Chapter 403 Pulmonary Tumors
Etiology
Primary tumors of the lung are rare in children and adolescents. An accurate estimate of frequency is difficult because the literature is limited primarily to case reports and case series. A high incidence of “inflammatory pseudotumors” further clouds the statistics. Bronchial adenomas (including bronchial carcinoid, adenoid cystic carcinoma and mucoepidermoid carcinomas) are the most common primary tumors; bronchial carcinoid tumors represent ≈ 80%. Carcinoids are low-grade malignancies; carcinoid syndrome is rare in children. Metastatic lesions are the most common forms of pulmonary malignancy in children; primary processes include Wilms tumor, osteogenic sarcoma, and hepatoblastoma (Part XXII). Adenocarcinoma and undifferentiated histology are the most common pathologic findings in primary lung cancer; pulmonary blastoma is rarer and frequently occurs in the setting of cystic lung disease. Mediastinal involvement with lymphoma is more common than primary pulmonary malignancies.
Clinical Manifestations and Evaluation
Pulmonary tumors may manifest as fever, hemoptysis, wheezing, cough, pleural effusion, chest pain, dyspnea, or recurrent or persistent pneumonia or atelectasis. Tumors may be suspected from plain chest radiographs; CT scanning of the chest is necessary for precise anatomic definition (Fig. 403-1). Bronchial tumors are occasionally diagnosed during fiberoptic bronchoscopy performed for persistent or recurrent pulmonary infiltrates or for hemoptysis.
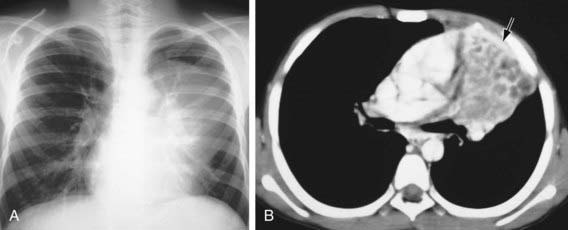
Figure 403-1 Endobronchial mucoepidermoid carcinoma in a 10 yr old boy who presented with cough and fever. A, The chest radiograph shows a left upper lobe mass, a hyperinflated left lower lobe, and a prominent left hilum. B, The CT scan shows complete obstruction of the left upper lobe bronchus by a low-attenuation mass that extends into the left mainstem bronchus.
(From Slovis TL, editor: Caffey’s pediatric diagnostic imaging, ed 11, vol 1, Philadelphia, 2008, Mosby.)
Patients with symptoms or with radiographic or other laboratory findings suggesting pulmonary malignancy should be evaluated carefully for a tumor at another site before surgical excision is carried out. Isolated primary lesions and isolated metastatic lesions discovered long after the primary tumor has been removed are best treated by excision. The prognosis varies and depends on the type of tumor involved; outcomes for inflammatory pseudotumors and primary pulmonary carcinoid tumors treated with resection are good.
Eggli KD, Newman B. Nodules, masses, and pseudomasses in the pediatric lung. Radiol Clin North Am. 1993;31:651-666.
Epstein DM, Aronchick JM. Lung cancer in childhood. Med Pediatr Oncol. 1989;17:510-513.
Hancock BJ, Di Lorenzo M, Youssef S, et al. Childhood primary pulmonary neoplasms. J Pediatr Surg. 1993;28:1133-1136.
Kaplan KA, Beierle EA, Faro A, et al. Recurrent pneumonia in children: a case report and approach to diagnosis. Clin Pediatr. 2006;45:15-22.
Keita O, Lagrange JL, Michiels JF, et al. Primary bronchogenic squamous cell carcinoma in children: report of a case and review of the literature. Med Pediatr Oncol. 1995;24:50-52.
McCahon E. Lung tumours in children. Pediatr Respir Rev. 2006;7:191-196.
Roviaro GC, Varoli F, Zannini P, et al. Lung cancer in the young. Chest. 1985;87:456-459.
Thomas R, Christopher DJ, Balamugesh T, et al. Clinico-pathologic study of pulmonary carcinoid tumours: a retrospective analysis and review of the literature. Respir Med. 2008;102:1611-1614.
Tian DL, Liu HX, Zhang L, et al. Surgery for young patients with lung cancer. Lung Cancer. 2003;42:215-220.