Chapter 664 Growth and Development
Growth patterns and development in children are often unique to the individual child. Statistically, normal is defined as 95% of a population that falls within 2 standard deviations of the mean from any given measurement.
Terms to describe some common deviations from normal are listed in Table 664-1. Congenital anomalies can be categorized into production problems and packaging problems. Production problems include abnormalities caused by malformation, dysplasia, or disruption that will not spontaneously resolve. Packaging problems include deformations caused by mechanical causes including in utero positioning and molding, and they usually resolve with time.
Table 664-1 TERMINOLOGIES FOR DEVIATIONS
| TERMINOLOGY | DESCRIPTION |
|---|---|
| Congenital | Anomaly that is apparent at birth |
| Deformation | A normally formed structure that is pushed out of shape by mechanical forces |
| Deformity | A body part altered in shape from normal, outside the normal range |
| Developmental | A deviation that occurs over time; one that might not be present or apparent at birth |
| Disruption | A structure undergoing normal development that stops developing or is destroyed or removed |
| Dysplasia | A tissue that is abnormal or wrongly constructed |
| Malformation | A structure that is wrongly built; failure of embryologic development or differentiation resulting in abnormal or missing structures |
In Utero Positioning
In utero positioning produces temporary joint and muscle contractures and affects the torsional alignment of the long bones, particularly those of the lower extremities. Normal full-term newborns can have up to 20-30-degree hip and knee flexion contractures. These contractures tend to resolve by 4-6 mo of age. The newborn hip externally rotates in extension up to 80-90 degrees and has limited internal rotation to ∼0-10 degrees. The lower leg often has inward rotation (internal tibial torsion). The face may also be distorted; the spine and upper extremities are less affected by the in utero position. The effects of in utero positioning, therefore, are physiologic in origin and resolve by 3-4 mo of age.
Growth and Development
Consideration of growth and development helps to formulate treatment strategies designed to preserve or restore normal growth potential. Growth is subject to many variables including genetics, nutrition, general health, endocrine status, mechanical forces, and physiologic age. Growth also varies between 2 anatomic regions and even between 2 bones of the same region.
Bone formation or ossification occurs in 2 different ways. In endochondral ossification, mesenchymal cells undergo chondrogenesis to form cartilage that matures to become bone. Most bones in the axial and appendicular skeleton are formed in this manner. In intramembranous ossification, osteoblasts are formed by direct differentiation of mesenchymal cells into bone. Flat bones of the skull and clavicle are examples of this pattern of bone formation.
Centers of Ossification
At the beginning of the fetal period the chondrocytes in the midshaft of the long bones form the primary centers of growth from which the bone eventually lengthens. Secondary centers of ossification appear in the chondroepiphysis and mostly appear postnatally. They direct the formation of bone throughout growth, particularly joint development. The ossification centers that are typically present at birth are the distal femur, proximal tibia, calcaneus, and talus.
Anatomic Locations: Descriptive Terms
Typical long bones are divided into the physis, eiphysis, metaphysis, diaphysis, and perichondrial ring (Fig. 664-1). The physis is the growth plate located at the end of bone. The epiphysis is typically a secondary ossification center that contributes to joint development. The metaphysis is the bone adjacent to the physis on the side away from the joint. The diaphysis is the central part or shaft of long bones. The perichondrial ring contributes to appositional growth.
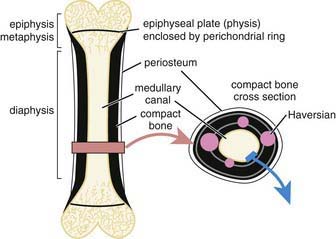
The articular cartilage also contributes to the growth of the epiphysis. The perichondrial ring, which surrounds the physes, and the perichondrium around the epiphyses and periosteum, which surrounds the metaphysis and diaphyseal regions of the bone, contribute to appositional or circumferential growth. Bones without physes (pelvis, scapulae, carpals, tarsals) grow by appositional bone growth from their surrounding perichondrium and periosteum. Other bones (metacarpals, metatarsals, phalanges, spine) grow by a combination of appositional and endochondral ossification.
Important Growth and Developmental Milestones
Some important musculoskeletal growth considerations are summarized in Table 664-2.
Table 664-2 SKELETAL GROWTH CONSIDERATIONS
Growth Patterns in Upper and Lower Extremities
The upper extremity grows longitudinally, primarily from physes of the proximal humeral physis and the distal radial and ulnar physes. In the lower extremity, most of the longitudinal growth occurs around the knee, in the distal femoral and the proximal tibial physes (Fig. 664-2).
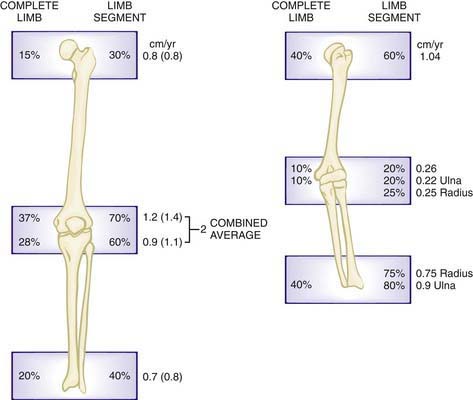
Figure 664-2 The contribution (%) of each physis to the overall length of the extremities.
(From Morrissy R, Weinstein S, editors: Lovell and Winter’s pediatric orthopedics, ed 5, Philadelphia, 2001, Lippincott Williams & Wilkins.)
In the hip joint, the acetabulum forms with the convergence of three primary ossification centers: ischium, ilium, and pubis.
Gait Maturation
Central nervous system maturation contributes significantly to the development of gait. In early ambulation (at 8-15 months), the child usually has a wide-based gait with hyperflexion of hips and knees, and initial contact with the heel. By the age of 2 yr, the wide gait diminishes, reciprocal arm swing begins, and there is increased stride length and velocity. Adult fluid gait patterns usually start developing by 3 yr and officially mature to an adult-like pattern by age 7 yr.
Ballock RT, O’Keefe RJ. The biology of the growth plate. J Bone Joint Surg Am. 2003;85:715-726.
Davids JR. Normal gait and assessment of gait disorders. In: Morrissy R, Weinstein S, editors. Lovell and Winter’s pediatric orthopedics. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2001:131-156.
Dimeglio A. Growth in pediatric orthopedics. In: Morrissy R, Weinstein S, editors. Lovell and Winter’s pediatric orthopedics. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2001:33-62.
Frick SL. Normal growth and development in pediatric orthopedics. In: Dormans JP, editor. Pediatric orthopedics: core knowledge in orthopedics. Philadelphia: Mosby; 2005:1-14.
Ogden J. Anatomy and physiology of skeletal development. In: Catterall A, editor. Skeletal injury in the child. ed 3. New York: Springer-Verlag; 2000:1-37.
Song KM, Little DG. Peak height velocity as a maturity indicator for males with idiopathic scoliosis. J Pediatr Orthop. 2000;20:286-288.
Westh RN, Menelaus MB. A simple calculation for the timing of the epiphyseal arrest. J Bone Joint Surg Br. 1981;63:117-119.