Chapter 351 Liver Abscess
Pyogenic liver abscesses are rare in children, with an incidence of 10/100,000 hospitalizations. Pyogenic hepatic abscesses can be caused by bacteria entering the liver via the portal circulation in cases of omphalitis, portal vein pylephlebitis, intra-abdominal infection, or abscess secondary to appendicitis or inflammatory bowel disease; a primary bacteremia (sepsis, endocarditis); ascending cholangitis associated with biliary tract obstruction caused by gallstones or sclerosing cholangitis, after a Kasai procedure, or secondary to choledochal cysts; contiguous infection or penetrating trauma; and cryptogenic biliary tract infections. Very rarely, liver abscesses occur after percutaneous liver biopsy. Hepatic abscesses can also occur in neonates in association with sepsis, umbilical vein infection, or cannulation; 50% are seen in children < 6 yr old. In adults with pyogenic liver abscesses, liver transplantation is a significant risk factor; it is not known if pediatric liver transplant patients are also at increased risk. Children with chronic granulomatous disease, Job syndrome or cancer are also at increased risk for a hepatic abscess.
In children with pyogenic liver abscesses, the most common pathogenic organisms include Staphylococcus aureus, Streptococcus spp; Escherichia coli, Klebsiella pneumoniae, Salmonella, and anaerobic organisms; Entamoeba histolytica or Toxocara canis–associated liver abscesses have also been reported in developing countries or in highly endemic areas.
Amebic disease is rare in the USA and is associated with immigrants from or travel to highly endemic areas. Recovery of E. histolytica from the stool is pathogenic and highly suggestive of an amebic abscess, but this must be distinguished from E. dispar, which looks similar but is nonpathogenic; antiamebic antibodies help identify E. histolyticum. Multiple microabscesses are most commonly secondary to bacteremia, candidemia, or cat scratch disease. Polymicrobial involvement is seen in ~50%; cryptogenic abscesses are often monomicrobial with S. aureus as the lead single agent in children.
Signs and symptoms are nonspecific and can include fever, chills, night sweats, malaise, fatigue, nausea, abdominal pain with right upper quadrant tenderness, and hepatomegaly; jaundice is uncommon. Diagnosis can be challenging and is often delayed; a high index of suspicion is necessary in children with risk factors. Serum aminotransferase and more often the alkaline phosphatase levels are elevated. The erythrocyte sedimentation rate is high, and leukocytosis is common. The results of blood cultures are positive in 50% of patients. Chest x-rays might show elevation of the right hemidiaphragm with decreased mobility or a right pleural effusion. Ultrasound or CT can confirm diagnosis (Figs. 351-1 to 351-3). Solitary liver abscesses (70% of cases) in the right lobe of the liver (75% of cases) are more common than multiple abscesses or solitary left lobe abscesses.
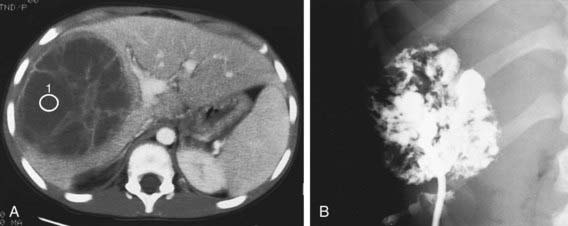
Figure 351-1 Liver abscess. A, Contrast-enhanced CT scan demonstrates a multioculated septated mass of decreased attenuation in the right lobe of the liver. There is increased attenuation of the septa. There is also faintly visible edema between the abscess and the enhanced normal liver. B, Injection of contrast material after percutaneous drainage of this documented streptococcal abscess demonstrates the multiocular nature of the lesion and its irregularly marginated wall.
(From Kuhn JP, Slovis TL, Haller JO: Caffrey’s pediatric diagnostic imaging, vol 2, ed 10, Philadelphia, 2004, Mosby, p 1470.)
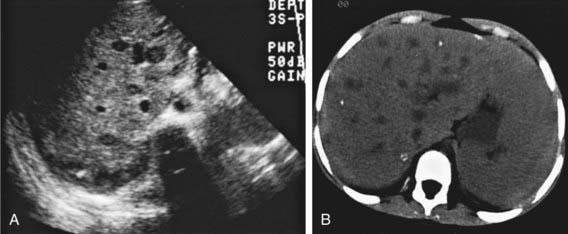
Figure 351-2 Hepatic candidiasis. Transverse sonogram (A) and CT scan (B) of the upper abdomen demonstrate “bull’s-eye” lesions in the right lobe of the liver in an immunocompromised patient. The calcifications seen on the CT scan are presumed to represent sequelae of prior infection. Liver biopsy demonstrated candidiasis.
(From Kuhn JP, Slovis TL, Haller JO: Caffrey’s pediatric diagnostic imaging, vol 2, ed 10, Philadelphia, 2004, Mosby, p 1472.)
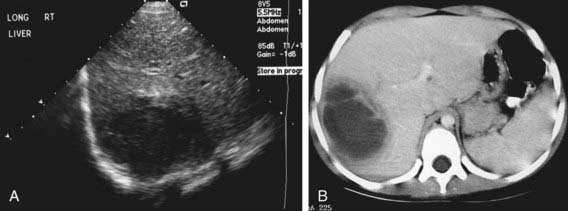
Figure 351-3 Amebic abscess. A, Sonogram demonstrates a hypoechogenic mass in the right lobe of the liver with a more hypoechoic surrounding rim. B, CT scan demonstrates a low-attenuation mass in the right lobe of the liver with a prominent halo.
(From Kuhn JP, Slovis TL, Haller JO: Caffrey’s pediatric diagnostic imaging, vol 2, ed 10, Philadelphia, 2004, Mosby, p 1473.)
Treatment requires percutaneous ultrasound- or CT-guided needle aspiration and less often open surgical drainage, particularly if multiple or large abscesses are present. Some place a drain and leave it in until the abscess wall collapses, others just do single or repeated aspirations. Aerobic and anaerobic cultures should be obtained. Some treat empirically without aspiration or drainage. If amebic disease is present, most do not attempt aspiration.
Antibiotic therapy should initially be broad spectrum but then narrowed, based on the culture results of the abscess fluid. Empirical initial antibiotic regimens include ampicillin/sulbactam, ticarcillin/clavulanic acid, or piperacillin/tazobactam. Others recommend a combination of a third-generation cephalosporin plus metronidazole. Amebic abscesses are treated with metronidazole or tinidazole plus paromomycin (oral nonabsorbable to treat the associated intestinal amebic infection). Antibiotic therapy for pyogenic abscess is intravenous for 2-3 wk followed by oral therapy to complete a 4-6 wk course. Mortality has decreased significantly since the 1980s with early diagnosis and initiation of appropriate therapy.
Fung CP, Change SC, Hu BS, et al. A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endopthalmitis? Gut. 2002;50:420-424.
Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol. 2004;2:1032-1038.
Kumar A, Srinivasan S, Sharma AK. Pyogenic liver abscess in children—South Indian experiences. J Pediatr Surg. 1998;33:417-421.
Margalit M, Elinav H, Ilan Y, et al. Liver abscess in inflammatory bowel disease: report of two cases and review of the literature. J Gastroenterol Hepatol. 2004;19:1338-1342.
Pereira FE, Musso C, Castelo JS. Pathology of pyogenic liver abscess in children. Pediatr Dev Pathol. 1999;2:537-543.
Pineiro-Carrero VM, Andres JM. Morbidity and mortality in children with pyogenic liver abscess. Am J Dis Child. 1989;143:1424-1427.