Chapter 301 Malocclusion
The oral cavity is essentially a masticatory instrument. The purpose of the anterior teeth is to bite off portions of large amounts of food. The posterior teeth reduce foodstuff to a soft, moist bolus. The cheeks and tongue force the food onto the areas of tooth contact. Establishing a proper relationship between the mandibular and maxillary teeth is important for physiologic and cosmetic reasons.
Variations in Growth Patterns
Growth patterns are classified into 3 main types of occlusion, determined when the jaws are closed and the teeth are held together (Fig. 301-1). According to the Angle Classification of Malocclusion, in class I occlusion (normal), the cusps of the posterior mandibular teeth interdigitate ahead of and inside the corresponding cusps of the opposing maxillary teeth. This relationship provides a normal facial profile.
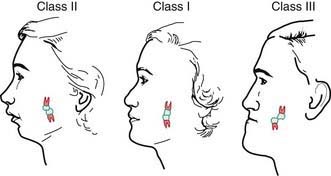
Figure 301-1 Angle classification of occlusion. The typical correspondence between the facial-jaw profile and molar relationship is shown.
In class II malocclusion, “buck teeth,” the cusps of the posterior mandibular teeth are behind and inside the corresponding cusps of the maxillary teeth. This common occlusal disharmony is found in ∼45% of the population. The facial profile can give the appearance of a “receding chin” (retrognathia) or protruding front teeth. The resultant increased space between upper and lower anterior teeth encourage finger sucking and tongue-thrust habits. Additionally, children with pronounced class II malocclusions are at greater risks of damage to the incisors due to trauma.
In class III malocclusion, “underbite,” the cusps of the posterior mandibular teeth interdigitate a tooth or more ahead of their opposing maxillary counterparts. The anterior teeth appear in cross bite with the mandibular incisors protruding beyond the maxillary incisors. The facial profile gives the appearance of a “protruding chin” (prognathia).
Cross Bite
Normally, the mandibular teeth are in a position just inside the maxillary teeth, so that the outside mandibular cusps or incisal edges meet the central portion of the opposing maxillary teeth. A reversal of this relation is referred to as a cross bite. Cross bites can be anterior, involving the incisors; can be posterior, involving the molars; or can involve single or multiple teeth.
Open and Closed Bites
If the posterior mandibular and maxillary teeth make contact with each other, but the anterior teeth are still apart, the condition is called an open bite. Open bites can result from skeletal growth pattern or digit sucking. If digit sucking is terminated before skeletal and dental growth is complete, the open bite might resolve naturally. If mandibular anterior teeth occlude inside the maxillary anterior teeth in an overclosed position, the condition is referred to as a closed or deep bite.
Treatment of open and closed bites consists of orthodontic correction, generally performed in the preteen or teenage years. Some cases require orthognathic surgery to position the jaws optimally in a vertical direction.
Dental Crowding
Overlap of incisors can result when the jaws are too small or the teeth are too large for adequate alignment of the teeth. Growth of the jaws is mostly in the posterior aspects of the mandible and maxilla, and therefore inadequate space for the teeth at 7 or 8 yr of age will not resolve with growth of the jaws. Spacing in the primary dentition is normal and favorable for adequate alignment of successor teeth.
Digit Sucking
Various and conflicting etiologic theories and recommendations for correction have been proposed for digit sucking in children. Prolonged digit sucking can cause flaring of the maxillary incisor teeth, an open bite, and a posterior cross bite. The prevalence of digit sucking decreases steadily from the age of 2 yr to ≈10% by the age of 5 yr. The earlier the habit is discontinued after the eruption of the permanent maxillary incisors (age 7-8 yr), the greater the likelihood that there will be lessening effects on the dentition.
A variety of treatments have been suggested, from behavioral modification to insertion of an appliance with extensions that serves as a reminder when the child attempts to insert the digit. The greatest likelihood of success occurs in cases in which the child desires to stop. Stopping of the habit will not rectify a malocclusion caused by a prior deviant growth pattern.