Chapter 624 Childhood Glaucoma
Glaucoma is a general term used to indicate damage to the optic nerve with visual field loss that is caused by or related to elevated pressure within the eye. It is classified according to the age of the patient at presentation and the association of other ocular or systemic conditions. Glaucoma that begins within the first 3 yr of life is called infantile (congenital); glaucoma that begins between the ages of 3 and 30 yr is called juvenile.
Primary glaucoma indicates that the cause is an isolated anomaly of the drainage apparatus of the eye (trabecular meshwork). More than 50% of infantile glaucoma is primary. In secondary glaucoma, other ocular or systemic abnormalities are associated, even if a similar developmental defect of the trabecular meshwork is also present. Primary infantile glaucoma occurs with an incidence of 0.03% (see Table 624-1 on the Nelson Textbook of pediatrics website at www.expertconsult.com).
Table 624-1 PRIMARY AND SECONDARY CHILDHOOD GLAUCOMAS
I.PRIMARY GLAUCOMAS
II.SECONDARY GLAUCOMAS
Adapted from Nelson LB: Harley’s pediatric ophthalmology, ed 4, Philadelphia, 1998, WB Saunders, p 294.
Clinical Manifestations
The symptoms of infantile glaucoma include the classic triad of epiphora (tearing), photophobia (sensitivity to light), and blepharospasm (eyelid squeezing) (Fig. 624-1). Each can be attributed to corneal irritation. Only about 30% of affected infants demonstrate the classic symptom complex. Signs of glaucoma include corneal edema, corneal and ocular enlargement, and conjunctival injection (Fig. 624-2).
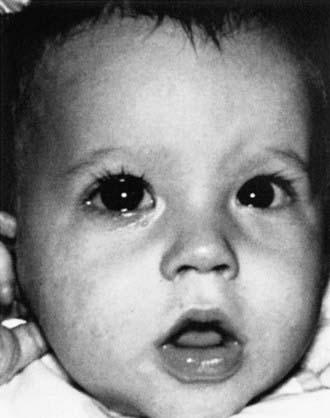
Figure 624-1 Tearing of the right eye caused by glaucoma. Note the increased corneal diameter of the right eye.
(From Nelson LB: Harley’s pediatric ophthalmology, ed 4, Philadelphia, 1998, WB Saunders, p 285.)

The sclera and cornea are more elastic in early childhood than later in life. An increase in intraocular pressure (IOP), therefore, leads to an expansion of the globe, including the cornea, and the development of buphthalmos (“ox eye”). If the cornea continues to enlarge, breaks occur in the endothelial basement membrane (Desçemet membrane) and can lead to permanent corneal scarring. These breaks in Desçemet membrane (Haab striae) are visible as horizontal edematous lines that cross or curve around the central cornea. They rarely occur beyond 3 yr of age or in corneas <12.0 mm in diameter. The cornea also becomes edematous and cloudy, with increased IOP. The corneal edema leads to tearing and photophobia. Glaucoma should be considered in a child in whom a nasolacrimal duct obstruction is suspected if any of these other signs or symptoms are present.
Children with unilateral glaucoma generally present early because the difference in the corneal size between the eyes can be noticed. When the disease is bilateral, parents might not recognize the increased corneal size. Many parents view the large eyes as attractive and do not seek help until other symptoms develop.
Cupping of the optic nerve head is detected by ocular examination. The optic nerve of an infant is easily distended by excessive pressure. Deep, central cupping readily occurs and can regress with normalization of pressure.
Some infants and children with early-onset glaucoma have more extensive maldevelopment of the anterior segment of the eye. The neurocristopathies comprise a spectrum of conditions relating to abnormal embryologic development of the anterior segment. They are usually bilateral and can include abnormalities of the iris, cornea, and lens. Other ocular anomalies that may be associated with glaucoma in infants and children are aniridia, cataract, spherophakia, and ectopia lentis. Glaucoma can also develop secondary to persistent hyperplastic primary vitreous or retinopathy of prematurity.
Trauma, intraocular hemorrhage, ocular inflammatory disease, and intraocular tumor are also important causes of glaucoma in the pediatric population. Systemic disorders associated with glaucoma in infants and children are Sturge-Weber syndrome, neurofibromatosis, Lowe syndrome, Marfan syndrome, congenital rubella, and a number of chromosomal syndromes.
Glaucoma is common in children with a history of congenital cataracts. Glaucoma can develop in up to 25% of children who have undergone cataract surgery early in life. The cause of aphakic glaucoma is not known but is thought to be a coexistent anterior chamber deformity. Children treated for cataracts need to be monitored closely for this dreaded complication.
Diagnosis and Treatment
The diagnosis of infantile glaucoma is made on recognition of the signs and symptoms. Although measurement of IOP may be helpful in monitoring treatment response, it is not a vital part of the diagnostic process. Once the diagnosis is established, treatment is started promptly. Unlike adult glaucoma, in which medication is often the first line of therapy, for infantile glaucoma, the treatment is primarily surgical. Procedures used to treat glaucoma in children include surgery to establish a more normal anterior chamber angle (goniotomy and trabeculotomy), to create a site for aqueous fluid to exit the eye (trabeculectomy and seton surgery), or to reduce aqueous fluid production (cyclocryotherapy and cyclophotocoagulation). Many children require several operations to lower and maintain their IOP adequately, and long-term medical therapy may be necessary as well. Patients with multiple ocular abnormalities and those with aphakic glaucoma generally require more surgeries to achieve and maintain adequate IOP control. Although vision may be reduced secondary to glaucomatous optic nerve damage or corneal scarring, amblyopia is the most common cause of loss of vision in these children.
Beck AD, Freedman S, Kammer J, et al. Aqueous shunt devices compared with trabeculectomy with mitomycin-C for children in the first two years of life. Am J Ophthalmol. 2003;136:994-1000.
Carter BC, Plager DA, Neely DE, et al. Endoscopic diode laser cyclophotocoagulation in the management of aphakic and pseudophakic glaucoma in children. J AAPOS. 2007;11:34-40.
Chen TC, Walton DS, Bhatia LS. Aphakic glaucoma after congenital cataract surgery. Arch Ophthalmol. 2004;122:1819-1825.
Coppens G, Stalmans I, Zeyen T, Casteels I. The safety and efficacy of glaucoma medication in the pediatric population. J Pediatr Ophthalmol Strabismus. 2009;46:12-18.
Morad Y, Donaldson CE, Kim YM, et al. The Ahmed drainage implant in the treatment of pediatric glaucoma. Am J Ophthalmol. 2003;135:821-829.
Sidoti PA, Belmonte SJ, Liebmann JM, et al. Trabeculectomy with mitomycin-C in the treatment of pediatric glaucomas. Ophthalmology. 2000;107:422-429.
Simon JW, Mehta N, Simmons ST, et al. Glaucoma after pediatric lensectomy/vitrectomy. Ophthalmology. 1991;98:670-674.