Chapter 631 External Otitis (Otitis Externa)
In an infant, the outer two thirds of the ear canal is cartilaginous and the inner one third is bony. In an older child and adult only the outer one third is cartilaginous. The epithelium is thinner in the bony portion than in the cartilaginous portion, there is no subcutaneous tissue, and epithelium is tightly applied to the underlying periosteum; hair follicles, sebaceous glands, and apocrine glands are scarce or absent. The skin in the cartilaginous area has well-developed dermis and subcutaneous tissue and contains hair follicles, sebaceous glands, and apocrine glands. The highly viscid secretions of the sebaceous glands and the watery, pigmented secretions of the apocrine glands in the outer portion of the canal combine with exfoliated surface cells of the skin to form cerumen, a protective, waxy, water-repellent coating.
The normal flora of the external canal consists mainly of aerobic bacteria and includes coagulase-negative staphylococci, Corynebacterium (diphtheroids), Micrococcus, and, occasionally, Staphylococcus aureus, viridans streptococci, and Pseudomonas aeruginosa. Excessive wetness (swimming, bathing, increased environmental humidity), dryness (dry canal skin and lack of cerumen), the presence of other skin pathology (previous infection, eczema, or other forms of dermatitis), and trauma (digital or foreign body, cotton tip applicators [Q-tips]) make the skin of the canal vulnerable to infection by the normal flora or exogenous bacteria.
Etiology
External otitis (swimmer’s ear, although it can occur without swimming) is caused most commonly by P. aeruginosa, but S. aureus, Enterobacter aerogenes, Proteus mirabilis, Klebsiella pneumoniae, streptococci, coagulase-negative staphylococci, diphtheroids, and fungi such as Candida and Aspergillus also may be isolated. External otitis results from chronic irritation and maceration from excessive moisture in the canal. The loss of protective cerumen may play a role, as may trauma, but cerumen impaction with trapping of water also can cause infection. Inflammation of the ear canal due to herpesvirus, varicella-zoster, other skin exanthems, and eczema also may predispose to external otitis.
Clinical Manifestations
The predominant symptom is acute ear pain, often severe, accentuated by manipulation of the pinna or by pressure on the tragus and by jaw motion. The severity of the pain and tenderness may be disproportionate to the degree of inflammation, because the skin of the external ear canal is tightly adherent to the underlying perichondrium and periosteum. Itching often is a precursor of pain and usually is characteristic of chronic inflammation of the canal or resolving acute otitis externa. Conductive hearing loss may result from edema of the skin and tympanic membrane (TM), serous or purulent secretions, or the canal skin thickening associated with chronic external otitis.
Edema of the ear canal, erythema, and thick, clumpy otorrhea are prominent signs of the acute disease. The cerumen usually is white and soft in consistency, as opposed to its usual yellow color and firmer consistency. The canal often is so tender and swollen that the entire ear canal and TM cannot be adequately visualized, and complete otoscopic examination may be delayed until the acute swelling subsides. If the TM can be visualized, it may appear either normal or opaque. TM mobility may be normal or, if thickened, reduced in response to positive and negative pressure.
Other physical findings may include palpable and tender lymph nodes in the periauricular region, and erythema and swelling of the pinna and periauricular skin. Rarely, facial paralysis, other cranial nerve abnormalities, vertigo, and/or sensorineural hearing loss are present. If these occur, necrotizing (malignant) otitis externa is probable. This invasive infection of the temporal bone and skull base requires immediate culture, intravenous antibiotics, and imaging studies to evaluate the extent of the disease. Surgical intervention to obtain cultures or debride devitalized tissue may be necessary. P. aeruginosa is the most common causative organism of necrotizing otitis externa. Fortunately, this disease is rare in children and is seen only in association with immunocompromise or severe malnourishment. In adults it is associated with diabetes mellitus.
Diagnosis
Diffuse external otitis may be confused with furunculosis, otitis media (OM), and mastoiditis. Furuncles occur in the lateral hair-bearing part of the ear canal; furunculosis usually causes a localized swelling of the canal limited to 1 quadrant, whereas external otitis is associated with concentric swelling and involves the entire ear canal. In OM, the TM may be perforated, severely retracted, or bulging and immobile; hearing usually is impaired. If the middle ear is draining through a perforated TM or tympanostomy tube, secondary external otitis may occur; if the TM is not visible owing to drainage or ear canal swelling, it may be difficult to distinguish acute OM with drainage from an acute external otitis. Pain on manipulation of the auricle and significant lymphadenitis are not common features of OM, and these findings assist in the differential diagnosis. In some patients with external otitis, the periauricular edema is so extensive that the auricle is pushed forward, creating a condition that may be confused with acute mastoiditis and a subperiosteal abscess; in mastoiditis, the postauricular fold is obliterated, whereas in external otitis the fold is usually better preserved. In acute mastoiditis, a history of OM and hearing loss is usual; tenderness is noted over the mastoid and not on movement of the auricle; and otoscopic examination may show sagging of the posterior canal wall.
Referred otalgia may come from disease in the paranasal sinuses, teeth, pharynx, parotid gland, neck and thyroid, and cranial nerves (trigeminal neuralgia) (herpes simplex virus, varicella zoster virus).
Treatment
Topical otic preparations containing neomycin (active against gram-positive organisms and some gram-negative organisms, notably Proteus spp.) with either colistin or polymyxin (active against gram-negative bacilli, notably Pseudomonas spp.) and corticosteroids are highly effective in treating most forms of acute external otitis. Newer preparations of eardrops (e.g., ofloxacin, ciprofloxacin) are preferable and do not contain potentially ototoxic antibiotics. If canal edema is marked, the patient may need referral to a specialist for cleaning and possible wick placement. An otic antibiotic and corticosteroid eardrop is often recommended. A wick can be inserted into the ear canal and topical antibiotics applied to the wick 3 times a day for 24-48 hr. The wick can be removed after 2-3 days, at which time the edema of the ear canal usually is markedly improved, and the ear canal and TM are better seen. Topical antibiotics are then continued by direct instillation. When the pain is severe, oral analgesics (e.g., ibuprofen, codeine) may be necessary for a few days. Careful evaluation for underlying conditions should be undertaken in patients with severe or recurrent otitis externa. An approach to management is noted in Figure 631-1.
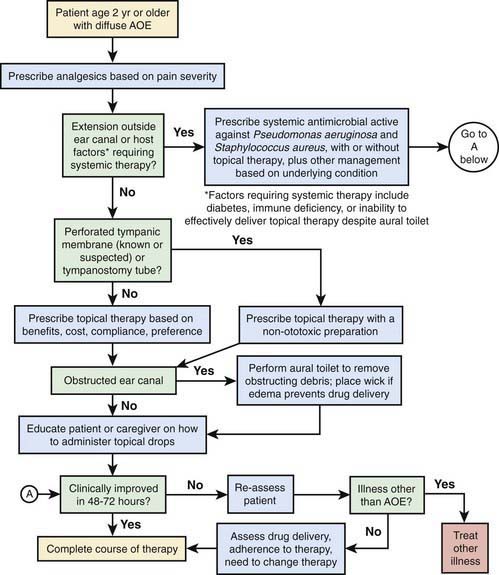
Figure 631-1 Flowchart for managing acute otitis externa (AOE).
(From Rosenfeld RM, Brown L, Cannon CR, et al: Clinical practice guideline: acute otitis externa, Otolaryngol Head Neck Surg 134:S4–S23, 2006.
As the inflammatory process subsides, cleaning the canal with a suction or cotton-tipped applicator to remove the debris enhances the effectiveness of the topical medications. In subacute and chronic infections, periodic cleansing of the canal is essential. In severe, acute external otitis associated with fever and lymphadenitis, oral or parenteral antibiotics may be indicated; an ear canal culture should be done, and empiric antibiotic treatment can then be modified if necessary, based on susceptibility of the organism cultured. A fungal infection of the external auditory canal, or otomycosis, is characterized by fluffy white debris, sometimes with black spores seen; treatment includes cleaning and application of antifungal solutions such as clotrimazole or nystatin; other antifungal agents include m-cresyl acetate 25%, gentian violet 2%, and thimerosal 1:1,000.
Prevention
Preventing external otitis may be necessary for individuals susceptible to recurrences, especially children who swim. The most effective prophylaxis is instillation of dilute alcohol or acetic acid (2%) immediately after swimming or bathing. During an acute episode of otitis externa, patients should not swim and the ears should be protected from excessive water during bathing. A hair dryer may be used to clear moisture from the ear after swimming as a method of prevention.
Other Diseases of the External Ear
Furunculosis
Furunculosis is caused by S. aureus and affects only the hair-containing outer third of the ear canal. Mild forms are treated with oral antibiotics active against S. aureus. If an abscess develops, incision and drainage may be necessary.
Acute Cellulitis
Acute cellulitis of the auricle and external auditory canal usually is caused by group A streptococcus and occasionally by S. aureus. The skin is red, hot, and indurated, without a sharply defined border. Fever may be present with little or no exudate in the canal. Parenteral administration of penicillin G or a penicillinase-resistant penicillin is the therapy of choice.
Perichondritis and Chondritis
Perichondritis is an infection involving the skin and perichondrium of the auricular cartilage; extension of infection to the cartilage is termed chondritis. The ear canal, especially the lateral aspect, also may be involved. Early perichondritis may be difficult to differentiate from cellulitis because both are characterized by skin that is red, edematous, and tender. The main cause of perichondritis/chondritis and cellulitis is trauma (accidental or iatrogenic, laceration or contusion), including ear piercing, especially when done through the cartilage. The most commonly isolated organism in perichondritis and chondritis is P. aeruginosa, although other gram-negative and, occasionally, gram-positive organisms may be found. Treatment involves systemic, often parenteral, antibiotics; surgery to drain an abscess or remove nonviable skin or cartilage may also be needed. Removal of all ear jewelry is mandatory in the presence of infection.
Dermatoses
Various dermatoses (seborrheic, contact, infectious eczematoid, or neurodermatoid) are common causes of inflammation of the external canal; scratching and the introduction of infecting organisms cause acute external otitis in these conditions.
Seborrheic dermatitis is characterized by greasy scales that flake and crumble as they are detached from the epidermis; associated changes in the scalp, forehead, cheeks, brow, postauricular areas, and concha are usual.
Contact dermatitis of the auricle or canal may be caused by earrings, or by topical otic medications such as neomycin, which may produce erythema, vesiculation, edema, and weeping. Poison ivy, oak, and sumac also may produce contact dermatitis. Hair care products have been implicated in sensitive individuals.
Infectious eczematoid dermatitis is caused by a purulent infection of the external canal, middle ear, or mastoid; the purulent drainage infects the skin of the canal, auricle, or both. The lesion is weeping, erythematous, or crusted.
Atopic dermatitis occurs in children with a familial or personal history of allergy; the auricle, particularly the postauricular fold, becomes thickened, scaly, and excoriated.
Neurodermatitis is recognized by intense itching and erythematous, thickened epidermis localized to the concha and orifice of the meatus.
Treatment of these dermatoses depends on the type but should include application of an appropriate topical medication, elimination of the source of infection or contact when identified, and management of any underlying dermatologic problem. In addition to topical antibiotics (or antifungals), topical steroids are helpful if contact dermatitis, atopic dermatitis, or eczematoid dermatitis is suspected.
Herpes Simplex Virus
Herpes simplex virus may appear as vesicles on the auricle and lips. The lesions eventually become encrusted and dry and may be confused with impetigo. Topical application of a 10% solution of carbamide peroxide in anhydrous glycerol is symptomatically helpful. The Ramsay Hunt syndrome (herpes zoster oticus with facial paralysis) may present with herpes vesicles in the ear canal and on the pinna and with facial paralysis and pain. Other cranial nerves may be affected as well, especially the 8th nerve. The current recommended treatment of herpes zoster oticus includes systemic antiviral agents, such as acyclovir, and corticosteroids. As many as 50% of patients with Ramsay Hunt syndrome do not completely recover their facial nerve function.
Bullous Myringitis
Commonly associated with an acute upper respiratory tract infection, bullous myringitis presents as an ear infection with more severe pain than usual. On examination, hemorrhagic or serous blisters (bullas) may be seen on the TM. The disease sometimes is difficult to differentiate from acute OM, because a large bulla may be confused with a bulging TM. The organisms involved are the same as those that cause acute OM, including both bacteria and viruses. Treatment consists of empiric antibiotic therapy and pain medications. In addition to ibuprofen or codeine for severe pain, a topical anesthetic eardrop may also provide some relief. Incision of the bullae, although not necessary, promptly relieves the pain.
Exostoses and Osteomas
Exostoses represent benign hyperplasia of the perichondrium and underlying bone (Chapter 495.2). Those involving the auditory canal tend to be found in people who swim often in cold water. Exostoses are broad-based, often multiple, and bilateral. Osteomas are benign bony growths in the ear canal of uncertain cause (Chapter 495.2). They usually are solitary and attached by a narrow pedicle to the tympanosquamous or tympanomastoid suture line. Both are more common in males; exostoses are more common than osteomas. Surgical treatment is recommended when large masses cause cerumen impaction, ear canal obstruction, or hearing loss.
Haddad JJr. Care of the draining ear in children. Emerg Pediatr. 1995;8:75.
Majumdar S, Wu K, Bateman ND, et al. Diagnosis and management of otalgia in children. Arch Dis Child Educ Pract Ed. 2009;94:33-36.
Nussinovitch M, Rimon A, Volovitz B, et al. Cotton-tip applicators as a leading cause of otitis externa. Int J Pediatr Otorhinolaryngol. 2004;68:433-435.
Roland PS, Belcher BP, Bettis R, et alCipro HC Study Group. A single topical agent is clinically equivalent to the combination of topical and oral antibiotic treatment for otitis externa. Am J Otolaryngol. 2008 Jul–Aug;29(4):255-261.
Roland PS, Eaton DA, Gross RD, et al. Randomized, placebo-controlled evaluation of Cerumenex and Murine earwax removal products. Arch Otolaryngol Head Neck Surg. 2004;130:1175-1177.
Roland PS, Stroman DW. Microbiology of acute otitis externa. Laryngoscope. 2002;112:1166-1177.
Rosenfeld RM, Brown L, Cannon CR, et al. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134:S4-S23.
Siddiq MA, Samra MJ. Otalgia. BMJ. 2008;336:276-277.
Van Balen FAM, Smit WM, Zuithoff PA, et al. Clinical efficacy of three common treatments in acute otitis externa in primary care: randomized controlled trial. BMJ. 2003;327:1201-1203.
Wall GM, Stroman DW, Roland PS, et al. Ciprofloxacin 0.3%/dexamethasone 0.1% sterile otic suspension for the topical treatment of ear infections. Pediatr Infect Dis J. 2009;28:141-144.