Image Formation and Radiographic Quality
OBJECTIVES
- 1. Define all the key terms in this chapter.
- 2. State all the important relationships in this chapter.
- 3. Describe the process of radiographic image formation.
- 4. Explain the process of beam attenuation.
- 5. Identify the factors that affect beam attenuation.
- 6. Describe the x-ray interactions termed photoelectric effect and Compton effect.
- 7. Define the term ionization.
- 8. State the composition of exit radiation.
- 9. Explain the process of creating the various shades of image brightness.
- 10. Describe the necessary components of radiographic quality.
- 11. Explain the importance of brightness and contrast to image quality.
- 12. Differentiate between high-contrast and low-contrast images.
- 13. Explain the importance of spatial resolution and both size and shape distortion to image quality.
- 14. State the effects of quantum noise, scatter, and image artifacts on image quality.
- 15. Recognize the advantages of digital imaging and the limitations of film-screen imaging.
- 16. Differentiate radiographic imaging from dynamic imaging.
KEY TERMS
absorption; artifact; attenuation; brightness; coherent scattering; Compton effect; Compton electron; contrast resolution; differential absorption; distortion; dynamic range; elongation; exit radiation; fluoroscopy; fog; foreshortening; grayscale; high-contrast images; image receptor (IR); invisible image; ionization; latent image; low-contrast images; magnification; manifest image; photoelectric effect; photoelectron; quantum noise; remnant radiation; saturation; scattering; secondary electron; shape distortion; size distortion; spatial resolution; subject contrast; tissue density; transmission; visible image
To produce a radiographic image, x-ray photons must pass through tissue and interact with an image receptor (IR), a device that receives the radiation leaving the patient. Both the quantity and the quality of the primary x-ray beam affect its interactions within the various tissues that make up anatomic parts. In addition, the composition of the anatomic tissues affects the x-ray beam interaction. The absorption characteristics of the anatomic part are determined by its thickness, atomic number of the atoms contained within it, and tissue density or compactness of the cellular structures. Finally, the radiation that exits the patient is composed of varying energies and interacts with the IR to form a latent or invisible image and must be processed.
A visible radiographic image is produced following the processing of the latent or invisible image. Depending on the type of imaging system, the acquiring, processing, and displaying of images can vary significantly. However, the attributes of a quality radiographic image are similar regardless of the type of imaging system. This chapter focuses on how images are formed and their quality after processing.
IMAGE FORMATION
Differential Absorption
The process of image formation is a result of differential absorption of the x-ray beam as it interacts with anatomic tissue. Differential absorption is a process whereby some amount of the x-ray beam is absorbed in the tissue, and some passes through (transmits) the anatomic part. The term differential is used because varying anatomic parts do not absorb the primary beam to the same degree. Anatomic parts composed of bone absorb more x-ray photons than parts filled with air. Differential absorption of the primary x-ray beam creates an image that structurally represents the anatomic area of interest (Fig. 3-1).
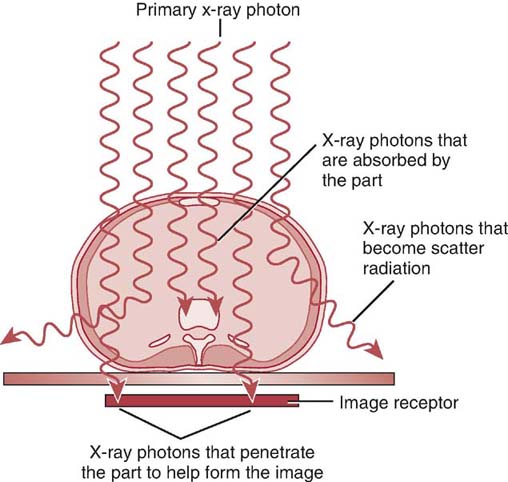
FIG. 3-1 As the primary x-ray beam interacts with an anatomic part, photons are absorbed, scattered, and transmitted. The differences in the absorption characteristics of the anatomic part create an image that structurally represents the part. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Creating a radiographic image by differential absorption requires several processes to occur: beam attenuation, absorption, and transmission.
Beam Attenuation
As the primary x-ray beam passes through anatomic tissue, it loses some of its energy (intensity). Fewer x-ray photons remain in the beam after it interacts with anatomic tissue. This reduction in the intensity or number of photons in the primary x-ray beam is known as attenuation. Beam attenuation occurs as a result of the photon interactions with the atomic structures that comprise the tissues. Two distinct processes occur during beam attenuation: absorption and scattering.
Absorption
As the energy of the primary x-ray beam is deposited within the atoms comprising the tissue, some x-ray photons are completely absorbed. Complete absorption of the incoming x-ray photon occurs when it has enough energy to remove (eject) an inner-shell electron. The ejected electron is called a photoelectron, and it quickly loses energy by interacting with nearby tissues. The ability to remove (eject) electrons, known as ionization, is a characteristic of x-rays. In the diagnostic range, this x-ray interaction with matter is known as the photoelectric effect.
With the photoelectric effect, an ionized atom has a vacancy, or electron hole, in its inner shell. An electron from an outer shell drops down to fill this vacancy. Because of the difference in binding energies between the two electron shells, a secondary x-ray photon is emitted (Fig. 3-2). This secondary x-ray photon typically has a very low energy and is unlikely to exit the patient.
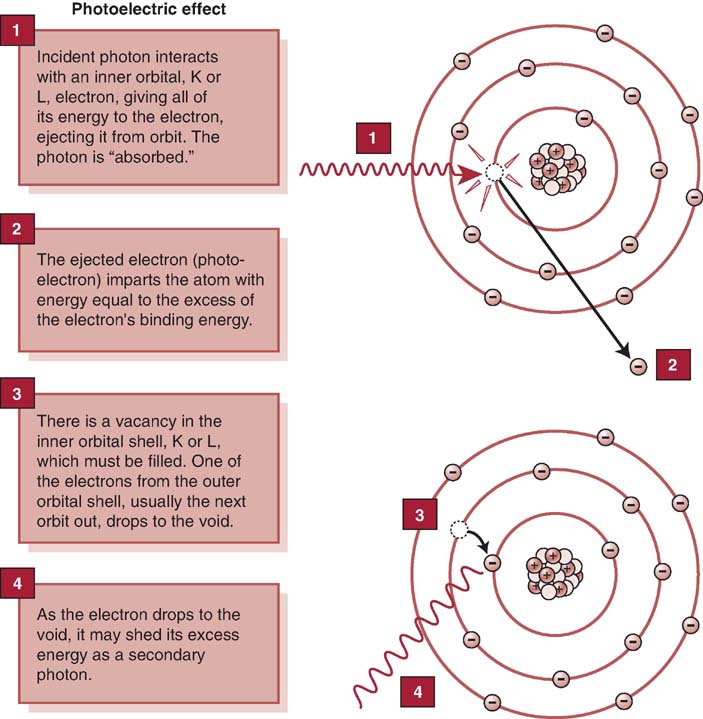
FIG. 3-2 The photoelectric effect is responsible for total absorption of the incoming x-ray photon. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
The probability of total photon absorption by the photoelectric effect depends on the energy of the incoming x-ray photon and the atomic number of the anatomic tissue. The energy of the incoming x-ray photon must be at least equal to the binding energy of the inner-shell electron. After absorption of a portion of x-ray photons, the overall quantity of the primary beam decreases as it passes through the anatomic part.
Scattering
Some incoming photons are not absorbed but lose energy and change direction during interactions with the atoms comprising the tissue. This process is called scattering. It results from an interaction between diagnostic x-rays and matter, known as the Compton effect. The loss of energy of the incoming photon occurs when it ejects an outer-shell electron from a tissue atom. The ejected electron is called a Compton electron or secondary electron. The remaining lower-energy x-ray photon changes direction and may leave the anatomic part and interact with the IR (Fig. 3-3).
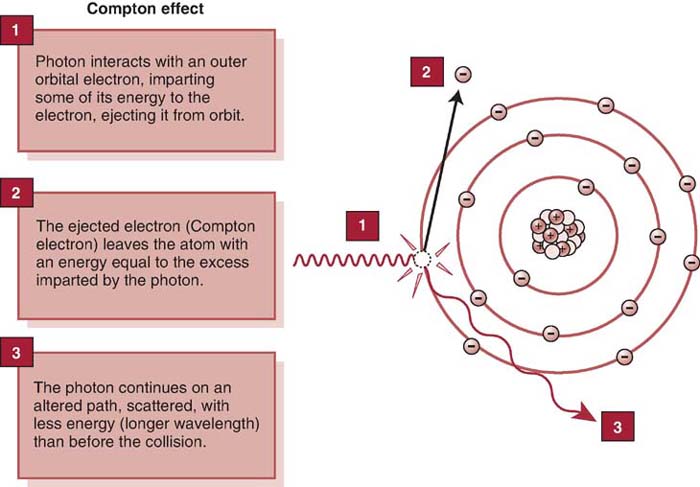
FIG. 3-3 During the Compton effect, the incoming photon loses energy and changes its direction. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Compton interactions can occur at any diagnostic x-ray energy and are an important interaction in radiography. The probability of a Compton interaction occurring depends on the energy of the incoming photon. It does not depend on the atomic number of the anatomic tissue. For example, a Compton interaction is just as likely to occur in soft tissue as in tissue composed of bone; however, if the tissue has more complex atoms, there are more opportunities for interaction. With higher atomic number particles, such as bone, if the energy of the incoming photon is sufficiently high, more scatter will occur; otherwise, more absorption will occur. For Compton interactions to occur, the energy of the photon is more important, whereas the atomic number of elements in the tissue is only related to the opportunity for x-ray interactions. When a higher kilovoltage peak (kVp) within the diagnostic range is used, the overall number of x-ray interactions within matter decrease because of increased photon transmission; however, the percentage of photoelectric interactions generally decreases at higher kilovoltages within the diagnostic range, whereas the percentage of Compton interactions is likely to increase at higher kilovoltages within the diagnostic range. Box 3-1 compares photoelectric and Compton interactions. Scattered and secondary radiations provide no useful information and must be controlled during radiographic imaging.
Coherent scattering is an interaction that occurs with low-energy x-rays, typically below the diagnostic range, also known as classical scattering. The incoming photon interacts with the atom, causing it to become excited. The x-ray does not lose energy, but it changes direction (Fig. 3-4). Coherent scattering could occur within the diagnostic range of the x-rays and may interact with the IR, but it is not considered an important interaction in radiography.
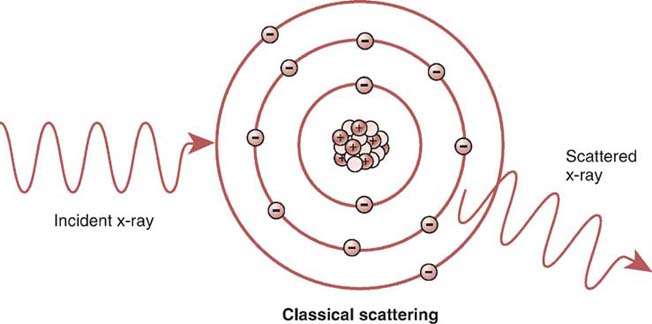
FIG. 3-4 Coherent (classical) scattering. The incoming photon interacts with the atom, causing it to become excited. The x-ray does not lose energy, but it changes direction. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
If a scattered photon strikes the IR, it does not contribute any useful information about the anatomic area of interest. If scattered photons are absorbed within the anatomic tissue, they contribute to radiation exposure to the patient. In addition, if the scattered photon leaves the patient and does not strike the IR, it could contribute to radiation exposure of anyone near the patient.
The preceding discussion focused on photon interactions that occur in radiography when using x-ray energies within the moderate range. X-rays with energies above the diagnostic range result in other interactions, namely, pair production and photodisintegration. X-ray interactions above the diagnostic range are important in positron emission tomography (PET) and radiation therapy.
Factors Affecting Beam Attenuation
The amount of x-ray beam attenuation is affected by the thickness of the anatomic part, the atomic number of the atoms contained within it, its tissue density, and the energy of the x-ray beam.
Tissue Thickness
Increasing the thickness of a given anatomic tissue increases beam attenuation by either absorption or scattering (Fig. 3-5). X-rays are exponentially attenuated and are generally reduced by approximately 50% for each 4 to 5 cm (1.6–2 inches) of tissue thickness (Fig. 3-6). More x-rays are needed to produce a radiographic image for a thicker anatomic part. Fewer x-rays are needed to produce a radiographic image for a thinner anatomic part.
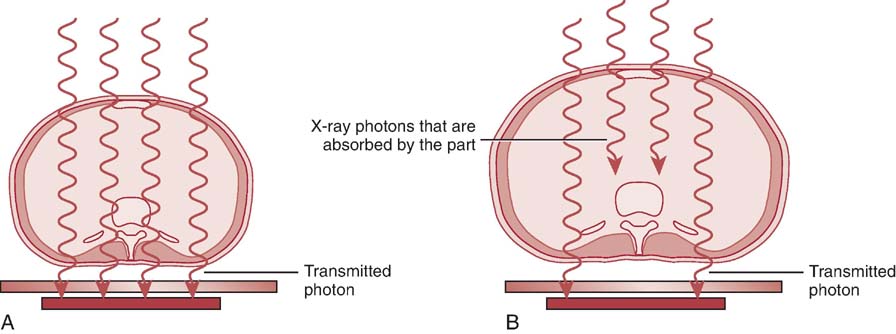
FIG. 3-5 A, A thinner patient transmits more radiation than a thicker patient. B, A thicker patient absorbs more radiation than a thinner patient. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
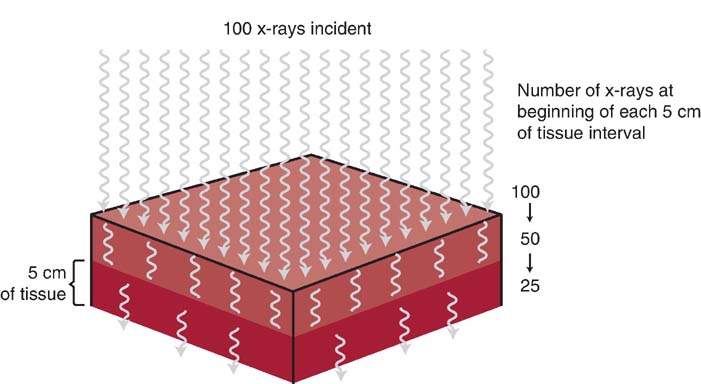
FIG. 3-6 X-rays are exponentially attenuated and generally reduced by approximately 50% for each 4 to 5 cm (1.6–2 inches) of tissue thickness. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Type of Tissue
Tissues composed of elements with a higher atomic number, such as bone (which has an effective atomic number of 13.8), attenuate the x-ray beam more than tissue composed of elements with a lower atomic number, such as fat (which has an effective atomic number of 6.3). The higher atomic number indicates there are more atomic particles for interactions with x-ray photons. X-ray absorption is more likely to occur in tissues with a higher effective atomic number than in those with a lower effective atomic number (Fig. 3-7).
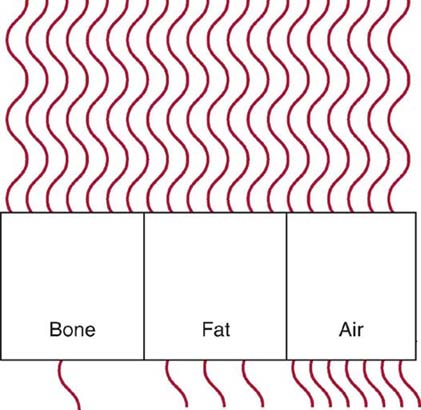
FIG. 3-7 Bone absorbs more radiation than fat and air. Air transmits more radiation than fat and bone. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Tissue density (matter per unit volume), or the compactness of atomic particles composing the anatomic part, also affects the amount of beam attenuation. For example, muscle (effective atomic number 7.4) and fat (effective atomic number 6.3) tissue are similar in effective atomic number; however, their atomic particles differ in compactness, and their tissue densities vary. Muscle tissue has atomic particles that are more densely packed or compact and therefore attenuate the x-ray beam more than fat cells. Bone is composed of tissue with a higher atomic number, and the atomic particles are more compacted or densely packed. Anatomic tissues are typically ranked on the basis of their attenuation properties. Four substances account for most of the beam attenuation in the human body: bone, muscle, fat, and air. Bone attenuates the x-ray beam more than muscle, muscle attenuates the x-ray beam more than fat, and fat attenuates the x-ray beam more than air. The effective atomic number of the anatomic part and its tissue density affect x-ray beam attenuation.
X-ray Beam Quality
The quality of the x-ray beam or its penetrating ability affects its interaction with anatomic tissue. Higher-penetrating x-rays (shorter wavelength with higher frequency) are more likely to be transmitted through anatomic tissue without interacting with the tissues' atomic structures. Lower-penetrating x-rays (longer wavelength with lower frequency) are more likely to interact with the atomic structures and be absorbed. The kilovoltage selected during x-ray production determines the energy or penetrability of the x-ray photon, and this affects its attenuation in anatomic tissue (Fig. 3-8). Beam attenuation decreases with a higher-energy x-ray beam and increases with a lower-energy x-ray beam. See Table 3-1 for factors affecting beam attenuation.
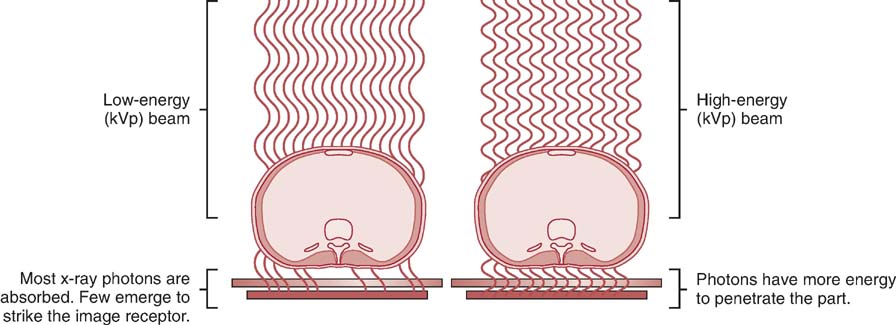
FIG. 3-8 The energy of the x-ray beam affects its interaction within anatomic tissues. Lower kVp results in more absorption in the tissue; higher kVp results in more transmission through the tissue. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Table 3-1
| Factor | Beam Attenuation | Absorption | Transmission |
|---|---|---|---|
| Tissue Thickness | |||
| • Increasing thickness | ↑ | ↑ | ↓ |
| • Decreasing thickness | ↓ | ↓ | ↑ |
| Tissue Atomic Number | |||
| • Increasing atomic number | ↑ | ↑ | ↓ |
| • Decreasing atomic number | ↓ | ↓ | ↑ |
| Tissue Density | |||
| • Increasing tissue density | ↑ | ↑ | ↓ |
| • Decreasing tissue density | ↓ | ↓ | ↑ |
| X-ray Beam Quality | |||
| • Increasing beam quality | ↓ | ↓ | ↑ |
| • Decreasing beam quality | ↑ | ↑ | ↓ |
Transmission
If the incoming x-ray photon passes through the anatomic part without any interaction with the atomic structures, it is called transmission (Fig. 3-9). The combination of absorption and transmission of the x-ray beam provides an image that structurally represents the anatomic part. Because scatter radiation is also a process that occurs during interaction of the x-ray beam and the anatomic part, the quality of the image created is compromised if scattered photons strike the IR.
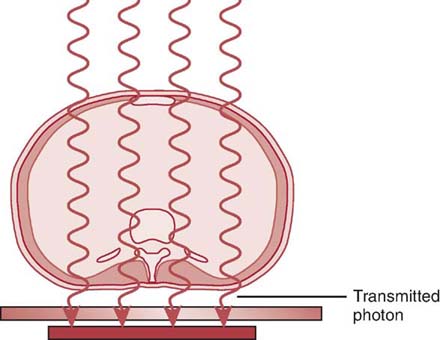
FIG. 3-9 Some incoming x-ray photons pass through the anatomic part without any interactions. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Exit Radiation
When the attenuated x-ray beam leaves the patient, the remaining x-ray beam, referred to as exit radiation or remnant radiation, is composed of both transmitted and scattered radiation (Fig. 3-10). The varying amounts of transmitted and absorbed radiation (differential absorption) create an image that structurally represents the anatomic area of interest. Scatter exit radiation (Compton interactions) that reach the IR do not provide any diagnostic information about the anatomic area. Scatter radiation creates unwanted exposure on the image called fog. Methods used to decrease the amount of scatter radiation reaching the IR are discussed in Chapter 7.
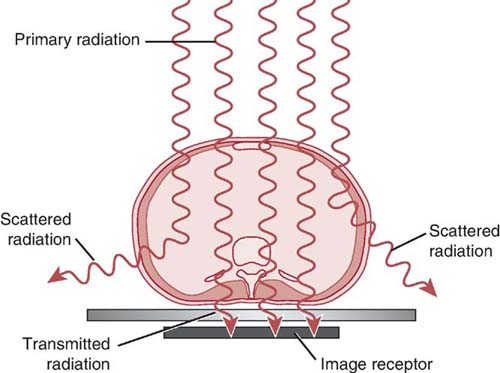
FIG. 3-10 Radiation that exits the anatomic part comprises transmitted and scattered radiation.(From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
The areas within the anatomic tissue that absorb incoming x-ray photons (photoelectric effect) create the light areas (increased brightness) on the displayed image. The incoming x-ray photons that are transmitted create dark areas (decreased brightness) on the displayed image. Anatomic tissues that vary in absorption and transmission create a range of dark and light areas (shades of gray) (Fig. 3-11). The various shades of gray recorded in the radiographic image make anatomic tissues visible. Skeletal bones are differentiated from the air-filled lungs because of their differences in absorption and transmission.
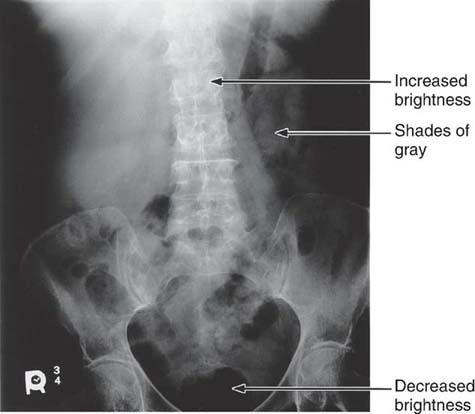
FIG. 3-11 Anatomic tissues vary in their absorption and transmission of x-ray photons to create the range of brightness or gray levels that structurally represent the anatomic area of interest. Increased brightness represents absorbed radiation, whereas decreased brightness represents transmitted radiation. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Less than 5% of the primary x-ray beam interacting with the anatomic part actually reaches the IR, and an even lower percentage is used to create the radiographic image. The exit radiation interacting with an IR creates the latent image, or invisible image. This latent image is not visible until it is processed to produce the manifest image, or visible image. IRs, acquisition, processing, and display are discussed in Chapters 4 and 5.
RADIOGRAPHIC QUALITY
A quality radiographic image accurately represents the anatomic area of interest, and information is well visualized for diagnosis. It is important to identify the attributes of a quality radiographic image before comprehending all the factors that affect its quality.
The visibility of the anatomic structures and the accuracy of their recorded structural lines (sharpness) determine the overall quality of the radiographic image. The visibility of the anatomic detail refers to the brightness and contrast of the image, and the accuracy of the structural lines is achieved by maximizing the amount of spatial resolution and minimizing the amount of distortion (Fig. 3-12). Visibility of the anatomic structures is achieved by the proper balance of image brightness and contrast.
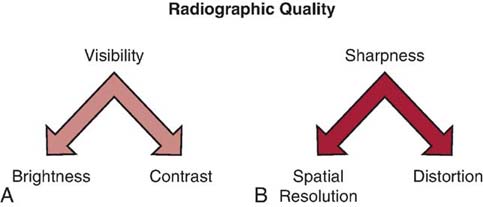
FIG. 3-12 Factors affecting radiographic image quality. A, Visibility factors. B, Sharpness factors. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
Image Brightness
Because the digital image is composed of numerical data, the brightness level displayed on the computer monitor can be easily altered to visualize the range of anatomic structures recorded. Brightness is the amount of luminance (light emission) of a display monitor.
A radiographic image must have sufficient brightness to visualize the anatomic structures of interest (Fig. 3-13). A radiographic image that is too light has too much brightness to visualize the structures of the anatomic part (Fig. 3-14). Conversely, a radiographic image that is too dark has insufficient brightness, and the anatomic part cannot be well visualized (Fig. 3-15).The radiographer must evaluate the overall brightness in the image to determine whether it is sufficient to visualize the anatomic area of interest. He or she then decides whether the radiographic image is diagnostic or unacceptable.

FIG. 3-13 Brightness. Radiographic image with sufficient brightness. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 3, St. Louis, 2020, Mosby.)

FIG. 3-14 Brightness. Radiographic image with excessive brightness. Brightness altered with postprocessing. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 3, St. Louis, 2020, Mosby.)

FIG. 3-15 Brightness. Radiographic image with insufficient brightness. Brightness altered with postprocessing. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 3, St. Louis, 2020, Mosby.)
The x-ray beam that exits the patient contains a wide range of x-ray intensities (often varying by more than 1000-fold). To adequately capture these intensity extremes, a receptor with a wide dynamic range is required. Because digital imaging provides a wide dynamic range and the computer can adjust for exposure errors, a greater margin of error exists for exposure techniques to yield acceptable brightness levels.
Because digital image processing can compensate for exposure errors, the image may display the appropriate level of brightness yet also have been over- or underexposed. As a result, the radiographer may be unaware of the exposure error. However, extreme exposure errors can affect image quality and be visible to the radiographer. When exposure to the digital IR is too low for the anatomic area, excessive quantum noise (discussed later in this chapter) may be visible. When the IR is extremely overexposed, saturation may occur where the image cannot be properly processed, and the quality is severely degraded (Fig. 3-16).

FIG. 3-16 Saturation. A, Radiographic image with sufficient exposure. B, Radiographic image with extreme overexposure; the quality is severely degraded. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 3, St. Louis, 2020, Mosby.
Image Contrast
In addition to sufficient brightness, the radiographic image must exhibit differences in the brightness levels (image contrast) to differentiate among anatomic tissues. The range of brightness levels is a result of the tissues' differential absorption of the x-ray photons. An image that has sufficient brightness but no differences appears as a homogeneous object (Fig. 3-17). This appearance indicates that the absorption characteristics of the object are equal. When the absorption characteristics of an object differ, the image has varying levels of brightness (Fig. 3-18). The anatomic tissues are easily differentiated because of these differences in brightness levels (i.e., contrast). Tissues that attenuate the x-ray beam equally are more difficult to visualize because the brightness levels are too similar to differentiate.
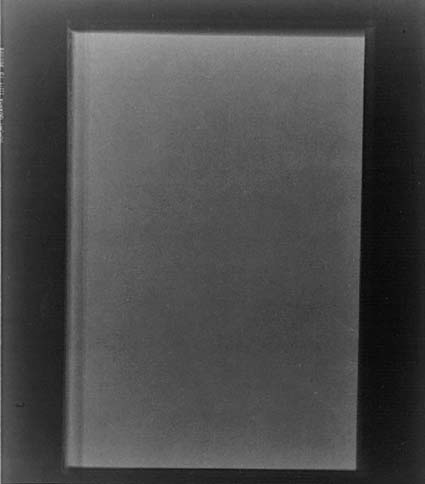
FIG. 3-17 Radiograph of a homogeneous object having no differences in brightness levels.
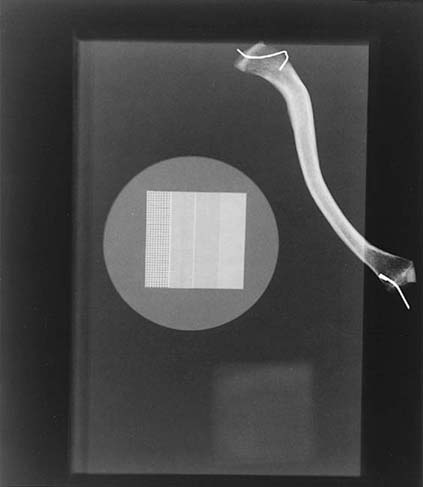
FIG. 3-18 An object with different absorption characteristics produces an image with varying brightness levels.
Radiographic contrast is the combined result of multiple factors associated with the anatomic structure, radiation quality, image-receptor capabilities, computer processing, and display. Subject contrast refers to the absorption characteristics of the anatomic tissue imaged and the quality of the x-ray beam. Differences in tissue thickness, density, and effective atomic number contribute to subject contrast (Fig. 3-19). For example, the chest is composed of tissues that vary greatly in x-ray lucency, such as the air-filled lungs, the heart, and the bony thorax. This anatomic region creates high subject contrast because the tissues attenuate the x-ray beam very differently compared with the abdomen for the same beam quality. When the thorax is imaged, great differences in brightness levels are recorded for the varying tissues (Fig. 3-20). The abdomen is composed of tissues that attenuate the x-ray beam similarly and is considered to be a region of low subject contrast. The brightness levels representing the organs in the abdomen are more similar (Fig. 3-21). Therefore, it is difficult to distinguish the stomach from the kidneys. As previously discussed, the quality of the x-ray beam also affects its attenuation in tissues, which alters subject contrast. Increasing the penetrating power of the x-ray beam decreases attenuation, reduces absorption, and increases x-ray transmission, resulting in fewer differences in the brightness levels recorded in the radiographic image.
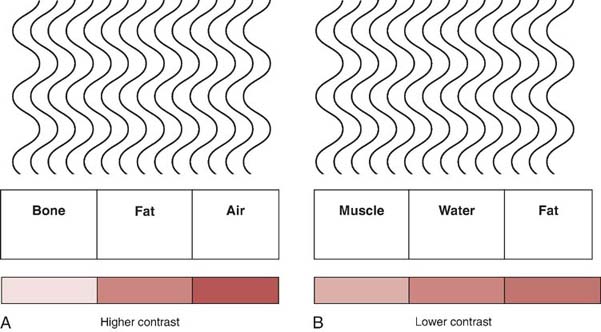
FIG. 3-19 A, Higher contrast resulting from great differences in radiation absorption between tissues that vary greatly in composition. B, Lower contrast resulting from fewer differences in the radiation absorption for tissues that are more similarly composed.

FIG. 3-20 The thorax is an anatomic area of high subject contrast because there is great variation in tissue composition.

FIG. 3-21 The abdomen is an anatomic area of low subject contrast because it is composed of similar tissue types.
Brightness is easily measurable; however, contrast is a more complex attribute. Evaluating radiographic quality in terms of contrast is more subjective. (It is affected by individual preferences.) The level of radiographic contrast desired in an image is determined by the composition of the anatomic tissue to be imaged and the amount of information needed to visualize the tissue for an accurate diagnosis. For example, the level of contrast desired in a chest image is different from that required in an extremity image.
Radiographic or image contrast is a term used to describe variations in brightness levels. In digital imaging, the number of different shades of gray that can be stored and displayed by a computer system is termed grayscale. Because the digital image is processed and reconstructed in the computer as digital data, its grayscale or contrast can be altered. Digital images can be displayed to show a range of gray levels from high to low contrast. High-contrast images display fewer shades of gray but greater differences among them (Fig. 3-22). Low-contrast images display a greater number of gray shades but smaller differences among them (Fig. 3-23).
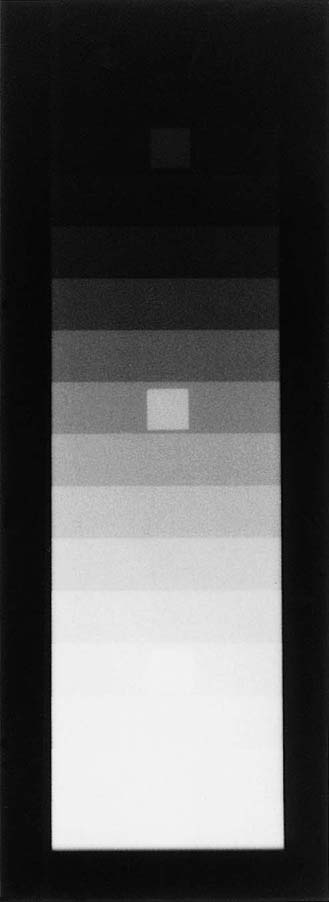
FIG. 3-22 High-contrast image showing fewer gray levels and greater differences among them.
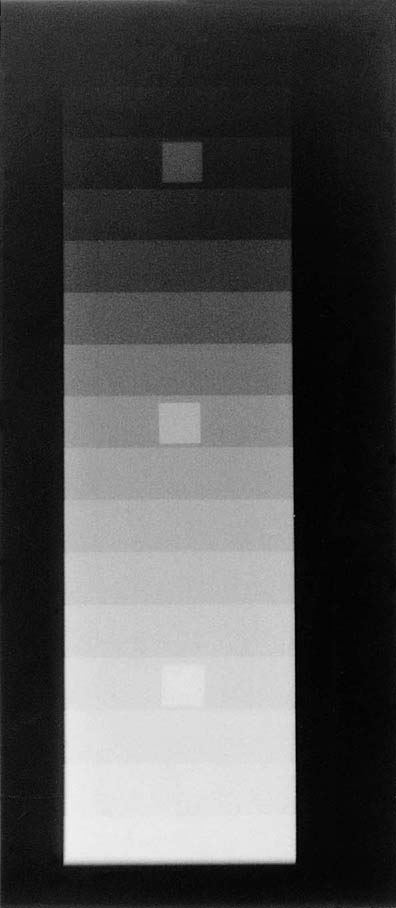
FIG. 3-23 Low-contrast image showing many gray levels and few differences among them.
Contrast resolution is a term associated with digital imaging and is used to describe the ability of the imaging system to distinguish between small objects that attenuate the x-ray beam similarly. The contrast resolution of the imaging system determines the level of visibility of small objects having similar brightness levels or shades of gray. Increasing the number of shades of gray increases the contrast resolution within the image. An image with increased contrast resolution increases the visibility of anatomic structures and the ability to distinguish among small anatomic areas of interest.
Spatial Resolution
The quality of a radiographic image depends on both the visibility and the accuracy of the anatomic structural lines (sharpness) displayed. Adequate visualization of the anatomic area of interest (brightness and contrast) is just one component of radiographic quality. To produce a quality radiographic image, the anatomic structures must be accurately recorded and with the greatest amount of sharpness. Spatial resolution is a term used to evaluate the accuracy of the anatomic structural lines displayed. Spatial resolution refers to the smallest object that can be detected in an image.
The ability of a radiographic image to demonstrate sharp lines determines the quality of the spatial resolution. The imaging process makes it impossible to produce a radiographic image without a certain degree of unsharpness. A radiographic image that has greater spatial resolution minimizes the unsharpness of the anatomic structural lines.
A radiographic image cannot be an exact reconstruction of the anatomic structure. Some information is always lost during the process of image formation. In addition, factors such as patient motion increase the amount of unsharpness recorded in the image (Fig. 3-24). Eliminating motion unsharpness is an important skill required of the radiographer. Voluntary motion, under the control of the patient, is best alleviated by effective communication. However, in some situations such as with children and older adults, patients may have difficulty controlling voluntary motion. Reducing the exposure time and using immobilization devices may be needed in addition to effective communication. Reducing the exposure time is the best method to eliminate motion unsharpness for involuntary motion, not under the control of the patient. A less common type of motion unsharpness is a result of equipment malfunction and is more difficult to identify.

FIG. 3-24 Image showing motion unsharpness. (From Mosby's Instructional Radiographic Series: Radiographic Imaging, St. Louis, 1998, Mosby.)
It is the radiographer's responsibility to minimize the amount of information lost by manipulating the factors that affect the sharpness of the displayed image. Diagnostic quality is achieved by maximizing the amount of spatial resolution and minimizing the amount of image distortion.
The sharpness and visibility of recorded detail have typically been discussed as two separate qualities of a radiographic image. Generally, this separation remains true except when imaging small anatomic structures. A small anatomic structure is best visualized when its brightness varies significantly from the background. If unsharpness is increased, the visibility of small anatomic details is compromised. An increase in the amount of unsharpness displayed in the image decreases the contrast of small anatomic structures, reducing the overall visibility of the structural lines. The spreading of the structural lines with increased unsharpness decreases the differences in brightness levels between the structural lines of the area of interest and the background. As a result, the difference in brightness levels between the area of interest and the background lessens (low contrast) and the visibility of the anatomic structure is reduced (Fig. 3-25).
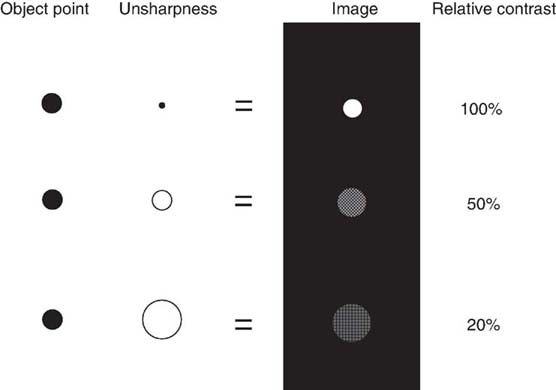
FIG. 3-25 Unsharpness and image contrast. Increasing the amount of unsharpness decreases the brightness between the area of interest and its surrounding background. (Modified from Sprawls P: Physical Principles of Medical Imaging Online, ed 2, http://www.sprawls.org/ppmi2.)
Distortion
Distortion results from the radiographic misrepresentation of either the size (magnification) or the shape of the anatomic part. When an image is distorted, spatial resolution is also reduced.
Size Distortion (Magnification)
The term size distortion (or magnification) refers to an increase in the image size of an object compared with its true or actual size. Radiographic images of objects are always magnified in terms of the true object size. The source-to-image receptor distance (SID) and object-to-image receptor distance (OID) have a geometric relationship and play an important role in minimizing the amount of size distortion of the radiographic image.
Because radiographers produce radiographs of three-dimensional objects, some size distortion always occurs as a result of OID. The parts of the object that are farther away from the IR are radiographically represented with greater size distortion than the parts of the object that are closer to the IR. Even if the object is in close contact with the IR, some part of the object is farther away than other parts of the object. SID also influences the total amount of magnification of the image. As SID increases, size distortion (magnification) decreases; as SID decreases, size distortion (magnification) increases.
Shape Distortion
In addition to size distortion, objects that are being imaged can be radiographically misrepresented by distortion of their shape. Shape distortion can radiographically appear in two different ways: elongation or foreshortening. Elongation refers to images of objects that appear longer than the true objects. Foreshortening refers to images that appear shorter than the true objects. Examples of elongation and foreshortening can be seen in Fig. 3-26.
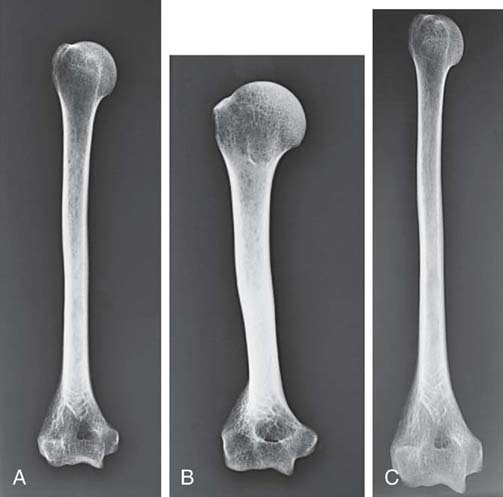
FIG. 3-26 A, No distortion. B, Foreshortened. C, Elongated. (From Mosby's Instructional Radiographic Series: Radiographic Imaging, St. Louis, 1998, Mosby.)
Shape distortion can arise from inaccurate central ray (CR) alignment of the tube, the part being radiographed, or the IR. Any misalignment of the CR among these three factors—tube, part, or IR—alters the shape of the part recorded in the image.
Sometimes shape distortion is advantageous in particular projections or positions. For example, CR angulation is sometimes required to elongate a part so that a particular anatomic structure can be visualized better. Also, rotating the part (and therefore creating shape distortion) is sometimes required to eliminate superimposition of objects that normally obstruct visualization of the area of interest. In general, shape distortion is not a necessary or desirable characteristic of radiographic images.
Both SID and OID determine the amount of magnification of the anatomic structures on the image. In addition, improper alignment of the CR, anatomic part, IR, or a combination of these components distorts the shape of the image.
Scatter
Scatter radiation, as previously described, can add unwanted exposure to the radiographic image as a result of Compton interactions. Unwanted exposure or fog on the image does not provide information about the anatomic area of interest. Scatter degrades or decreases the visibility of the anatomic structures. The scatter or unwanted exposure displayed in the image has the effect of decreasing the contrast by masking the desired brightness of the image and changing the degree of difference (Fig. 3-27).

FIG. 3-27 Scatter and fog.
Fog produced because of scatter reaching the IR can be visualized on a digital image. Even though the computer can change the contrast or gray levels displayed in a digital image, scatter radiation reaching the IR does not provide any information about the area of interest. Because digital IRs can detect low levels of radiation intensity, they are more sensitive to scatter radiation.
Quantum Noise
Image noise contributes no useful diagnostic information and serves only to detract from the quality of an image. Quantum noise (mottle) is a concern in digital imaging and is photon dependent. Quantum noise is visible as brightness fluctuations in the image. The fewer the photons reaching the IR to form the image, the greater the visibility of quantum noise on the digital image.
As previously mentioned, the digital computer system can adjust for low or high x-ray exposures during image acquisition. When the x-ray exposure to the IR is too low (i.e., when there is a decreased number of photons), computer processing alters the appearance of the digital image to make the brightness acceptable, but the image displays increased quantum noise (Fig. 3-28). Certain postprocessing options may render quantum noise more or less noticeable.
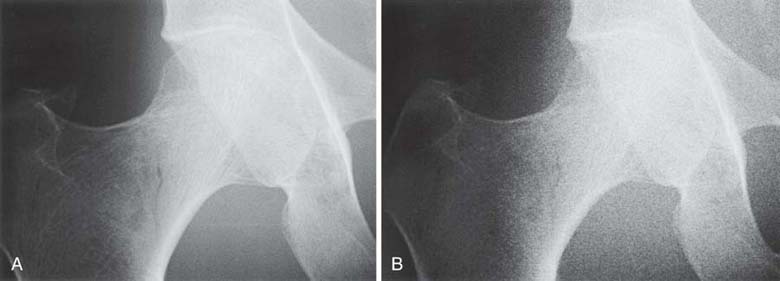
FIG. 3-28 A, Image created using an appropriate x-ray exposure technique. B, Image shows increased quantum noise as a result of insufficient x-ray exposure to the image receptor. (From Johnston JN, Fauber TL: Essentials of Radiographic Physics and Imaging, ed 2, St. Louis, 2016, Mosby.)
The exposure technique should be selected on the basis of the requirements of the type of radiographic procedure being performed. Although the computer can adjust for both low- and high-exposure technique errors, the radiographer is still responsible for selecting exposure techniques that produce diagnostic quality images while avoiding unnecessary exposure to the patient. Exposures that are too low adversely affect the quantum noise of an image even though the computer can adjust the brightness. Exposures that are too high result in excessive radiation exposure to the patient.
Image Artifacts
An artifact is any unwanted brightness level on a radiographic image. Artifacts are detrimental to images because they can impede visibility of anatomy, pathologic conditions, or patient-identification information. They decrease the overall quality of the radiographic image.
Errors such as double-exposing an IR or the improper use of equipment can result in image artifacts and must be avoided. Foreign bodies are a class of artifacts imaged within a patient's body. Variation in exposure techniques may be necessary when imaging for a suspected foreign body.
Artifacts from patient clothing and items imaged that are not a part of the area of interest are the same regardless of the type of imaging systems. The radiographer must be diligent in removing clothing or items that could obstruct visibility of the anatomic area of interest (Fig. 3-29). Scatter radiation or fog and image noise have also been classified as radiographic artifacts because they add unwanted information on the displayed image.

FIG. 3-29 Image artifact. (From Long B, Rollins J, Smith B: Merrill's Atlas of Radiographic Positioning and Procedures, ed 13, St. Louis, 2016, Mosby.)
Digital image artifacts can be a result of errors during extraction of the latent image from the IR, inadequate CR imaging plate erasure, or performance of the electronic detectors and will be discussed in subsequent chapters.
Digital versus Film-Screen Imaging
Although film-screen imaging served as a good medium for radiographic imaging for many decades, it has many limitations that can be overcome with digital imaging. One major deficiency is the limited dynamic range (the range of exposure intensities an IR can accurately detect). This limitation renders a film-screen IR very sensitive to underexposure or overexposure, which may necessitate image retakes. A limited dynamic range also restricts the visibility of structures that differ greatly in x-ray attenuation. An example is the difficulty of optimally visualizing both soft tissue and bony structures within a given film image.
Other drawbacks of film-screen imaging involve the cost of film itself, the necessity of developing the latent image into a manifest image via chemical processing, and potential artifacts related to film handling and chemical processing. The time required to process the film before viewing the radiograph can delay the progress of an examination or diagnosis. Automatic film processors incur considerable equipment and maintenance costs and demand frequent quality-control procedures.
Another restriction associated with a film image is that after the film has been processed, the image is permanent, and further adjustments cannot be made. There is no option to alter the brightness (for film, density, the amount of blackness after processing) or contrast of the manifest image. Therefore, the anatomic area that is to be optimally imaged must be selected at the time of exposure. For example, when an image is taken in the thoracic region, the exposure technique must be selected depending on whether the area of interest is the lungs or the ribs. A related issue is the limited contrast resolution, which is the ability to distinguish tissues of similar subject contrast, of film-screen receptors. Even if technique factors are chosen to optimize soft tissue contrast, the differential absorption among various soft tissues is slight and not well differentiated using film-screen imaging.
In addition, film images cannot be electronically stored or duplicated, displayed on computer monitors, or transmitted over computer networks unless they are digitized after processing. Traditional film archives consume significant space and are frequently prone to loss of films. In addition, personnel costs associated with maintaining the archive and the expense of storing radiographs and then retrieving them when needed for comparison is prohibitive. Film-screen imaging is discussed more thoroughly in Chapter 9.
Digital imaging overcomes many limitations of film-screen radiography. Digital radiographic images can be quickly acquired and displayed and can be efficiently transmitted, processed, interpreted on a display monitor, stored, and retrieved via electronic means.
Radiography creates a static (stationary) image of the anatomic area of interest whereas dynamic imaging, or fluoroscopy, provides imaging of the movement of internal structures.
DYNAMIC IMAGING: FLUOROSCOPY
Fluoroscopy (Fig. 3-30) differs from static imaging by its use of a continuous beam of x-rays to create images of moving internal anatomic structures that can be viewed on a display monitor. Internal structures, such as the vascular or gastrointestinal systems, can be visualized in their normal state of motion with the aid of special liquid or gas substances (contrast media) that are either injected or instilled (i.e., ingested). The equipment used in fluoroscopy has undergone major changes over the past few years. Image-intensified fluoroscopy is rapidly being replaced with flat-panel detector fluoroscopy. Regardless of the type of fluoroscopic equipment, the x-ray tube is usually positioned underneath the table, and the x-rays pass through the patient to interact with a device that converts the x-rays into either light intensities (image-intensified) or digital data (flat-panel detector).

FIG. 3-30 Digital fluoroscopy using flat-panel detector technology. (Courtesy of Siemens Healthcare, Malvern, PA.)
Fluoroscopy is discussed in detail in Chapter 10.
Regardless of the type of imaging system (digital, film, or fluoroscopic), the process of differential absorption for image formation remains the same. The varying x-ray intensities exiting the anatomic area of interest form the image.
CHAPTER SUMMARY
- • A radiographic image is a result of the differential absorption of the primary x-rays that interact with tissues of varying composition within the anatomic area of interest.
- • Beam attenuation occurs when the primary x-ray beam loses energy as it interacts with anatomic tissues.
- • X-rays have the ability to eject electrons (ionization) from atoms within anatomic tissue.
- • Three primary processes occur during x-ray interaction with anatomic tissues: absorption, transmission, and scattering.
- • Total absorption of the incoming x-ray photon is a result of the photoelectric effect.
- • Scattering of the incoming x-ray photon is a result of the Compton effect.
- • Scatter radiation reaching the IR provides no useful information and creates unwanted exposure or fog on the radiographic image.
- • The process of differential absorption remains the same for image formation regardless of the type of IR.
- • A radiographic image is composed of varying brightness levels that structurally represent the anatomic area of interest.
- • The visibility and accuracy of the recorded anatomic structural lines determine thwe overall quality of the radiographic image.
- • Visibility of the anatomic structures is achieved by the proper balance of image brightness and contrast.
- • Image contrast provides the ability to distinguish among the types of irradiated tissues.
- • Grayscale is the number of different shades of gray that can be stored and displayed in a digital image.
- • Spatial resolution refers to the accuracy of the anatomic structural lines displayed.
- • Distortion describes the magnification or misrepresentation in shape of the anatomic structures.
- • Scatter radiation produces unwanted exposure on the image, known as fog.
- • Quantum noise is a result of too few photons reaching the IR and is a concern in digital imaging.
- • An artifact is any unwanted brightness level on a radiographic image.
- • Digital IRs have a wider dynamic range compared with film-screen IRs.
- • Fluoroscopy differs from static imaging by its use of a continuous beam of x-rays to create images of moving internal structures (dynamic imaging) that can be viewed on a display monitor.
REVIEW QUESTIONS
1. The process whereby a radiographic image is created by variations in absorption and transmission of the exiting x-ray beam is known as ________________.
A. attenuation
B. the photoelectric effect
C. the Compton effect
D. differential absorption
2. Which of the following processes occur during the x-ray beam interaction with tissue?
1. Absorption
2. Photon transmission
3. Scattering
A. 1 and 2 only
B. 1 and 3 only
C. 2 and 3 only
D. 1, 2, and 3
3. The ability of an x-ray photon to remove an atom's electron is a characteristic known as ________________.
A. attenuation
B. scattering
C. ionization
D. absorption
4. The x-ray interaction responsible for absorption is ________________.
A. differential
B. photoelectric
C. attenuation
D. Compton
5. The x-ray interaction responsible for scattering is ________________.
A. differential
B. photoelectric
C. attenuation
D. Compton
6. Remnant radiation is composed of which of the following?
1. Transmitted radiation
2. Absorbed radiation
3. Scattered radiation
A. 1 and 2 only
B. 1 and 3 only
C. 2 and 3 only
D. 1, 2, and 3
7. What interaction causes unwanted exposure to the image, known as fog?
A. Compton
B. Transmitted
C. Photoelectric
D. Absorption
8. Which of the following factors would affect beam attenuation?
1. Tissue atomic number
2. Beam quality
3. Fog
A. 1 and 2 only
B. 1 and 3 only
C. 2 and 3 only
D. 1, 2, and 3
9. The high brightness areas on a radiographic image are created by ________________.
A. transmitted radiation
B. scattered radiation
C. absorbed radiation
D. primary radiation
10. An anatomic part that transmits the incoming x-ray photon would create an area of ________________ on the radiographic image.
A. fog
B. high brightness
C. low brightness
D. noise
11. The process of creating a radiographic image by differential absorption varies for film-screen and digital imaging.
A. True
B. False
12. Which attribute(s) of a radiographic image affect(s) the visibility of sharpness?
A. Distortion
B. Contrast
C. Brightness
D. B and C
13. A radiographic image with many shades of gray but few differences among them is said to have ________________.
A. high contrast
B. low contrast
C. saturation
D. excessive noise
14. Which of the following is defined as the range of exposure intensities that an image receptor can accurately detect?
A. Saturation
B. Spatial resolution
C. Quantum noise
D. Dynamic range
15. Fluoroscopy uses a continuous beam of x-rays to create images of moving internal anatomic structures.
A. True
B. False