Chapter 199 Brucella
Human brucellosis, caused by organisms of the genus Brucella, continues to be a major public health problem worldwide. Humans are accidental hosts and acquire this zoonotic disease from direct contact with an infected animal or consumption of products of an infected animal. Although brucellosis is widely recognized as an occupational risk among adults working with livestock, much of the brucellosis in children is food-borne and is associated with consumption of unpasteurized milk products. It is also a potential agent of bioterrorism (Chapter 704).
Etiology
Brucella abortus (cattle), B. melitensis (goat/sheep), B. suis (swine), and B. canis (dog) are the most common organisms responsible for human disease. These organisms are small, aerobic, non–spore-forming, nonmotile, gram-negative coccobacillary bacteria that are fastidious in their growth but can be grown on various laboratory media including blood and chocolate agars.
Epidemiology
Because of improved sanitation, brucellosis has become rare in industrialized countries. Brucellosis exists worldwide and is especially prevalent in the Mediterranean basin, Arabian Gulf, Indian subcontinent, and parts of Mexico and Central and South America. In industrialized countries, recreational or occupational exposure to infected animals is a major risk factor for the development of disease. In the USA, 50% of cases occur in California and Texas. Among children, geographic locations that are endemic for B. melitensis remain areas of increased risk for the development of infection. In such locations, unpasteurized milk from goats or camels may be used to feed children, thus leading to the development of brucellosis. A history of travel to endemic regions or consumption of exotic food or unpasteurized dairy or dairy products may be an important clue to the diagnosis of human brucellosis.
Pathogenesis
Routes of infection for these organisms include inoculation through cuts or abrasions in the skin, inoculation of the conjunctival sac of the eye, inhalation of infectious aerosols, or ingestion of contaminated meat or dairy products. The risk for infection depends on the nutritional and immune status of the host, the route of inoculum, and the species of Brucella. For reasons that remain unclear, B. melitensis and B. suis tend to be more virulent than B. abortus or B. canis.
The major virulence factor for Brucella appears to be its cell wall lipopolysaccharide. Strains containing smooth lipopolysaccharide have been demonstrated to have greater virulence and are more resistant to killing by polymorphonuclear leukocytes. These organisms are facultative intracellular pathogens that can survive and replicate within the mononuclear phagocytic cells (monocytes, macrophages) of the reticuloendothelial system. Even though Brucella are chemotactic for entry of leukocytes into the body, the leukocytes are less efficient at killing these organisms than other bacteria despite the assistance of serum factors such as complement.
Organisms that are not phagocytosed by the leukocytes are ingested by the macrophages and become localized within the reticuloendothelial system. Specifically, they reside within the liver, spleen, lymph nodes, and bone marrow and result in granuloma formation. Antibodies are produced against the lipopolysaccharide and other cell wall antigens. This provides a means of diagnosis and probably has a role in long-term immunity. The major factor in recovery from infection appears to be development of a cell-mediated response resulting in macrophage activation and enhanced intracellular killing. Specifically, sensitized T lymphocytes release cytokines (e.g., interferon-γ and tumor necrosis factor-α), which activate the macrophages and enhance their intracellular killing capacity.
Clinical Manifestations
Brucellosis is a systemic illness that can be very difficult to diagnose in children without a history of animal or food exposure. Symptoms can be acute or insidious in nature and are usually nonspecific, beginning 2-4 wk after inoculation. Although the clinical manifestations do vary, the classic triad of fever, arthralgia/arthritis, and hepatosplenomegaly can be demonstrated in most patients. Some present as a fever of unknown origin. Other associated symptoms include abdominal pain, headache, diarrhea, rash, night sweats, weakness/fatigue, vomiting, cough, and pharyngitis. A common constellation of symptoms in children is refusal to eat, lassitude, refusal to bear weight, and failure to thrive. Besides hepatosplenomegaly, the physical findings on examination are usually few, with the exception of arthritis. The fever pattern can vary widely, and virtually any organ or tissue can be involved.
If abnormalities are demonstrated on physical examination, monoarticular arthritis of the knees and hips in children and of the sacroiliac joint in adolescents and adults can be found. Although headache, mental inattention, and depression may be demonstrated in patients with brucellosis, invasion of the nervous system occurs in only about 1% of cases. Neonatal and congenital infections with these organisms have also been described. These have been transmitted transplacentally, from breast milk, and through blood transfusions. The signs and symptoms associated with brucellosis are vague and not pathognomonic.
Diagnosis
Routine laboratory examinations of the blood are not helpful; thrombocytopenia, neutropenia, anemia, or pancytopenia may occur. A history of exposure to animals or ingestion of unpasteurized dairy products may be more helpful. A definitive diagnosis is established by recovering the organisms in the blood, bone marrow, or other tissues. Although automated culture systems and the use of the lysis-centrifugation method have shortened the isolation time from weeks to days, it is prudent to alert the clinical microbiology laboratory that brucellosis is suspected. Isolation of the organism still may require as long as 4 wk from a blood culture sample unless the laboratory is using an automated culture system such as the lysis centrifugation method where the organism can be recovered in <5 days. Bone marrow cultures may be superior to blood cultures when evaluating patients with previous antimicrobial therapy. Caution is advised when using automated bacterial identification systems, because isolates have been misidentified as other gram-negative organisms (Haemophilus influenzae type b).
In the absence of positive culture results, various serologic tests have been applied to the diagnosis of brucellosis. The serum agglutination test (SAT) is the most widely used and detects antibodies against B. abortus, B. melitensis, and B. suis. This method does not detect antibodies against B. canis because this organism lacks the smooth lipopolysaccharide. No single titer is ever diagnostic, but most patients with acute infections have titers of ≥1 : 160. Low titers may be found early in the course of the illness, requiring the use of acute and convalescent sera testing to confirm the diagnosis. Because patients with active infection have both an immunoglobulin M (IgM) and an IgG response and the SAT measures the total quantity of agglutinating antibodies, the total quantity of IgG is measured by treatment of the serum with 2-mercaptoethanol. This fractionation is important in determining the significance of the antibody titer because low levels of IgM can remain in the serum for weeks to months after the infection has been treated. It is important to remember that all titers must be interpreted in light of a patient’s history and physical examination. False-positive results due to cross-reacting antibodies to other gram-negative organisms such as Yersinia enterocolitica, Francisella tularensis, and Vibrio cholerae can occur. In addition, the prozone effect can give false-negative results in the presence of high titers of antibody. To avoid this issue, serum that is being tested should be diluted to ≥1 : 320.
Among newer tests, the enzyme immunoassay appears to be the most sensitive method for detecting Brucella antibodies but less specific as compared to agglutination tests. Polymerase chain reaction assays are also becoming available but at this time are mostly limited to research facilities but could be particularly useful in patients with complications (e.g., neurobrucellosis) where serologic testing often fails.
Differential Diagnosis
Brucellosis may be confused with other infections such as tularemia, cat scratch disease, typhoid fever, and fungal infections due to histoplasmosis, blastomycosis, or coccidioidomycosis. Infections caused by Mycobacterium tuberculosis, atypical mycobacteria, rickettsiae, and Yersinia can present in a similar fashion to brucellosis.
Treatment
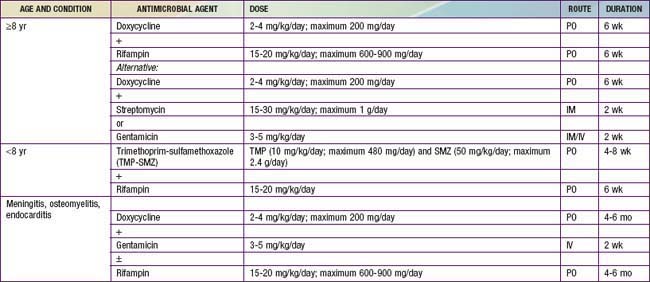
Many antimicrobial agents are active in vitro against the Brucella species, but the clinical effectiveness does not always correlate with these results. Doxycycline is the most useful antimicrobial agent and, when combined with an aminoglycoside, is associated with the fewest relapses (Table 199-1). Treatment failures with β-lactam antimicrobial agents, including the 3rd generation cephalosporins, may be due to the intracellular nature of the organism. Agents that provide intracellular killing are required for eradication of this infection. Similarly, it is apparent that prolonged treatment is the key to preventing disease relapse. Relapse is confirmed by isolation of Brucella within weeks to months after therapy has ended and is usually not associated with antimicrobial resistance.
The onset of initial antimicrobial therapy may precipitate a Jarisch-Herxheimer–like reaction, presumably due to a large antigen load. It is rarely severe enough to require corticosteroid therapy.
Prognosis
Before the use of antimicrobial agents, the course of brucellosis was often prolonged and may have led to death. Since the institution of specific therapy, most deaths are due to specific organ system involvement (e.g., endocarditis) in complicated cases. The prognosis after specific therapy is excellent if patients are compliant with the prolonged therapy (see Table 199-1).
Prevention
Prevention of brucellosis is dependent on effective eradication of the organism from cattle, goats, and swineherds as well as from other animals. Pasteurization of milk and dairy products for human consumption remains an important aspect of prevention. No vaccine currently exists for use in children and, therefore, education of the public continues to have a prominent role in prevention of this disease.
Franco MP, Mulder M, Gilman RH, et al. Human brucellosis. Lancet Infect Dis. 2007;7:775-786.
Pappas G, Akritidis N, Bosilkovski M, et al. Brucellosis. N Engl J Med. 2005;352:2325-2336.
Ramin B, MacPherson P. Human brucellosis. BMJ. 2010;341:884-885.
Shen MW. Diagnostic and therapeutic challenges of childhood brucellosis in a nonendemic country. Pediatrics. 2008;121:e1178-e1183.
Skalsky K, Yahav D, Bishara J, et al. Treatment of human brucellosis: systematic review and meta-analysis of randomizes controlled trials. BMJ. 2008;336:701-704.
Solera J, Geijo P, Largo J, et al. A randomized, double-blind study to assess the optimal duration of doxycycline treatment for human brucellosis. Clin Infect Dis. 2004;39:1776-1782.
Troy SB, Rickman LS, Davis CE. Brucellosis in San Diego: epidemiology and species-related differences in acute clinical presentations. Medicine. 2005;84:174-187.