Chapter 609 Bell Palsy
Bell palsy is an acute unilateral facial nerve palsy that is not associated with other cranial neuropathies or brainstem dysfunction. It is a common disorder at all ages from infancy through adolescence and usually develops abruptly about 2 wk after a systemic viral infection. The preceding infection is caused by the herpes simplex virus, varicella-zoster virus, Epstein-Barr virus, Lyme disease, mumps virus, or Mycoplasma (Table 609-1). Active or reactivation of herpes simplex or varicella-zoster virus may be the most common cause of Bell palsy (Fig. 609-1). The disease is occasionally a postinfectious allergic or immune demyelinating facial neuritis. It also may be a focal toxic or inflammatory neuropathy and has been associated with ribavirin and interferon-α therapy for hepatitis C.
Table 609-1 ETIOLOGIES OF ACUTE PERIPHERAL FACIAL PALSY
COMMON
LESS COMMON INFECTIONS
OTHER LESS COMMON CONDITIONS
* Implicated in idiopathic Bell palsy.
† Noncaseating granulomas with facial (lips, eyelids) edema, recurrent alternating facial paralysis, family history, migraines, or headaches.
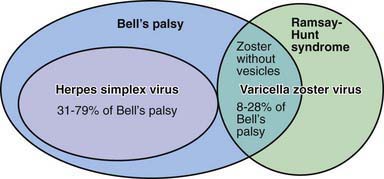
Figure 609-1 Involvement of herpes simplex and varicella zoster viruses in acute facial palsy.
(From Hato N, Murakami S. Gyo K: Steroid and antiviral treatment for Bell’s palsy, Lancet 371:1818–1820, 2008.)
Clinical Manifestations
The upper and lower portions of the face are paretic, and the corner of the mouth droops. Patients are unable to close the eye on the involved side and can develop an exposure keratitis at night. Taste on the anterior 2/3 of the tongue is lost on the involved side in about 50% of cases; this finding helps to establish the anatomic limits of the lesion as being proximal or distal to the chorda tympani branch of the facial nerve. Numbness and paresthesias do not usually occur, but ipsilateral numbness of the face is reported in a few cases and probably is due to viral (especially herpes) or postviral immunologic impairment of the trigeminal and the facial nerves. Several grading systems have been devised for Bell palsy, including the Sunnybrook, House-Brackmann, and Yanagihara systems.
Treatment
Oral prednisone (1 mg/kg/day for 1 wk, followed by a 1-wk taper) started within the first 3-5 days results in improved outcome and is a traditional treatment. Because of the recovery of herpes simplex virus in the neural fluid of the 7th nerve, some also recommend adding oral acyclovir or valacyclovir to the prednisone therapy. Alone, antiviral agents are not effective in reducing adverse sequelae (synkinesis, autonomic dysfunction) but added to prednisone may be associated with an additional small benefit for a complete recovery. Surgical decompression of the facial canal, theoretically to provide more space for the swollen facial nerve, is not of value. Physiotherapy to the facial muscles is recommended in some chronic cases with poor recovery, but the efficacy of this treatment is uncertain. Protection of the cornea with methylcellulose eyedrops or an ocular lubricant is especially important at night. Some plastic surgeons use botulinum toxin to treat chronic unilateral ptosis, but this has little application in pediatric patients.
Prognosis
The prognosis is excellent. More than 85% of patients recover spontaneously with no residual facial weakness. Another 10% have mild facial weakness as a sequela, and only 5% are left with permanent severe facial weakness. In patients who do not recover within a few weeks (chronic), electrophysiologic examination of the facial nerve helps to determine the degree of neuropathy and regeneration. In chronic cases, other causes of facial neuropathy should be considered, including facial nerve tumors such as schwannomas and neurofibromas, infiltration of the facial nerve by leukemic cells or by a rhabdomyosarcoma of the middle ear, brainstem infarcts or tumors, and traumatic injury of the facial nerve.
Facial Palsy at Birth
Facial palsy at birth is usually a compression neuropathy from forceps application during delivery and recovers spontaneously in a few days or weeks in most cases. Congenital absence of the depressor angularis oris muscle causes facial asymmetry, especially when an affected infant cries, and is often associated with other congenital anomalies, especially of the heart. It is not a facial nerve lesion but is a cosmetic defect that does not interfere with feeding. Infants with Möbius syndrome can have bilateral or, less commonly, unilateral facial palsy; this syndrome is usually caused by symmetric calcified infarcts in the tegmentum of the pons and medulla oblongata during mid-gestation or late fetal life, although it rarely is a developmental anomaly of the brainstem.
De Almeida JR, Khabori MA, Guyatt GH, et al. Combined corticosteroid and antiviral treatment for Bell palsy. JAMA. 2009;302:985-993.
Eidlitz-Markus T, Gilai A, Mimouri M, et al. Recurrent facial nerve palsy in pediatric patients. Eur J Pediatr. 2001;160:659-663.
Furuta Y, Ohtani F, Aizawa, et al. Varicella-zoster virus reactivation is an important cause of acute peripheral facial paralysis in children. Pediatr Infect Dis J. 2005;24:97-101.
Hato N, Murakami S, Gyo K. Steroid and antiviral treatment for Bell’s palsy. Lancet. 2008;371:1818-1820.
Madhok V, Falk G, Fahey T, Sullivan. Prescribe prednisolone alone for Bell’s palsy diagnosed within 72 hours of symptom onset. BMJ. 2009;338:410-411.
Salinas RA, Alvarez G, Ferreira J: Corticosteroids for Bell’s palsy (idiopathic facial paralysis), Cochrane Database Syst Rev (4):CD001942, 2004.
Steiner JF. Treatment of Bell palsy—translating uncertainty into practice. JAMA. 2009;302:1003-1004.
Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med. 2007;357:1598-1607.