Chapter 243 Parvovirus B19
Parvovirus B19 is the cause of erythema infectiosum or fifth disease.
Etiology
Parvovirus B19 (B19) is a member of the genus Erythrovirus in the family Parvoviridae. Parvoviruses are small DNA viruses that infect a variety of animal species. As a group, parvoviruses include a number of important animal pathogens, such as canine parvovirus and feline panleukopenia virus; B19 does not infect other animals, and animal parvoviruses do not infect humans. B19 is one of only two parvoviruses that are pathogenic in humans. The other such virus is the newly described human bocavirus. Although the clinical significance of human bocavirus is not yet fully defined, this virus may be associated with upper and lower respiratory tract infection in young children and will not be further discussed in this chapter.
B19 is composed of an icosahedral protein capsid without an envelope and contains a single-stranded DNA genome of approximately 5.5 kb. It is relatively heat and solvent resistant. It is antigenically distinct from other mammalian parvoviruses and has only one known serotype. Parvoviruses replicate in mitotically active cells and require host cell factors present in late S phase to replicate. B19 can be propagated in vitro only in erythropoietin-stimulated erythropoietic cells derived from human bone marrow, umbilical cord blood, or primary fetal liver culture.
Epidemiology
Infections with parvovirus B19 are common and occur worldwide. Clinically apparent infections, such as the rash illness of erythema infectiosum and transient aplastic crisis, are most prevalent in school-aged children, 70% of cases occurring in patients between 5 and 15 yr of age. Seasonal peaks occur in the late winter and spring, with sporadic infections throughout the year. Seroprevalence increases with age, 40-60% of adults having evidence of prior infection.
Transmission of B19 is by the respiratory route, presumably via large droplet spread from nasopharyngeal viral shedding. The transmission rate is 15-30% among susceptible household contacts, and mothers are more commonly infected than fathers. In outbreaks of erythema infectiosum in elementary schools, the secondary attack rates range from 10% to 60%. Nosocomial outbreaks also occur, with secondary attack rates of 30% among susceptible health care workers.
Although respiratory spread is the primary mode of transmission, B19 is also transmissible in blood and blood products, as documented among children with hemophilia receiving pooled-donor clotting factor. Given the resistance of the virus to solvents, fomite transmission could be important in child-care centers and other group settings, but this mode of transmission has not been established.
Pathogenesis
The primary target of B19 infection is the erythroid cell line, specifically erythroid precursors near the pronormoblast stage. Viral infection produces cell lysis leading to a progressive depletion of erythroid precursors and a transient arrest of erythropoiesis. The virus has no apparent effect on the myeloid cell line. The tropism for erythroid cells is related to the erythrocyte P blood group antigen, which is the primary cell receptor for the virus and is also found on endothelial cells, placental cells, and fetal myocardial cells. Thrombocytopenia and neutropenia are often observed clinically, but the pathogenesis of these abnormalities is unexplained.
Experimental infection of normal volunteers with B19 revealed a biphasic illness. From 7 to 11 days after inoculation, subjects had viremia and nasopharyngeal viral shedding with fever, malaise, and rhinorrhea. Reticulocyte counts dropped to undetectable levels but resulted in only a mild, clinically insignificant fall in serum hemoglobin. With the appearance of specific antibodies, symptoms resolved and serum hemoglobin returned to normal. Several subjects experienced a rash associated with arthralgia 17-18 days after inoculation. Some manifestations of B19 infection, such as transient aplastic crisis, appear to be a direct result of viral infection, whereas others, including the exanthem and arthritis, appear to be postinfectious phenomena related to the immune response. Skin biopsy of patients with erythema infectiosum reveals edema in the epidermis and a perivascular mononuclear infiltrate compatible with an immune-mediated process.
Individuals with chronic hemolytic anemia and increased red blood cell (RBC) turnover are very sensitive to minor perturbations in erythropoiesis. Infection with B19 leads to a transient arrest in RBC production and a precipitous fall in serum hemoglobin, often requiring transfusion. The reticulocyte count drops to undetectable levels, reflecting the lysis of infected erythroid precursors. Humoral immunity is crucial in controlling infection. Specific immunoglobulin M (IgM) appears within 1-2 days of infection and is followed by anti-B19 IgG, which leads to control of the infection, restoration of reticulocytosis, and a rise in serum hemoglobin.
Individuals with impaired humoral immunity are at increased risk for more serious or persistent infection with B19, which usually manifests as chronic RBC aplasia, although neutropenia, thrombocytopenia, and marrow failure are also described. Children undergoing chemotherapy for leukemia or other forms of cancer, transplant recipients, and patients with congenital or acquired immunodeficiency states (including AIDS) are at risk for chronic B19 infections.
Infections in the fetus and neonate are somewhat analogous to infections in immunocompromised persons. B19 is associated with nonimmune fetal hydrops and stillbirth in women experiencing a primary infection but does not appear to be teratogenic. Like most mammalian parvoviruses, B19 can cross the placenta and cause fetal infection during primary maternal infection. Parvovirus cytopathic effects are seen primarily in erythroblasts of the bone marrow and sites of extramedullary hematopoiesis in the liver and spleen. Fetal infection can presumably occur as early as 6 wk of gestation, when erythroblasts are first found in the fetal liver; after the 4th mo of gestation, hematopoiesis switches to the bone marrow. In some cases, fetal infection leads to profound fetal anemia and subsequent high-output cardiac failure (Chapter 97). Fetal hydrops ensues and is often associated with fetal death. There may also be a direct effect of the virus on myocardial tissue that contributes to the cardiac failure. However, most infections during pregnancy result in normal deliveries at term. Some of the asymptomatic infants from these deliveries have been reported to have chronic postnatal infection with B19 that is of unknown significance.
Clinical Manifestations
Many infections are clinically inapparent. Infected children characteristically demonstrate the rash illness of erythema infectiosum. Adults, especially women, frequently experience acute polyarthropathy with or without a rash.
Erythema Infectiosum (Fifth Disease)
The most common manifestation of parvovirus B19 is erythema infectiosum, also known as fifth disease, which is a benign, self-limited exanthematous illness of childhood.
The incubation period for erythema infectiosum is 4-28 days (average 16-17 days). The prodromal phase is mild and consists of low-grade fever in 15-30% of cases, headache, and symptoms of mild upper respiratory tract infection. The hallmark of erythema infectiosum is the characteristic rash, which occurs in 3 stages that are not always distinguishable. The initial stage is an erythematous facial flushing, often described as a “slapped-cheek” appearance (Fig. 243-1). The rash spreads rapidly or concurrently to the trunk and proximal extremities as a diffuse macular erythema in the 2nd stage. Central clearing of macular lesions occurs promptly, giving the rash a lacy, reticulated appearance (Fig. 243-2). The rash tends to be more prominent on extensor surfaces, sparing the palms and soles. Affected children are afebrile and do not appear ill. Some have petechiae. Older children and adults often complain of mild pruritus. The rash resolves spontaneously without desquamation but tends to wax and wane over 1-3 wk. It can recur with exposure to sunlight, heat, exercise, and stress. Lymphadenopathy and atypical papular, purpuric, vesicular rashes are also described.


Arthropathy
Arthritis and arthralgia may occur in isolation or with other symptoms. Joint symptoms are much more common among adults and older adolescents with B19 infection. Females are affected more frequently than males. In one large outbreak of fifth disease, 60% of adults and 80% of adult women reported joint symptoms. Joint symptoms range from diffuse polyarthralgia with morning stiffness to frank arthritis. The joints most often affected are the hands, wrists, knees, and ankles, but practically any joint may be affected. The joint symptoms are self-limited and, in the majority of patients, resolve within 2-4 wk. Some patients may have a prolonged course of many months, suggesting rheumatoid arthritis. Transient rheumatoid factor positivity is reported in some of these patients but with no joint destruction.
Transient Aplastic Crisis
The transient arrest of erythropoiesis and absolute reticulocytopenia induced by B19 infection leads to a sudden fall in serum hemoglobin in individuals with chronic hemolytic conditions. This B19-induced RBC aplasia or transient aplastic crisis occurs in patients with all types of chronic hemolysis and/or rapid RBC turnover, including sickle cell disease, thalassemia, hereditary spherocytosis, and pyruvate kinase deficiency. In contrast to children with erythema infectiosum only, patients with aplastic crisis are ill with fever, malaise, and lethargy and have signs and symptoms of profound anemia, including pallor, tachycardia, and tachypnea. Rash is rarely present. The incubation period for transient aplastic crisis is shorter than that for erythema infectiosum because the crisis occurs coincident with the viremia. Children with sickle cell hemoglobinopathies may also have a concurrent vasoocclusive pain crisis, further confusing the clinical presentation.
Immunocompromised Persons
Persons with impaired humoral immunity are at risk for chronic parvovirus B19 infection. Chronic anemia is the most common manifestation, sometimes accompanied by neutropenia, thrombocytopenia, or complete marrow suppression. Chronic infections occur in persons receiving cancer chemotherapy or immunosuppressive therapy for transplantation and persons with congenital immunodeficiencies, AIDS, and functional defects in IgG production who are thereby unable to generate neutralizing antibodies.
Fetal Infection
Primary maternal infection is associated with nonimmune fetal hydrops and intrauterine fetal demise, with the risk for fetal loss after infection estimated at <5%. The mechanism of fetal disease appears to be a viral-induced RBC aplasia at a time when the fetal erythroid fraction is rapidly expanding, leading to profound anemia, high-output cardiac failure, and fetal hydrops. Viral DNA has been detected in infected abortuses. The second trimester seems to be the most sensitive period, but fetal losses are reported at every stage of gestation. If maternal B19 infection is suspected, fetal ultrasonography and measurement of the peak systolic flow velocity of the middle cerebral artery are sensitive, noninvasive procedures to diagnose fetal anemia and hydrops. Most infants infected in utero are born normally at term, including some who have had ultrasonographic evidence of hydrops. A small subset of infants infected in utero may acquire a chronic or persistent postnatal infection with B19 that is of unknown significance. Congenital anemia associated with intrauterine B19 infection has been reported in a few cases, sometimes following intrauterine hydrops. This process may mimic other forms of congenital hypoplastic anemia (e.g., Diamond-Blackfan syndrome). Fetal infection with B19 has not been associated with other birth defects. B19 is only one of many causes of hydrops fetalis (Chapter 97.2).
Myocarditis
B19 infection has been associated with myocarditis in fetuses, infants, children, and a few adults. Diagnosis has often been based on serologic findings suggestive of a concurrent B19 infection, but in many cases B19 DNA has been demonstrated in cardiac tissue. B19-related myocarditis is plausible because fetal myocardial cells are known to express P antigen, the cell receptor for the virus. In the few cases in which histology is reported, a predominantly lymphocytic infiltrate is described. Outcomes have varied from complete recovery to chronic cardiomyopathy to fatal cardiac arrest. Although B19-associated myocarditis seems to be a rare occurrence, there appears to be enough evidence to consider B19 as a potential cause of lymphocytic myocarditis, especially in infants and immunocompromised persons.
Other Cutaneous Manifestations
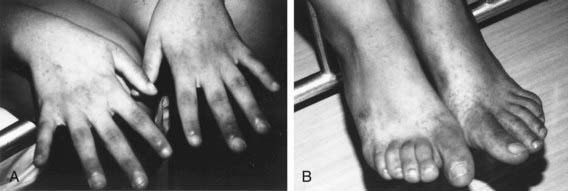
A variety of atypical skin eruptions have been reported with B19 infection. Most of these are petechial or purpuric in nature, often with evidence of vasculitis on biopsy. Among these rashes, the papular-purpuric “gloves and socks” syndrome (PPGSS) is well established in the dermatologic literature as distinctly associated with B19 infection (Fig. 243-3). PPGSS is characterized by fever, pruritus, and painful edema and erythema localized to the distal extremities in a distinct “gloves and socks” distribution, followed by acral petechiae and oral lesions. The syndrome is self-limited and resolves within a few weeks. Although PPGSS was initially described in young adults, a number of reports of the disease in children have since been published. In those cases linked to B19 infection, the eruption is accompanied by serologic evidence of acute infection.
Diagnosis
The diagnosis of erythema infectiosum is usually based on clinical presentation of the typical rash and rarely requires virologic confirmation. Similarly, the diagnosis of a typical transient aplastic crisis in a child with sickle cell disease is generally made on clinical grounds without specific virologic testing.
Serologic tests for the diagnosis of B19 infection are available. B19-specific IgM develops rapidly after infection and persists for 6-8 weeks. Anti-B19 IgG serves as a marker of past infection or immunity. Determination of anti-B19 IgM is the best marker of recent/acute infection on a single serum sample; seroconversion of anti-B19 IgG antibodies in paired sera can also be used to confirm recent infection. Demonstration of anti-B19 IgG in the absence of IgM, even in high titer, is not diagnostic of recent infection.
Serologic diagnosis is unreliable in immunocompromised persons; diagnosis in these patients requires methods to detect viral DNA. Because the virus cannot be isolated by standard cell culture, methods to detect viral particles or viral DNA, such as polymerase chain reaction and nucleic acid hybridization, are necessary to establish the diagnosis. These tests are not widely available outside of research centers or reference laboratories. Prenatal diagnosis of B19-induced fetal hydrops can be accomplished by detection of viral DNA in fetal blood or amniotic fluid by these methods.
Differential Diagnosis
The rash of erythema infectiosum must be differentiated from rubella, measles, enteroviral infections, and drug reactions. Rash and arthritis in older children should prompt consideration of juvenile rheumatoid arthritis, systemic lupus erythematosus, serum sickness, and other connective tissue disorders.
Treatment
There is no specific antiviral therapy for B19 infection. Commercial lots of intravenous immune globulin (IVIG) have been used with some success to treat B19-related episodes of anemia and bone marrow failure in immunocompromised children. Specific antibody may facilitate clearance of the virus; it is not always necessary, however, because cessation of cytotoxic chemotherapy with subsequent restoration of immune function often suffices. In patients whose immune status is not likely to improve, such as patients with AIDS, administration of IVIG may give only a temporary remission, and periodic re-infusions may be required. In patients with AIDS, clearance of B19 infection has been reported after initiation of highly active antiretroviral therapy (HAART) without the use of IVIG.
No controlled studies have been published regarding dosing of IVIG for B19-induced RBC aplasia. Doses reported with good results in a limited number of cases include 200 mg/kg/day for 5-10 days and 1g/kg/day for 3 days. IVIG should not be used for treatment of B19-induced arthropathy.
B19-infected fetuses with anemia and hydrops have been managed successfully with intrauterine RBC transfusions, but this procedure has significant attendant risks. Once fetal hydrops is diagnosed, regardless of the suspected cause, the mother should be referred to a fetal therapy center for further evaluation because of the high risk for serious complications (Chapter 97.2).
Complications
Erythema infectiosum is often accompanied by arthralgias or arthritis in adolescents and adults that may persist after resolution of the rash. B19 may rarely cause thrombocytopenic purpura. Neurologic conditions, including aseptic meningitis, encephalitis, and peripheral neuropathy, have been reported in both immunocompromised and healthy individuals in association with B19 infection. The incidence of stroke may be increased in children with sickle cell disease following B19-induced transient aplastic crisis. B19 is also a cause of infection-associated hemophagocytic syndrome, usually in immunocompromised persons.
Prevention
Children with erythema infectiosum are not likely to be infectious at presentation because the rash and arthropathy represent immune-mediated, postinfectious phenomena. Isolation and exclusion from school or child care are unnecessary and ineffective after diagnosis.
Children with B19-induced RBC aplasia, including the transient aplastic crisis, are infectious upon presentation and demonstrate a more intense viremia. Most of these children require transfusions and supportive care until their hematologic status stabilizes. They should be isolated in the hospital to prevent spread to susceptible patients and staff. Isolation should continue for at least 1 wk and until after resolution of fever. Pregnant caregivers should not be assigned to these patients. Exclusion of pregnant women from workplaces where children with erythema infectiosum may be present (e.g., primary and secondary schools) is not recommended as a general policy because it is unlikely to reduce their risk. There are no data to support the use of IVIG for postexposure prophylaxis in pregnant caregivers or immunocompromised children. No vaccine is currently available.
Douvoyiannis M, Litman N, Goldman DL. Neurologic manifestations associated with parvovirus B19 infection. Clin Infect Dis. 2009;48:1713-1723.
Heegaard ED, Brown KE. Human parvovirus B19. Clin Microbiol Rev. 2002;15:485-505.
Khan J. Human bocavirus: clinical significance and implications. Curr Opin Pediatr. 2008;20:62-66.
Lindblom A, Heyman M, Gustafsson I, et al. Parvovirus B19 infection in children with acute lymphoblastic leukemia is associated with cytopenia resulting in prolonged interruptions of chemotherapy. Clin Infect Dis. 2008;46:528-536.
Messina MF, Ruggeri C, Rosana M, et al. Purpuric gloves and socks syndrome caused by parvovirus B19 infection. Pediatr Infect Dis J. 2003;22:755-756.
Nigro G, Bastianon V, Colloridi V, et al. Human parvovirus B19 infection in infancy associated with acute and chronic lymphocytic myocarditis and high cytokine levels: report of 3 cases and review. Clin Infect Dis. 2000;31:65-69.
Ramirez MM, Mastrobattista JM. Diagnosis and management of human parvovirus B19 infection. Clin Perinatol. 2005;32:697-704.
Smith SB, Libow LF, Elston DM, et al. Gloves and socks syndrome: early and late histopathologic features. J Am Acad Dermatol. 2002;47:749-754.
Smith-Whitley K, Zhao H, Hodinka RL, et al. Epidemiology of human parvovirus B19 in children with sickle cell disease. Blood. 2004;103:422-427.
Young NS, Brown KE. Parvovirus B19. N Engl J Med. 2004;350:586-597.