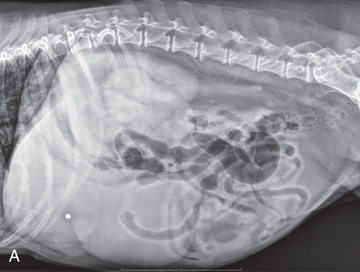
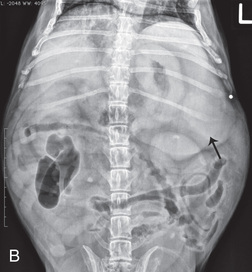
With generalized hepatomegaly, caudal displacement of the stomach, right kidney, transverse colon, and cranial duodenal flexure may occur, along with dorsal displacement of the pylorus. On VD views, the enlarged liver will cause displacement of the body and pyloric portion of the stomach caudally, and to the left (see Fig, 40.4). Both lateral and VD abdominal views should be examined to evaluate liver size because hepatomegaly is sometimes obvious only on one view.
Causes of generalized hepatomegaly are numerous, and radiographs alone are insufficient in most instances to narrow the list. Hepatic congestion, steroid hepatopathy, hepatic lipidosis, inflammatory and infiltrative disease, and primary and metastatic neoplasia are all possibilities. Hepatic ultrasound can be used to determine internal architecture and is better suited than radiography for narrowing the list of considerations for hepatomegaly.
Visualization of focal hepatomegaly depends on the degree of enlargement and the lobe affected. Focal hepatic masses usually result in distortion of the hepatic outline and are continuous with the liver in at least one projection.12-14 Left hepatic masses result in displacement of the stomach and spleen dorsally and to the right (Fig. 40.8). Right-sided hepatic masses displace the stomach and duodenum to the left and dorsally and the small bowel caudally (Fig. 40.9). The right kidney and distal extremity of the spleen may also be displaced caudally by a right-sided hepatic mass.
With few exceptions, masses located cranial to the ventral aspect of the stomach are hepatic in origin.12 Although hepatic masses classically result in caudal displacement of the stomach, a focal mass can extend caudal to the stomach (Fig. 40.10).13,14 Differentiation of a caudally located hepatic mass from a splenic mass based on radiographs alone is difficult in these instances. Differentials for focal hepatic masses include primary and metastatic neoplasia, abscess, granuloma, and hepatic cyst.

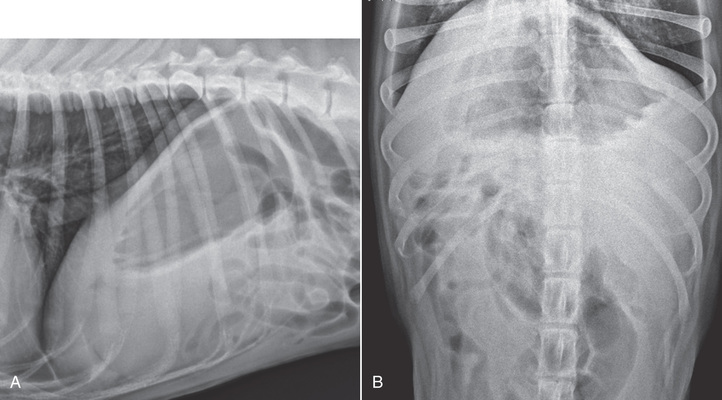
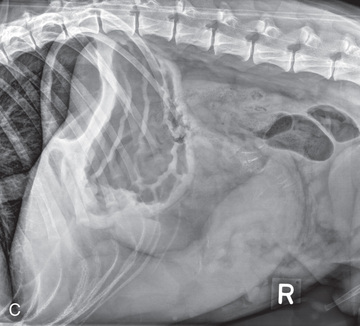
As with subtle hepatomegaly, slight decreases in hepatic size are not identified accurately radiographically. Marked microhepatia results in cranial displacement of the stomach and decreased distance between the diaphragm and gastric lumen (Fig. 40.11). Hepatic atrophy due to a congenital portosystemic shunt and hepatic cirrhosis are the two most common causes of microhepatia. Diaphragmatic hernia with displacement of the liver cranial to the diaphragm can give the appearance of a small liver, but there will be intrathoracic abnormalities in this instance.
Hepatic Opacity
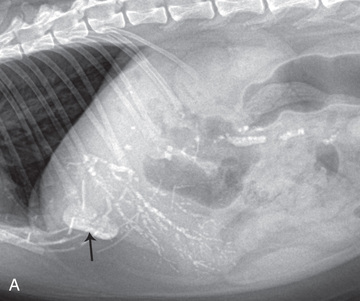
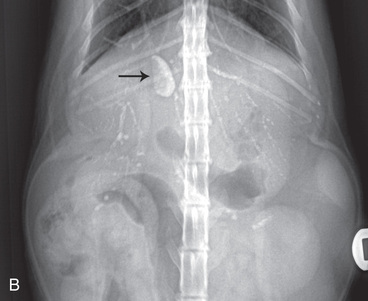
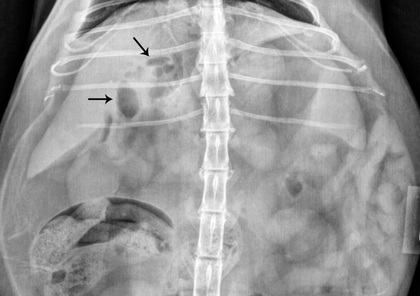
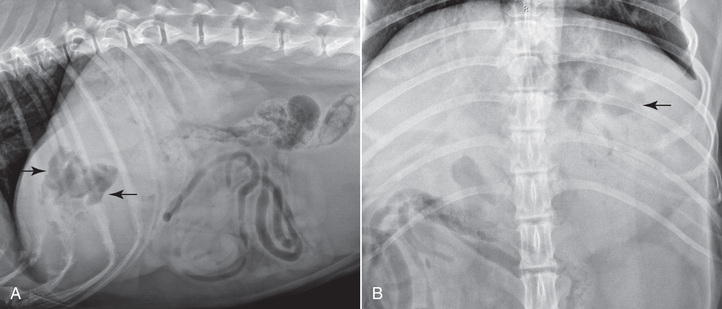
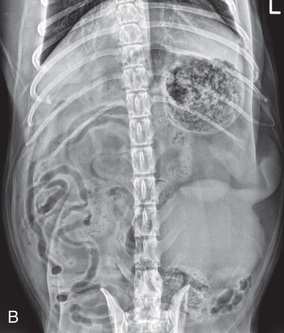
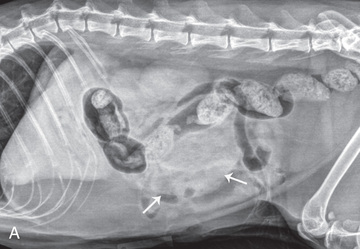
The normal liver is of soft tissue opacity. Mineral opacities can occur in the hepatic parenchyma or biliary system.16 Choleliths should be considered when focal mineral opacities are visible in the area of the gallbladder (Fig. 40.12). Linear trails of mineralized opacities extending peripherally within the hepatic parenchyma are indicative of choledocholiths, or calculi within the bile ducts.17 Biliary calculi are uncommon in dogs and cats but are visible radiographically if they contain sufficient calcium (see Fig. 40.12).18-25 These are often incidental findings, but choledocholiths can cause biliary obstruction, especially in the cat. Mineralization of the gallbladder wall has been associated with gallbladder carcinoma, as well as cholecystitis or cystic mucinous hyperplasia.16,26
Hepatic parenchymal mineralization may be localized or diffuse and have a variety of patterns.16 Dystrophic calcification of hepatic granulomas, abscesses, hematomas, neoplastic masses, or areas of hepatic necrosis have been documented (see Fig. 40.9). Mineralization of the biliary tree is seen occasionally in dogs with bile duct carcinoma.27 Echinococcosis infection can result in large hepatic soft tissue masses with mineralization of varying patterns and should be considered in endemic areas.28
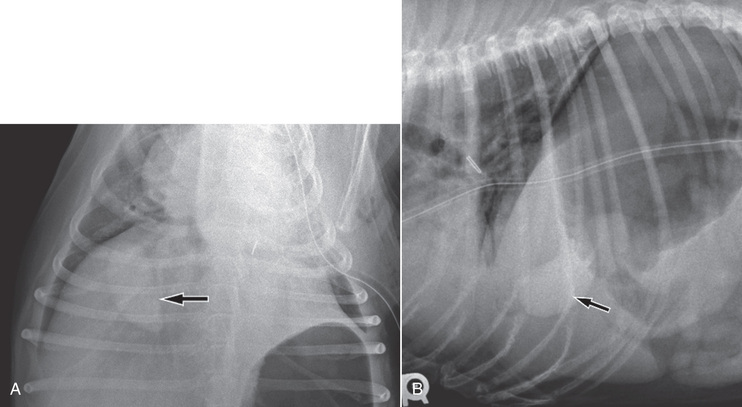
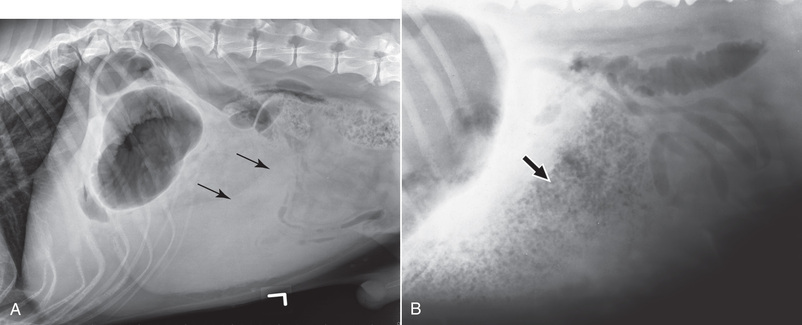
Radiolucent areas within the liver are indicative of intrahepatic gas, either in the biliary system, portal venous system, or hepatic parenchyma. Gas within portal vessels may occur because of severe necrotizing gastritis or enteritis, which is often associated with gastric dilation and volvulus complex. Gastrointestinal ulceration, distention, trauma, or interventional procedures may allow gas to ascend into the portovenous circulation (Fig. 40.13).1,29,30 A linear, branching radiolucent appearance, similar to air bronchograms, may be visible.
Gas in or around the gallbladder occurs with emphysematous cholecystitis, and this can be found in both diabetic and nondiabetic dogs.31,32 Gas is seen initially in the gallbladder wall, followed by more complete filling of the lumen. The gas eventually extends to the pericholecystic tissues. Gas bubbles conforming to the shape of the distended gallbladder can be seen within 24 to 48 hours of onset of disease. Obstruction of the cystic duct may be a common predisposing factor for emphysematous cholecystitis. Gas lucencies within the biliary system can also be seen after surgery of the duodenum or biliary system.1 Incidental reflux of gas into the bile duct from the duodenum is occasionally seen in cats. This may be because of incompetence of the sphincter of Oddi.4
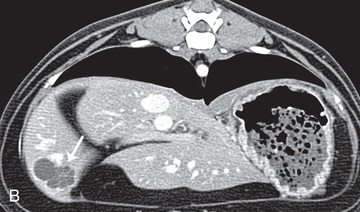
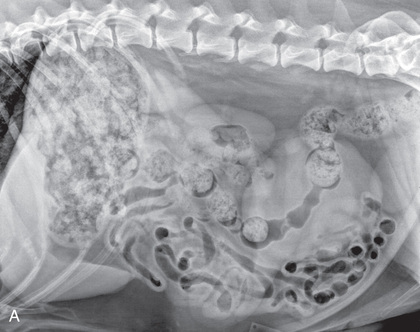
Hepatic abscess with gas-forming organisms may result in gas opacities within the hepatic parenchyma.33-36 These abscesses appear as irregularly stippled or mottled gas patterns, usually in a localized area (Fig. 40.14). Hepatomegaly or a hepatic mass is typically present with hepatic abscess with or without gas formation. Abscesses may be secondary to necrotic tumors, ascending portal infection, adjacent infection (pancreatitis), or penetrating wounds.
Imaging of Portosystemic Shunts
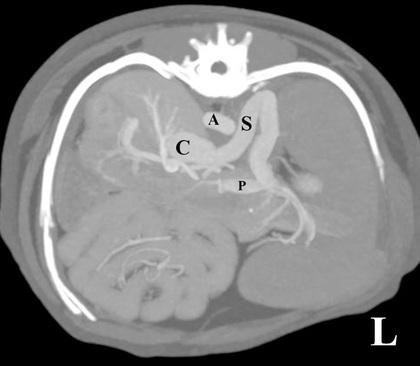
Portosystemic shunts are congenital or acquired anomalies of the portal vasculature in which blood bypasses the liver and enters the systemic circulation directly.37 Various imaging techniques have been used to identify and characterize the anomalous vessels, including cranial mesenteric portography, percutaneous splenoportography, and operative mesenteric portography.37-43 Portography, where the portal system is opacified with iodinated contrast medium, provides visualization of the anomalous vessel, any acquired collateral vessels, the direction of portal blood flow, and patency of the portal vein and its branches. Computed tomography (CT) angiography has largely replaced radiographic portography in the evaluation of portosystemic shunts.44-51 CT is minimally invasive and provides visualization of the portal vein and portal tributaries following intravenous injection of contrast medium (Fig. 40.15). With dual-phase CT angiography, post-contrast images are acquired during calculated peak hepatic arterial and portal venous phases. Three-dimensional vascular models can be created providing very detailed evaluation of the shunt origin and termination point, enabling surgical planning. In a survey of CT angiography studies, the most common extrahepatic shunts identified were (named from origin to insertion) spleno-phrenic, spleno-azygous, spleno-caval, right gastric-caval, and right gastric-caval with caudal loop.50,51
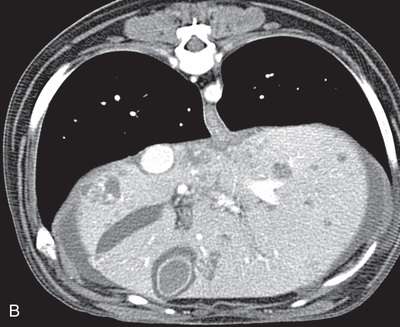
Computed Tomographic Imaging of Hepatic Masses
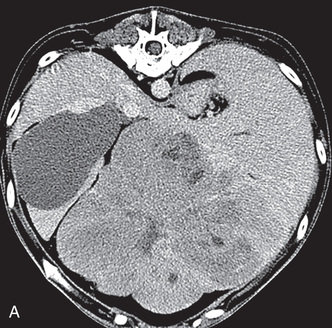
CT is commonly used for evaluation of hepatic masses, helping to determine exact location in terms of lobe or lobes involved, vascular involvement, and extent of disease for surgical planning. Multiphase contrast-enhanced CT protocols have been used to evaluate patterns of contrast uptake of hepatic masses to help differentiate benign from malignant disease.52-54 In triple-phase studies post-contrast images are acquired at 13 to 20 seconds (hepatic arterial phase), 30 to 40 seconds (early portal venous phase), and 120 seconds (equilibrium or delayed phase) after injection.52,53 In these studies, most hepatocellular carcinomas had heterogenous enhancement in all phases, and were hypoattenuating compared to normal liver parenchyma in the portal and delayed phase (Fig. 40.16). Metastatic lesions within the liver were homogeneous, with hypoattenuation compared to normal liver in all postcontrast phases. Benign hepatic adenomas had more diffuse enhancement in the hepatic arterial phase, with persistent enhancement in the portal venous phase. Finally, nodular hyperplastic lesions were homogeneous, often with marked contrast enhancement in the hepatic arterial and portal venous phases, with isoattenuation compared to normal hepatic parenchyma in the delayed phase. In a similar study using dual-phase contrast imaging, with images acquired within 30 seconds and at least 60 seconds post initiation of contrast administration, no CT features were significantly associated with benign or malignant hepatic lesions.54 There appears to be enough overlap in the contrast enhancement pattern of hepatocellular carcinomas, hepatic adenomas, hepatic metastases, and hepatic nodular hyperplasia, that CT findings alone are not sufficient to accurately predict benign from malignant disease. Histopathology remains the gold standard.54
Hepatic Ultrasound
Ultrasound examination of the liver allows detailed evaluation of hepatic internal architecture, including the hepatic vasculature and biliary system. Ultrasound is also useful in guiding aspirates and biopsies for nonsurgical, less invasive diagnoses.
The liver can be imaged through a combination of subcostal, subxiphoid, and right and left intercostal windows. Intercostal windows may be the best way to evaluate the liver in a deep-chested dog, patients with gas-distended stomach, or in dogs with microhepatia. The right dorsal intercostal window allows excellent visualization of the porta hepatis, the caudate liver lobe, and the right kidney in many dogs. Biliary obstruction, and intra- and extrahepatic portosystemic shunts may be visualized with this window. This window can also be used in cats but is not as often needed. The selection of transducer and frequency for hepatic evaluation depends on patient size and size of the liver. Transducer frequencies ranging from 5 to 10 MHz will accommodate most small animal patients. Transducers with smaller footprints are best for intercostal windows.
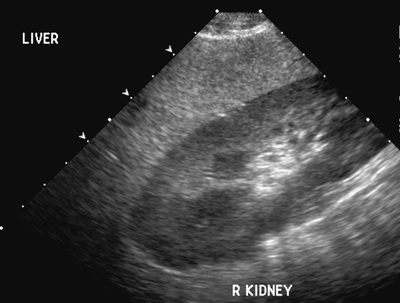
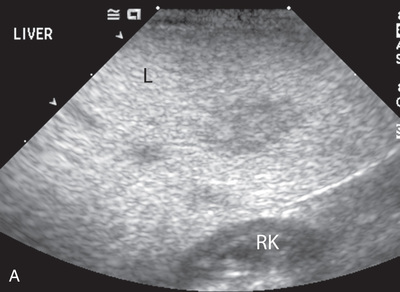
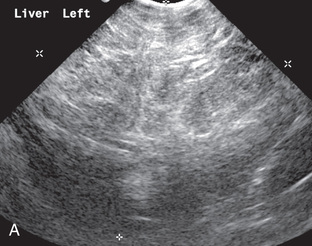
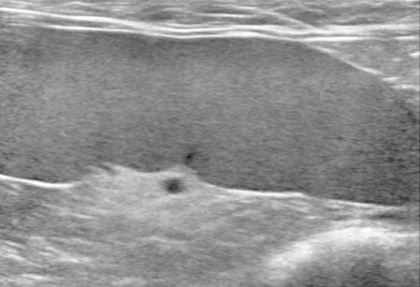
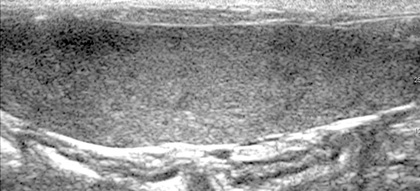
Based on the individual scatter pattern, each abdominal organ has a characteristic texture and appearance. The liver has a moderately coarse texture and is usually hypoechoic to the spleen (Fig. 40.17).55-59 When using the right renal cortex for comparison to the caudate liver lobe, the liver may be isoechoic, or slightly hypoechoic or hyperechoic. The renal cortex of many normal cats is hyperechoic due to lipid deposition, and this should be considered before interpreting the liver as hypoechoic.60,61 Assessment of echogenicity in any organ is subjective and dependent on several variables. Any change should be correlated with the overall clinical picture.
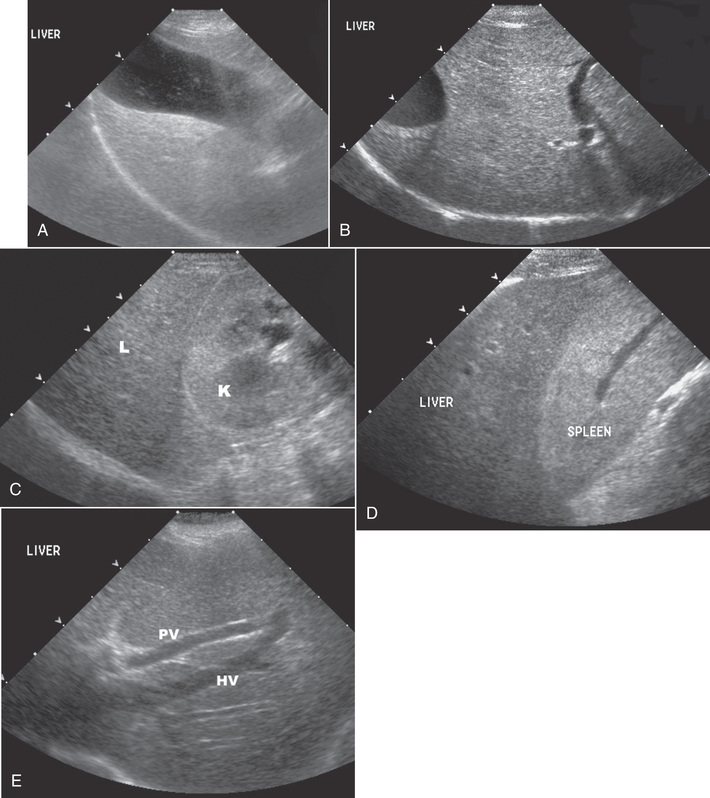
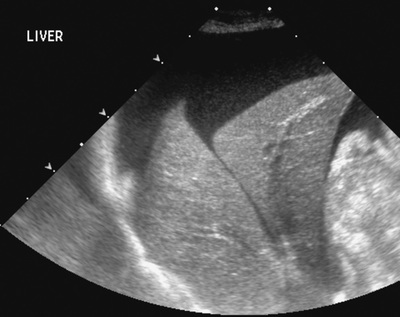
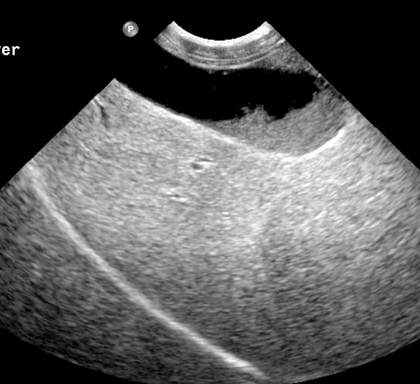
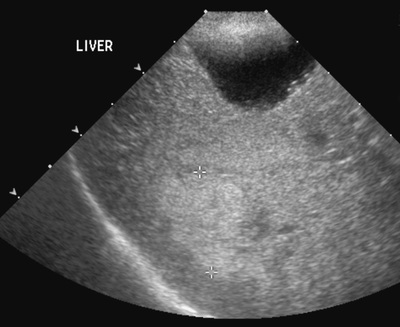
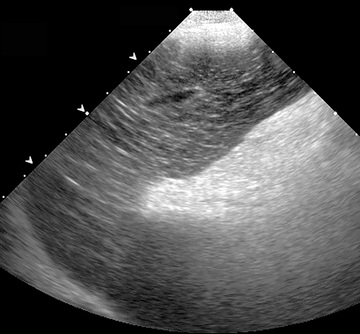
Hepatic margins should be smooth and sharp but are better visualized sonographically if adjacent peritoneal fluid is present (Fig. 40.18). The liver is bordered cranially and dorsally by an echogenic line representing the interface between the diaphragm and lung/pleura. A mirror-image artifact is frequently noted deep to the diaphragmatic interface, giving the false impression of liver on both sides of the diaphragm (see Chapter 4 for a detailed explanation of this artifact).
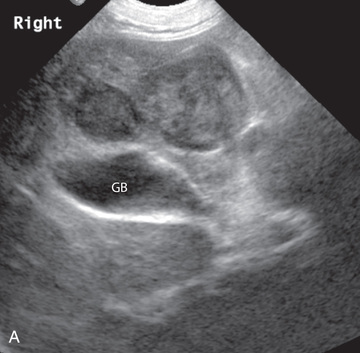
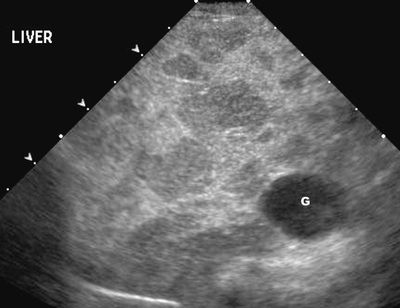
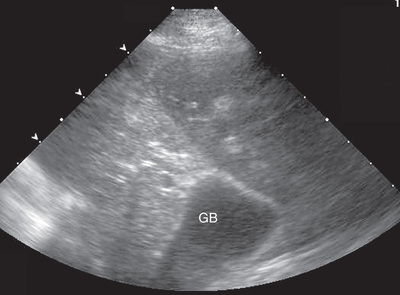
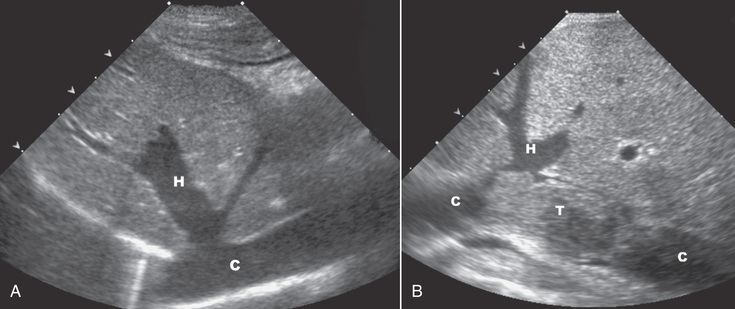
As with assessing echogenicity, the ultrasound assessment of liver size is also subjective and based on operator experience, patient conformation, and adjacent organs.62 A small liver is difficult to evaluate sonographically, because gas from a more cranial located stomach can obscure visualization. The gallbladder may appear large relative to overall hepatic size (Fig. 40.19). Liver size may appear decreased in dogs with a deep thoracic cavity wherein liver location is more completely within the costal arch. Intercostal ultrasound windows may be needed in these patients. The enlarged liver can be examined relatively easily with ultrasound, because it extends well beyond the xiphoid cartilage and covers the right kidney more completely (Fig. 40.20). Liver margins may appear rounded and may extend beyond the left lateral margin of the stomach.
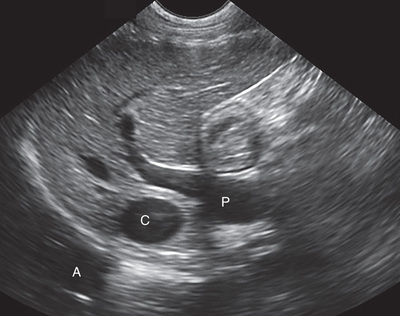
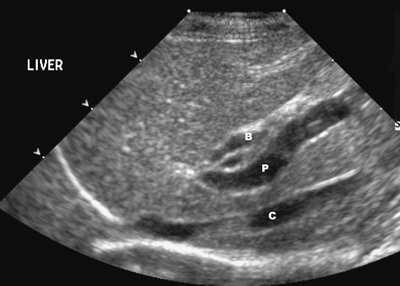
Hepatic and portal veins are visualized routinely within hepatic parenchyma. Portal veins are smoothly tapering vessels characterized by bright, echogenic borders (see Fig. 40.17E).55-58,63 The larger left and smaller right branch originate from the main portal vein near the porta hepatis, although they branch in different imaging planes.63 Portal blood flow courses normally from the hepatic hilus toward the periphery. Hepatic veins are anechoic linear structures extending through the parenchyma. Hepatic vein borders are not echogenic except at their confluence with the caudal vena cava, immediately adjacent to the diaphragm. Hepatic venous flow courses normally toward the hepatic hilus, into the caudal vena cava. In many dogs, the right lateral dorsal intercostal window provides an excellent window to the aorta, caudal vena cava, and main portal vein (Fig. 40.21). Normal hepatic arteries are not visualized easily without color Doppler examination. The caudal vena cava can be visualized coursing through the liver in the right lateral abdominal quadrant.
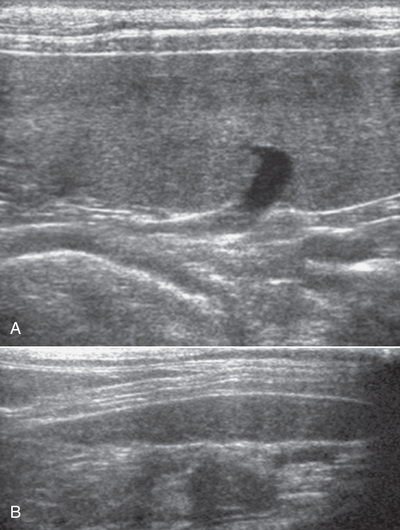
The gallbladder is well visualized as an oval, anechoic structure in the right cranioventral portion of the liver (see Fig. 40.17A). Gallbladder size varies widely, and distention is normal in fasting or anorexic patients. Normal gallbladder volume in the dog is 1 mL/kg or less body weight, and it can be measured with the ellipsoid formula (length × width × height × 0.52).64,65 Cats may have a more uniform gallbladder volume of 2.4 mL, with no apparent association with body weight.64,66 Intraluminal gallbladder contents are typically anechoic, although gallbladder sludge, which is dependent echogenic material without acoustic shadowing, is seen frequently (Fig. 40.22). Although sludge is common in dogs with no indication of biliary disease, there is more recent evidence that it could be an indication of gallbladder dysmotility.67,68
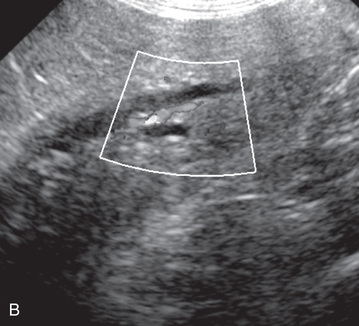
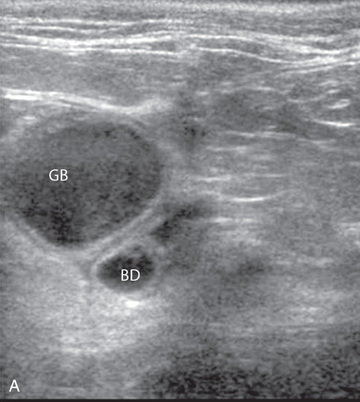
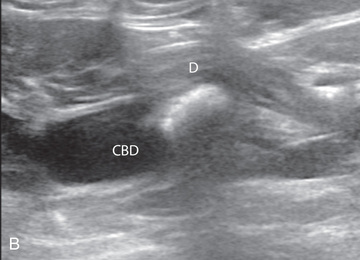
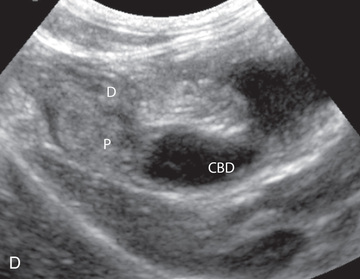
The normal gallbladder wall is thin and poorly visualized. In the cat, gallbladder wall thickness should be less than 1 mm or not visualized at all.69 The normal canine gallbladder wall typically measures 1-2 mm, but normal ranges have not been established.70,71 A duplicate or septated gallbladder is seen occasionally as a normal variation in cats and is caused by abnormal embryonic development.72 The common bile duct is immediately ventral to the portal vein but is visible more consistently in the cat, where it can usually be followed to the duodenal papilla (Fig. 40.23). Normal common bile duct diameter in the cat is 4 mm or less.73 If visible, the canine bile duct should be 3 mm or less.74 Normal intrahepatic bile ducts are not visible.
Abnormal Sonographic Appearance of the Liver
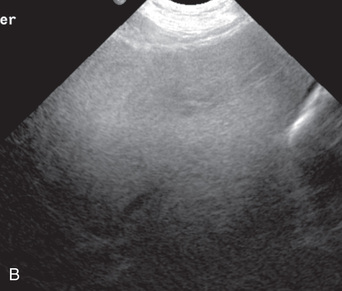
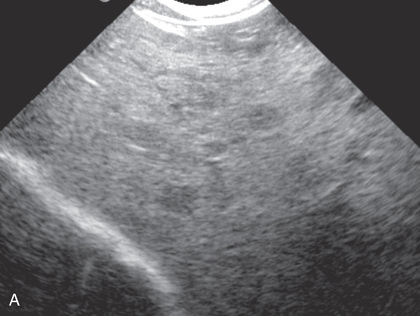
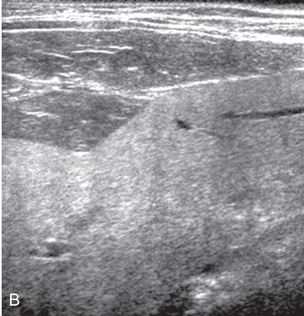
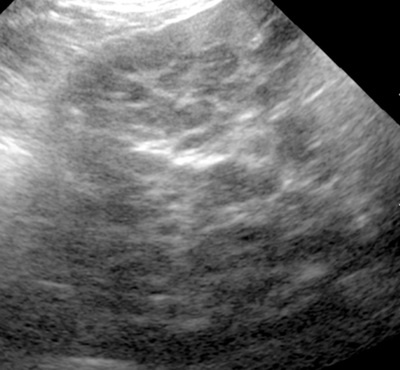
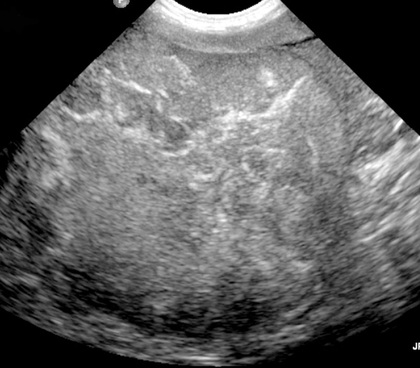
Ultrasound is helpful in differentiating between diffuse and focal hepatic disease in patients with hepatomegaly and/or elevated liver enzymes. Diffuse hepatic disease may cause no change in the ultrasound appearance of the liver. However, changes in hepatic echogenicity, increase or decrease in size, and irregular or rounded margins point to diffuse hepatopathy.55-58,75-80 A hyperechoic liver is identified by comparison with the echogenicity of an adjacent organ, such as liver being hyperechoic to renal cortex, or isoechoic or hyperechoic to spleen. Loss or decreased visualization of the usually conspicuous periportal echoes and abnormally increased attenuation of sound as it passes through the liver are indications of hyperechoic hepatic parenchyma (Fig. 40.24). Several diffuse hepatopathies can potentially result in either a diffusely hyperechoic liver, or a mottled appearance (i.e., hyperechoic parenchymal background with poorly defined hypoechoic nodules).55-58,75-80 Vacuolar hepatopathies, including lipidosis and steroid hepatopathy, are likely the most frequent diagnosis when this appearance is seen (Fig. 40.25). Hepatic lipidosis in cats is the most common diffuse feline hepatopathy, and it results in a liver parenchyma that is hyperechoic to adjacent falciform fat. However, a nonpathologic hyperechoic liver can be present in some obese cats, and ultrasound alone is likely insufficient for the diagnosis.77,79,81 Chronic hepatitis with parenchymal fibrosis can also cause increased echogenicity, although liver size is variable and may be normal, increased, or decreased. Hepatic cirrhosis typically results in a small, irregular, hyperechoic liver (Fig. 40.26). Ascites often accompanies cirrhosis, enhancing visualization of irregular liver margins resulting from formation of regenerative nodules. Other hepatic diseases that may result in increased/mottled parenchymal echogenicity include chronic hepatitis, lymphosarcoma, amyloidosis, and cholangiohepatitis. In cats with cholangitis/cholangiohepatitis complex the liver can appear normal, or hyperechoic, secondary to lipidosis; hypoechoic liver may also occur.64,76,82 Mast cell infiltration in the liver results in a variable appearance, from normal to increased echogenicity and size. Hypoechoic nodules may be present83 (Fig. 40.27). However, the sonographic appearance of the liver (and spleen) may be a poor predictor of cytologic mast cell infiltration.84-86
A decrease in hepatic echogenicity results in increased periportal echoes and abnormal comparison to the renal cortex, because the liver becomes hypoechoic to the cortex. Decreased hepatic echogenicity may occur with hepatic congestion, lymphosarcoma, leukemia, amyloidosis, and cholangiohepatitis; a dilated caudal vena cava and hepatic veins will accompany hepatic congestion. Acute suppurative hepatitis can cause hypoechogenicity from inflammation and edema. However, this may be uncommon, even with severe disease.75,87
As noted previously, diffuse, even severe hepatic disease can appear normal sonographically. It is apparent that ultrasound alone is insufficient to accurately characterize the various hepatopathies, or even differentiate normal from abnormal. Acoustic impedance of normal versus diseased tissue may simply be insufficient to permit visible change.80,88,89 Any suspected hepatopathy should be compared with clinical signs and laboratory data, and a biopsy is necessary for definitive diagnosis.90,91 Prebiopsy coagulation screening is a useful precaution when liver disease is suspected.
Focal hepatic disease appears as a nodule or mass that differs in texture and echogenicity from surrounding normal liver parenchyma. They may interrupt the hepatic margin, resulting in change of shape or contour. Relatively small nodules can be detected, especially when using high-frequency transducers. However, although ultrasound is sensitive in detecting hepatic nodules, it is not specific; and numerous considerations are possible for focal disease. Cysts, abscesses, primary or metastatic neoplasia, hematomas, granulomas, nodular hyperplasia, and focal extramedullary hematopoiesis can all produce focal hepatic disease and may be difficult to differentiate on the basis of ultrasound appearance alone.55-58,77,92 However, ultrasound is extremely useful in differentiating cystic versus solid masses; focal, multifocal, or diffuse distribution of masses, and the relation of the mass to adjacent structures, such as large blood vessels, diaphragm, or gallbladder.
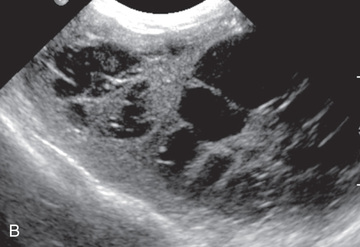
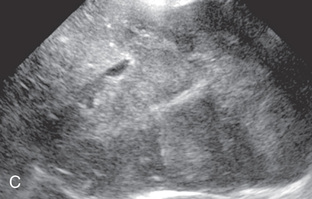
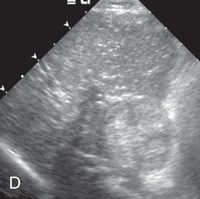
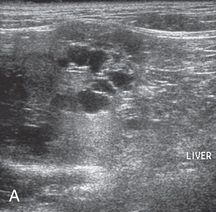
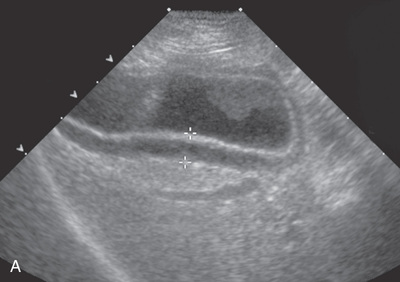
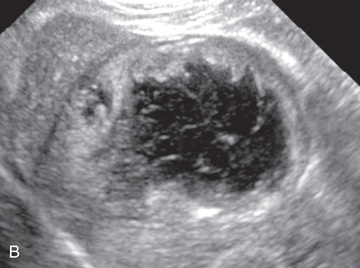
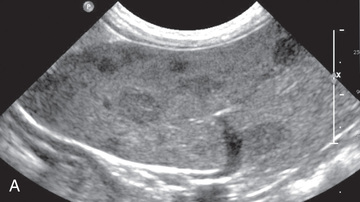
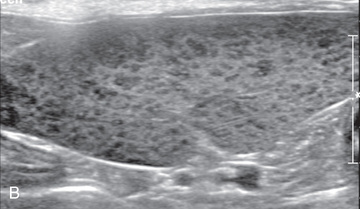
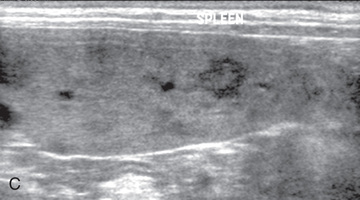
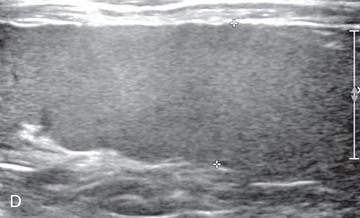
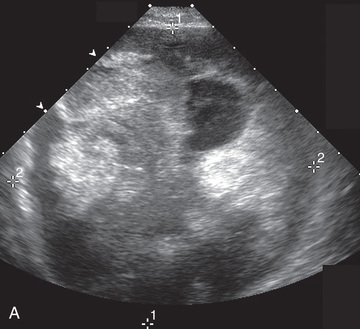
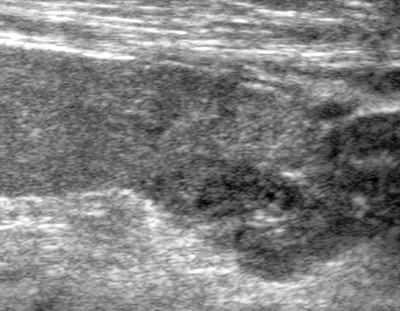
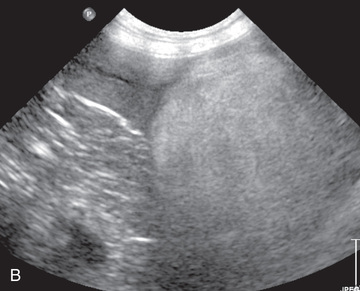
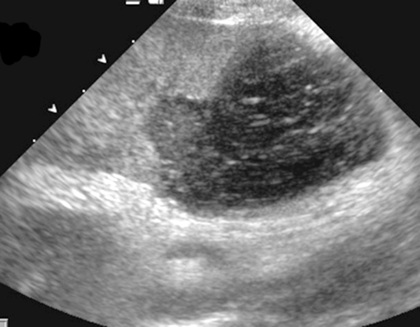
Hepatic neoplastic masses are variable in appearance, and they can be hyperechoic, hypoechoic, or mixed echogenicity, solid, cystic, or cavitated (Fig. 40.28).56-58,64,75-83,93-105 The ultrasound appearance is not specific for a particular tumor, and as in diffuse disease, there appears to be poor correlation to cytologic and histopathologic diagnosis.56,58,76,77,83,85,92,93,106-109 A positive cytological diagnosis of neoplasia is often accurate, but a negative cytologic evaluation does not rule out neoplasia.109 Primary hepatic tumors are classified as massive (e.g., with a solitary mass affecting a single lobe), multifocal (e.g., with nodular disease in multiple lobes), and diffuse (e.g., multifocal coalescing nodules in all lobes).95,98 Hepatocellular carcinoma is the most common primary tumor in the dog, and it is most often massive in classification (see Fig. 40.28A). Other primary hepatic tumors include cholangiocarcinoma, which is the second most common primary hepatic neoplasia in the dog, neuroendocrine tumor, hemangiosarcoma, and histiocytic sarcoma (see Fig. 40.28B).95-100 Hepatic lymphosarcoma may result in a normal appearing liver, or a diffuse increase or decrease in echogenicity; more focal changes include hypoechoic nodules/areas (see Fig. 40.28C).88,89,110 Metastatic disease in the liver is the most common hepatic malignancy in the dog at 2.5 times the frequency of primary hepatic neoplasia, and most often originates from the spleen, gastrointestinal tract, and pancreas.97 Like primary hepatic neoplasia, metastatic disease may be hyperechoic or hypoechoic, but more often it has a multifocal nodular or mass-like appearance (see Fig. 40.28D).93,94,108 Metastatic disease cannot be differentiated from primary hepatic malignancy based solely on the ultrasound appearance.93,94,108 Target lesions, which are focal masses with a hyperechoic center and hypoechoic periphery, are most commonly associated with malignancy, but they have been reported with benign disease processes (see Fig. 40.27B).58,92,111 Biliary cystadenoma (bile duct adenoma) is the most common primary hepatic neoplasia in the cat, and it may be focal or multifocal.100-105 Although variable in appearance, the presence of a cystic component somewhere in the mass is a consistent finding (Fig. 40.29). Biliary cystadenomas may appear multilocular, containing thin-walled cysts, or as hyperechoic masses with a cystic component. Most cystic portions of these masses will be characterized by acoustic enhancement. Cholangiocarcinoma is the most common primary hepatic malignancy in the cat.100-105
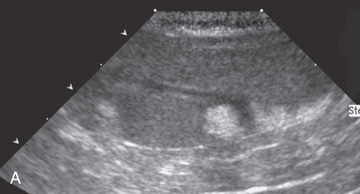
Hepatic nodular hyperplasia, a common benign lesion in older dogs, is usually silent clinically but may result in elevations in serum alkaline phosphatase.96,112 It has a variety of sonographic appearances and cannot be differentiated from neoplasia without biopsy (Fig. 40.30). Hyperechoic, hypoechoic, isoechoic, and mixed echogenicity nodules, some with cavitation, are all possible.113
Contrast-enhanced ultrasonography is being used with some success in improving visualization of hepatic nodules and differentiating benign and malignant hepatic nodular disease.114-116 After injection of an ultrasound contrast agent, benign regenerative nodules were isoechoic to surrounding normal liver during peak normal liver perfusion, whereas malignant nodules were hypoechoic to surrounding liver at peak normal liver perfusion. Identification of tumor type was not possible.
Chronic hepatitis may also result in a diffuse nodular appearance (Fig. 40.31). Hyperechoic hepatic parenchyma surrounds multifocal hypoechoic nodules (nodular hyperplasia).55,58,77 Liver size may be normal or decreased. Hepatocutaneous syndrome (superficial necrolytic dermatitis) also can result in a nodular appearance, and it should be suspected when the liver parenchyma has a honeycomb appearance with hyperechoic hepatic parenchyma surrounding hypoechoic focal nodular areas (Fig. 40.32).117-121 These patients have concurrent dermal lesions in the footpads and mucocutaneous junctions. A biopsy is critical in making the diagnosis.
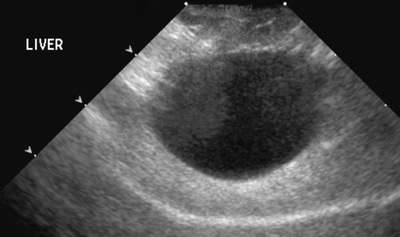
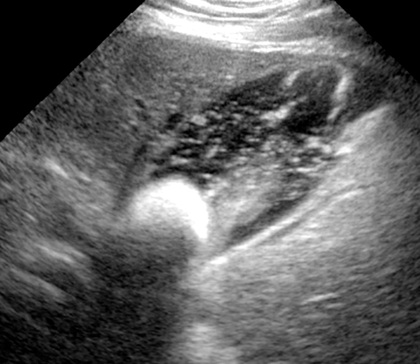
Hepatic abscesses and hematomas have a variable appearance depending on duration. Abscesses often have an echogenic rim with a central anechoic or hypoechoic area.34,36,122-124 They may contain gas, resulting in an echogenic interface with deep acoustic shadowing (Fig. 40.33). Hepatic abscesses may appear as a simple hypoechoic mass resembling nodular hyperplasia or neoplasia. Hematomas may be hyperechoic initially because of gas or red blood cell aggregates and then progress to hypoechoic or anechoic and finally back to hyperechoic because of reorganization or possible mineralization.55,125,126 Hepatic cysts have a more consistent appearance, as a fluid-filled, anechoic structure with a well-defined, thin wall and acoustic enhancement. Usually an incidental finding, hepatic cysts have the potential to produce clinical signs if large enough or numerous enough to replace liver parenchyma. They can be associated with polycystic kidney disease, so the kidneys should be evaluated carefully for cystic structures if hepatic cysts are noted.
Liver lobe torsion is variable in appearance.127,128 The abnormally positioned lobe may be hypoechoic or mixed in echogenicity. Doppler evidence of blood flow is reduced or absent in the abnormally positioned lobe (Fig. 40.34).
Disease of the Biliary System
Ultrasound is very advantageous in the diagnosis of gallbladder and bile duct disease, and it is an important component in determining the cause of icterus. Abnormal wall thickness, luminal contents, obstruction, and neoplastic disease may be diagnosed on ultrasound examination.
Thickening of the gallbladder wall is a nonspecific sign found with primary gallbladder inflammation or neoplasia, or secondary to systemic diseases that have a secondary effect on the gallbladder wall.57,64,71,129,130 Wall thickening can appear double layered with a central hypoechoic layer between hyperechoic layers, or it may be diffusely thickened, irregular, and hyperechoic (Fig. 40.35). Primary inflammatory conditions of the gallbladder that result in hyperechoic thickening include cholecystitis, such as secondary to biliary stasis, irritation from cholelith, or ascending infection, and cholangiohepatitis (see Fig. 40.35B).56,57,64,71,130-132 In one study, the finding of immobile gallbladder sludge had a 70% sensitivity and 100% specificity for the diagnosis of bactibilia and bacterial cholecystitis.133 Emphysematous cystitis, usually associated with a septic process and gas-forming bacteria, results in intraluminal echogenic foci and reverberation artifact.64,134,135 Cystic mucinous hyperplasia is noted as an incidental finding at necropsy, but it may be a predisposing factor in gallbladder mucocele formation.64,136,137 Hyperplastic gallbladder wall epithelium, cystic accumulations of mucus, and papillary projections create the appearance of sessile or polypoid masses along an irregularly thickened gallbladder wall (see Fig. 40.35C). Edema of the gallbladder wall can be present secondary to right-sided congestive heart failure, portal hypertension, hypoproteinemia, sepsis, and anaphylaxis (see Fig. 40.35A).56,57,71,125,129 Peritoneal fluid surrounding the gallbladder can result in a false impression of wall thickening. Percutaneous cholecystocentesis for culture and cytology of the intraluminal bile should be performed with care.71 Gallbladder thickening may be permanent because of inflammation and fibrosis despite resolution of the underlying disease process.55,64

Cholecystoliths, or calculi within the gallbladder, are echogenic focal structures, often with acoustic shadowing, and they may be single or multiple.20,25,64,136,138 They are typically mobile, falling to the dependent portion of the gallbladder (Fig. 40.36). Choledocholiths are stones within the bile duct, hepatic ducts, and interlobar ducts. Although cholecystoliths and choledocholiths are frequently incidental, they have the potential to cause biliary obstruction, or can arise secondary to obstruction. Choledocholiths located in the distal bile duct, in or around the duodenal papilla, are one of the more common causes of biliary obstruction in cats, and they are often associated with cholangiohepatitis.139
As noted earlier, intraluminal echogenic, dependent, mobile biliary sludge is present in up to 53% of asymptomatic dogs, and 35% to 48% of all dogs regardless of health status.67,140,141 More recently, it was noted that dogs with biliary sludge may have decreased gallbladder emptying compared to dogs without sludge.68 It is hypothesized that decreased emptying may predispose to gallbladder mucocele formation secondary to biliary stasis, bile inspissation, and increased mucus accumulation.68 Gallbladder emptying can be determined by measuring gallbladder volume pre- and post-feeding. After a 12-hour fast, volume is determined using the previously noted ellipsoid formula. At 60 and 120 minutes post meal or prokinetic agent, such as erythromycin, gallbladder volume is reassessed. In normal dogs, gallbladder volume post feeding should be less than 1 mL/kg, or it should be reduced by at least 25%.64,65
Gallbladder mucocele is an accumulation of nondependent sludge, semisolid mucus, and inspissated bile, creating an intraluminal centralized echogenicity with peripheral striations, creating a stellate appearance (Fig. 40.37).142-149 Hyperplasia of mucus-secreting glands results in abnormal accumulation of mucus within the lumen with subsequent biliary obstruction by mucinous plugs within the cystic and bile duct. Distention of the intrahepatic and/or extrahepatic biliary system may be present. Ischemic necrosis of the gallbladder wall can lead to rupture. Gallbladder mucoceles have been associated with a 50% incidence of loss of gallbladder wall integrity and/or acute rupture.142 The presence of discontinuity of gallbladder wall, pericholecystic hyperechoic fat, and/or pericholecystic fluid is strongly suggestive of gallbladder rupture (see Fig. 40.37B).142-144,146 Contrast-enhanced ultrasound evaluation of the gallbladder allows identification of ischemic necrosis or rupture of the gallbladder wall with a higher sensitivity and specificity than conventional sonography.150 Cholecystocentesis is discouraged in patients with a gallbladder mucocele, because wall rupture may be imminent. Dogs diagnosed with gallbladder mucocele are more likely to have hyperadrenocorticism.151,152 A biliary mucocele is identified occasionally as an incidental finding in patients without clinical signs or serum biochemical changes. Feline gallbladder mucoceles are uncommon, because cats have fewer mucus-secreting glands in the gallbladder compared to dogs.138,153
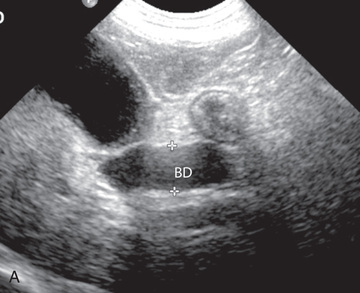
Extrahepatic biliary obstruction results in a retrograde dilation of the biliary system.154 With complete obstruction, the gallbladder and cystic duct distend within 24 hours with progressive dilation of the common bile duct within 48 hours (Fig. 40.38). Gallbladder distention may be minimal in the face of chronic inflammation and fibrosis.64 Progressive dilation of the common bile duct and hepatic ducts occur during the next 3 to 4 days with dilation of lobar and interlobar ducts by 7 days. This results in multiple tortuous, irregularly branching anechoic linear tracks within the liver. These can be differentiated from hepatic vessels with color Doppler interrogation (see Fig. 40.38B). Pancreatitis is one of the most common causes of extrahepatic biliary obstruction in the dog, with neoplasia of the liver, bile duct, pancreas, or duodenum also capable of causing obstruction (Fig. 40.39). Sludge associated with gallbladder mucocele may also result in obstruction. Tumors and inflammation of the bile duct, pancreas, and duodenum, along with choledocholithiasis, are more commonly noted in the cat (see Fig. 40.39A, B, and D).138,155 In 30 cats with extrahepatic biliary obstruction, gallbladder distension was present in only 13 (43%), and it was not considered a reliable indicator of biliary obstruction. More reliable was dilation of the bile duct, present in 29 (97%) obstructed cats.138 Focal sludge accumulation within the feline bile duct cannot easily be differentiated from a neoplastic mass. Incomplete or early obstruction may not cause visible biliary dilation. Bile duct dilation may be prolonged, persisting after relief of the obstruction.55

Cholangitis/cholangiohepatitis complex is an important biliary disease in cats. Ultrasound changes with this disease include thickened gallbladder wall, often with a palisade type irregular mucosa, intraluminal gallbladder or bile duct sludge, choleliths/choledocholiths, and thickened, tortuous, and sometimes dilated bile ducts (see Fig. 40.39A).25,64,76,82,156,157 No ultrasound changes are present in some cats with cholangitis/cholangiohepatitis.
Vascular Disease
Venous congestion occurs with right-sided congestive heart failure or obstructive lesions in the posthepatic caudal vena cava. The hepatic caudal vena cava and hepatic veins both dilate in response to the elevated pressure (Fig. 40.40). The liver may also enlarge and become hypoechoic, although echogenicity changes may not be consistent. Dilation of the caudal vena cava and hepatic veins, along with ascites, suggests the possibility of disease cranial to the diaphragm.
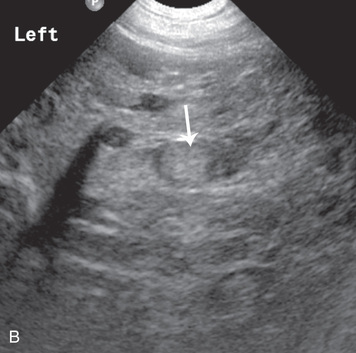
Ultrasonography can be used to identify most portosystemic shunts reliably, although detection of these vascular anomalies requires a good knowledge of vascular anatomy. An abnormal shunting vessel is the most reliable indication of portosystemic shunt, but other changes, including a small liver that is uniform and normal in echogenicity, decreased or absent intrahepatic portal vasculature, decreased size of extrahepatic portal veins, enlarged kidneys, and renal/ureteral/cystic and/or urethral calculi (urate calculi), are often present (Fig. 40.41; see Fig. 40.19).55,158-163
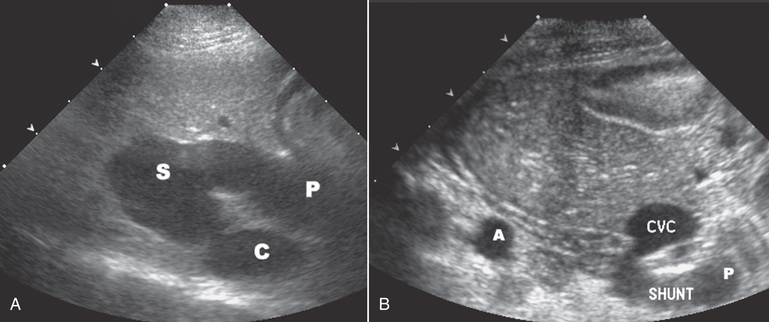
Extrahepatic shunts affect cats and small-breed dogs primarily, and the most common finding is a single shunt vessel connecting the portal vein, or more likely a major tributary of the portal vein, such as splenic, left gastric, or right gastric vein, to the caudal vena cava between the right renal vein and hepatic veins (see Fig. 40.41B).158-163 Extrahepatic shunt vessels may be difficult to visualize because of poor acoustic windows associated with the small liver or the presence of bowel gas. A right dorsal intercostal window, in addition to routine views, is helpful in detecting the anomalous shunt vessel. In this window, the portal vein and caudal vena cava are visible as they enter the porta hepatis, and abnormal shunting vessels may be identified more easily. The portion of the portal vein cranial to the origin of the shunt is often decreased in size, with a portal vein:aortic ratio of less than 0.65, whereas the normal ratio is 0.7 to 1.25.159 Pulsed-wave or color Doppler interrogation of the caudal vena cava is helpful in assessing for abnormal turbulence where a shunting vessel enters.158,159 Shunt vessels terminating in the azygous vein may be more difficult to follow, but they might be seen terminating in an enlarged azygous vein adjacent to the aorta or esophagus. Acquired extrahepatic shunt vessels attributable to hepatic disease and portal hypertension may appear as a grouping of multiple variably sized, tortuous vessels, often medial to the spleen and left kidney. In some patients, these abnormal vessels are not visualized easily without color flow Doppler imaging.160
Intrahepatic shunts, affecting primarily large-breed dogs, are usually easier to identify. A right lateral intercostal window, in addition to the standard ventral abdominal approach, is helpful in visualizing the intrahepatic shunting vessel between main portal vein and caudal vena cava (see Fig. 40.41A).158,159,164 Left divisional shunts, such as a patent ductus venosus, right divisional shunts, and central-divisional shunts can be identified. Contrast harmonic sonography has been used to detect increased hepatic arterial flow as an indicator of portosystemic shunting and may be useful as an additional diagnostic test.165
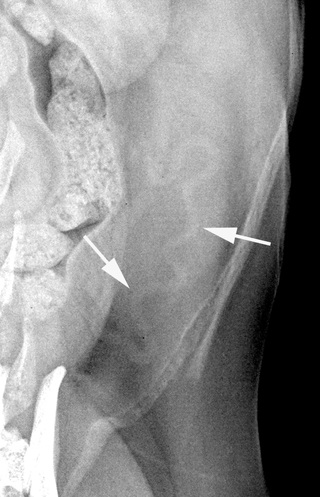
An uncommon form of splenosystemic shunt has been described in cats.166 These splenosystemic shunts were identified as an anomalous vessel arising from the splenic vein, coursing caudal to the left kidney assuming a generally tortuous path, and continuing to the left renal vein, caudal vena cava adjacent to the renal vein, or medial to the left kidney. Neutered female cats were overrepresented. It could not be determined whether these shunts were congenital or acquired in origin. However, these shunts do not appear to share similar clinical or anatomic features with previously described congenital portosystemic shunts in cats. This type of shunt can occasionally be visible in survey abdominal radiographs as a tortuous vessel caudal to the spleen in VD radiographs (Fig. 40.42).
Radiology of the Spleen
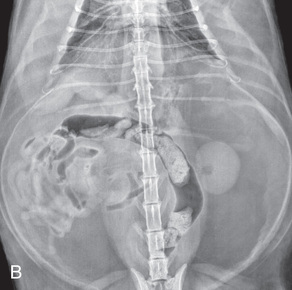
The spleen is a dynamic organ; and in the dog, the size and location of the spleen can vary widely. There are numerous variations on the radiographic appearance of the normal spleen in dogs and to a lesser extent in cats.1-5,8,167 The spleen is divided into a proximal extremity, termed the head of the spleen; a body; and a distal extremity, termed the tail of the spleen. The proximal extremity is relatively fixed in the left craniodorsal aspect of the abdomen. The distal extremity is not fixed, and in the dog, the position of this portion of the spleen can vary considerably. On VD views of the canine abdomen, the proximal extremity of the spleen is seen typically as a triangular soft tissue opacity caudolateral to the gastric fundus and craniolateral to the left kidney (Fig. 40.43A). The remainder of the spleen may extend caudally, adjacent to the left lateral abdominal wall, or more medially across the midline. When the spleen extends medially, the full length of the spleen is not visualized completely.
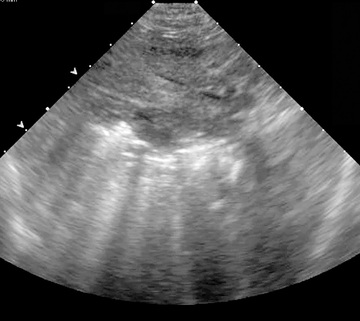
On lateral views, the triangular soft tissue opacity of the proximal extremity of the spleen is located dorsally, caudal to the stomach. The distal extremity is visualized typically as a triangular soft tissue opacity immediately caudal and slightly ventral to the pylorus or liver (see Fig. 40.1A). The distal extremity of the spleen is often more conspicuous on right lateral views of the abdomen but may silhouette the caudal margin of the liver and be poorly visualized as a separate structure.
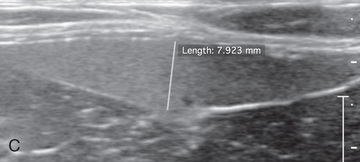
The feline spleen is thinner and smaller compared with the canine spleen and less variable in size and position (see Fig. 40.43B; also see Fig. 40.1C). Like the dog, the proximal extremity of the spleen can be visualized on VD views in the left cranial abdomen, caudolateral to the stomach and craniolateral to the left kidney. On VD views, the distal extremity usually extends caudally along the left lateral abdominal wall, but the amount of spleen visualized varies depending on body fat, positioning, gastric contents, and splenic position.167
On lateral abdominal views in the cat, the proximal extremity may be visualized caudal and dorsal to the gastric fundus. The distal extremity of a normal spleen is rarely visualized in the cat. In 100 cats with a presumably normal spleen, the distal extremity was visualized on a lateral radiograph in only one cat.167
In both dogs and cats, it is important to realize that the entire spleen is rarely visualized on a single radiographic projection. When the x-ray beam is perpendicular to the spleen, there may be insufficient x-ray absorption to allow its visualization. When the x-ray beam is parallel to the long axis of the spleen, the resultant soft tissue opacity represents only a portion of the spleen.8
Splenic Size
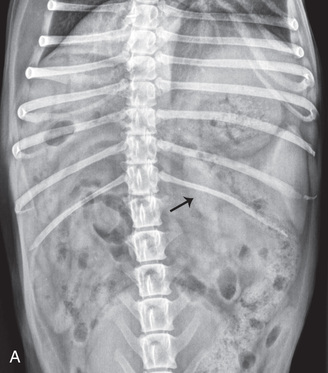
Radiographic assessment of splenic size in the dog is very subjective, because normal size varies widely. Feline splenic size appears to be more consistent. Splenomegaly in the cat is considered if the distal extremity is visible on the lateral projection of the abdomen.167,168 In the dog, and to a lesser extent in the cat, generalized splenomegaly results in thickened, rounded, blunted margins, and dorsal and caudal displacement of the jejunum on lateral views (Fig. 40.44). Organ displacement on the VD view as a result of the enlarged spleen depends on the portion of the spleen that is enlarged and the degree of enlargement. The jejunum may be displaced to the right or left, whereas an enlarged proximal extremity results in cranial displacement of the stomach.
Considerations for diffuse splenomegaly are numerous and include inflammation caused by infection with toxoplasmosis, fungal organisms, Mycoplasma haemofelis, ehrlichiosis, hyperplasia (e.g., hemolytic disorders), systemic lupus erythematosus, chronic bacteremic disorders, congestion (e.g., from impaired venous drainage), portal hypertension, splenic torsion/infarction, anesthetic drugs, and infiltrative disease (e.g., primary and metastatic neoplasia, and extramedullary hematopoiesis).169-173 Lymphosarcoma, leukemia, systemic mastocytosis, multiple myeloma, and malignant histiocytosis can all result in diffuse neoplastic splenic enlargement. Splenomegaly in the cat is less likely to be benign, because the feline spleen is considered nonsinusoidal and less capable of storing large amounts of blood.172,174 Compared with the dog, generalized splenomegaly in the cat is most commonly caused by neoplastic infiltration, primarily lymphosarcoma and mast cell tumor (see Fig. 40.44B).175,176
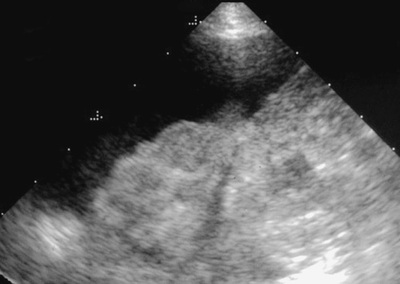
Splenic torsion occurs when the spleen rotates around its mesenteric axis, resulting in complete occlusion of venous drainage and eventual arterial occlusion. This results in marked splenomegaly, as well as an atypical splenic location.177,178 The spleen may undergo torsion on its own or in association with gastric volvulus. It may acquire a reverse C-shape on the lateral view or may simply appear as a mass in the ventral abdomen (Fig. 40.45). The proximal extremity of the spleen may not be visualized in the normal left craniodorsal location because of the malposition or accompanying peritoneal fluid. If gas-producing bacteria proliferate within the ischemic parenchyma, emphysematous changes may occur and result in a mottled or foamy radiographic appearance (see Fig. 40.45B).29,179 CT has been used in the diagnosis of splenic torsion, and the findings include splenomegaly, a corkscrew-like soft tissue mass representing the rotated splenic pedicle, and lack of contrast enhancement.180
A splenic mass results in local displacement of adjacent viscera according to the location of the mass in the spleen (Figs. 40.46 and 40.47). Although often sharply marginated, the splenic mass may be obscured partially or completely by secondary peritoneal hemorrhage. A mass in the body or distal extremity of the spleen is a very common cause of a ventral abdominal mass, and on the lateral view results in dorsal and caudal displacement of the jejunum. On VD views, distal splenic masses may be midline or to the right or left of midline.

Masses of the proximal extremity of the spleen are less common than distal masses and may displace the stomach cranially with caudal, medial, and ventral displacement of the jejunum and descending colon. The left kidney may be displaced caudally as well.
Differentials for a splenic mass include benign and neoplastic conditions. Primary and metastatic neoplasia, hematoma, nodular hyperplasia, extramedullary hematopoiesis, and abscess are all considerations.176,181-183 Hemangiosarcoma is the most common neoplasm of the canine spleen, but splenic hematoma and hyperplastic nodules are the most common cause of splenic lesions.183 Peritoneal effusion may accompany both benign and neoplastic diseases.
Normal splenic opacity is that of soft tissue. Mineralization of the spleen may be the result of dystrophic calcification of abscesses, hematomas, fungal granulomas, or neoplastic masses.16 Gas within the spleen may result from splenic torsion (see Fig. 40.45B). As noted in the liver, gas may ascend into the portovenous circulation and affect the spleen.1,29,30 Gas-forming organisms in splenic abscesses can create focal radiolucencies.
Ultrasound of the Spleen
The spleen is well suited to ultrasound examination because of the superficial location and lack of intervening gas-containing structures. Higher frequency transducers may be used because of the superficial location.
Splenic location varies. The proximal extremity of the spleen is in the left craniolateral abdominal quadrant and may be beneath the costal arch. Intercostal windows are sometimes necessary in deep-chested dogs. The canine splenic body and distal extremity may extend caudally along the left lateral abdomen or move medially across the ventral midline. It often appears folded on itself. The feline spleen is more consistent in location, along the left lateral abdominal wall, and rarely folds on itself unless enlarged.
The splenic parenchyma has a uniform echotexture with a fine, dense pattern.184,185 Echogenicity of the canine spleen is slightly greater than the liver and renal cortex (Fig. 40.48). Renal cortical echogenicity of some normal cats may equal or exceed splenic echogenicity due to lipid deposition.60,61,172 Splenic margins are linear and smooth, with mild indentations noted along the mesenteric border where splenic veins exit. Splenic arteries are not usually seen without Doppler interrogation. Tissue surrounding splenic veins at the hilus may be highly echogenic normally because of capsular invagination and fat.184 Splenic size is subjective and based on sonographer experience.
When enlarged, the spleen may extend caudally or more completely cover the ventral abdomen. Splenic borders become rounded or blunted, or appear to bulge from the capsule, compared with the normal sharp, linear appearance (Fig. 40.49). The spleen has no absolute size limits in the dog. The normal feline spleen is less variable in size than the dog, and objective measurements have been determined. Mean splenic height, measured in the transverse plane, in the proximal third of the spleen, adjacent to a splenic vein, is 7.1 mm, with a range from 5.1 to 9.1 mm (see Fig. 40.48C).186 Similar splenic measurements were determined in a second study, where normal feline splenic height was 8.2 ±1.4 mm (range: 5.3 to 11.1 mm).172
Abnormal Splenic Sonographic Findings
Diffuse Disease
As in the liver, diffuse splenic disease potentially causes changes in size, shape, or echogenicity. However, these changes may be difficult to identify or characterize, especially with mild or early disease. Splenomegaly with either normal or decreased echogenicity has numerous causes, including congestion, neoplasia, infarction, inflammation, immune-mediated disease, chronic hemolytic anemia, parasitic infection, extramedullary hematopoiesis, and bacterial or fungal infection.83,173,175,177,184,185,187-193
Extramedullary hematopoiesis often results in generalized splenomegaly, with normal echogenicity, or a coarse or mottled appearance. Lymphoid hyperplasia can also have a diffuse mottled appearance.
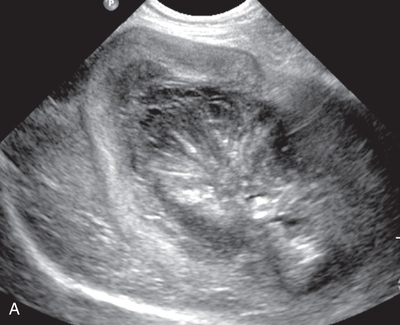
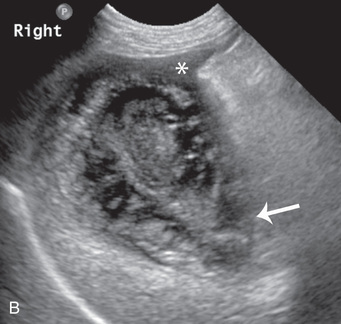
Splenic congestion as a result of a phenothiazine and pentobarbital drug group results in splenomegaly with no associated change in echogenicity.187 Congestion from portal hypertension appears similar, but dilated splenic veins may also be present. Splenic torsion, a form of splenic congestion, has a variety of appearances.177,178,188 Splenomegaly may be the only finding. However, splenomegaly with a diffuse hypoechoic parenchyma, separated by linear echogenicities that represent dilated hyperechoic vessels, is highly suggestive of torsion (Fig. 40.50). Splenic veins may be dilated with visible intravascular echogenicities representing formed thrombi or static echogenic blood. Complete absence of flow at the splenic hilus is also common, as is accompanying peritoneal fluid. A hyperechoic triangular area surrounding the splenic veins has been associated with splenic torsion.189 Gas within the parenchyma may indicate the presence of necrosis and gas-forming organisms. Diffuse splenic infarction as a result of other disease processes can have an identical appearance.190,191
Diffuse neoplastic infiltration of the spleen has a variety of appearances, and tumor type cannot be determined from the ultrasound appearance.83,88,173,175,184,185,192,193
Lymphosarcoma, mast cell tumor, malignant histiocytosis, leukemic infiltration, and multiple myeloma can all result in splenomegaly with normal or decreased echogenicity. The parenchyma may appear uneven or coarse. Focal or multifocal nodules of varying sizes that are usually hypoechoic may also be present (Fig. 40.51; see Fig. 40.49). A diffuse nodular pattern of small hypoechoic nodules, termed a Swiss cheese appearance, is suggestive of lymphosarcoma, but other tumors (e.g., malignant histiocytosis and mast cell tumor) must also be considered.173
Splenitis due to fungal infection, such as histoplasmosis in cats, can result in irregular splenomegaly with a hypoechoic to subtle mottled or, rarely, discrete nodular appearance. These changes are most apparent when using a transducer frequency of at least 9 MHz frequency (Fig. 40.52).194
Diffusely increased splenic echogenicity is less common but may be seen with chronic vascular compromise, peritonitis, infection, or diffuse nonneoplastic infiltrative disease, such as extramedullary hematopoiesis.184,185
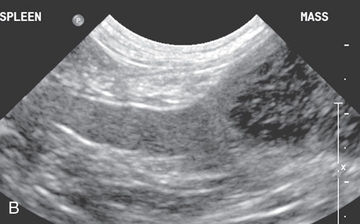
As in the liver, numerous considerations exist for focal disease, including primary and secondary neoplasia, nodular hyperplasia, hematoma, focal extramedullary hematopoiesis, abscess, and infarction (Figs. 40.53 and 40.54; see Figs. 40.51 and 40.52). Lymphosarcoma, one of the most common splenic tumors, has a variety of appearances. In addition to the diffuse changes described previously, lymphosarcoma may also produce focal hypoechoic or anechoic nodules or a single complex or cavitated mass.88,173,175 Histiocytic sarcoma also creates focal hypoechoic splenic nodules/masses. Splenic masses attributable to hemangiosarcoma are typically complex with hypoechoic, hyperechoic, and anechoic areas caused by hemorrhage, necrosis, and fibrotic or calcified tissue (see Fig. 40.54).184,185 Peritoneal fluid often accompanies hemangiosarcoma, and the liver should be evaluated carefully for metastasis. Splenic hematomas are similar in appearance to those described in the liver and may be associated with acute or previous trauma or develop from neoplastic disease (Fig. 40.55).181,184,185,195 Splenic hematomas are indistinguishable sonographically from splenic hemangiosarcoma, and both may enlarge over time.196
Metastatic carcinoma can result in variably sized hypoechoic nodules; target-like nodular lesions can also occur (see Fig. 40.51C).
Splenic abscesses are uncommon, but they can have a complex appearance similar to hemangiosarcoma or hematoma.184,185,197 Splenic abscesses can vary from a simple hypoechoic, poorly-defined area to a complex, cavitated mass. Echogenic areas with shadowing within the mass may indicate gas formation (Fig. 40.56). Myelolipomas are fatty, hyperechoic nodules occasionally seen in the normal spleen, especially along the peripheral margin or adjacent to vessels (Fig. 40.57).198,199 Splenic myelolipomas are benign incidental findings but can be quite large. Rarely, mast cell tumors have been reported to cause hyperechoic nodules in the spleen.175

The echogenicity of focal splenic infarction changes over time. Initially infarcts are hypoechoic and may appear as a well-demarcated round or bulging mass or simple focal enlargement of the spleen (Fig. 40.58).179,180 With age, infarcts become increasingly echogenic and often are demarcated sharply from the normal splenic parenchyma. With color Doppler interrogation, there is a lack of blood flow in the infarcted area.
Nodular hyperplasia in the spleen has a similar appearance to that in the liver, and it is likely the most common abnormality of the spleen identified on ultrasound.55 The splenic border may simply be smoothly irregular or isoechoic; hypoechoic or hyperechoic nodules may be present. Hyperplastic nodules can be quite large and complex. Extramedullary hematopoiesis can appear as hypoechoic, hyperechoic, or mixed echogenicity nodules and/or masses (see Fig. 40.52).
Metastatic carcinoma can result in variably sized hypoechoic nodules; target-like nodular lesions can also occur (see Fig. 40.51C).
As in the liver, splenic ultrasound is sensitive but not specific. It is critical to remember that the ultrasound appearance of both diffuse and focal splenic disease is nonspecific, with a large amount of overlap between normal and diseased spleen and between various splenic diseases. A normal ultrasound appearance does not rule out disease. Splenic nodules/masses are commonly encountered incidentally, and they are frequently benign.200 Tissue samples are necessary for a more definitive diagnosis. Although diagnosis of diffuse splenic disease (e.g., lymphosarcoma or extramedullary hematopoiesis) may be achieved with needle aspiration, cavitated mass lesions (e.g., hemangiosarcoma or hematoma) may be diagnosed more accurately by splenectomy and histopathologic evaluation.201 Tru-Cut biopsies of the spleen using 18 g needles have been reported with minimal complications.203