Chapter 213 Relapsing Fever (Borrelia)
Relapsing fever is characterized by recurring fevers and flulike symptoms such as headaches, myalgia, arthralgia, and rigors.
Etiology
Relapsing fever is an infection transmitted by arthropods (lice or ticks) and caused by spirochetes of the genus Borrelia.
Louse-borne (epidemic) relapsing fever is caused by Borrelia recurrentis and is transmitted from person to person by Pediculus humanus, the human body louse. Human infection occurs as a result of crushing lice during scratching, facilitating entry of infected hemolymph through abraded or normal skin or mucous membranes.
Tick-borne (endemic) relapsing fever is caused by several species of Borrelia and is transmitted to humans by Ornithodoros ticks. Borrelia hermsii and Borrelia turicatae are the common species in the western USA, and Borrelia dugesi is the major cause of disease in Mexico and Central America. Human infection occurs when saliva, coxal fluid, or excrement is released by the tick during feeding, thereby permitting spirochetes to penetrate the skin and mucous membranes.
Epidemiology
Louse-borne relapsing fever tends to occur in epidemics associated with war, poverty, famine, and poor personal hygiene, often in association with typhus. This form of relapsing fever is no longer seen in the USA but is endemic in parts of East Africa.
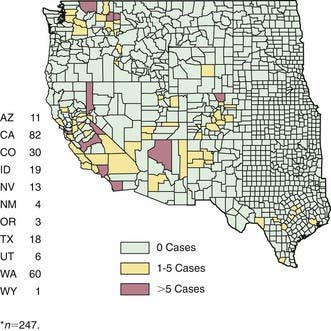
Ornithodoros ticks, which transmit endemic relapsing fever, are distributed worldwide, including the western USA, prefer warm, humid environments and high altitudes and are found in rodent burrows, caves, and other nesting sites (Fig. 213-1). Rodents (e.g., squirrels, chipmunks) are the principal reservoirs. Infected ticks gain access to human dwellings on the rodent host. Human contact is often unnoticed because these soft ticks have a painless bite and detach immediately after a short blood meal.
Pathology and Pathogenesis
Relapsing fever is cyclical because the Borrelia organisms undergo antigenic (phase) variation. Multiple variants evolve simultaneously during the first relapse, with one type becoming predominant. Spirochetes isolated during the primary febrile episode differ antigenically from those recovered during a subsequent relapse. During febrile episodes, spirochetes enter the bloodstream, induce the development of specific immunoglobulin M (IgM) and IgG antibody, and undergo agglutination, immobilization, lysis, and phagocytosis. During remission, Borrelia spirochetes sometimes remain in the bloodstream. The number of relapses in untreated patients depends on the number of antigenic variants of the infecting strain.
Clinical Manifestations
Relapsing fever is characterized by febrile episodes lasting 2-9 days, separated by afebrile intervals of 2-7 days. Louse-borne disease has an incubation period of 2-14 days and has longer periods of pyrexia, fewer relapses, and longer remission periods than tick-borne disease. The incubation period of tick-borne disease is usually 7 days (range, 2-9 days). Each form of relapsing fever is characterized by sudden onset of high fever, lethargy, headache, photophobia, nausea, vomiting, myalgia, and arthralgia. Additional symptoms can appear later and include abdominal pain, a productive cough, mild respiratory distress, and bleeding manifestations, including epistaxis, hemoptysis, hematuria, and hematemesis. During the end of the primary febrile episode, a diffuse, erythematous, macular, or petechial rash lasting up to 2 days can develop over the trunk and shoulders. There may also be lymphadenopathy, pneumonia, and splenomegaly. Hepatic tenderness associated with hepatomegaly is a common sign, with jaundice in half of affected children. Central nervous system manifestations include lethargy, stupor, meningismus, convulsions, peripheral neuritis, focal neurologic deficits, and cranial nerve paralysis and may be the principal feature of late relapses in tick-borne disease. Severe manifestations include myocarditis, hepatic failure, and disseminated intravascular coagulopathy.
The initial symptomatic period characteristically ends with a crisis in 2-9 days, marked by abrupt diaphoresis, hypothermia, hypotension, bradycardia, profound muscle weakness, and prostration. In untreated patients, the first relapse occurs within 1 wk, followed by usually 3 but up to 10 relapses, with symptoms during each relapse becoming milder and shorter as the afebrile remission period lengthens.
Diagnosis
Diagnosis depends on demonstration of spirochetes by dark-field microscopy or in thin or thick blood smears stained with Giemsa or Wright’s stain and by blood culture. During afebrile remissions, spirochetes are not found in the blood. Serologic tests have not been standardized, are generally not available, and produce cross reactions with other spirochetes, including Borrelia burgdorferi, the agent of Lyme disease.
Treatment
Oral or parenteral tetracycline is the drug of choice for louse-borne and tick-borne relapsing fever. For children >8 yr of age and young adults, tetracycline (500 mg PO every 6 hr) or doxycycline (100 mg PO every 12 hr) for 10 days is effective. Single-dose treatment with tetracycline (500 mg PO) or erythromycin is efficacious in adults, but experience in children is limited. In children <8 yr of age, erythromycin (50 mg/kg/day divided every 6 hr PO) for a total of 10 days is recommended. Penicillin and chloramphenicol are also effective.
Resolution of each febrile episode either by natural crisis or as a result of antimicrobial treatment is often accompanied by the Jarisch-Herxheimer reaction, which is due to massive release of antigen. Corticosteroid or antipyretic pretreatment do not prevent the reaction.
Prognosis
With adequate therapy, the mortality rate for relapsing fever is <5%. A majority of patients recover from their illness with or without treatment after the appearance of anti-Borrelia antibodies, which agglutinate, kill, or opsonize the spirochete.
Prevention
No vaccine is available. Disease control requires avoidance or elimination of the arthropod vectors. In epidemics of louse-borne disease, good personal hygiene and delousing of persons, dwellings, and clothing with commercially available insecticides can prevent dissemination. The risk for tick-borne disease can be minimized in endemic areas by maintaining rodent-free dwellings. Giving prophylactic doxycycline for 4 days after a tick bite can prevent tick-borne relapsing fever due to Borrelia persica.
Butler TC. Relapsing fever: new lessons about antibiotic action. Ann Intern Med. 1985;102:397-399.
Centers for Disease Control and Prevention. Tickborne relapsing fever outbreak after a family gathering—New Mexico, August 2002. MMWR Morb Mortal Wkly Rep. 2003;52:809-812.
Dworkin MS, Schwan TG, Anderson DEJr, et al. Tick-borne relapsing fever. Infect Dis Clin North Am. 2008;22:449-468. viii
Fritz CL, Bronson LR, Smith CR, et al. Isolation and characterization of Borrelia hermsii associated with two foci of tick-borne relapsing fever in California. J Clin Microbiol. 2004;42:1123-1128.
Grosskinsky S, Schott M, Brenner C, et al. Borrelia recurrentis employs a novel multifunctional surface protein with anti–complement, anti opsonic and invasive potential to escape innate immunity. PloS One. 2009;4:e4858.
Hasin T, Davidovitch N, Cohen R, et al. Postexposure treatment with doxycycline for the prevention of tick-borne relapsing fever. N Engl J Med. 2006;355:148-154.
Larsson C, Bergstrom S. A novel and simple method for laboratory diagnosis of relapsing fever Borreliosis. Open Microbiol J. 2008;2:10-12.
Schwan TG, Policastro PF, Miller Z, et al. Tick-borne relapsing fever caused by Borrelia hermsii, Montana. Emerg Infect Dis. 2003;9:1151-1154.
Vial L, Diatta G, Tall A, et al. Incidence of tick-borne relapsing fever in west Africa: longitudinal study. Lancet. 2006;368:37-43.