Chapter 562 Hyperthyroidism
Hyperthyroidism results from excessive secretion of thyroid hormone; during childhood, with few exceptions, it is due to Graves disease (Table 562-1). Graves disease is an autoimmune disorder; production of thyroid-stimulating immunoglobulin (TSI) results in diffuse toxic goiter. Germline mutations of the thyroid-stimulating hormone (TSH) receptor resulting in constitutively activating (gain-of-function) mutations are found in both familial (autosomal dominant) and sporadic cases of non-autoimmune hyperthyroidism. These patients, whose disease can appear in the neonatal period or in later childhood, have thyroid hyperplasia with goiter and suppressed levels of TSH. Different activating mutations have been identified in some cases of thyroid adenomas. Hyperthyroidism occurs in some patients with McCune-Albright syndrome as a result of an activating mutation of the α subunit of the G-protein; these patients tend to have a multinodular goiter. Other rare causes of hyperthyroidism that have been observed in children include toxic uninodular goiter (Plummer disease), hyperfunctioning thyroid carcinoma, thyrotoxicosis factitia, subacute thyroiditis, and acute suppurative thyroiditis.
Table 562-1 CAUSES OF HYPERTHYROIDISM
| CAUSES OF HYPERTHYROIDISM | PATHOPHYSIOLOGIC FEATURES | INCIDENCE |
|---|---|---|
| CIRCULATING THYROID STIMULATORS | ||
| Graves disease | Thyroid-stimulating immunoglobulins | Common |
| Neonatal Graves disease | Thyroid-stimulating immunoglobulins | Rare |
| Thyrotropin-secreting tumor | Pituitary adenoma | Very rare |
| Choriocarcinoma | Human chorionic gonadatropin secretion | Rare |
| THYROIDAL AUTONOMY | ||
| Toxic multinodular goiter | Activating mutations in thyrotropin receptor or G-protein | Common |
| Toxic solitary adenoma | Activating mutations in thyrotropin receptor or G-protein | Common |
| Congenital hyperthyroidism | Activating mutations in thyrotropin receptor | Very rare |
| Iodine-induced hyperthyroidism (Jod-Basedow) | Unknown; excess iodine results in unregulated thyroid hormone production | Uncommon in USA and other iodine-sufficient areas |
| DESTRUCTION OF THYROID FOLLICLES (THYROIDITIS) | ||
| Subacute thyroiditis | Probable viral infection | Uncommon |
| Painless or postpartum thyroiditis | Autoimmune | Common |
| Amiodarone-induced thyroiditis | Direct toxic drug effects | Uncommon |
| Acute (infectious) thyroiditis | Thyroid infection (e.g., bacterial, fungal) | Uncommon |
| EXOGENOUS THYROID HORMONE | ||
| Iatrogenic | Excess ingestion of thyroid hormone | Common |
| Factitious | Excess ingestion of thyroid hormone | Rare |
| Hamburger thyrotoxicosis | Thyroid gland included in ground beef | Probably rare |
| ECTOPIC THYROID TISSUE | ||
| Struma ovarii | Ovarian teratoma containing thyroid tissue | Rare |
| Metastatic follicular thyroid cancer | Large tumor mass capable of secreting thyroid hormone autonomously | Rare |
| Pituitary resistance to thyroid hormone | Mutated thyroid hormone receptor with greater expression in the pituitary compared with peripheral tissues | Rare |
Adapted from Cooper DS: Hyperthyroidism, Lancet 362:459–468, 2003.
Suppression of plasma TSH indicates that the hyperthyroidism is not pituitary in origin. Hyperthyroidism due to excess thyrotropin secretion is rare and, in most cases, is caused by pituitary resistance to thyroid hormone. TSH-secreting pituitary tumors have been reported only in adults. In infants born to mothers with Graves disease, hyperthyroidism is almost always a transitory phenomenon; classic Graves disease during the neonatal period is rare. Choriocarcinoma, hydatidiform mole, and struma ovarii have caused hyperthyroidism in adults but have not been recognized as causes in children.
Studies have examined the health and quality of life of subjects with subclinical hyperthyroidism (i.e., with TSH <0.1 mU/L) or who are euthyroid on antithyroid medication. These studies suggest that subclinical hyperthyroidism carries a risk of late-life atrial fibrillation and that treatment of hyperthyroidism with antithyroid medication does not reliably induce remission that is durable when medication is discontinued. There appears to be no difference in long-term quality of life among hyperthyroid patients treated with antithyroid medication, radioiodine ablation, or surgery. Quality of life was diminished relative to control subjects in all three cases (Chapter 562.1).
562.1 Graves Disease
Epidemiology
Graves disease occurs in approximately 0.02% of children (1 : 5,000). It has a peak incidence in the 11- to 15-yr old; there is a 5 : 1 female to male ratio. Most children with Graves disease have a positive family history of some form of autoimmune thyroid disease. In Japan, familial Graves disease, defined as Graves disease in a 1st-degree relative, occurs in 2-3% of cases.
Etiology
Enlargement of the thymus, splenomegaly, lymphadenopathy, infiltration of the thyroid gland and retro-orbital tissues with lymphocytes and plasma cells, and peripheral lymphocytosis are well-established findings in Graves disease. In the thyroid gland, T helper cells (CD4+) predominate in dense lymphoid aggregates; in areas of lower cell density, cytotoxic T cells (CD8+) predominate. The percentage of activated B lymphocytes infiltrating the thyroid is higher than in peripheral blood. A postulated failure of T suppressor cells allows expression of T helper cells, sensitized to the TSH antigen, which interact with B cells. These cells differentiate into plasma cells, which produce thyrotropin receptor–stimulating antibody (TRSAb). TRSAb binds to the receptor for TSH and stimulates cyclic adenosine monophosphate, resulting in thyroid hyperplasia and unregulated overproduction of thyroid hormone. In addition to TRSAb, thyrotropin receptor-blocking antibody (TRBAb) may also be produced, and the clinical course of the disease usually correlates with the ratio between the two antibodies.
The ophthalmopathy occurring in Graves disease appears to be caused by antibodies against antigens shared by the thyroid and eye muscle. TSH receptors have been identified in retro-orbital adipocytes and might represent a target for antibodies. The antibodies that bind to the extraocular muscles and orbital fibroblasts stimulate the synthesis of glycosaminoglycans by orbital fibroblasts and produce cytotoxic effects on muscle cells.
In whites, Graves disease is associated with HLA-B8 and HLA-DR3; the latter carries a 7-fold relative risk for Graves disease. Graves disease is also associated with other HLA-D3–related disorders such as Addison disease, type 1 diabetes mellitus, myasthenia gravis, and celiac disease. Systemic lupus erythematosus, rheumatoid arthritis, vitiligo, idiopathic thrombocytopenic purpura, and pernicious anemia have been described in children with Graves disease. In family clusters, the conditions associated most commonly with Graves disease are autoimmune lymphocytic thyroiditis and hypothyroidism. In Japanese children, Graves disease is associated with different HLA haplotypes: HLA-DRB1*0405 and HLA-DQB1*0401.
Clinical Manifestations
About 5% of all patients with hyperthyroidism are <15 yr of age; the peak incidence in these children occurs during adolescence. Although rare, Graves disease has begun between 6 wk and 2 yr of age in children born to mothers without a history of hyperthyroidism. The incidence is about 5 times higher in girls than in boys.
The clinical course in children is highly variable but usually is not so fulminant as in many adults (Table 562-2). Symptoms develop gradually; the usual interval between onset and diagnosis is 6-12 mo and may be longer in prepubertal children compared with adolescents. The earliest signs in children may be emotional disturbances accompanied by motor hyperactivity. The children become irritable and excitable, and they cry easily because of emotional lability. They are restless sleepers and tend to kick their covers off. Their schoolwork suffers as a result of a short attention span and poor sleep. Tremor of the fingers can be noticed if the arm is extended. There may be a voracious appetite combined with loss of or no increase in weight. Recent height measurements might show an acceleration in growth velocity.
Table 562-2 MAJOR SYMPTOMS AND SIGNS OF HYPERTHYROIDISM AND OF GRAVES DISEASE AND CONDITIONS ASSOCIATED WITH GRAVES DISEASE
MANIFESTATIONS OF HYPERTHYROIDISM
Symptoms
Signs
MANIFESTATIONS OF GRAVES DISEASE
CONDITIONS ASSOCIATED WITH GRAVES DISEASE
Adapted from Weetman AP: Graves disease, N Engl J Med 343:1236–1248, 2000.
The size of the thyroid is variable. It may be so minimally enlarged that it initially escapes detection, but with careful examination, a diffuse goiter, soft with a smooth surface, is found in almost all patients. Exophthalmos is noticeable in most patients but is usually mild. Lagging of the upper eyelid as the eye looks downward, impairment of convergence, and retraction of the upper eyelid and infrequent blinking may be present (Figs. 562-1 and 562-2). Ocular manifestations can produce pain, lid erythema, chemosis, decreased extraocular muscle function, and decreased visual acuity (corneal or optic nerve involvement). The skin is smooth and flushed, with excessive sweating. Muscular weakness is uncommon but may be severe enough to result in clumsiness. Tachycardia, palpitations, dyspnea, and cardiac enlargement and insufficiency cause discomfort but rarely endanger the patient’s life. Atrial fibrillation is a rare complication. Mitral regurgitation, probably resulting from papillary muscle dysfunction, is the cause of the apical systolic murmur present in some patients. The systolic blood pressure and the pulse pressure are increased. Reflexes are brisk, especially the return phase of the Achilles reflex. Many of the findings in Graves disease result from hyperactivity of the sympathetic nervous system.

Figure 562-1 A 15 yr old girl with classic Graves disease. Clinical features include a goiter and exophthalmos. She was treated with antithyroid drugs, to which she had a good response.

Figure 562-2 Retraction of upper eyelids in the primary gaze (Dalrymple sign).
(From Kanski JJ: Systemic diseases and the eye: signs and differential diagnosis, London, 2001, Mosby.)
Thyroid crisis, or thyroid storm, is a form of hyperthyroidism manifested by an acute onset, hyperthermia, severe tachycardia, heart failure, and restlessness. There may be rapid progression to delirium, coma, and death. Precipitating events include trauma, infection, radioactive iodine treatment, or surgery. Apathetic, or masked, hyperthyroidism is another variety of hyperthyroidism characterized by extreme listlessness, apathy, and cachexia. A combination of both forms can occur. These symptom complexes are rare in children.
Laboratory Findings
Serum levels of thyroxine (T4), triiodothyronine (T3), free T4, and free T3 are elevated. In some patients, levels of T3 may be more elevated than those of T4. Levels of TSH are suppressed to below the lower range of normal. Antithyroid antibodies, including thyroid peroxidase antibodies, are often present. Most patients with newly diagnosed Graves disease have measurable TRSAb; the two methods to measure TRSAb are thyroid-stimulating immunoglobulin (TSI) or thyrotropin-binding inhibitor immunoglobulin (TBII). Measurement of TSI or TBII is useful in confirming the diagnosis of Graves disease. Radioiodine is rapidly and diffusely concentrated in the thyroid, but this study is rarely necessary. Children who experience an acceleration of growth might also have advanced skeletal maturation. Bone density may be reduced at diagnosis but returns to normal with treatment.
Differential Diagnosis
Diagnosis is rarely difficult once hyperthyroidism is considered. Elevated levels of T4 or free T4 and T3 in association with suppressed levels of TSH are usually diagnostic (see Table 562-1). The presence of TRSAb establishes the cause as Graves disease.
Other causes of hyperthyroidism are uncommon. If a thyroid nodule is palpable, or if T3 is preferentially elevated, a functional thyroid nodule must be considered. Radionuclide study is diagnostic, with uptake in the nodule and absent uptake in the rest of the gland (hot nodule). Children with a toxic multinodular goiter may have either a TSH receptor activating mutation or McCune-Albright syndrome. If precocious puberty, polyostotic fibrous dysplasia, or café-au-lait pigmentation is present, the autonomous thyroid disorder of McCune-Albright syndrome is likely. Hyperthyroidism associated with some form of thyroiditis, e.g., subacute thyroiditis, is relatively rare in childhood. Patients with generalized thyroid hormone resistance have elevated levels of free T4, but levels of TSH are inappropriately elevated or normal. Patients with greater pituitary resistance to thyroid hormone than generalized thyroid hormone resistance also have clinical hyperthyroidism. They must be differentiated from patients with TSH-secreting pituitary tumors who have elevated serum levels of the TSH α chain. Most other causes of hyperthyroxinemia are uncommon but can result in erroneous diagnosis. Patients with elevated thyroxine-binding globulin (TBG) levels or familial dysalbuminemic hyperthyroxinemia have normal levels of free T4 and TSH.
When hyperthyroxinemia is caused by exogenous thyroid hormone, levels of free T4 and TSH are the same as those seen in Graves disease, but the level of thyroglobulin is very low, whereas in patients with Graves disease, it is elevated.
Treatment
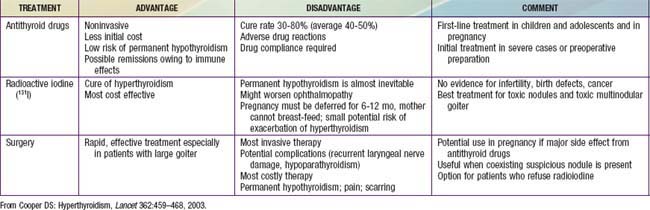
Most pediatric endocrinologists recommend initial medical therapy using antithyroid drugs rather than radioiodine or subtotal thyroidectomy, although radioiodine is gaining acceptance as initial treatment in children >10 yr of age. All therapeutic options have advantages and disadvantages (Table 562-3). The 2 antithyroid drugs used historically are propylthiouracil (PTU) and methimazole (Tapazole). Both compounds inhibit incorporation of trapped inorganic iodide into organic compounds, and they might also suppress TRSAb levels by directly affecting intrathyroidal autoimmunity. However, there are important differences between the drugs. Methimazole is at least 10 times more potent than PTU on a weight basis and has a much longer serum half-life (6-8 hr vs 0.5 hr); PTU generally is administered 3 times daily, but methimazole can be given once daily. Unlike methimazole, PTU is heavily protein bound and has a lesser ability to cross the placenta and to pass into breast milk; theoretically, PTU is the preferred drug during pregnancy and for nursing mothers. Due to reports of severe liver disease in patients treated with PTU, with some patients requiring liver transplant or potentially suffering a fatal outcome, the consensus is to use only methimazole to treat children with Graves disease.
Adverse reactions occur with antithyroid drugs; most are mild, but some are life threatening. Minor adverse effects occur in approximately 10-20%, and more-severe adverse effects occur in 2-5% of children. Reactions are unpredictable and can occur after therapy of any duration. Transient granulocytopenia (<2,000/mm3) is common; it is asymptomatic and is not a harbinger of agranulocytosis, and it usually is not a reason to discontinue treatment. Transient urticarial rashes are common. They may be managed by a short period off therapy, and then restarting the antithyroid drug. The most severe reactions are hypersensitive and include agranulocytosis (0.1-0.5%), hepatitis (0.2-1%), a lupus-like polyarthritis syndrome, glomerulonephritis, and an ANCA-positive vasculitis involving the skin and other organs. Severe liver disease, including liver failure requiring transplant, have been reported exclusively with PTU. The most common liver disease associated with methimazole is cholestatic jaundice, reversible when the drug is discontinued. Patients with severe adverse effects should be treated with radioiodine or thyroidectomy. Cases of congenital skin defects (aplasia cutis) have been seen in infants exposed in fetal life to methimazole, but this association does not appear to be a strong one.
The initial dosage of methimazole is 0.25-1.0 mg/kg/24 hr given once or twice daily. Smaller initial dosages should be used in early childhood. Careful surveillance is required after treatment is initiated. Rising serum levels of TSH to greater than normal indicates overtreatment and leads to increased size of the goiter. Clinical response becomes apparent in 3-6 wk, and adequate control is evident in 3-4 mo. The dose is decreased to the minimal level required to maintain a euthyroid state.
Most studies report a remission rate of approximately 25% after 2 years of antithyroid drug treatment in children. Some studies find that longer treatment is associated with higher remission rates, with one study reporting a 50% remission rate after 4.5 years of drug treatment. If a relapse occurs, it usually appears within 3 mo and almost always within 6 mo after therapy has been discontinued. Therapy may be resumed in case of relapse. Patients older than 13 yr of age, boys, those with a higher body mass index, and those with small goiters and modestly elevated T3 levels appear to have earlier remissions.
A β-adrenergic blocking agent such as propranolol (0.5-2.0 mg/kg/24 hr orally, divided 3 times daily) or atenolol (1-2 mg/kg orally given once daily) is a useful supplement to antithyroid drugs in the management of severely toxic patients. Additional therapies for thyroid storm are listed in Table 562-4. Thyroid hormones potentiate the actions of catecholamines, including tachycardia, tremor, excessive sweating, lid lag, and stare. These symptoms abate with the use of propranolol, which does not, however, alter thyroid function or exophthalmos.
Table 562-4 MANAGEMENT OF THYROID STORM IN ADOLESCENTS
| GOAL | TREATMENT |
|---|---|
| Inhibition of thyroid hormone formation and secretion | Propylthiouracil (PTU), 400 mg every 8 hr PO or by nasogastric tube Sodium iodide, 1 g IV in 24 hr, or saturated solution of KI, 5 drops every 8 hr |
| Sympathetic blockade | Propranolol, 20-40 mg every 4-6 hr, or 1.mg IV slowly (repeat doses until heart rate slows); not indicated in patients with asthma or heart failure that is not rate related |
| Glucocorticoid therapy | Hydrocortisone, 50-100 mg IV every 6 hr |
| Supportive therapy | Intravenous fluids (depending on indication: glucose, electrolytes, multivitamins) Temperature control (cooling blankets, acetaminophen; avoid salicylates) O2 if required Digitalis for heart failure and to slow ventricular response; pentobarbital for sedation Treatment of precipitating event (e.g., infection) |
From Goldman L, Ausiello D: Cecil Textbook of Medicine, ed 22, Philadelphia, 2004, WB Saunders, p 1401.
Radioiodine treatment or surgery is indicated when adequate cooperation for medical management is not possible, when adequate trial of medical management has failed to result in permanent remission, or when severe side effects preclude further use of antithyroid drugs. Either of these treatments may also be preferred by the patient or parent.
Radioiodine is an effective, relatively safe first or alternative therapy for Graves disease in children >10 yr of age. Pretreatment with antithyroid drugs is unnecessary; if a patient is taking them, they should be stopped a week before radioiodine administration. Many pediatric endocrinologists prefer to select a dose of radioiodine to ensure complete ablation of thyroid tissue. A dose of 300 µCi/g of thyroid tissue, or a total dose of approximately 15 mCi, will achieve this goal. Essentially all patients treated at this dose will become hypothyroid; the time course to hypothyroidism averages 11 wk, with a range of 9-28 wk. Because the full effects of treatment may not be complete for 1-6 mo, adjunctive therapy with a β-adrenergic antagonist and lower doses of antithyroid drugs are recommended. With lower treatment doses of radioiodine, hypothyroidism occurs in 10-20% of patients after the 1st year and in about 3% per year thereafter. Although there have been concerns about radiation oncogenesis and genetic damage, follow-up for as long as 50 yr has not shown this in treated children. The use of lower doses of radioactive iodine (50-200 µCi/g) is associated with an increased risk of benign adenomas (0.6-1.9% in one study). Albeit second primary neoplasms are rare, a few studies report an increased risk of second primary neoplasms, including leukemia, in adult patients with Graves disease treated with radioactive iodine. Because children may be more susceptible to the effects of radioactive iodine, some cardiologists prefer surgery for children <10 yr of age who are candidates for a more definitive treatment.
Subtotal thyroidectomy, a safe procedure when performed by an experienced team, is done only after the patient has been brought to a euthyroid state. This may be accomplished with methimazole over 2-3 mo. After a euthyroid state has been attained, a saturated solution of potassium iodide, 5 drops/24 hr, are added to the regimen for 2 wk before surgery to decrease the vascularity of the gland. Complications of surgical treatment are rare and include hypoparathyroidism (transient or permanent) and paralysis of the vocal cords. The incidence of residual or recurrent hyperthyroidism or hypothyroidism depends on the extent of the surgery. Most recommend near-total thyroidectomy. The incidence of recurrence is low, and most patients become hypothyroid.
The ophthalmopathy remits gradually and usually independently of the hyperthyroidism. Severe ophthalmopathy can require treatment with high-dose prednisone, orbital radiotherapy (of questionable value), or orbital decompression surgery. Cigarette smoking is a risk factor for thyroid eye disease and should be avoided or discontinued to avoid progression of eye involvement.
Abraham-Nordling M, Torring O, Hamberger B, et al. Graves’ disease: a long-term quality-of-life follow up of patients randomized to treatment with antithyroid drugs, radioiodine, or surgery. Thyroid. 2005;15:1279-1286.
Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726-736.
Barrio R, Lopez-Capape M, Martinez-Badas I, et al. Graves’ disease in children and adolescents: response to long-term treatment. Acta Paediatr. 2005;94:1583.
Brent GA. Graves’ disease. N Engl J Med. 2008;358:2594-2605.
Cassio A, Corrias A, Gualandi S, et al. Influence of gender and pubertal stage at diagnosis on growth outcome in childhood thyrotoxicosis: results of a collaborative study. Clin Endocrinol (Oxf). 2006;64:53-57.
Cooper DS. Antithyroid drugs. N Engl J Med. 2005;352:905-917.
Food and Drug Administration. FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. (website) www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm Accessed September 15, 2010
Glaser NS, Styne DM. Predicting the likelihood of remission in children with Graves’ disease: a prospective, multicenter study. Pediatrics. 2008;121:e481-e488.
Goldstein SM, Katoqitz WR, Moshang T, et al. Pediatric thyroid-associated orbitopathy: the Children’s Hospital of Philadelphia experience and literature review. Thyroid. 2008;18:997-999.
Haentjens P, Van Meerhaeghe A, Poppe K, et al. Subclinical thyroid dysfunction and mortality: an estimate of relative and absolute excess all-cause mortality based on time-to-event data from cohort studies. Eur J Endocrinol. 2008;159:329-341.
Iwama S, Ikezaki A, Kikuoka N, et al. Association of HLA-DR, DQ genotypes and CTLA-4 gene polymorphism with Graves’ disease in Japanese children. Horm Res. 2005;63:55-60.
Kaguelidou F, Alberti C, Castanet M, et al. Predictors of autoimmune hyperthyroidism relapse in children after discontinuation of antithyroid drug treatment. J Clin Endocrinol Metab. 2008;93:3817.
Kharlip J, Cooper DS. Recent developments in hyperthyroidism. Lancet. 2009;373:1930-1932.
Laurberg P, Wallin G, Tallstedt L, et al. TSH-receptor autoimmunity in Graves’ disease after therapy with anti-thyroid drugs, surgery, or radioiodine: a 5-year prospective randomized study. Eur J Endocrinol. 2008;158:69-75.
Ma C, Kuang A, Xie J, et al: Radioiodine treatment for pediactric Graves’ disease, Cochrane Database Syst Rev CD006294, 2008.
Mesto S, Auvinen A, Huhtala H, et al. Increased cancer incidence after radioiodine treatment for hyperthyroidism. Cancer. 2007;109:1972-1979.
Nabhan Z, Kreher NC, Eugster EA. Hashitoxicosis in children: clinical features and natural history. J Pediatr. 2005;146:533-536.
Pearce EN. Diagnosis and management of thyrotoxicosis. BMJ. 2006;332:1369-1373.
Pinto T, Cummings EA, Barnes D, et al. Clinical course of pediatric and adolescent Graves’ disease treated with radioactive iodine. J Pediatr Endocrinol Metab. 2007;20:973-980.
Rahhal SN, Eugster EA. Thyroid stimulating immunoglobulin is often negative in children with Graves’ disease. J Pediatr Endocrinol Metab. 2008;21:1085-1088.
Read CH, Tansey MJ, Menda Y. A 36-year retrospective analysis of the efficacy and safety of radioactive iodine in treating young Graves’ patients. J Clin Endocrinol Metab. 2004;89:4229-4233.
Rivkees SA, Dinauer C. An optimal treatment for pediatric graves’ disease is radioiodine. J Clin Endocrinol Metab. 2007;92:797.
Rivkees SA, Mattison DR. Ending propylthiouracil-induced liver failure in children. N Engl J Med. 2009;360:1574-1575.
Sugino K, Ito K, Mimura T, et al. Surgical treatment of Graves’ disease in children. Thyroid. 2004;14:447-452.
562.2 Congenital Hyperthyroidism
Etiology and Pathogenesis
Neonatal Graves disease is caused by transplacental passage of TRSAb, but the clinical onset, severity, and course may be modified by the concurrent presence of TRBAb and by the transplacental passage of antithyroid drugs taken by the mother. Very high levels of TRSAb usually result in classic neonatal hyperthyroidism, but if the infant has been exposed to antithyroid drugs, onset of symptoms is delayed by 3-4 days to allow degradation of the maternally derived antithyroid drug. If TRBAb is also present, onset of hyperthyroid symptoms may be delayed for several weeks. The mothers of these infants have active Graves disease, Graves disease in remission, a past history of Graves disease managed by radioactive iodine ablation or surgery, or rarely hypothyroidism and a history of lymphocytic thyroiditis.
Neonatal hyperthyroidism occurs in only about 2% of infants born to mothers with a history of Graves disease. The finding of very high levels of TRSAb in these mothers (usually >500% of normal) predicts the occurrence of an affected infant. Fetal tachycardia and goiter can allow prenatal diagnosis. Unlike Graves disease at all other ages, neonatal hyperthyroidism affects boys as often as girls. One would expect twins to be equally affected, but one case reported one twin to be hyperthyroid and the other twin to be hypothyroid. Both eventually recovered to euthyroidism.
The disorder usually remits spontaneously within 6-12 wk but can persist longer, depending on the levels of TRSAb. Mild asymptomatic hyperthyroxinemia also occurs. Rarely, classic neonatal Graves disease does not remit but persists for several years or longer. These children have impressive family histories of Graves disease. In these infants, TRSAb transfer from the mother apparently blends with the infantile onset of autonomous Graves disease.
Clinical Manifestations
Many of the infants are premature and appear to have intrauterine growth restriction. Most have goiters. The infant is extremely restless, irritable, and hyperactive and appears anxious and unusually alert. Microcephaly and ventricular enlargement may be present. The eyes are opened widely and appear exophthalmic (Fig. 562-3). There may be extreme tachycardia and tachypnea, and the temperature is elevated. In severely affected infants, there is a progression of symptoms; weight loss occurs despite a ravenous appetite, hepatosplenomegaly increases, and jaundice can occur. Severe hypertension and cardiac decompensation can occur. The infant can die if therapy is not instituted promptly. The serum level of T4 or free T4 and T3 are markedly elevated, and TSH is suppressed. Advanced bone age, frontal bossing with triangular facies, and cranial synostosis are common, especially in infants with persistent clinical manifestations of hyperthyroidism.

Figure 562-3 Twin boys with neonatal hyperthyroidism confirmed by abnormal thyroid function tests. Clinical features include lack of subcutaneous tissue owing to a hypermetabolic state and a wide-eyed, anxious stare. They were given the diagnosis of neonatal Graves disease, but in fact, their mother did not have Graves disease; they had persistent, not transient, hyperthyroidism. At age 8 yr, they were treated with radioiodine. They are now believed to have had some other form of neonatal hyperthyroidism, such as a constitutive activation of the thyroid-stimulating hormone (TSH) receptor.
Treatment
Treatment of the neonate consists of oral administration of propranolol (1-2 mg/kg/24 hr, orally in 3 divided doses) and methimazole (0.25-1.0 mg/kg/24 hr given every 12 hr); Lugol solution (1 drop every 8 hr) may be added. When propranolol is used during pregnancy to treat thyrotoxicosis, it crosses the placenta and can cause respiratory depression in the newborn infant. If the thyrotoxic state is severe, parenteral fluid therapy and corticosteroids may be indicated. If heart failure occurs, digitalization is indicated. After a euthyroid state is reached, only antithyroid drug treatment is necessary. The dose should be gradually tapered to keep the infant euthyroid. Most cases remit by 3-4 mo of age.
Occasionally, neonatal hyperthyroidism does not remit but persists into childhood. These patients can have an impressive family history of hyperthyroidism. Neonatal hyperthyroidism, without evidence for autoimmune disease in mother or infant, may be due to a mutation in the TSHR gene that produced constitutive activation of the receptor. Neonatal hyperthyroidism has also been reported in patients with McCune-Albright syndrome, a result of an activating mutation of the α subunit of the G-protein. Under these circumstances, hyperthyroidism recurs when antithyroid drugs are discontinued; these children eventually must be treated with radioiodine or surgery.
Prognosis
Advanced osseous maturation, microcephaly, and mental retardation occur when treatment is delayed. Intellectual development is normal in most treated infants with neonatal Graves disease, though some manifest neurocognitive problems from in utero hyperthyroidism. In some infants, in utero hyperthyroidism appears to suppress the hypothalamic-pituitary-thyroid feedback mechanism, and they develop permanent central hypothyroidism, requiring lifelong thyroid hormone treatment.
Azizi F, Khamseh ME, Bahreynian M, et al. Thyroid function and intellectual development of children of mothers taking methimazole during pregnancy. J Endocrinol Invest. 2002;25:586-589.
Chester J, Rotenstein D, Ringkananont U, et al. Congenital neonatal hyperthyroidism caused by germline mutations in the TSH receptor gene. J Pediatr Endocrinol Metab. 2008;21:479-486.
Cohen O, Pinchas-Hamiel O, Sivan E, et al. Serial in utero ultrasonographic measurements of the fetal thyroid: a new complimentary tool in the management of maternal hyperthyroidism in pregnancy. Prenat Diagn. 2003;23:740-742.
Hashemipour M, Hasani N, Amini M, et al. Thyroid function abnormalities among first-degree relatives of Iranian congenital hypothyroidism neonates. Pediatr Int. 2010;52:467-471.
Kempers MJ, van Tijn DA, van Trotsenburg AS, et al. Central congenital hypothyroidism due to gestational hyperthyroidism: detection where prevention failed. J Clin Endocrinol Metab. 2003;88:5851-5857.
Mastorakos G, Mitsiades NS, Doufas AG, et al. Hyperthyroidism in McCune-Albright syndrome with a review of thyroid abnormalities sixty years after the first report. Thyroid. 1997;7:433-439.
O’Connor MJ, Paget-Brown AO, Clarke WL. Premature twins of a mother with Graves’ disease with discordant thyroid function: a case report. J Perinatol. 2007;27:388-389.
Papendieck P, Chiesa A, Prieto L, et al. Thyroid disorders of neonates born to mothers with Graves’ disease. J Pediatr Endocrinol Metab. 2009;22:547-553.
Peleg D, Cada S, Peleg A, et al. The relationship between maternal serum thyroid-stimulating immunoglobulin and fetal and neonatal thyrotoxicosis. Obstet Gynecol. 2002;99:1040-1043.
Weber G, Ielo V, Vigone MC, et al. Neonatal hyperthyroidism: report of eight cases. Ital J Pediatr. 2001;27:757.