Chapter 498 Neoplasms of the Liver
Hepatic tumors are rare in children. Primary tumors of the liver account for approximately 1% of malignancies in children, with an annual incidence of 1.6 cases per million children in the USA. Between 50-60% of hepatic tumors in children are malignant, with >65% of these malignancies being hepatoblastomas and most of the remainder, hepatocellular carcinomas. Rare hepatic malignancies include embryonal sarcoma, angiosarcoma, malignant germ cell tumor, rhabdomyosarcoma of the liver, and undifferentiated sarcoma. More common childhood malignancies such as neuroblastoma and lymphoma can metastasize to the liver. Benign liver tumors, which usually present in the first 6 mo of life, include hemangiomas, hamartomas, and hemangioendotheliomas.
Hepatoblastoma
Epidemiology
Hepatoblastoma occurs predominantly in children <3 yr of age. The etiology is unknown. Hepatoblastomas are associated with familial adenomatous polyposis. Alterations in the antigen-presenting cell (APC)/β-catenin pathway have been found in most of the tumors evaluated. Hepatoblastoma also is associated with Beckwith-Wiedemann syndrome, which can show a similar loss of genomic imprinting of the insulin-like growth factor-2 gene. Low birthweight is associated with increased incidence of hepatoblastoma, with the risk increasing as birthweight decreases.
Pathogenesis
Hepatoblastoma can be epithelial type, containing fetal or embryonal malignant cells (either as a mixture or as pure elements), or the mixed type, containing mesenchymal and epithelial elements. Pure fetal histology predicts a more favorable outcome.
Clinical Manifestations
Hepatoblastoma usually presents as a large, asymptomatic abdominal mass. It arises from the right lobe 3 times more often than the left and usually is unifocal. As the disease progresses, weight loss, anorexia, vomiting, and abdominal pain may ensue. Metastatic spread of hepatoblastoma most commonly involves regional lymph nodes and the lungs.
A valuable serum tumor marker, α-fetoprotein (AFP), is used in the diagnosis and monitoring of hepatic tumors. AFP level is elevated in almost all hepatoblastomas. Bilirubin and liver enzymes usually are normal. Anemia is common, and thrombocytosis occurs in about 30% of patients. Hepatitis B and C serology should be obtained but usually are negative in hepatoblastoma.
Diagnostic imaging should include plain radiographs and ultrasonography of the abdomen to characterize the hepatic mass. Ultrasonography can differentiate malignant hepatic masses from benign vascular lesions. Either CT or MRI is an accurate method of defining the extent of intrahepatic tumor involvement and the potential for surgical resection. Evaluation for metastatic disease should include CT of the chest.
Treatment
In general, the cure of malignant hepatic tumors in children depends on complete resection of the primary tumor (Fig. 498-1). As much as 85% of the liver can be resected, with hepatic regeneration noted within 3-4 mo after surgery. Cisplatin in combination with vincristine and 5-fluorouracil or doxorubicin is effective treatment for hepatoblastoma and increases the chances of cure after complete surgical resection. In low-stage tumors, survival rates >90% can be achieved with multimodal treatment, including surgery and adjuvant chemotherapy. With tumors unresectable at diagnosis, survival rates of approximately 60% can be obtained. Metastatic disease further reduces survival, but complete regression of disease often can be obtained with chemotherapy and surgical resection of the primary tumor and isolated pulmonary metastatic disease, resulting in survival rates of about 25%. Liver transplant is a viable option for unresectable primary hepatic malignancies and results in good long-term survival. Pretransplant medical condition is an important predictor of outcome, and thus transplant is much more effective as the primary surgery than as salvage therapy.
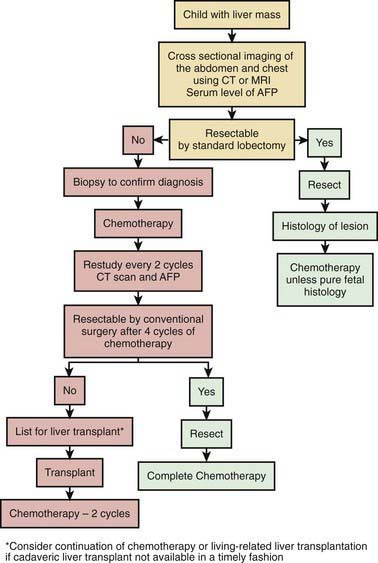
Figure 498-1 Algorithm for the management of a child who presents with a hepatoblastoma. AFP, α-fetoprotein.
(From Tiao GM, Bobey N, Allen S, et al: The current management of hepatoblastoma: a combination of chemotherapy, conventional resection, and liver transplantation, J Pediatr 146:204–211, 2005.)
Hepatocellular Carcinoma
Epidemiology
Hepatocellular carcinoma occurs mostly in adolescents and often is associated with hepatitis B or C infection. It is more common in East Asia and other areas where hepatitis B is endemic, the incidence has decreased following the introduction of hepatitis B vaccination. In these areas it also tends to occur in a bimodal pattern, with the younger age peak overlapping the age of hepatoblastoma presentation. It also occurs in the chronic form of hereditary tyrosinemia, galactosemia, glycogen storage disease, α1-antitrypsin deficiency, and biliary cirrhosis. Aflatoxin B contamination of food is another risk factor.
Pathogenesis
Hepatocellular carcinoma usually presents as a multicentric, invasive tumor consisting of large pleomorphic cells with a lack of underlying cirrhosis. The fibrolamellar variant of hepatocellular carcinoma occurs more often in adolescent and young adult patients. Although previous reports have suggested that the fibrolamellar type has a better prognosis, more recent data analysis refutes this.
Clinical Manifestations
Hepatocellular carcinoma usually presents as a hepatic mass, abdominal distention, and symptoms of anorexia, weight loss, and abdominal pain. Hepatocellular carcinoma can present as an acute abdominal crisis with rupture of the tumor and hemoperitoneum. The AFP level is elevated in approximately 60% of children with hepatocellular carcinoma. Evidence of hepatitis B and C infection usually is found in endemic areas but not in Western countries or with the fibrolamellar type. Bilirubin usually is normal, but liver enzymes may be abnormal.
Diagnostic imaging should include plain radiographs and ultrasonography of the abdomen to characterize the hepatic mass. Ultrasonography can differentiate malignant hepatic masses from benign vascular lesions. Either CT or MRI is an accurate method of defining the extent of intrahepatic tumor involvement and the potential for surgical resection. Evaluation for metastatic disease should include CT of the chest.
Treatment
Because of the multicentric origin of hepatocellular carcinoma, complete resection of this tumor is accomplished in only 30-40% of cases. Even with complete surgical resection, only 30% of children are long-term survivors. Chemotherapy, including cisplatin, doxorubicin, etoposide, and 5-fluorouracil, has shown some activity against this tumor, but improved long-term outcome has been difficult to achieve. Other techniques such as chemoembolization and liver transplantation are under study as therapy for hepatocellular carcinomas.
Austin MT, Leys CM, Feurer ID, et al. Liver transplantation for childhood hepatic malignancy: a review of the United Network for Organ Sharing (UNOS) database. J Pediatr Surg. 2006;41:182-186.
Litten JB, Tomlinson GE. Liver tumors in children. Oncologist. 2008;13:812-820.
Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907-1916.
Perilongo G, Maibach R, Shafford E, et al. Cisplatin versus cisplatin plus doxorubicin for standard-risk hepatoblastoma. N Engl J Med. 2009;361:1662-1670.
Tiao GM, Bobey N, Allen S, et al. The current management of hepatoblastoma: a combination of chemotherapy, conventional resection, and liver transplantation. J Pediatr. 2005;146:204-211.