Chapter 306 Dental Trauma
Traumatic oral injuries may be categorized into three groups: injuries to teeth, injuries to soft tissue (contusions, abrasions, lacerations, punctures, avulsions, and burns), and injuries to jaw (mandibular and/or maxillary fractures).
Injuries to Teeth
Approximately 10% of children between 18 mo and 18 yr of age sustain significant tooth trauma. There appear to be 3 age periods of greatest predilection: toddlers (1-3 yr), usually due to falls or child abuse; school-aged children (7-10 yr), usually from bicycle and playground accidents; and adolescents (16-18 yr), often the result of fights, athletic injuries, and automobile accidents. Injuries to teeth are more common among children with protruding front teeth. Children with craniofacial abnormalities or neuromuscular deficits are also at increased risk for dental injury. Injuries to teeth can involve the hard dental tissues, the dental pulp (nerve), and injuries to the periodontal structure (surrounding bone and attachment apparatus) (Fig. 306-1 and Table 306-1).
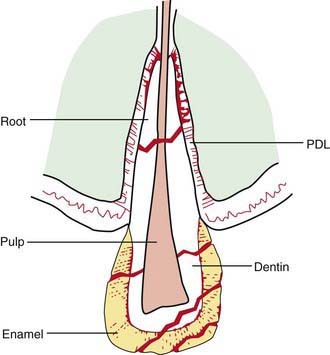
Figure 306-1 Tooth fractures can involve enamel, dentin, or pulp and can occur in the crown or root of a tooth. PDL, periodontal ligament.
(From Pinkham JR: Pediatric dentistry: infancy through adolescence, Philadelphia, 1988, WB Saunders, p 172.)
Table 306-1 INJURIES TO CROWNS OF TEETH
| TYPE OF TRAUMA | DESCRIPTION | TREATMENT AND REFERRAL |
|---|---|---|
| Enamel infraction (crazing) | Incomplete fracture of enamel without loss of tooth structure | Initially might not require therapy but should be assessed periodically by dentist |
| Enamel fractures | Fracture of only the tooth enamel | Tooth may be smoothed or treated to replace fragment |
| Enamel and dentin fracture | Fracture of enamel and dentinal layer of the tooth. Tooth may be sensitive to cold or air. Pulp may become necrotic, leading to periapical abscess. | Refer as soon as possible. Area should be treated to preserve the integrity of the underlying pulp. |
| Enamel, dentin fracture involving the pulp | Bacterial contamination can lead to pulpal necrosis and periapical abscess. The tooth might have the appearance of bleeding or might display a small red spot. | Refer immediately. The dental therapy of choice depends on the extent of injury, the condition of the pulp, the development of the tooth, time elapsed from injury, and any other injuries to the supporting structures. Therapy is directed toward minimizing contamination in an effort to improve the prognosis. |
From Josell SD, Abrams RG: Managing common dental problems and emergencies, Pediatr Clin North Am 38:1325–1342, 1991.
Fractures of teeth may be uncomplicated (confined to the hard dental tissues) or complicated (involving the pulp). Exposure of the pulp results in its bacterial contamination, which can lead to infection and pulp necrosis. Such pulp exposure complicates therapy and can lower the likelihood of a favorable outcome.
The teeth most often affected are the maxillary incisors. Uncomplicated crown fractures are treated by covering exposed dentin and by placing an aesthetic restoration. Complicated crown fractures usually require endodontic therapy (root canal). Crown-root fractures and root fractures usually require extensive dental therapy. Such injuries in the primary dentition can interfere with normal development of the permanent dentition, and therefore, significant injuries of the primary incisor teeth are usually managed by extraction.
Traumatic oral injuries should be referred to a dentist as soon as possible. Even when the teeth appear intact, a dentist should promptly evaluate the patient. Baseline data (radiographs, mobility patterns, responses to specific stimuli) enable the dentist to assess the likelihood of future complications.
Injuries to Periodontal Structures
Trauma to teeth with associated injury to periodontal structures that hold the teeth usually manifests as mobile or displaced teeth. Such injuries are more common in the primary than in the permanent dentition. Categories of trauma to the periodontium include concussion, subluxation, intrusive luxation, extrusive luxation, and avulsion.
Concussion
Injuries that produce minor damage to the periodontal ligament are termed concussions. Teeth sustaining such injuries are not mobile or displaced but react markedly to percussion (gentle hitting of the tooth with an instrument). This type of injury usually requires no therapy and resolves without complication. Primary incisors that sustain concussion can change color, indicating pulpal degeneration, and should be evaluated by a dentist.
Subluxation
Subluxated teeth exhibit mild to moderate horizontal mobility and/or vertical mobility. Hemorrhage is usually evident around the neck of the tooth at the gingival margin. There is no displacement of the tooth. Many subluxated teeth need to be immobilized by splints to ensure adequate repair of the periodontal ligament. Some of these teeth develop pulp necrosis.
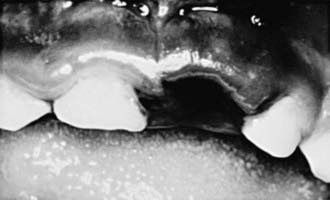
Intrusion
Intruded teeth are pushed up into their socket, sometimes to the point where they are not clinically visible. Intruded primary incisors can give the false appearance of being avulsed (knocked out). To rule out avulsion, a dental radiograph is indicated (Figs. 306-2 and 306-3).

Extrusion
Extrusion injury is characterized by displacement of the tooth from its socket. The tooth is usually displaced to the lingual (tongue) side, with fracture of the wall of the alveolar socket. These teeth need immediate treatment; the longer the delay, the more likely the tooth will be fixed in its displaced position. Therapy is directed at reduction (repositioning the tooth) and fixation (splinting). The pulp of such teeth often becomes necrotic and requires endodontic therapy. Extrusive luxation in the primary dentition is usually managed by extraction because complications of reduction and fixation can result in problems with development of permanent teeth.
Avulsion
If avulsed permanent teeth are replanted within 20 min after injury, good success may be achieved; if the delay exceeds 2 hr, however, failure (root resorption, ankylosis) is common. The likelihood that normal reattachment will follow replantation of the tooth is related to the viability of the periodontal ligament. Parents confronted with this emergency situation can be instructed to do the following:
After the tooth is replanted, it must be immobilized to facilitate reattachment; endodontic therapy is always required. The initial signs of complications associated with replantation can appear as early as 1 wk after trauma or as late as several years later. Close dental follow-up is indicated for at least 1 yr.
Prevention
To minimize the likelihood of dental injuries:
Additional Considerations
Children who experience dental trauma might also have sustained head or neck trauma, and therefore neurologic assessment is warranted. Tetanus prophylaxis should be considered with any injury that disrupts the integrity of the oral tissues. The possibility of child abuse should always be considered.