Chapter 240 Mumps
Mumps is an acute self-limited infection, once commonplace but now unusual in developed countries because of widespread use of vaccination. It is characterized by fever, bilateral or unilateral parotid swelling and tenderness, and the frequent occurrence of meningoencephalitis and orchitis. Although no longer common in countries with extensive vaccination programs, mumps remains endemic in the rest of the world, warranting continued vaccine protection.
Etiology
Mumps virus is in the family Paramyxoviridae and the genus Rubulavirus. It is a single-stranded pleomorphic RNA virus encapsulated in a lipoprotein envelope and possessing 7 structural proteins. Two surface glycoproteins, HN (hemagglutinin-neuraminidase) and F (fusion), mediate absorption of the virus to host cells and penetration into cells, respectively. Both of these proteins stimulate production of protective antibodies. Mumps virus exists as a single immunotype, and humans are the only natural host.
Epidemiology
In the prevaccine era, mumps occurred primarily in young children between the ages of 5 and 9 yr and in epidemics about every 4 yr. Mumps infection occurred more often in the winter and spring months. In 1968, just after the introduction of the mumps vaccine, 185,691 cases were reported in the USA. Following the recommendation for routine use of mumps vaccine in 1977, the incidence of mumps in young children fell dramatically (Fig. 240-1), the disease occurring instead in older children, adolescents, and young adults. Outbreaks continued to occur even in highly vaccinated populations as a result of to vaccine failure and also of undervaccination of susceptible persons. After implementation of the 2-dose recommendation for the measles-mumps-rubella (MMR) vaccine for measles control in 1989, the number of mumps cases declined further. During 2001-2003, <300 mumps cases were reported each year. In 2006, the largest mumps epidemic in the last 20 years occurred in the USA. A total of 6584 cases occurred, 85% of them in 8 Midwestern states. Twenty-nine percent of the cases occurred in patients 18-24 yr old, most of whom were attending college. An analysis of 4039 patients with mumps seen in the first 7 months of the epidemic indicated that 63% had received >2 doses of the MMR vaccine.
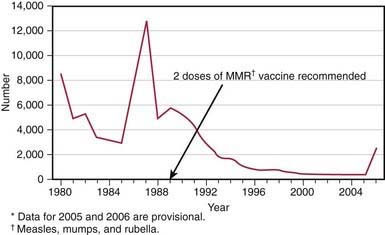
Figure 240-1 Number of reported mumps cases by year in the USA from 1980 to 2006 (data for 2005 and 2006 are provisional). Mumps vaccine was first licensed in 1967 and recommended for routine use in 1977. After expanded recommendation for 2 doses of measles-mumps-rubella (MMR) vaccine in 1989 for measles control, mumps incidence further declined. During 2001–2003 there were <300 mumps cases each year, a 99% decline from the 185,691 cases reported in 1968. More than 2,500 cases were reported in the 1st half of 2006 as part of a multistate outbreak, the largest number of cases in the USA since 1991.
(From the Centers for Disease Control and Prevention: Summary of notifiable diseases—United States, 2004, MMWR Morb Mortal Wkly Rep 53:1–79, 2006.).
Mumps is spread from person to person by respiratory droplets. Virus appears in the saliva from up to 7 days before to as long as 7 days after onset of parotid swelling. The period of maximum infectiousness is 1-2 days before to 5 days after onset of parotid swelling. Viral shedding before onset of symptoms and in asymptomatic infected individuals impairs efforts to contain the infection in susceptible populations. The U.S. Centers for Disease Control and Prevention (CDC), the American Academy of Pediatrics, and the Health Infection Control Practices Advisory Committee recommend an isolation period of 5 days after onset of parotitis for patients with mumps in both community and health care settings.
Pathology and Pathogenesis
Mumps virus targets the salivary glands, central nervous system (CNS), pancreas, testes, and, to a lesser extent, thyroid, ovaries, heart, kidneys, liver, and joint synovia.
Following infection, initial viral replication occurs in the epithelium of the upper respiratory tract. Infection spreads to the adjacent lymph nodes by the lymphatic drainage, and viremia ensues, spreading the virus to targeted tissues. Mumps virus causes necrosis of infected cells and is associated with a lymphocytic inflammatory infiltrate. Salivary gland ducts are lined with necrotic epithelium, and the interstitium is infiltrated with lymphocytes. Swelling of tissue within the testes may result in focal ischemic infarcts. The cerebrospinal fluid (CSF) frequently contains mononuclear pleocytosis, even in individuals without clinical signs of meningitis.
Clinical Manifestations
The incubation period for mumps ranges from 12 to 25 days but is usually 16-18 days. Mumps virus infection may result in clinical presentation ranging from asymptomatic or nonspecific symptoms to the typical illness associated with parotitis with or without complications involving several body systems. The typical patient presents with a prodrome lasting 1-2 days and consisting of fever, headache, vomiting, and achiness. Parotitis then appears and may be unilateral initially but becomes bilateral in about 70% of cases (Fig. 240-2). The parotid gland is tender, and parotitis may be preceded or accompanied by ear pain on the ipsilateral side. Ingestion of sour or acidic foods or liquids may enhance pain in the parotid area. As swelling progresses, the angle of the jaw is obscured and the ear lobe may be lifted upward and outward (Figs. 240-2 and 240-3). The opening of Stensen duct may be red and edematous. The parotid swelling peaks in approximately 3 days, then gradually subsides over 7 days. Fever and the other systemic symptoms resolve in 3-5 days. A morbilliform rash is rarely seen. Submandibular salivary glands may also be involved or may be enlarged without parotid swelling. Edema over the sternum due to lymphatic obstruction may also occur.
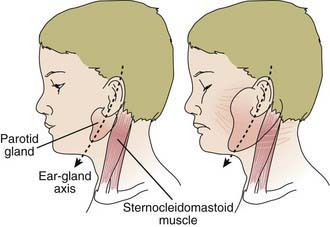
Figure 240-2 Schematic drawing of a parotid gland infected with mumps (right) compared with a normal gland (left). An imaginary line bisecting the long axis of the ear divides the parotid gland into 2 equal parts. These anatomic relationships are not altered in the enlarged gland. An enlarged cervical lymph node is usually posterior to the imaginary line.
(From Mumps [epidemic parotitis]. In Krugman S, Ward R, Katz SL, editors: Infectious diseases in children, ed 6, St Louis, 1977, Mosby, p 182.)

Figure 240-3 A child with mumps showing parotid swelling.
(From the Centers for Disease Control and Prevention: Public health image library [PHIL] [website]. http://phil.cdc.gov/phil/home.asp. Accessed March 8, 2011.)
Diagnosis
When mumps was highly prevalent, the diagnosis could be made on the basis of a history of exposure to mumps infection, an appropriate incubation period, and development of typical clinical findings. Confirmation of the presence of parotitis could be made with demonstration of an elevated serum amylase value. Leukopenia with a relative lymphocytosis was a common finding. Today, in patients with parotitis lasting >2 days and of unknown cause, a specific diagnosis of mumps should be confirmed or ruled out by virologic or serologic means. This step may be accomplished by isolation of the virus in cell culture, detection of viral antigen by direct immunofluorescence, or identification of nucleic acid by reverse transcriptase polymerase chain reaction. Virus can be isolated from upper respiratory tract secretions, CSF, or urine during the acute illness. Serologic testing is usually a more convenient and available mode of diagnosis. A significant increase in serum mumps immunoglobulin G (IgG) antibody between acute and convalescent serum specimens as detected by complement fixation, neutralization hemagglutination, or enzyme immunoassay (EIA) tests establishes the diagnosis. Mumps IgG antibodies may cross react with antibodies to parainfluenza virus in serologic testing. More commonly, an EIA for mumps IgM antibody is used to identify recent infection. Skin testing for mumps is neither sensitive nor specific and should not be used.
Differential Diagnosis
Parotid swelling may be caused by many other infectious and noninfectious conditions. Viruses that have been shown to cause parotitis include parainfluenza 1 and 3 virus, influenza A virus, cytomegalovirus, Epstein-Barr virus, enteroviruses, lymphocytic choriomeningitis virus, and HIV. Purulent parotitis, usually caused by Staphylococcus aureus, is unilateral, is extremely tender, is associated with an elevated white blood cell count, and may involve purulent drainage from Stensen duct. Submandibular or anterior cervical adenitis due to a variety of pathogens may also be confused with parotitis. Other noninfectious causes of parotid swelling include obstruction of Stensen duct, collagen vascular diseases such as Sjögren syndrome, systemic lupus erythematosus, and tumor.
Complications
The most common complications of mumps are meningitis, with or without encephalitis, and gonadal involvement. Uncommon complications include conjunctivitis, optic neuritis, pneumonia, nephritis, pancreatitis, and thrombocytopenia.
Maternal infection with mumps during the 1st trimester of pregnancy results in increased fetal wastage. No fetal malformations have been associated with intrauterine mumps infection. However, perinatal mumps disease has been reported in infants born to mothers who acquired mumps late in gestation.
Meningitis and Meningoencephalitis
Mumps virus is neurotropic and is thought to enter the CNS via the choroid plexus and infect the choroidal epithelium and ependymal cells, both of which can be found in CSF along with mononuclear leukocytes. Symptomatic CNS involvement occurs in 10-30% of infected individuals, but CSF pleocytosis has been found in 40-60% of patients with mumps parotitis. The meningoencephalitis may occur before, along with, or following the parotitis. It most commonly manifests 5 days after the parotitis. Clinical findings vary with age. Infants and young children have fever, malaise, and lethargy, whereas older children, adolescents, and adults complain of headache and demonstrate meningeal signs. In 1 series of children with mumps and meningeal involvement, findings were fever in 94%, vomiting in 84%, headache in 47%, parotitis in 47%, neck stiffness in 71%, lethargy in 69%, and seizures in 18%. In typical cases, symptoms resolve in 7-10 days. CSF in mumps meningitis has a white blood cell pleocytosis of 200-600/mm3 with a predominance of lymphocytes. The CSF glucose content is normal in most patients, but a moderate hypoglycorrhachia (glucose content 20-40 mg/dL) may be seen in 10-20% of patients. The CSF protein content is normal or mildly elevated.
Less common CNS complications of mumps include transverse myelitis, aqueductal stenosis, and facial palsy. Sensorineural hearing loss is rare but has been estimated to occur in 0.5-5.0/100,000 cases of mumps. There is some evidence that this sequela is more likely in patients with meningoencephalitis.
Orchitis and Oophoritis
In adolescent and adult males, orchitis is 2nd only to parotitis as a common finding in mumps. Involvement in prepubescent boys is extremely rare, but after puberty, orchitis occurs in 30-40% of males. It begins within days following onset of parotitis in the majority of cases and is associated with moderate to high fever, chills, and exquisite pain and swelling of the testes. In ≤30% of cases the orchitis is bilateral. Atrophy of the testes may occur, but sterility is rare even with bilateral involvement.
Oophoritis is uncommon in postpubertal females but may cause severe pain and may be confused with appendicitis when located on the right side.
Pancreatitis
Pancreatitis may occur in mumps with or without parotid involvement. Severe disease is rare, but fever, epigastric pain, and vomiting are suggestive. Epidemiologic studies have suggested that mumps may be associated with the subsequent development of diabetes mellitus, but a causal link has not been established.
Cardiac Involvement
Myocarditis has been reported in mumps, and molecular studies have identified mumps virus in heart tissue taken from patients with endocardial fibroelastosis.
Treatment
No specific antiviral therapy is available for mumps. Management should be aimed at reducing the pain associated with meningitis or orchitis and maintaining adequate hydration. Antipyretics may be given for fever.
Prognosis
The outcome of mumps is nearly always excellent, even when the disease is complicated by encephalitis, although fatal cases due to CNS involvement or myocarditis have been reported.
Prevention
Immunization with the live mumps vaccine is the primary mode of prevention used in the USA. It is given as part of the MMR 2-dose vaccine schedule, at 12-15 mo of age for the 1st dose and 4-6 yr of age for the 2nd dose. If not given at 4-6 yr, the 2nd dose should be given before children enter puberty. Antibody develops in 95% of vaccinees after 1 dose. One study showed vaccine effectiveness of 88% for 2 doses of MMR vaccine, compared with 64% for a single dose. Immunity appears to be long lasting. However, studies from the United Kingdom and the recent epidemic in the USA suggest that both antibody levels and vaccine effectiveness may decline, contributing to mumps outbreaks in older vaccinated populations.
As a live-virus vaccine, MMR should not be administered to pregnant women or to severely immunodeficient or immunosuppressed individuals. HIV-infected patients who are not severely immunocompromised may receive the vaccine, because the risk for severe infection with mumps outweighs the risk for serious reaction to the vaccine. Individuals with anaphylactoid reactions to egg or neomycin may be at risk for immediate-type hypersensitivity reactions to the vaccine. Persons with other types of reactions to egg or reactions to other components of the vaccine are not restricted from receiving the vaccine.
In 2006, in response to the multistate outbreak in the USA, evidence of immunity to mumps through vaccination was redefined. Acceptable presumptive evidence of immunity to mumps now consists of 1 of the following: (1) documentation of adequate vaccination, (2) laboratory evidence of immunity, (3) birth before 1957, and (4) documentation of physician-diagnosed mumps. Evidence of immunity through documentation of adequate vaccination is now defined as 1 dose of a live mumps virus vaccine for preschool-aged children and adults not at high risk and 2 doses for school-aged children (i.e., grades K-12) and for adults at high risk (i.e., health care workers, international travelers, and students at post–high school educational institutions).
All persons who work in health care facilities should be immune to mumps. Adequate mumps vaccination for health care workers born during or after 1957 consists of 2 doses of a live mumps virus vaccine. Health care workers with no history of mumps vaccination and no other evidence of immunity should receive 2 doses, with >28 days between doses. Health care workers who have received only 1 dose previously should receive a 2nd dose. Because birth before 1957 is only presumptive evidence of immunity, health care facilities should consider recommending 1 dose of a live mumps virus vaccine for unvaccinated workers born before 1957 who do not have a history of physician-diagnosed mumps or laboratory evidence of mumps immunity. During an outbreak, health care facilities should strongly consider recommending 2 doses of a live mumps virus vaccine to unvaccinated workers born before 1957 who do not have evidence of mumps immunity.
Adverse reactions to mumps virus vaccine are rare. Parotitis and orchitis have been reported rarely. Other reactions such as febrile seizures, deafness, rash, purpura, encephalitis, and meningitis may not be causally related to the strain of mumps vaccine virus used for immunization in the USA. Higher rates of aseptic meningitis following vaccination for mumps have been associated with vaccine strains used elsewhere in the world, including the Leningrad 3 and Urabe Am 9 strains. Transient suppression of reactivity to tuberculin skin testing has been reported after mumps vaccination.
Azimi PH, Cramblett HG, Haynes RE. Mumps meningoencephalitis in children. JAMA. 1969;207:509-512.
Centers for Disease Control and Prevention. Update: mumps outbreak—New York and New Jersey, June 2009–January 2010. MMWR Morb Mortal Wkly Rep. 2010;59:125-128.
Centers for Disease Control and Prevention. Mumps epidemic—United Kingdom, 2004–2005. MMWR Morb Mortal Wkly Rep. 2006;55:173-178.
Centers for Disease Control and Prevention. Mumps epidemic—Iowa, 2006. MMWR Morb Mortal Wkly Rep. 2006;55:366-368.
Centers for Disease Control and Prevention. Update: multistate outbreak of mumps—United States, January 1–May 2, 2006. MMWR Morb Mortal Wkly Rep. 2006;55:559-564.
Centers for Disease Control and Prevention. Notice to readers: updated recommendations of the Advisory Committee on Immunization Practices (ACIP) for the control and elimination of mumps. MMWR Morb Mortal Wkly Rep. 2006;55:629-630.
Centers for Disease Control and Prevention. Updated recommendations for isolation of patients with mumps. MMWR Morb Mortal Wkly Rep. 2008;57:1103-1105.
Cohen C, White JM, Glynn JR, et al. Vaccine effectiveness estimates 2004–2005 mumps outbreak, England. Emerg Infect Dis. 2007;13:12-17.
Davidkin I, Jakinen S, Paananen A, et al. Etiology of mumps-like illness in children and adolescents vaccinated for measles, mumps and rubella. J Infect Dis. 2005;1991:719-723.
Dayan GH, Quinlisk MP, Parker AA, et al. Recent resurgence of mumps in the United States. N Engl J Med. 2008;358:1580-1589.
Endo A, Izuni H, Miyashita M, et al. Facial palsy associated with mumps parotitis. Pediatr Infect Dis J. 2001;20:815-816.
Harling R, White JM, Ramsay ME, et al. The effectiveness of the mumps component of the MMR vaccine: a case control study. Vaccine. 2005;23:4070-4074.
Horel L, Amir J, Reish O, et al. Mumps arthritis in children. Pediatr Infect Dis J. 1990;9:928-929.
Kanra G, Kara A, Cengiz AB, et al. Mumps meningoencephalitis effect on hearing. Pediatr Infect Dis J. 2002;21:1167-1169.
Kupers TA, Petrich JM, Holloway AW, et al. Depression of tuberculin hypersensitivity by live attenuated mumps virus. J Pediatr. 1970;76:716-721.
Rubin SA, Li Q, Audet SA, et al. Antibody induced by immunization with the Jeryl Lynn mumps vaccine strain effectively neutralizes a heterologous wild-type mumps virus associated with a large outbreak. J Infect Dis. 2008;198:508-515.
Ternavasio-de la Vega HG, Boronat M, Ojeda A, et al. Mumps orchitis in the post-vaccine era (1967–2009). Medicine. 2010;89:96-116.
Thompson JA. Mumps: a cause of aqueductal stenosis. J Pediatr. 1979;94:923-924.