Chapter 686 Disorders Involving Cartilage Matrix Proteins
Functional disturbances of cartilage matrix proteins result in several bone and joint disorders. They fall into five groups corresponding primarily to the defective proteins: three collagens and the noncollagenous proteins COMP (cartilage oligomeric matrix protein), matrilin 3, and aggrecan. The clinical phenotypes differ between and within the groups, especially the spondyloepiphyseal dysplasia (SED) group. In some groups, there is substantial variation in clinical severity.
Spondyloepiphyseal Dysplasias
The term spondyloepiphyseal dysplasia refers to a heterogeneous group of disorders characterized by shortening of the trunk and, to a lesser extent, the limbs. Severity ranges from achondrogenesis type II to the slightly less severe hypochondrogenesis (these two types are lethal in the perinatal period) to SED congenita and its variants, including Kniest dysplasia (which are apparent at birth and are usually nonlethal), to late-onset SED (which might not be detected until adolescence or later). The radiographic hallmarks are abnormal development of the vertebral bodies and of epiphyses, the extent of which corresponds to the clinical severity. Most of the SEDs result from heterozygous mutations of COL2A1; they are autosomal dominant disorders. The mutations are dispersed throughout the gene; there is a poor correlation between the mutation’s location and the resultant clinical phenotype. For familial cases, prenatal diagnosis is possible if the mutation is identified. Schimke immuno-osseous dysplasia may be an exception because it is an autosomal recessive disorder characterized by short stature, hyperpigmented macules, unusual facies, proteinuria and progressive renal failure, cerebral ischemia, and a T-cell defect with lymphopenia and recurrent infections.
Lethal Spondyloepiphyseal Dysplasias
Achondrogenesis type II (OMIM 200610) is characterized by severe shortening of the neck and trunk and especially the limbs and by a large, soft head. Fetal hydrops and prematurity are common; infants are stillborn or die shortly after birth. Hypochondrogenesis (OMIM 200610) refers to a clinical phenotype intermediate between achondrogenesis type II and SED congenita. It is typically lethal in the newborn period.
The severity of radiographic changes correlates with the clinical severity (Fig. 686-1). Both conditions produce short, broad tubular bones with cupped metaphyses. The pelvic bones are hypoplastic, and the cranial bones are not well mineralized. The vertebral bodies are poorly ossified in the entire spine in achondrogenesis type II and in the cervical and sacral spine in hypochondrogenesis. The pedicles are ossified in both.

Spondyloepiphyseal Dysplasia Congenita
The phenotype of this group, SED congenita (OMIM 183900), is apparent at birth. The head and face are usually normal, but a cleft palate is common. The neck is short and the chest is barrel shaped (Fig. 686-2). Kyphosis and exaggeration of the normal lumbar lordosis are common. The proximal segments of the limbs are shorter than the hands and feet, which often appear normal. Some infants have clubfoot or exhibit hypotonia.
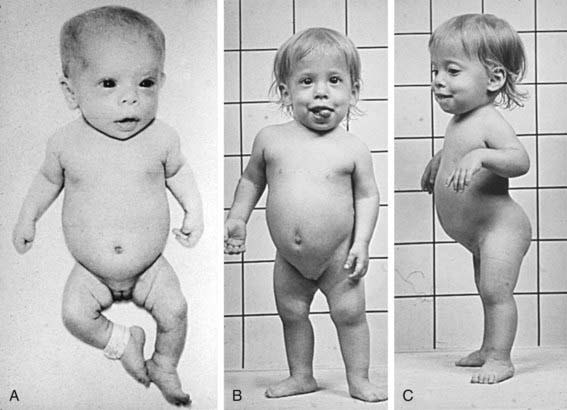
Figure 686-2 Spondyloepiphyseal dysplasia congenita is shown in infancy (A) and early childhood (B, C). Note the short extremities, relatively normal hands, flat facies, and exaggerated lordosis.
Skeletal radiographs of the newborn reveal short tubular bones, delayed ossification of vertebral bodies, and proximal limb bone epiphyses (Fig. 686-3). Hypoplasia of the odontoid process, a short, square pelvis with a poorly ossified symphysis pubis, and mild irregularity of metaphyses are apparent.

Figure 686-3 Radiograph of spondyloepiphyseal dysplasia congenita pelvis demonstrating squared pelvis, hypoplastic capital femoral epiphyses, and femoral necks that are wide and short.
Infants usually have normal developmental milestones; a waddling gait typically appears in early childhood. Childhood complications include respiratory compromise from spinal deformities and spinal cord compression due to cervicomedullary instability. The disproportion and shortening become progressively worse with age, and adult heights range from 95 to 128 cm. Myopia is typical; adults are predisposed to retinal detachment. Precocious osteoarthritis occurs in adulthood and requires surgical joint replacement.
Kniest Dysplasia
The Kniest dysplasia variant of SED (OMIM 156550) manifests at birth with a short trunk and limbs associated with a flat face, prominent eyes, enlarged joints, cleft palate, and clubfoot. Radiographs show vertebral defects and short tubular bones with epiphyseal irregularities and metaphyseal enlargement that gives rise to a dumbbell appearance.
Motor development is often delayed because of the joint deformities, although intelligence is normal. Hearing loss and myopia commonly develop during childhood, and retinal detachment can occur as a late complication. Joint enlargement progresses during childhood and becomes painful; it is accompanied by flexion contractures and muscle atrophy, which may be incapacitating by adolescence.
Late-Onset Spondyloepiphyseal Dysplasia
Late-onset spondyloepiphyseal dysplasia is a mild to very mild clinical phenotype characterized by slightly short stature associated with mild epiphyseal and vertebral abnormalities on radiographs. It is typically detected during childhood or adolescence but can go unrecognized until adulthood when precocious osteoarthritis appears. This designation is nosologically distinct from SED tarda, which is clinically similar but results from mutation of the X-linked gene SEDL.
Aggrecan-Related Spondyloepiphyseal Dysplasias
Mutations of aggrecan have been detected in two SED-like conditions. SED-Kimberley is relatively mild, with short stature, stocky build, and early onset osteoarthritis of weight-bearing joints. A more severe and generalized clinical phenotype with characteristic radiographic changes including widened metaphyses is observed in SEMD-Aggrecan type.
Stickler Dysplasia (Hereditary Osteoarthro-Ophthalmopathy)
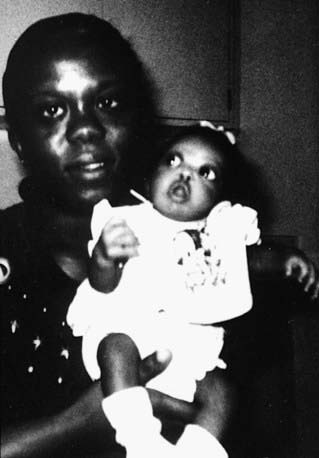
Short stature is not a feature of Stickler dysplasia (OMIM 184840). It resembles SED because of its joint and eye manifestations. Mutations of genes encoding type XI collagen, which functionally interacts with type II collagen, have been identified in Stickler-like disorders (OMIM 184840, OMIM 215150). Stickler dysplasia is often identified in the newborn because of cleft palate and micrognathia (Pierre Robin anomaly, Chapter 303). Infants typically have severe myopia and additional ophthalmologic complications, including choroidoretinal and vitreous degeneration; retinal detachment is common during childhood (Fig. 686-4). Sensorineural hearing loss can arise during adolescence, which is when symptoms of osteoarthritis can also begin. Special attention must be given to the eye complications even in childhood.
Schmid Metaphyseal Dysplasia
Schmid metaphyseal dysplasia (OMIM 156500) is one of several chondrodysplasias in which metaphyseal abnormalities dominate the radiographic features. It typically manifests in early childhood with mild short stature, bowing of the legs, and a waddling gait (Fig. 686-5). Joints, such as the wrist, may be enlarged. Radiographs show flaring and irregular mineralization of the metaphyses of tubular bones of the proximal limbs (Fig. 686-6). Coxa vara is usually present and can require surgical correction. Short stature becomes more evident with age and affects the lower extremities more than the upper extremities; the manifestations are limited to the skeleton.

Figure 686-5 Female patient with metaphyseal dysplasia, type Schmid. The facies are normal and stature is mildly reduced. Mild tibia vara is present.

Figure 686-6 Radiograph of lower extremities in Schmid metaphyseal dysplasia showing short tubular bones and metaphyseal flaring and irregularities, abnormal capital femoral epiphyses, and femoral necks. The epiphyses are normal. Coxa vara is present.
Schmid metaphyseal chondrodysplasia is due to heterozygous mutations of the gene encoding type X collagen; it is an autosomal dominant trait. The distribution of type X collagen is restricted to the region of growing bone in which cartilage is converted into bone. This might explain why radiographic changes are confined to the metaphyses.
Pseudoachondroplasia and Multiple Epiphyseal Dysplasia
Pseudoachondroplasia (OMIM 177170) and multiple epiphyseal dysplasia (MED) (OMIM 600969) are two distinct phenotypes that are grouped together because they result from mutations of the gene encoding COMP. The mutations are heterozygous in both; they are autosomal dominant traits. The clinical phenotypes are restricted to skeletal tissues.
Newborns with pseudoachondroplasia are average in size and appearance. Gait abnormalities and short stature mainly affect the limbs and become apparent in late infancy. The short stature becomes marked as the child grows and is associated with generalized joint laxity (Fig. 686-7). The hands are short, broad, and deviated in an ulnar direction; the forearms are bowed. Developmental milestones and intelligence are usually normal. Lumbar lordosis and deformities of the knee develop during childhood; the latter often requires surgical correction. Pain is common in weight-bearing joints during childhood and adolescence, and osteoarthritis develops late in the 2nd decade of life. Adults range in height from 105 to 128 cm.
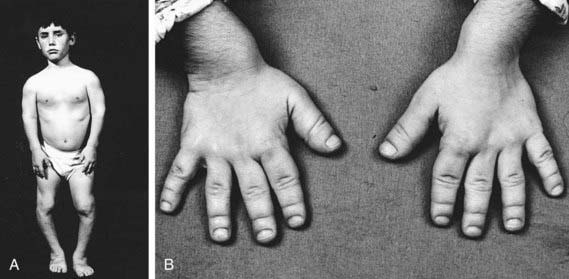
Figure 686-7 A, Pseudoachondroplasia in an adolescent boy. The facies and head circumference are normal. There is shortening of all extremities and bowing of the lower extremities. B, Photograph of hands, demonstrating short stubby fingers.
Skeletal radiographs show distinctive abnormalities of vertebral bodies and of both epiphyses and metaphyses of tubular bones (Fig. 686-8).

Figure 686-8 A, Lateral thoracolumbar spine radiograph of a patient with pseudoachondroplasia showing central protrusion (tonguing) of the anterior aspect of upper lumbar and lower thoracic vertebrae. Note reduced vertebral body heights (platyspondyly) and secondary lordosis. B, Lower extremity radiograph of patient with pseudoachondroplasia showing large metaphyses, poorly formed epiphyses, and marked bowing of the long bones.
The MED phenotype has skeletal abnormalities that predominantly affect the epiphyses as noted on radiographs. Two classic forms are a severe Fairbank type and a mild Ribbing type. Because of overlap in clinical features and because COMP mutations are found in both types, they may be considered clinical variants.
The more severe clinical phenotype has its onset during childhood, with mild short-limbed short stature, pain in weight-bearing joints, and a waddling gait. Radiographs show delayed and irregular ossification of epiphyses. In more mildly affected patients the disorder might not be recognized until adolescence or adulthood. Radiographic changes may be limited to the capital femoral epiphyses. In the latter case, mild MED must be distinguished from bilateral Legg-Calvé-Perthes disease (Chapter 670.3). Precocious osteoarthritis of hips and knees is the major complication in adults with MED. Adult heights range from 136 to 151 cm.
There are families with clinical and radiographic manifestations of MED that are not due to mutations of COMP. Some are linked to the gene encoding one of the type IX collagen chains. It has been suggested that COMP and type IX collagen interact functionally in cartilage matrix, thus explaining why mutations of different genes produce similar pictures. Mutations of the genes coding for another cartilage matrix protein, matrilin 3, and the diastrophic dysplasia sulfate transporter have also been found in patients with MED. For familial cases of pseudoachondroplasia and MED resulting from mutation in COMP, prenatal diagnosis is available.
Boerkoel CF, O’Neill S, Andre JL, et al. Manifestations and treatment of Schimke immuno-osseous dysplasia: 14 new cases and a review of the literature. Eur J Pediatr. 2000;159:1-7.
Horton WA, Hecht JT. Chondrodysplasias: disorders of cartilage matrix proteins. In: Royce PM, Steinmann B, editors. Connective tissue and its heritable disorders. New York: Wiley-Liss; 2002:909-938.
Kennedy J, Jackson G, Ramsden S, et al. Comp mutation screening as an aid for the clinical diagnosis and counselling of patients with a suspected diagnosis of pseudoachondroplasia or multiple epiphyseal dysplasia. Eur J Hum Genet. 2005;13:547-555.
Kennedy J, Jackson GC, Barker FS, et al. Novel and recurrent mutations in the c-terminal domain of comp cluster in two distinct regions and result in a spectrum of phenotypes within the pseudoachondroplasia—multiple epiphyseal dysplasia disease group. Hum Mutat. 2005;25:593-594.
Tompson SW, Merriman B, Funari VA, et al. A recessive skeletal dysplasia, semd aggrecan type, results from a missense mutation affecting the c-type lectin domain of aggrecan. Am J Hum Genet. 2009;84:72-79.
Unger S, Bonafe L, Superti-Furga A. Multiple epiphyseal dysplasia: clinical and radiographic features, differential diagnosis and molecular basis. Best Pract Res Clin Rheumatol. 2008;22:19-32.