Chapter 61 Emergency Medical Services for Children
The overwhelming majority of the 30 million children who present annually for emergency care in the USA are seen at community hospital emergency departments (EDs). Visits to children’s hospital EDs account for just 11% of initial emergency care encounters. This distribution suggests that the greatest opportunity to optimize care for acutely ill or injured pediatric patients, on a population basis, occurs broadly as part of a systems-based approach to emergency services, an approach that incorporates the unique needs of children at every level. Conceptually, emergency medical services for children (EMSC) are characterized by an integrated, continuum of care model (see Fig. 61-1 on the Nelson Textbook of Pediatrics website at  www.expertconsult.com). The model is designed such that patient care flows seamlessly from the primary care medical home through transport and on to hospital-based definitive care. It includes the following 5 principal domains of activity:
www.expertconsult.com). The model is designed such that patient care flows seamlessly from the primary care medical home through transport and on to hospital-based definitive care. It includes the following 5 principal domains of activity:

Figure 61-1 The emergency medical services for children (EMSC) continuum of care: Seriously ill and injured children interface with a large number of health care personnel as they move through the EMSC system.
The federal EMSC program of the Health Resources and Services Administration’s Maternal and Child Health Bureau has stewarded improvements in the care of children in the context of the continuum of care model. The programmatic mission of the EMSC program is as follows:
EMSC funding to states and U.S. territories has created a national framework upon which necessary advances in education, advocacy, and research are taking place. EMSC grantees, constituents, and stakeholders as well as professional organizations such as the American Academy of Pediatrics are collaboratively engaged in implementation activities and projects that address the pediatric-specific recommendations stemming from the comprehensive 2006 Institute of Medicine (IOM) report The Future of Emergency Care in the United States Health System.
The Primary Care Physician and Office Preparedness
The primary care physician (PCP) has multiple important roles in EMSC. Through anticipatory guidance, the PCP can help shape the attitudes, knowledge, and behaviors of parent and child, with the primary goal of preventing acute medical events, such as injury and status asthmaticus. The point of care initiation for many acute problems is often the PCP office. From the standpoint of personnel, equipment, training, and protocols, the PCP office setting must be adequately prepared to initially manage acute and emergency exacerbations of common pediatric conditions, such as respiratory distress and seizures. Further, on rare occasion, the PCP office environment may be confronted with a child in clinical extremis and requiring resuscitative intervention and stabilization. It is, therefore, incumbent upon the PCP not only to ensure access to emergency medical services (EMS), that is, 911 system activation, but also to ensure that there is adequate, on-site psychomotor skill preparation to deal with such an emergency. Office preparedness requires training and continuing education for staff members, protocols for emergency intervention, ready availability of appropriate resuscitation drugs and equipment, and knowledge of local EMS resources and ED capabilities.
Staff Training and Continuing Education
It is a reasonable expectation that all office staff, including receptionists and medical assistants, be trained in cardiopulmonary resuscitation (CPR) and that their certification be maintained on an annual basis. Nurses and physicians should also have training in a systematic approach to pediatric resuscitation. Core knowledge may be obtained through standardized courses in advanced life support (ALS) offered by national medical associations and professional organizations. Frequent recertification is important for knowledge retention and skill maintenance. Examples are the Pediatric Advanced Life Support (PALS) and Pediatric Emergency Assessment, Recognition and Stabilization (PEARS) courses sponsored by the American Heart Association, the Advanced Pediatric Life Support (APLS) course sponsored by the American Academy of Pediatrics (AAP) and the American College of Emergency Physicians (ACEP), and the Emergency Nurses Pediatric Course (ENPC) sponsored by the Emergency Nurses Association (ENA).
Protocols
Standardized protocols for telephone triage of seriously ill or injured children are essential. When a child’s status is in question and prehospital care is available, ambulance transport in the care of trained personnel is always preferable to transport by privately owned vehicle (POV). This obviates the potentially serious medical consequences of relying on unskilled and distraught parents without the ability to provide even basic life support (BLS) measures to an unstable child during transport to an ED. Practitioners can work with their local pediatric emergency care resource center (e.g., children’s hospital or academic department of pediatrics) to develop and maintain written protocols for office-based management of a range of conditions, including anaphylaxis, cardiopulmonary arrest, head trauma, ingestions, shock, status asthmaticus, status epilepticus, and upper airway obstruction. Regular practice using mock code scenarios has been shown to improve office-based practitioner confidence and self-efficacy in managing these problems.
Resuscitation Equipment
Availability of necessary equipment is a vital part of an emergency response. Every physician’s office should have essential resuscitation equipment and medications packaged in a pediatric resuscitation cart or kit (Table 61-1). This cart or kit should be checked on a regular basis and kept in an accessible location known to all office staff. Outdated medications, a laryngoscope with a failed light source, or an empty oxygen tank represents a potential catastrophe in a resuscitation setting. Such an incident can be easily avoided if an equipment checklist and maintenance schedule are implemented. A pediatric kit that includes posters, laminated cards, or a color-coded length-based resuscitation tape specifying emergency drug doses and equipment size is invaluable in avoiding critical therapeutic errors during resuscitation.
Table 61-1 RECOMMENDED DRUGS AND EQUIPMENT FOR PEDIATRIC OFFICE EMERGENCIES
| PRIORITY | |
|---|---|
| DRUGS | |
| Oxygen | E |
| Albuterol for inhalation | E |
| Epinephrine (1 : 1,000) | E |
| Activated charcoal | S |
| Antibiotics | S |
| Anticonvulsants (diazepam/lorazepam) | S |
| Corticosteroids (parenteral/oral) | S |
| Dextrose (25%) | S |
| Diphenhydramine (parenteral, 50 mg/mL) | S |
| Epinephrine (1 : 10,000) | S |
| Atropine sulfate (0.1 mg/mL) | S |
| Naloxone (0.4 mg/mL) | S |
| Sodium bicarbonate (4.2%) | S |
| INTRAVENOUS FLUIDS | |
| Normal saline (NS) or lactated Ringer solution (500-mL bags) | S |
| 5% dextrose, 0.45 NS (500-mL bags) | S |
| Equipment for Airway Management | |
| Oxygen and delivery system | E |
| Bag-valve-mask (450-mL and 1,000-mL) | E |
| Clear oxygen masks, breather and non-rebreather, with reservoirs (infant, child, adult) | E |
| Suction device, tonsil tip, bulb syringe | E |
| Nebulizer (or metered-dose inhaler with spacer/mask) | E |
| Oropharyngeal airways (sizes 00-5) | E |
| Pulse oximeter | E |
| Nasopharyngeal airways (sizes 12-30F) | S |
| Magill forceps (pediatric, adult) | S |
| Suction catheters (sizes 5-14F) | S |
| Nasogastric tubes (sizes 6-14F) | S |
| Laryngoscope handle (pediatric, adult) with extra batteries, bulbs | S |
| Laryngoscope blades (straight 0-4; curved 2-3) | S |
| Endotracheal tubes (uncuffed 2.5-5.5; cuffed 6.0-8.0) | S |
| Stylets (pediatric, adult) | S |
| Esophageal intubation detector or end-tidal carbon dioxide detector | S |
| EQUIPMENT FOR VASCULAR ACCESS AND FLUID MANAGEMENT | |
| Butterfly needles (19-25 gauge) | S |
| Catheter-over-needle device (14-24 gauge) | S |
| Arm boards, tape, tourniquet | S |
| Intraosseous needles (16-, 18-gauge) | S |
| Intravenous tubing, micro-drip | S |
| MISCELLANEOUS EQUIPMENT AND SUPPLIES | |
| Color-coded tape or preprinted drug doses | E |
| Cardiac arrest board/backboard | E |
| Sphygmomanometer (infant, child, adult, thigh cuffs) | E |
| Splints, sterile dressings | E |
| Automated external defibrillator with pediatric capabilities | S |
| Spot glucose test | S |
| Stiff neck collars (small/large) | S |
| Heating source (overhead warmer/infrared lamp) | S |
E, essential; S, strongly suggested.
Adapted from American Academy of Pediatrics, Committee on Pediatric Emergency Medicine; Frush K: Preparation for emergencies in the offices of pediatricians and pediatric primary care providers, Pediatrics 120:200–212, 2007.
To facilitate emergency response when a child needs rapid intervention in the office, all personnel should have designated roles. Organizing a “code team” within the office ensures that necessary equipment is made available to the physician in charge, that an appropriate medical record detailing all interventions and the child’s response is generated, and that the 911 call for EMS response or a transport team is made in a timely fashion.
Transport
Once the child has been stabilized, a decision must be made on how to transport a child to a facility capable of providing definitive care. If a child has required airway or cardiovascular support, has altered mental status or unstable vital signs, or has significant potential to deteriorate en route, it is not appropriate to send the child via POV, regardless of proximity to a hospital. Even when an ambulance is called, it is the PCP’s responsibility to initiate essential life support measures and to attempt to stabilize the child before transport.
In metropolitan centers with numerous public and private ambulance agencies, the PCP must be knowledgeable about the level of service that is provided by each. The availability of BLS vs ALS services, the configuration of the transport team, and pediatric expertise vary markedly among agencies and across jurisdictions. BLS services provide basic support of airway, breathing, and circulation, whereas ALS units are capable of providing resuscitation drugs and procedural interventions as well. Some communities may have only BLS services available, whereas others may have a 2-tiered system, providing both BLS and ALS. It may be appropriate to consider medical air transport when definitive or specialized care is not available within an immediate community or when ground transport times are prolonged. In that case, initial transport via ground to an appropriate helicopter landing zone or a local hospital for interval stabilization may be undertaken, pending arrival of the air transport team. Independent of whether a child is to be transported by air or ground, copies of the pertinent medical records and any radiologic studies or laboratory results should be sent with the patient, and a call made to the physicians at the receiving facility to alert them to the referral and any treatments administered. Such notification is not merely a courtesy; direct physician-to-physician communication is essential to ensure adequate transmission of patient care information, to allow mobilization of necessary resources in the ED, and to redirect the transport if the emergency physician believes that the child would be better treated at a facility with specialized services.
Pediatric Prehospital Care
Prehospital care refers to emergency assistance rendered by trained emergency medical personnel before a child reaches a treating medical facility. The goals of prehospital care are to further minimize systemic insult or injury through a series of well-defined and appropriate interventions and to embrace principles that ensure patient safety. Most communities in the USA have a formalized EMS system; the organizational structure and nature of emergency medical response depend greatly on local demographics and population base. EMS may be provided by volunteers or career professionals working in a fire-based or independent “third service” response system. Key points to recognize in negotiation of the juncture between the community physician and the local EMS system include access to the system, provider capability, and destination determination.
Access to the EMS System
Virtually all Americans have access to the 911 telephone service that provides direct access to a dispatcher who coordinates police, fire, and EMS responses. Some communities have an enhanced 911 system, in which the location of the caller is automatically provided to the dispatcher, permitting emergency response even if the caller, such as a young child, cannot give an address. The extent of medical training for these dispatchers varies among communities, as do the protocols by which they assign an emergency response level (BLS vs ALS). In some smaller communities, no coordinated dispatch exists, and emergency medical calls are handled by the local law enforcement agency.
When activating the 911 system, the physician must make clear to the dispatcher the nature of the medical emergency and the condition of the child. In many communities, emergency medical dispatchers are trained to ask a series of questions per protocol that determines the appropriate level of provider to be sent.
Provider Capability
There are many levels of training for prehospital EMS providers, ranging from individuals capable of providing only first aid to those trained and licensed to provide ALS. All EMS personnel, whether basic emergency medical technicians (EMTs) or paramedics, receive training in pediatric emergencies; however, pediatric cases actually constitute roughly 10% of all EMS transports.
First responders may be law enforcement officers or firefighters, who are dispatched to provide emergency medical assistance, or bystanders. Public safety personnel have a minimum of 40 hours of training in first aid and CPR. Their role is to provide rapid response and stabilization pending the arrival of more highly trained personnel. In some smaller communities, this may be the only prehospital emergency medical response available.
In the USA, the bulk of emergency medical response is provided by EMTs, who may be volunteers or paid professionals. Basic EMTs may staff an ambulance after undergoing a training program of approximately 100 hours. They are licensed to provide BLS services but may receive further training in some jurisdictions to expand their scope of practice to include intravenous catheter placement and fluid administration, management of airway adjuncts, and the use of an automated external defibrillator.
Paramedics, or EMT-Ps, represent the highest level of EMT response, with medical training and supervised field experience of approximately 1,000 hours. Paramedic skills include advanced airway management, including endotracheal intubation; placement of peripheral, central, or intraosseous lines; intravenous administration of drugs; administration of nebulized aerosols; needle thoracostomy; and cardioversion and defibrillation. These professionals provide ALS services, functioning out of an ambulance equipped as a mobile intensive care unit. In a consensus policy statement entitled Equipment for Ambulances, the American College of Surgeons Committee on Trauma, the ACEP, the National Association of EMS Physicians, the Pediatric Equipment Guidelines Committee of the EMSC Partnership Stakeholder Group, and the AAP have published guideline standards for essential ambulance equipment, medications, and supplies necessary to provide BLS and ALS care across the age spectrum. This essential equipment list represents one of the reference standards that the federal EMSC program has adopted as a performance measure for state-level operational readiness to care for children in an EMS system.
Both basic EMTs and paramedics function under the delegated licensing authority of a supervisory EMS medical director. This physician oversight of prehospital practice is broadly characterized under the umbrella term medical control. Direct, or on-line, medical control refers to medical direction either at the scene or in real time via voice or video transmission. Indirect, or off-line, medical control refers to the administering of medical direction prior to and after the provision of care. Off-line activities such as provider education and training, protocol development, and medical leadership of quality assurance/quality improvement programs represent areas in need of greater pediatric input. As a measure of the degree to which EMSC permanence is being established in state EMS systems, the federal EMSC program has required demonstration of participation in on-line and off-line medical direction activities for pediatric patients and the seating of an EMSC advisory committee at the state level. These advisory bodies are well positioned to support EMS agencies in their pediatric readiness as well as provide a forum for the active engagement of pediatric care experts at a system level.
Destination Determination
The destination to which a pediatric patient is transported may be defined by parental preference, provider preference, or jurisdictional protocol, which is typically predicated on field assessment of anatomic and physiologic criteria and, in the case of trauma, mechanism of injury. In communities served by an organized trauma or regionalized EMS system that incorporates pediatric designation based on objectively verified hospital capabilities, seriously ill or injured children may be triaged by protocol to the highest-level center reachable within a reasonable amount of time. The mantra is to deliver the child to the “right care in the right time,” even if it requires bypassing closer hospitals. An exception is the child in full arrest, for whom expeditious transport to the nearest facility is always warranted. Regionalization in the context of EMS is defined as a geographically organized system of services that ensures access to care at a level appropriate to patient needs while maintaining efficient use of available resources. This system concept is especially germane in the care of children, given the relative scarcity of facilities capable of managing the full range and scope of pediatric conditions (Fig. 61-2). Regionalized systems of care coordinated with emergency medical dispatch, field triage, and EMS transport have demonstrated efficacy in improving outcomes for pediatric trauma patients, especially for younger children and children with isolated head injury. Emerging evidence also suggests a similar benefit conferred to children in shock identified in the field who are preferentially transported to hospital EDs with documented pediatric ALS capability. The existence of statewide or regional standardized systems that formally recognize hospitals able to stabilize and/or manage pediatric medical emergencies is another federal EMSC performance measure against which operational capacity to provide optimal pediatric emergency care in this country is currently being judged.
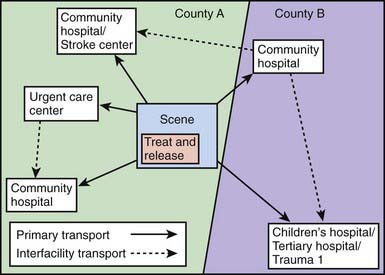
Figure 61-2 Transport options within a coordinated, regionalized emergency medical services system model. The objective is to ensure access to definitive care at a level appropriate to meet patient needs. Solid arrows, primary transport; dotted arrows, interfacility transport.
(Adapted from Institute of Medicine, Committee on the Future of Emergency Care in the US Health System: Hospital-based emergency care: at the breaking point, Washington, DC, 2006, National Academies Press.)
In communities that do not have a hospital with the equipment and personnel resources to provide definitive pediatric inpatient care, interfacility transport of a child to a regional center should be undertaken after initial stabilization (Chapter 61.1). When interfacility transport is to be undertaken, indications for transfer, parental consent for transfer, and acceptance of the patient by the receiving physician must all be clearly documented in the medical record.
The Emergency Department
The ability of hospital EDs to respond to the emergency care of children varies and depends on a number of factors in addition to availability of equipment and supplies. Training, awareness, and experience of the staff as well as access to pediatricians and medical and surgical subspecialists also play a key role. The majority of children who require emergency care are evaluated in community hospitals by physicians, nurses, and other health care providers with variable degrees of pediatric training and experience. Although children account for 25-30% of all ED visits, only a fraction of these encounters represent true emergencies. Because the volume of critical pediatric cases is low, emergency physicians and nurses working in community hospitals often have limited opportunity to reinforce their knowledge and skills in the assessment of ill or injured children and in pediatric resuscitation. General pediatricians from the community may be consulted when a seriously ill or injured child presents to the ED, and they should have a structured approach to the initial evaluation and treatment of an unstable child of any age, regardless of the underlying diagnosis. Early recognition of life-threatening abnormalities in oxygenation, ventilation, perfusion, and central nervous system function and rapid intervention to correct those abnormalities are key to successful resuscitation and stabilization of the pediatric patient.
In its 2006 report The Future of Emergency Care in the U.S. Health System, the IOM strongly recommended that hospitals and EMS systems appoint qualified coordinators for pediatric emergency care, a recommendation consistent with pediatric emergency readiness guidelines advocated by the AAP and ACEP. Only 18% of EDs in the USA currently appoint a physician coordinator, and 12% appoint a nursing coordinator for pediatric emergency care. EDs that do appoint these positions tend to be more prepared as measured by compliance with nationally published guidelines on the care of children in the ED.
Minimum standards must be met by community EDs to ensure that children receive the best emergency care possible. Updated guidelines for the care of children in the ED have been published and are endorsed by the AAP, the ACEP, and the ENA. These guidelines provide current information on policies, procedures, protocols, quality assurance methods, and equipment and supplies considered essential for managing pediatric emergencies. Specific recommendations on equipment, supplies, and medications for the ED are listed and updates are available on the AAP website. Sample policies, procedures, and protocols specifically addressing the needs of children in the ED are listed in Table 61-2.
Table 61-2 GUIDELINES FOR PEDIATRIC-SPECIFIC POLICIES, PROCEDURES, AND PROTOCOLS FOR THE EMERGENCY DEPARTMENT
Illness and injury triage
Pediatric patient assessment and reassessment
Documentation of pediatric vital signs, abnormal vital signs, and actions to be taken for abnormal vital signs
Immunization assessment and management of the underimmunized patient
Sedation and analgesia for procedures, including medical imaging
Consent (including situations in which a parent is not immediately available)
Social and mental health issues
Physical or chemical restraint of patients
Child maltreatment (physical and sexual abuse, sexual assault, and neglect) mandated reporting criteria, requirements, and processes
Death of the child in the emergency department
Do-not-resuscitate orders
Communication with patient’s medical home or primary health care provider
Medical imaging policies that address age- or weight-appropriate dosing for children receiving studies that impart ionizing radiation, consistent with ALARA (as low as reasonably achievable) principles
Adapted from American Academy of Pediatrics Committee on Pediatric Emergency Medicine; American College of Emergency Physicians Pediatric Committee; Emergency Nurses Association Pediatric Committee: Joint policy statement—guidelines for care of children in the emergency department, Pediatrics 124:1233–1243, 2009.
The way in which the family supports the child during a crisis and, consequently, how the family is supported in the ED when caring for the child are critical to patient recovery, family satisfaction, and the mitigation of post-traumatic stress. Commitment to patient and family–centered care in the ED ensures that the patient and family experience guides the practice of culturally sensitive care and promotes patient dignity, comfort, and autonomy. In the ED setting, particular issues such as family presence deserve specific attention. Surveys of parents have indicated that most want to be with their child during invasive procedures and even during resuscitation. Allowing their presence has been shown to reduce parental and patient anxiety and does not interfere with procedure performance. Patient and family–centered care is also associated with improved care quality and patient safety.
Emerging Issues in EMSC
Of the pediatric-specific recommendations promulgated by the IOM in its widely publicized 2006 report on the future of emergency care, 3 have emerged as especially important moving forward for EMSC. The first has to do directly with increased federal funding for the EMSC program, which supports more than 70 grantees with an established presence in all 50 states, 5 U.S. territories, and the District of Columbia. The grant awards cover 4 distinct categories ranging from basic science and clinical investigation to public sector capacity-building programs to national technical assistance centers to multicenter trials conducted within a large research network. Through the diversity of activity generated within the program, and in collaboration with stakeholders, the EMSC program affords synergistic opportunity to further the progress realized in the program’s first 25 years. Congressional reauthorization in 2009 of the EMSC authorizing legislation, the Wakefield Act, ensures program stability in the near term.
In addition to EMSC resource support, the IOM also recommended that (1) federal agencies in partnership with state and regional planning bodies and emergency care provider organizations convene a panel with multidisciplinary expertise to develop strategies for addressing pediatric needs in the event of a disaster and (2) the U.S. Department of Health and Human Services conduct a study to examine the gaps and opportunities in emergency care research, including pediatric emergency care, and recommend a strategy for the optimal organization and funding of the research effort. Both of these recommendations have generated activity of significant import to the emergency care community, EMSC specifically, and warrant mention.
Disaster Preparedness
Children constitute about 30% of the population; in a catastrophic event, natural or man-made, several unique factors place children at disproportionate, increased risk. During the day large groups of children are typically cohorted, separate from their families, in schools and daycare centers where mass casualties can easily occur and reunification is challenging. Further, in the event of a biologic or chemical attack, unique anatomic, developmental, and physiologic features make children especially vulnerable to absorption and/or inhalation of toxic agents. In the days and weeks following the 2005 Gulf Coast hurricanes Katrina and Rita, pediatricians in Houston taught us lessons in the rendering of care to large numbers of acutely displaced families in the Astrodome, a reminder that when the need arises, EMSC knows no bounds. In 2008, Congress established the National Commission on Children and Disasters with a mandate to conduct a comprehensive study to examine and assess the needs of children as they relate to preparation for, response to, and recovery from all hazards, including major disasters and emergencies. The Commission’s report to the President and to Congress is due in late 2010.
Research
Building the evidence base for pediatric emergency care and EMSC is especially challenging, given the relative infrequency of critical conditions of research interest and need, and the rare occurrence of adverse outcomes. No single medical center or EMS agency is able to generate sufficient sample size to conduct scientifically rigorous controlled studies, let alone randomized trials, of emergency pediatric problems. In 2001, the Health Resources and Services Administration announced a competitive research funding opportunity, entitled the EMSC Network Development Demonstration Project (NDDP). The NDDP funding stream has supported a now mature national research network known as the Pediatric Emergency Care Applied Research Network (PECARN), which accounts for more than 800,000 ED visits of children distributed among nearly two dozen sites around the country. The PECARN is exploring some of the most vexing questions in pediatric emergency care and challenging practice dogma by leveraging the strength of its number of potential subject enrollees in randomized, controlled trials. According to the specific IOM recommendation, the National Resource Center (NRC) of the EMSC program has generated a comprehensive Gap Analysis of EMS Related Research, which can be accessed electronically from the EMSC NRC website, www.childrensnational.org/EMSC.
Advocacy for EMSC
By definition the scope of EMSC has both breadth and depth. EMSC encompasses service delivery along a continuum that links distinct clinical settings, involves professionals from multiple disciplines, and cares for children from preterm infancy to young adulthood. EMSC also embraces the fundamental tenants of pediatric medicine, including an emphasis on prevention, attention to the phenomenon of growth and development, and the incorporation of the principles of patient and family–centered care at every encounter. Yet, in order to be effective and valued, programmatically, EMSC must focus on the generation of quantifiable indicators and performance against benchmarked, population-based measures. Accommodating such broad accountability involves attention to process, collaboration, and the need for advocacy. Advocacy in support of core EMSC issues can take on many forms; for example, legislative advocacy with elected officials for continued budgetary support of the federal program, regulatory advocacy with policy-makers on the role of EMSC in at state and local levels, community advocacy with end users such as children, families, and PCPs, and institutional advocacy to encourage hospitals to incorporate the elements that make a difference in the care of children.
American Academy of Pediatrics Committee on Emergency MedicineAmerican College of Emergency Physicians Pediatric CommitteeO’Malley PJ, Brown K, Krug SE. Patient and family-centered care and the role of the emergency physician providing care to a child in the emergency department. Ann Emerg Med. 2006;48:643-645.
American Academy of Pediatrics Committee on Pediatric Emergency MedicineAmerican College of Emergency Physicians Pediatric CommitteeEmergency Nurses Association Pediatric CommitteeGausche-Hill M, Krug SE. Joint policy statement—guidelines for care of children in the emergency department. Pediatrics. 2009;124:1233-1243.
American Academy of Pediatrics Committee on Pediatric Emergency MedicineFrush K, Krug SE. Patient safety in the pediatric emergency care setting. Pediatrics. 2007;120:1367-1375.
American Academy of PediatricsCommittee on Pediatric Emergency MedicineFrush K. Preparation for emergencies in the offices of pediatricians and pediatric primary care providers. Pediatrics. 2007;120:200-212.
American Academy of Pediatrics Section on OrthopaedicsAmerican Academy of Pediatrics Committee on Pediatric Emergency MedicineAmerican Academy of Pediatrics Section on Critical Care; American Academy of Pediatrics Section on SurgeryAmerican Academy of Pediatrics Section on Transport MedicineAmerican Academy of Pediatrics Committee on Pediatric Emergency MedicinePediatric Orthopaedic Society of North AmericaTuggle D, Krug SE. Management of pediatric trauma. Pediatrics. 2008;121:849-854.
American College of Surgeons Committee on Trauma, American College of Emergency Physicians, National Association of EMS Physicians, Pediatric Equipment Guidelines Committee—Emergency Medical Services for Children (EMSC) Partnership for Children Stakeholder Group, American Academy of Pediatrics. Equipment for ambulances. Pediatrics. 2009;124:e166-e171.
Ball JW, Liao E, Kavanaugh D, et al. The emergency medical services for children program: accomplishments and contributions. Clin Pediatr Emerg Med. 2006;7:6-14.
Burt CW, Middleton KR. Factors associated with ability to treat pediatric emergencies in US hospitals. Pediatr Emerg Care. 2007;23:681-689.
Carcillo J, Kuch B, Han Y, et al. Use of PALS/APLS by community physicians to reverse all-cause pediatric shock is associated with reduced mortality and functional morbidity: a multicenter cohort study. Pediatrics. 2009;124:500-508.
Cichon M, Lyons E, Fuchs S, et al. A statewide model program to improve emergency department readiness for pediatric care. Ann Emerg Med. 2009;54:198-204.
Committee on Pediatric Emergency MedicineKrug SE, Frush K. Patient safety in the pediatric emergency care setting. Pediatrics. 2007;120:1367-1375.
EMSC National Resource Center. EMSC performance measures: 2007 edition. Implementation manual for state partnership grantees. EMSC National Resource Center, Washington, DC, 2007. http://bolivia.hrsa.gov/emsc/PerformanceMeasures/PerformanceMeasuresComplete.htm. Accessed July 13, 2009
EMSC National Resource Center, Children’s National Medical Center. Gap analysis of EMS related research: report to the Federal Interagency Committee on EMS (website). www.childrensnational.org/emsc. Accessed March 17, 2010
Gausche-Hill M, Schmitz C, Lewis RJ. Pediatric preparedness of United States emergency departments: a 2003 survey. Pediatrics. 2007;120:1229-1237.
Institute of Medicine, Committee on the Future of Emergency Care in the US Health System. Emergency care for children: growing pains. Washington, DC: National Academies Press; 2006.
Institute of Medicine, Committee on the Future of Emergency Care in the US Health System. Emergency medical services: at the crossroads. Washington, DC: National Academies Press; 2006.
Institute of Medicine, Committee on the Future of Emergency Care in the US Health System. Hospital-based emergency care: at the breaking point. Washington, DC: National Academies Press; 2006.
Institute of Medicine, Committee on Pediatric Emergency Medical Services. Durch JS, Lohr KN, editors. Institute of Medicine report: emergency medical services for children. Washington, DC: National Academy Press, 1993.
Junkins E, O’Connell J, Mann N. Pediatric trauma systems in the United States: do they make a difference? Clin Pediatr Emerg Med. 2006;7:76-81.
National Commission on Children and Disasters: 2010 Report to the President and Congress, AHRQ Pub No 10-M037, Rockville, MD, October 2010, Agency for Healthcare Research and Quality. http://www.ahrq.gov/prep/nccdreport. Accessed November 16, 2010.
Sirbaugh PE, Gurwitch KD, Macias CG, et al. Caring for evacuated children housed in the Astrodome: creation and implementation of a mobile pediatric emergency response team: regionalized caring for displaced children after a disaster. Pediatrics. 2006;117:S428-S438.
Toback S, Fiedor M, Kilpela B, et al. Impact of a pediatric primary care office-based mock code program on physician and staff confidence to perform life-saving skills. Pediatr Emerg Care. 2006;22:415-422.
Wright J. Emergency medical services for children and the Institute of Medicine revisited, 1993–2006. Clin Pediatr Emerg Med. 2006;7:69-70.
61.1 Interfacility Transport of the Seriously Ill or Injured Pediatric Patient*
Patients often seek treatment at facilities that lack sufficient expertise to treat their conditions, necessitating transfer to more appropriate specialty centers. This is especially pronounced in pediatrics. EMS providers or parents usually take children to local EDs first, where their conditions and physiologic stabilities are assessed. Although bringing a child directly to the local ED may be proper logistically, local EDs can be less than ideal for pediatric emergencies. Children account for 27% of all ED visits but only 6% of EDs have all the necessary supplies for pediatric emergencies. Also, general EDs are less likely to have pediatric expertise or policies in place for the care of children. Outcomes for critically ill children treated in pediatric intensive care units (PICUs) are better than for those treated in adult ICUs. When pediatric critical care is required, transport to a regional PICU is indicated. In addition, often the type of subspecialty care needed (e.g., pediatric orthopedics) is available only at the pediatric center.
Pediatric transport medicine consists of the interfacility transfer of infants, children, and adolescents from community facilities to pediatric centers that can provide the needed level of expertise. Transport is performed by pediatric transport professionals on specially age-equipped ground, rotorcraft, or fixed-wing ambulances. Pediatric transport medicine is a multidisciplinary field comprising pediatric critical care and pediatric emergency medicine physicians (and, sometimes for very young infants, neonatologists); nurses, respiratory therapists, and paramedics with advanced training for pediatric transport; and communications specialists. The goal is to deliver quality pediatric care to the region’s children while optimizing the use of regional resources. For the individual child, the aim is to stabilize and, when appropriate, begin treating as soon as possible—that is, at the local ED and during transport, well before arrival at the referral center.
The AAP Section on Transport Medicine, the Association of Air Medical Services, the Federal Aviation Administration (FAA), and others have published recommendations regarding transport programs. Models for pediatric transport services vary depending on the needs and available resources in a geographic region, but all should have certain basic components: a network of community hospitals and regional pediatric centers; an established communications and dispatch system that easily facilitates transfer to the pediatric center; ground and/or air ambulances; medical and nursing leadership from pediatric critical care or pediatric emergency medicine (or neonatology); experienced pediatric medical control physicians (MCPs); a multidisciplinary team of pediatric transport professionals specially trained to provide the appropriate level of care required during transport; operational and clinical policies and procedures that guarantee safe, state-of-the-art, and timely pediatric critical care transport; and a database for quality and performance assessment.
Communications and Dispatch Center
Communications are one of the most vital components of a regional transport system. Treating a critically ill or injured child is an uncommon event for most community physicians. Therefore, they need to know whom, how, and when to call for assistance in the stabilization and transfer of a pediatric patient. The communications and dispatch center provides a single telephone number for such calls.
The communications and dispatch center coordinates communications among the outlying facility, receiving unit, medical control physician, transport team, and others. This center may be part of a hospital unit (e.g., ED, PICU), self-contained in a single institution (e.g., Emergency Communications and Information Center), or based off-site as a freestanding center coordinating communications and dispatch for multiple transport programs.
Staffing varies depending on the type of center. On-duty nurses or physicians may receive calls at unit-based models with low volumes. In contrast, dedicated communications specialists usually staff self-contained or freestanding centers, which tend to be busier. The communications specialist has numerous responsibilities, including answering the referring physician’s call promptly; documenting essential patient demographic information; arranging for immediate consultation with the medical control physician; dispatching the transport team to the referring facility expeditiously; updating the referring facility with any changes in the arrival time; and coordinating medical control and other necessary transport-related calls. The transport team must be equipped with a cellular telephone or radio for immediate contact with the receiving and referring facilities.
Medical Control Physician
The MCP is involved in the clinical care and safe transport of the patient from the time of referral through arrival at the receiving hospital unit. The MCP’s oversight increases once the transport team arrives at the referring facility. The MCP should have expertise in pediatric critical care or pediatric emergency medicine (or sometimes neonatology). Besides having the knowledge required to stabilize a critically ill or injured child, the MCP must be familiar with the transport environment; the transport team members’ capabilities; the program’s policies and procedures; and the region’s geography, medical resources, and regulations regarding interhospital transport. The MCP must possess good interpersonal and communication skills and must be able to maintain collegiality with the referring hospital’s staff during a potentially difficult and stressful situation.
Once a transport call is received, the MCP must be immediately available to confer with the referring physician. Although the MCP may have other responsibilities, these transport responsibilities take priority in order to avoid undue delays when transferring a critically ill child. Often the MCP recommends further testing or therapeutic interventions that can be delivered by the referring hospital before the transport team arrives. The MCP may seek additional guidance from other specialists, as necessary. Because the child’s condition may change rapidly, the MCP must remain ready to give additional advice. All conversations and recommendations regarding the care of the patient should be documented. Some centers record these conversations.
After discussion with the referring physician—and, when warranted, with the transport staff—the MCP determines the best team composition and vehicle for transport. The MCP usually does not accompany the team but remains available, by phone or radio, to supervise care.
It is worth noting that the MCP assumes significant responsibility for a patient whom the MCP has never personally evaluated. Telemedicine may obviate this shortcoming and may even change transport medicine as telecommunications systems evolve.
Transport Team
Transport team composition varies among programs—and sometimes within an individual program. The team’s composition is based on a variety of factors, including the severity of the child’s illness or injury; the distance to the referring facility; the team members’ advanced practice abilities; the referrer’s (reasonable or unreasonable) insistence that a physician be present; the program’s historical professional makeup; and the region’s staffing regulations. The team should be composed of physicians, nurses, respiratory therapists, and/or paramedics who have experience in pediatric critical care or pediatric emergency medicine (or neonatology in some cases) as well as advanced education and training in those cognitive and procedural areas important for pediatric critical care transport. There is a lower incidence of transport-related morbidity for critically ill and injured children transported by pediatric specialty teams than for those transported by generalist teams.
Various scoring systems have been developed to predict the need for a physician during transport. It seems that a team member’s training, experience, and skill in treating critically ill patients are more important considerations than that team member’s professional degree. Team members must understand basic pediatric pathophysiology and collectively must be able to assess and monitor a critically ill or injured child; manage the airway and provide respiratory support; obtain vascular access; and administer those medications commonly used in pediatric critical care transport. They must be familiar with the physiologic alterations as well as practical difficulties of the transport environment and, importantly, must be comfortable working in an out-of-hospital setting. Physicians are less often deployed on transport teams in part because of the advanced training that other health care professionals on the transport team receive.
The transport team should have a designated team leader who, in addition to the team leader’s many other responsibilities, interacts with the MCP during the transport. Once the team arrives at the referring facility, the team should reassess the child’s condition, review all of the pertinent diagnostic studies and therapies, and discuss the situation with the referring staff and parents. If the patient’s condition has changed significantly, the team leader may need to contact the MCP for additional advice. Otherwise, the team leader should notify the MCP before starting to bring the child to the receiving facility. Any care delivered by the team during transport should be documented, and copies of all medical records—including laboratory data, radiographs, and scans—should accompany the child to the pediatric center. The receiving unit must be updated prior to arrival so it can finalize preparations for the patient.
Ground versus Air Ambulance
Transport options include ground, rotorcraft, and fixed-wing ambulances. Vehicle selection depends on the child’s emergency needs; transport team’s capabilities; any out-of-ordinary staffing or equipment requirements (e.g., for extracorporeal membrane oxygenation, inhaled nitric oxide or helium); referring facility’s abilities; distance; terrain; traffic patterns; ground or air ambulance availability; helicopter landing pad or airport access; weather conditions; and expense.
The transport vehicle must be equipped with electrical power, oxygen, and suction and must have sufficient space for the equipment and supplies that the team brings along—stretcher or isolette, monitor, ventilator, oxygen tank(s), medication pack(s), infusion pumps, and more. Compared with helicopters, ambulances are more spacious and able to carry more weight, so they can accommodate larger teams and more equipment. Another advantage of ground ambulance transport is the ability to stop en route if the patient’s condition deteriorates; this feature greatly facilitates the performance of certain interventions, such as intubation.
An airplane may be able to fly to an area when distance (>150 miles), altitude, or weather precludes helicopter use. The use of an airplane necessitates several ambulance transfers.
Transport Physiology
When possible, the transport team tries to provide the same care during transport as the patient would receive in the specialty center. This can be difficult, though, because of limitations in personnel, equipment, and space as well as other environmental challenges.
The team and child are subjected to variable intensities of background noise and vibration while traveling in the vehicle cabin. Noise can impair the team’s ability to auscultate breath sounds, heart sounds, and blood pressure, another reason for monitoring vital signs mechanically and relying on other assessment modalities, such as the level of mentation, skin color, and capillary refill. To mitigate noise, the helicopter crew and patient should wear helmets or headphones (or another wearable noise attenuator such as MiniMuffs [Natus Medical Incorporated, San Carlos, CA]. Motion and vibration can lead to increased metabolic rate, shortness of breath, and fatigue in the patient, as well as motion sickness in the patient and staff.
On fixed- or certain rotary-wing transports, the patient may suffer adverse physiologic effects from altitude. With increasing altitude, the barometric (atmospheric) pressure decreases and gases expand. As the barometric pressure drops and gas expands, the partial pressures of ambient oxygen (PO2) and, consequently, arterial oxygen (PAO2) decrease. For example, at 8,000 feet—an elevation at which unpressurized airplanes may fly, as well as the effective cabin altitude for many pressurized airplanes flying at 35,000 to 40,000 feet—the barometric pressure, PO2, PAO2, and arterial oxygen saturation fall to 565 mm Hg, 118 mm Hg, 61 mm Hg, and 93%, respectively. (In comparison, the barometric pressure, PO2, PAO2, and arterial oxygen saturation are 760 mm Hg, 159 mm Hg, 95 mm Hg, and 100% at sea level.) Although healthy individuals usually tolerate these changes well, patients with respiratory insufficiency, significant blood loss, or shock may decompensate and should receive supplemental oxygen.
Gases expand 10-15% at the few thousand feet at which helicopters typically fly, and approximately 30% at 8,000 feet. Gases within the body itself also expand as the altitude increases. Gas expansion must be appreciated during transport via air of a patient with a pneumocephalus, pneumothorax, bowel obstruction, or another condition involving entrapped gas. Prior to transport, a pneumothorax should be decompressed, and a nasogastric tube inserted for ileus.
Safety
Safety is of paramount importance and mandates constant vigilance by everyone involved. Accident rates for pediatric air and ground transport are estimated at approximately 1/1,000 transports. The team should routinely attend pilot briefs, as well as perform safety inspections of the vehicles and equipment, aided by checklists. When in doubt, the MCP should solicit input from the staff about whether to transport via air or ground ambulance or to employ lights and sirens, decisions that cannot be taken lightly. The pilot’s or driver’s judgment as to the safety of proceeding during inclement weather or with a mechanical problem must not be overruled.
Organizations, such as the FAA and the National Transportation Safety Board, play a role in ensuring safe interfacility transport. The Commission on Accreditation of Medical Transport Systems (CAMTS) is an independent, peer review organization established in 1990 in response to the number of air medical accidents in the 1980s. CAMTS, through voluntary participation, audits and accredits fixed-wing, rotary-wing, and ground interfacility medical transport services.
Family-Centered Care
Family-centered care represents a philosophy that respects the important role that family members play in a child’s care. It recognizes family members and health care providers as partners in caring for the child. Family presence during transport is beneficial because it provides support to children in stressful situations and assists health care providers in delivering care to patients with complex and/or chronic medical problems.
As care is transitioned from the referring hospital, it is the transport team’s responsibility to maintain family-centered care. The team meets with family members to explain the transport process, obtain consent, and discuss anticipated management. When possible, the transport team should attempt to accommodate a family member’s presence on-board. However, the family member and child may need to be separated when the child is critically ill and rapid transport is essential, or if there are space or weight limitations in the air or ground ambulance. In these situations, it is important that family members have a clear understanding of how the child will be cared for during the separation.
Referring Hospital Responsibilities
Transfer of a patient to another facility requires written documentation by the referring physician of the need and reasons for transfer, including a statement that the risks and benefits as well as any alternatives have been discussed with the parents. The parent’s informed consent to the transfer should be obtained.
Federal law under the Emergency Medical Treatment and Active Labor Act (EMTALA), part of the Consolidated Omnibus Budget Reconciliation Act (COBRA), imposes specific requirements that a patient presenting to an ED be given a medical screening examination without regard to ability to pay. If upon examination an emergency medical condition is found, the hospital is required to stabilize the patient or to transfer the patient to another facility if unable to stabilize the patient or if requested by the patient. The primary requirement is that the referring physician must certify that the medical risks of transfer are outweighed by its potential benefits. The receiving hospital must agree to accept the patient and have the space and staff to provide the necessary treatment. The transferring hospital is responsible for arranging for the transfer and ensuring that it is performed by qualified medical personnel with appropriate equipment. It must send copies of the patient’s medical records and test results, even those that become available after the transfer is complete.
Some referring hospitals have entered into transfer agreements with specialty centers in the interests of facilitating the smooth and safe transfer of the pediatric patient. Having prepared forms for all of the above purposes also aids in the transfer process.
Educational Outreach
Besides safe and rapid transport, regional pediatric transport programs (and their specialty centers) have an obligation to provide educational opportunities to community health care providers so that these providers can acquire the necessary skills to evaluate and stabilize a critically ill or injured child until the transport team arrives. These learning activities may include transport case reviews; lectures on pediatric acute care topics; resuscitation programs such as the PALS course, APLS course, and S.T.A.B.L.E. (sugar and safe care, temperature, airway, blood pressure, lab work, emotional support) program; and rotations through the specialty center’s pediatric ED and PICU. These activities also help cement relationships with the referring facility’s staff.
Ajizian SJ, Nakagawa TA. Interfacility transport of the critically ill pediatric patient. Chest. 2007;132:1361-1367.
American Academy of Pediatrics, Section on Transport Medicine. Woodward GA, Insoft RM, Kleinman ME, editors. Air and ground transport of neonatal and pediatric patients. Chicago: American Academy of Pediatrics, 2007.
Institute of Medicine Committee on the Future of Emergency Care in the United States Health System. Emergency care for children: growing pains. Washington, DC: National Academies Press; 2007.
King BR, King TM, Foster RL, et al. Pediatric and neonatal transport teams with and without a physician: a comparison of outcomes and interventions. Pediatr Emerg Care. 2007;23:77-82.
King BR, Woodward GA. Pediatric critical care transport: the safety of the journey; a five-year review of vehicular collisions involving pediatric and neonatal transport teams. Prehosp Emerg Care. 2002;6:449-454.
McCloskey KA, King WD, Byron L. Pediatric critical care transport: is a physician always needed on the team? Ann Emerg Med. 1989;18:961-966.
Nieman CT, Merlino JI, Kovach B, et al. Intubated pediatric patients requiring transport: a review of patients, indications, and standards. Air Med J. 2001;21:22-25.
Philpot C, Day S, Marcdante K, et al. Pediatric interhospital transport: diagnostic discordance and hospital mortality. Pediatr Crit Care Med. 2008;9:15-19.
Woodward GA, Insoft RM, Pearson-Shaver AL, et al. The state of pediatric interfacility transport: consensus of the second national pediatric and neonatal interfacility transport medicine leadership conference. Pediatr Emerg Care. 2002;18:38-43.
61.2 Outcomes and Risk Adjustment
The publication of the IOM reports To Err is Human: Building a Safer Health System and Crossing the Quality Chasm: A New Health System for the 21st Century marked the beginning of a heightened public and professional urgency to improve the quality of health care. Health services research has documented wide variation in the likelihood that patients receive quality, evidence-based health care, and this can negatively impact the health of children and youth. The complexities of delivering high-quality health care are magnified in the ED. Patients are in crisis, EDs are often overcrowded, patient-physician relationships are based on brief interactions, and the variety of complaints and diagnoses is immense. Furthermore, in this complex era, health care professionals, patients, purchasers, and policy makers are demanding more transparency and accountability from health care providers.
Outcome Measures in Emergency Medical Services for Children
Improving the quality of pediatric emergency care requires measurement. Emergency Care for Children: Growing Pains, one report of the 2007 IOM series on the future of emergency care, recommends that pediatric emergency medical systems specifically support the development of national standards for emergency care performance measurement. The Donabedian structure-process-outcome model has set the framework for most contemporary quality measurement and improvement activities. Structural elements provide indirect quality-of-care measures related to a physical setting and resources. Process indicators provide a measure of the quality of care and services by evaluating the method or process by which care is delivered, including both technical and interpersonal components. Outcome elements describe valued results related to lengthening life, relieving pain, reducing disabilities, and satisfying the consumer.
Defining relevant outcomes for pediatric emergency care is difficult. Process measures are abundant and typically focus on a particular condition or chief complaint. Yet defining outcomes pertinent to all pediatric emergency patients is critical to improve and transform emergency care delivery to children. A true “outcome based” approach describes observable measures such as mortality, risk of organ system failure, and disability. Although extremely important, such outcomes are quite rare, and it is often difficult to extricate the contribution of a brief ED encounter from what has taken place in the overall health care system in measuring these outcomes. An alternative approach is a “resource based” outcome measure definition related to the level of care required. Children who are more ill, in general, require more resources. Thus, resource use across groups of patients reflects relative severity of illness in the groups. Given the episodic and brief nature of emergency care, as well as the continuing trends of increasing ED volumes and overcrowding that make it increasingly important to provide each and every ED patient with timely and necessary resources, adopting a “resource based” approach to outcome measures in EMSC is sensible. Examples of resource based outcomes include need for hospital admission (ED disposition), ED length of stay, costs, and diagnostic and therapeutic interventions performed in the ED.
Risk Adjustment
Measuring outcomes offers opportunities for EDs and other components of the health care system to make effective improvements over time, benchmark, and compare their end results with those of other institutions. Meaningful comparisons between EDs or within an ED over time generally require risk adjustment, which accounts for patient-related attributes such as age, or for pre-existing conditions associated with the outcome of interest. Risk-adjustment “levels the playing field,” so that comparison of outcomes is as fair and meaningful as possible. Because children present to EDs with illnesses of varying acuity, ranging from rashes and colds to cardiac arrest, there is an inextricable linkage of severity to outcomes. Severity typifies the concept of “risk”—the higher the severity, the higher the risk of a given outcome. Without risk adjustment, EDs with sicker patients may appear to have worse outcomes.
A large number of instruments have been developed to adjust for severity or risk in clinical research and quality improvement activities. Two severity indices were developed for patients in intensive care units: the APACHE (Acute Physiology And Chronic Health Evaluation) system for adults and the PRISM (Pediatric Risk of Mortality) score for pediatric patients. These indices are not well-suited for EMSC, given the extremely low rate of mortality. Several disease-specific acuity scoring systems are available for use in EMSC. The majority of these are intended for use in trauma patients, including the Injury Severity Score, Trauma Score, and Pediatric Trauma Score. Others are available for asthma, croup, and febrile young children. These measures cannot be applied broadly to all pediatric emergency patients.
Risk Adjustment Tools in EMSC
The choice of a risk-adjustment tool depends on several factors, including the population under study, the setting, and the outcomes of interest. Two risk-adjustment tools have been developed specifically for pediatric emergency medicine, the second-generation Pediatric Risk of Admission (PRISA II) score and the Revised Pediatric Emergency Assessment Tool (RePEAT).
Pediatric Risk of Admission II
PRISA II uses components of acute and chronic medical history and physiology to determine the probability of hospitalization. The outcome measure of interest is mandatory hospital admission (admissions utilizing therapies best delivered on an inpatient basis). The patient-related attributes contributing to the PRISA II risk-adjustment score are listed in Table 61-3. Analytic models including the PRISA II score had good calibration (how well the probabilities predicted from the model correlated with the observed outcomes in the population) and discrimination (the ability to categorize subjects correctly into the categories of interest) with respect to mandatory hospital admission. Construct validity of the PRISA score was demonstrated by measuring the rates of the secondary outcomes: mandatory admission, PICU admission, and mortality. As the probability of hospital admission rose, the proportion of patients with these increasing care requirements also increased. This finding strongly supports the use of the PRISA II score as a valid measure of severity of illness. In addition, PRISA II was used to demonstrate racial/ethnic differences in severity-adjusted hospitalization rates, and also demonstrated that teaching hospitals had higher than expected severity-adjusted admission rates in comparison with non-teaching hospitals.
Revised Pediatric Emergency Assessment Tool
The Revised Pediatric Emergency Assessment Tool uses a limited set of data collected at the time of triage to model severity of illness as reflected by the level of care provided in the ED. This tool was developed to predict the level of care provided—routine assessment (clinical examination only ± nonprescription medicine), specific ED care (ED diagnostics and/or therapeutics), or hospital admission—with the implicit assumption that patients with a higher level of care have a higher severity of illness. The patient-related attributes contributing to the RePEAT risk-adjustment score are listed in Table 61-4. As with PRISA II, analytic models including the RePEAT score had good calibration and discrimination with respect to predicting ED care and hospital admission. Furthermore, analytic models that compare costs and ED length of stay between EDs are improved by adjustment for severity of illness using the RePEAT score. These results demonstrate that RePEAT is a reasonable marker of severity of illness and that inclusion of this severity index substantially improves the ability to compare outcomes between EDs.
Chamberlain JM, Joseph JG, Pollack MM. Differences in severity-adjusted pediatric hospitalization rates are associated with race/ethnicity. Pediatrics. 2007;119:e1319-e1324.
Chamberlain JM, Patel KM, Pollack MM. The pediatric risk of hospital admission score: a second-generation severity-of-illness score for pediatric emergency patients. Pediatrics. 2005;115:388-395.
Chamberlain JM, Patel KM, Pollack MM. The association of emergency department care factors with admission and discharge decisions for pediatric patients. J Pediatr. 2006;149:644-649.
Donabedian A. The quality of care: how can it be assessed? JAMA. 1988;260:1743-1748.
Gorelick MH, Alessandrini EA, Cronan K, et al. Revised pediatric emergency assessment tool (RePEAT): a severity index for pediatric emergency care. Acad Emerg Med. 2007;14:316-323.
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press; 2001.
Institute of Medicine. The future of emergency care in the United States health system. Washington, DC: National Academies Press; 2006.
Institute of Medicine. To err is human: building a safer health care system. Washington, DC: National Academy Press; 2000.
Knaus WA, Wagner DP, Draper EA, et al. The APACHE III prognostic system: risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100:1619-1636.
MacKenzie EJ. Injury severity scales: overview and directions for future research. Am J Emerg Med. 1984;2:537-549.
Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated pediatric risk of mortality score. Crit Care Med. 1996;24:743-752.
61.3 Principles Applicable to the Developing World
International pediatric emergency medicine, or IPEM, is an emerging academic field whose practitioners are committed to international collaboration aimed at improving the quality of care for children outside their national borders (see Tables 61-5 and 61-6 on the Nelson Textbook of Pediatrics website at
www.expertconsult.com).
Table 61-5 PEDIATRIC EMERGENCY MEDICINE (PEM) PROFESSIONAL ORGANIZATIONS
| Australia, New Zealand | |
| PEM Section, Canadian Association of Emergency Physicians (CAEP) | Canada |
| France | |
| PEM Section, Canadian Paediatric Society (CPS) | Canada |
| Israel | |
| Italy | |
| Mexico | |
| Spain | |
| Turkey | |
| Europe | |
| USA | |
| USA | |
| USA |
Table 61-6 PEDIATRIC EMERGENCY MEDICINE RESEARCH COLLABORATIVES
| PREDICT: Paediatric Research in Emergency Departments International Collaborative | Australia, New Zealand | www.pems.org.au |
| PERC: Pediatric Emergency Research Canada | Canada | www.perc-canada.ca |
| PECARN: Pediatric Emergency Care Applied Research Network | USA | www.pecarn.org |
| PEM-CRC: Collaborative Research Committee of the American Academy of Pediatrics | USA | www.aap.org/sections/PEM/pemcrc.htm |
| REPEDS: Research in European Paediatric Emergency Departments | Belgium, France, Great Britain, Hungary, Israel, Italy, Northern Ireland, Saudi Arabia, Spain, Sweden, Turkey | www.pemdatabase.org/REPEM |
Many models currently exist for the delivery of emergency care. The triage officer model is one in which a practitioner who works in an emergency department briefly provides intake for all patients and calls specialists to provide definitive care depending on the nature of the presenting complaint. The multiple physician model describes a scenario in which patients are divided by their chief complaints into medical, surgical, and pediatric groups. The field of emergency medicine provides a specialist skilled in the recognition, stabilization, and definitive treatment of a wide variety of acute illnesses and injuries. This approach to managing an emergency center is more efficient, relies less heavily on specialist availability, and requires fewer highly trained practitioners to operate. Children and adolescents constitute a subpopulation of emergency patients that deserves special attention because of pediatric-specific conditions, unique anatomy and physiology, developmental staging, and parental interactions.
Pediatric emergency medicine (PEM) depends on the health care priorities and resources of a given geographic or physical setting. The places in which emergency care takes place range from the community (for those with no access to organized medical care) to state-of-the-art pediatric emergency departments in populated centers. The scope ranges from care of the individual patient to populations of children involved in large-scale disasters. Barriers to quality care are different in each situation and in each part of the world, with the implication for the astute IPEM practitioner that solutions must be targeted to the local context of health care within a given environment.
EMSC and the Continuum of Care Model
Emergency Medical Services for Children is a U.S. federal initiative designed to reduce child and youth disability and death due to severe illness or injury. The EMSC program has developed an operational framework for conceptualizing a systems approach to emergency care for children, known as the continuum of care model. The model specifically refers to the seamless care of ill and injured children from the community and medical home through to definitive care and return to the community. It has the following 5 principal components:
This framework can also be applied to discussion of emergency care for children on an international level. With medical infrastructures that may not be consistent or well organized, or that have been weakened by civil strife, natural disasters, and economic loss, the focus of child health in the developing world has been on prevention and acute care.
Applying the Continuum of Care Model to the Developing World
Prevention
Infectious Diseases
International child health has focused mainly on reducing preventable childhood illnesses, primarily through immunizations. Enormous advances have been realized in measles, neonatal tetanus, and polio reduction; wild-type smallpox was eradicated in 1978. Although there are advocates for providing primary care interventions (e.g., vaccinations) in the ED, the role of the PEM practitioner in this area of prevention has been limited.
Injuries
Injuries are a leading cause of childhood morbidity and mortality. Unintentional injuries contribute the majority of mortality to children aged 5 to 19 yr. Intentional injuries, an underrecognized and underreported phenomenon primarily for cultural reasons, make a smaller but significant contribution. Unintentional injuries cause 2000 childhood deaths daily or 830,000 annually worldwide. The burden of these deaths is borne disproportionately by children in middle- and lower-income countries, where more than 95% of all injury deaths occur. For each of these deaths, many more children are permanently disabled and an even larger number are treated and released without permanent sequelae.
The World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) have outlined several proven injury prevention strategies of which child health practitioners in the global community must be aware. The top 3 causes of injury mortality are traffic-related injuries, burns, and drowning. There are 7 specific effective strategies for reducing road traffic injuries: a minimum drinking age, appropriate child restraints and seatbelts, helmets for motorcycle and bicycle riders, reduced vehicle speeds around schools and residential areas, running lights on motorcycles, graduated licensing for drivers, and separation of different types of road users. There is insufficient evidence to demonstrate that school-based programs on drunk-driving, increased pedestrian visibility, or designated driver programs are effective. Although these strategies have been proven effective, the data are based on research from the United Stated and may not be generalizable to other countries. It may be difficult to reduce vehicle speeds around schools when there is insufficient infrastructure for street signs. Alternatively, lack of separation of car and bus traffic from bicyclists and pedestrians contributes to unsafe and dangerous road conditions. This is more of a problem in lower- and middle-income countries, where bicycles and motorized two-wheel vehicles are used to carry children as well as goods, while the drivers negotiate among rapidly moving vehicles. With rising income, these countries have seen increases in both the number of cars and the number of two-wheeled vehicles, with a corresponding increase in the number of related injuries.
For reducing drowning deaths, strategies that have proven effective focus on creating barriers between children and water hazards, such as covering wells, buckets, and other standing sources of water, and placing high fences around pools (Chapter 67). Burns have been addressed by advocating for installation of smoke detectors and lowering the temperature of water from water heaters (Chapter 68).
For the PEM practitioner, involvement in prevention depends largely on the local epidemiology of injuries and the factors contributing to those injuries. Involvement can include parental and patient education or activism to change local practices through laws and new community standards. One can also work on a larger scale on projects initiated by a group such as the WHO, UNICEF, or Safe Kids Worldwide to develop and evaluate intervention strategies that target specific preventable injuries.
Out-of-Hospital Care
Out-of-hospital care comprises access to emergency services, prehospital care, and interfacility transport of patients. Morbidity and mortality arise from delayed or limited access to emergency care, lack of prehospital care, transport without proper monitoring or trained personnel, or delayed transport to a higher level of care. Safe transport of seriously ill children is a neglected global health issue. An emergency response system must address the following links in the patient’s care: a communication system with prompt activation of EMS, the correct assessment and initial treatment of the patient, and the rapid transport to definitive care.
Access to Care
When a child is injured or ill, a parent or caretaker must be able to access help and activate EMS. Many countries around the world have dedicated emergency numbers to rapidly dispatch medical, police, or fire services. The universal U.S. emergency number system 911 today covers the large majority of the country and has enhanced features of automatically linking the phone number to an address. However, there remain limitations to universal access resulting from absence of phones in some households, unclear addresses in rural areas, and insufficient reach of the emergency system. In low- and middle-income countries, no such universal emergency numbers have been established, requiring access by direct dialing to an ambulance, if such private services exist. In most low- and middle-income countries, the family must bring the ill or injured child to the health facility for stabilization and treatment. For this to occur, families must overcome financial and geographic barriers, which can result in delayed presentation for care. This delay predictably increases the acuity of the illness or injury and associated complications, and decreases the likelihood of full recovery and survival.
Prehospital Care
In regions with maturing EMS systems, there must be adequately trained personnel to stabilize and transport the child to a medical facility. The quality and level of training of such prehospital personnel vary tremendously among countries and within regions of the same country. In urban areas, there is a greater concentration of medical care and therefore a greater opportunity to have strong prehospital training. In most of Asia and sub-Saharan Africa, trained personnel are used primarily to transfer patients between health facilities, and not from the initial site of illness or injury. In most high-income countries, EMS are dispatched to the patient.
A different approach to prehospital work is exemplified by the French EMS, called Service d’Aide Médicale d’Urgence (SAMU). In this system, a physician is integral to the prehospital team. A physician, often a general practitioner without EM specialization, will staff the ambulance and go to the patient’s home to assess, stabilize, and initiate treatment. This system is used in other countries, including Argentina and Portugal. There are no clear data on the cost-effectiveness and patient outcomes associated with delivery of patients to the nearest facility vs bringing hospital resources to the patient.
Around the world, the effort to establish standardized approaches to prehospital care exists primarily in the form of courses to educate EMS and hospital personnel in the emergency management of patients. For trauma care, the WHO manuals Prehospital Trauma Care Systems and Guidelines for Essential Trauma Care both focus on guidelines for prehospital and trauma care systems that are affordable and sustainable. The AAP course Pediatric Education for Prehospital Professionals (PEPP) is a dynamic, modularized teaching tool designed to provide specific pediatric prehospital education that can be adapted to any EMS system. Table 61-7 lists additional prehospital resources.
Table 61-7 PEDIATRIC EMERGENCY MEDICINE (PEM) RESOURCES
| Prehospital | |
| Hospital care | |
| Humanitarian emergencies | |
| Access to academic publications relevant to PEM | |
| Involvement | |
| Health organizations involved in international PEM activities | |
Although most middle- and high-income countries have a system of trained EMS workers, low-income countries lack this advanced tier of emergency care. In these countries, it becomes necessary to train a cadre of first responders who can initiate lifesaving care for the ill and injured patient. First responders can be drawn from specific populations, such as students, soldiers, or public servants. Training needs to emphasize basic lifesaving and limb-saving interventions, including how to stop bleeding and support breathing, accessing advanced care, and splinting broken limbs. In Ghana, for example, 335 taxi drivers participated in a first-aid course that relied heavily on demonstration and practice rather than knowledge transfer through didactic sessions. Taxi drivers were selected because they already provided much of the transport for injured patients, either voluntarily or for pay by the family. Two years after the course, external evaluators favorably rated the quality of their care in comparison with that of a group of untrained drivers. In rural areas, such first responders become vital in providing emergency interventions when more definitive care is distant. Thus, a system of trained first responders forms the foundation of an effective prehospital system.
Methods of Transport
In many low-income countries, there is no means of transport other than the family’s motorized or other type of transport. Health centers may only have one vehicle for transport to a higher-level facility. This vehicle may also be utilized for outreach primary care services, such as offering immunizations and collecting drugs and equipment from a central supply location, and, sometimes, may be improperly used for personal reasons by local officials or politicians. In large cities, taxis and auto rickshaws are frequently used because they are rapidly available and well disseminated within cities. Where there are organized prehospital systems, different types of vehicles are adapted for emergency transportation, from fully equipped ambulances to basic transport with trained personnel. The WHO recommends identifying transport vehicles in advance, choosing vehicles that can be repaired and maintained locally, and equipping the vehicles according to recognized standards. Therefore the provision of available and appropriately staffed and equipped transport vehicles is crucial to the realization of recommended emergency care plans.
Hospital-Based Care
Once a child has reached a medical facility for the care of an injury or illness, adequate emergency services must be available. In many countries, the ED serves only as a triage area where patients are distinguished by their likely disease process and directed for admission to the corresponding unit within the hospital. Strengthening emergency services includes seeing the ED as a unit where definitive treatment can be provided to the ill and injured child. Critically ill children must receive not only prompt care but also correct care. Such expedience and accuracy are ensured by implementation of an effective triage system, moving the sickest patients to immediate care and standardizing the initial care of emergency conditions.
Triage
Children requiring emergency care frequently are not promptly recognized. Too often, children presenting to EDs are treated on a first-come first-served basis, in an approach that creates long waiting times for critically ill children, a contributor to unnecessary mortality. Medical facilities need to adopt an efficient and effective triage system in order to rapidly respond to the needs of patients and to assign the appropriate amount of resources. To this end, WHO has developed a course entitled Emergency Triage Assessment and Treatment (ETAT). This course teaches health practitioners to triage patients on arrival as having emergency, priority, or nonurgent signs and to provide emergency treatment for life-threatening conditions. ETAT emphasizes the evaluation of a patient’s ABCD status to identify emergency situations—the patency of the airway (A), the quality of breathing (B), the quality of circulation and presence of coma or convulsions (C), and the presence of severe dehydration (D).
One of the benefits of the ETAT guidelines is that they can be adapted to centers with limited resources and are applicable to areas with high morbidity and mortality from meningitis, dehydration, malaria, respiratory illness, and malnutrition. Another benefit is that the care algorithms are based on limited diagnostic studies, that is, hemoglobin measurement, blood smear for malaria, and bedside blood glucose testing. Widely accepted triage assessment guidelines are teachable to emergency care staff, and their adoption can provide better organization within a health care center. At the Queen Elizabeth Central Hospital in Blantyre, Malawi, for example, the institution of triage and rapid treatment in its emergency care center led to a 50% decrease in the mortality of children within 24 hours of presentation to the hospital.
Beyond triage, education on overall emergency center organization is a low-resource intervention that can obviate some of the obstacles to quality care delivery. Additionally, the arrangement of short-stay areas (hydration and infusion rooms) can lessen the burden on inpatient units.
Pediatric-Specific Emergency Centers
Descriptions on the development of pediatric-specific emergency centers are insufficient. Anecdotally, most countries have developed at least one pediatric-capable center, usually as part of an academic medical center. The emergency services in these centers are variable but certainly can be a starting point from which to build overall improvement in pediatric emergency care.
Practitioners
Throughout the world, nurses, paramedics, and nonspecialist physicians provide most of the care to acutely ill or injured children. The majority of sick children attend local clinics or district or central hospitals, where financial and human resources are not always matched to the potential acuity of presenting patient complaints. Nominal supervision is provided to staff attending these patients. Pediatric EDs located in tertiary hospitals are often staffed by training physicians with little or no supervision from faculty, who themselves may have limited exposure to or training in PEM. General hospitals lack dedicated pediatric staff; guidelines as to which patients should be moved to a higher level of care are often not standardized and depend on local influences and/or cultural beliefs about health and illness.
Clinical Guidelines
The Integrated Management of Childhood Illnesses (IMCI) guidelines were developed by the WHO and UNICEF to provide assistance in the initial triage and management of the presenting signs and symptoms of the major killers of the under–5 yr population in first-level health facilities (e.g., clinics, health centers, and outpatient departments of hospitals). The flow charts within each chapter of the IMCI manuals allow easy accessibility to materials that can enhance education and outreach to less experienced health workers.
Evaluations in various countries of the implementation of IMCI guidelines have shown improvements in health worker performance and quality of care as well as decreases in delay in treatment and mortality of under–5 yr children. These guidelines also dramatically reduce the cost of health care. The WHO website provides all the necessary implementation tools, including course manuals and evaluation tools.
Trauma
Morbidity and mortality from trauma is one of the most prevalent problems for children worldwide. Trauma care presents the challenge of sequential, often simple, interventions that must be performed in a timely manner to limit the severity of the outcome. However, with lack of specific training, signs and symptoms of pediatric trauma may go unrecognized or may be underappreciated. Trauma courses such as Advanced Trauma Life Support (ATLS) are educational tools that can be disseminated to improve the quality of care at emergency centers worldwide. Not expressly addressed in the ATLS course is specific concern about child abuse as the cause of trauma. This is an area of pediatric care that many countries do not yet address in their medical training, their law enforcement, or their judicial systems. The epidemiologic need for reliable trauma registries is great, as is the need to identify personnel with trauma management skill sets and dedicated trauma centers to serve as higher-level referral sites.
Equipment
Pediatric emergency textbooks, pediatric and emergency medicine professional organizations, WHO, and nongovernmental and governmental health organizations have all published pediatric emergency equipment guidelines, for a variety of settings in which acutely ill and injured children would present. Although these equipment guidelines may represent minimum supplies to treat the widest variety of pediatric emergencies, the roles of substitution and improvisation often provide for equivalent function of recommended supplies.
Inpatient Services
After the initial stabilization, children requiring ongoing care are admitted to the hospital. The quality of inpatient services varies greatly depending on institutional and provider experience, comfort with pediatric conditions, and the resources available to treat them. The WHO has produced the Pocket Book of Hospital Care for Children, which is based on IMCI guidelines and focuses on inpatient management of high-morbidity/high-mortality illnesses common in developing countries.
Humanitarian Disasters
Children are a vulnerable population who experience disproportionate suffering during humanitarian emergencies, either natural (earthquakes, tsunamis, hurricanes, floods, and droughts) or manmade (armed conflicts, terrorist attacks). The under–5 yr population is especially susceptible to infectious diseases, malnutrition, and trauma following disasters. The Rainbow Center for Global Child Health at the Case Western Reserve University School of Medicine offers a training course, Management of Humanitarian Emergencies: Focus on Children and Families, that concentrates on the needs of children in disasters. The intent of the Center is to educate and train health professionals, relief workers, and policymakers to recognize and address the unique needs of children affected by manmade and natural disasters worldwide. The AAP also maintains a CHILDisaster Network, which acts as an electronic database of child health professionals with education and experience in humanitarian emergencies. Nongovernmental organizations can access the database to solicit practitioners to aid in disaster response.
The WHO’s Manual for the Health Care of Children in Humanitarian Emergencies is based on IMCI guidelines and addresses the emergency care of children in disaster situations in which hospital facilities and resources are not immediately available. It goes beyond the IMCI guidelines by discussing initial assessment and management of trauma, burns, and poisonings. Pre-existing IMCI guidelines assumed a functioning health system that facilitated the referral of children, which may not be available in all emergency situations. This manual also includes the initial management of severe conditions, such as injuries, burns, neonatal illness, and psychosocial problems, which are considered high priority in acute care settings.
Improvement in Quality of Care
In many locations, low-resource interventions are the easiest to provide and can often make large differences in the quality of care offered by any given practitioner or health care center. A long-term goal should be the establishment of ongoing quality assessment and critical incident monitoring. International PEM development should incorporate all stakeholders in the delivery of emergency care in a given catchment area. This effort may include consumers, public health and government officials, and health care officers and practitioners. One may also make use of relationships with local and foreign universities, professional organizations (see Table 61-5), and governmental and nongovernmental organizations.
Promotion of the Emergency Medicine Model
Because EM is not recognized as a specialty in most countries, little effort has been devoted to developing the infrastructure needed to provide the subspecialist model of emergency care. Promotion of and advocacy for this EM model are critical to improving the quality of prehospital and hospital-based care for children. EM promotion should include training in PEM. Practitioners worldwide must be facile in aspects of emergency care specific to children, including unique anatomy and physiology, developmental and behavioral factors, specific childhood diseases, and the presence of families. Subspecialty training is available in several developed countries but is slowly spreading as a subspecialty of pediatric or emergency medicine in areas with developing medical training.
Exchange and Dissemination of Information
The WHO established the HINARI (Health InterNetwork Access to Research Initiative) program to allow free or reduced-cost access to more than 6200 journal publications. This Internet access is made available to the 108 countries with gross national income per capita less than $3500. For middle-income countries not meeting the financial eligibility, Internet access continues to be a barrier, and resources may be limited to out-of-date textbooks and journals.
Another valuable tool is the website Pemdatabase.org. This nonproprietary site was started as an online resource for PEM practitioners. It contains links to PEM abstracts and articles, evidence-based reviews, pediatric resuscitation websites, relevant journals, as well as PEM conferences and professional organizations.
Research Support and Training
Several examples of inter-institutional international research collaborations could serve as models for facilities in the developing world (see Table 61-6). Researchers can assist with developing low-cost mechanisms for data collection and database management. Additionally, training in the importance of utilizing evidence-based practices and appropriate research design can be useful.
Exchange Programs
Clinical exchange programs that bring practitioners from lower-resourced areas to places with more sophisticated emergency care exist. The International Pediatric Emergency Medicine Elective offered by the Hospital for Sick Children in Toronto and the Stecker Scholars Program at Ohio State University are two of many formal and informal partnerships.
Duke T, Kelly J, Weber M, et al. Hospital care for children in developing countries: clinical guidelines and the need for evidence. J Trop Pediatr. 2006;52:1-2.
HINARI Access to Research Initiative. About HINARI (website). http://www.who.int/hinari/about/en. Accessed March 20, 2009
International Federation of Emergency Medicine. About IFEM (website). http://www.ifem.cc/about/about.htm. Accessed April 2, 2009
Khan AN, Rubin DH. International pediatric emergency care: establishment of a new specialty in a developing country. Pediatr Emerg Care. 2003;19:181-184.
Molyneux E. Emergency care for children in resource-constrained countries. Trans R Soc Trop Med Hyg. 2009;103:11-15.
Molyneux E, Ahmad S, Roberston A. Improved triage and emergency care for children reduces inpatient mortality in a resource-constrained setting. Bull World Health Org. 2006;84:314-319.
Moss WJ, Ramakrishnan M, Storms D, et al. Child health in complex emergencies. Bull World Health Org. 2006;84:58-64.
Nolan T, Angos P, Cunha AJLA, et al. Quality of hospital care for seriously ill children in less-developed countries. Lancet. 2001;357:106-110.
Norton R, Hyder AA, Bishai D, et al. Unintentional injuries. In: Jamison DT, Breman JG, Measham AR, et al, editors. Disease control priorities in developing countries. ed 2. New York: Oxford University Press and the World Bank; 2006:737-753. This book can be downloaded from www.dcp2.org/pubs
Peden M, Oyegbite K, Ozannr-Smith J, et al, editors. World report on child injury prevention. Geneva: WHO Press, 2009. This report can be downloaded from www.who.int/violence_injury_prevention/child/injury/world_report/en/index.html
Siddiqui EU, Razzak JA. Pediatric emergency medicine—an evolving sub-speciality in Pakistan. J Coll Physicians Surg Pak. 2008;18:135-136.
United Nations Children’s Fund (UNICEF). Progress for children: a world fit for children statistical review, No. 6. New York: UNICEF; 2007. This booklet can be downloaded from www.unicef.org/publications/index.html
United States Agency for International Development. The first modern pediatric ER in the region opens in Georgia (website). www.usaid.gov/stories/georgia/ss_ge_er.html. Accessed March 20, 2009
Walker DM, Tolentino VR, Teach SJ. Trends and challenges in international pediatric emergency medicine. Curr Opin Pediatr. 2007;19:247-252.
World Health Organization (WHO). Emergency triage assessment and treatment (ETAT): manual for participants. Geneva: WHO Press; 2005. This manual is available for download from www.who.int/child_adolescent_health/documents/9241546875/en/index.html
World Health Organization (WHO). Guidelines for essential trauma care. Geneva: WHO Press; 2004. This book can be downloaded from www.who.int/violence_injury_prevention/publications/services/guidelines_traumacare/en/index.html
World Health Organization (WHO). Integrated management of childhood illness (IMCI). Geneva: WHO Press; 2007. This book can be downloaded from www.who.int/child_adolescent_health/topics/prevention_care/child/imci/en/index.html
World Health Organization (WHO). Prehospital trauma care systems. Geneva: WHO Press; 2005. This book can be downloaded from www.who.int/violence_injury_prevention/publications/services/39162_oms_new.pdf