107
Relative Motion Orthoses
The Concepts and Application to Hand Therapy Management of Finger Extensor Tendon Zone III and VII Repairs, Acute and Chronic Boutonnière Deformity, and Sagittal Band Injury
Wyndell H. Merritt,, and Julianne Wright Howell
Simulated Relative Motion Extension or Relative Motion Flexion PENCIL Test
The “pencil test” is a practical way to simulate a relative motion flexion (RMF) or relative motion extension (RME) orthosis. Simply place a pencil or tongue depressor above (RMF) or below (RME) the proximal phalanx of the affected digit and opposite for the neighboring digits and observe while the digit is flexed and extended for the desired response. If the index or small are the affected digit, the pencil can be balanced by weaving it in the same way (above or below) as the affected digit using the central two digits for support. The pencil test is a quick and useful tool to simulate the relative motion positions during hand examination to decide if either position offers the desired response or as an “exercise device” to position the MCP joint in relative flexion–extension or during wide-awake local anesthesia and no tourniquet surgery to guide the choice of orthosis and postoperative instruction details.
3,17,57

The concept of relative motion (RM) is not new; it was proposed in the late 1970s as an idea to mobilize extensor tendon zones V and VI repairs.
1–3
The idea of active finger motion controlled by an orthosis was suggested to minimize the morbidity of tendon adhesions and joint stiffness seen after 4 to 6 weeks of immobilization. The original 1978 RM orthosis design permitted active motion of only the metacarpophalangeal (MCP) joints.
3,4
Over the past 40 years, the orthosis design, concept, and nomenclature have evolved, and use has expanded into therapy management for a variety of hand conditions.
3
RM orthoses have been known by many names, such as the Wyndell Merritt splint,
5–7
immediate controlled active motion (ICAM, an acronym chosen to emphasize that it is active motion rather than dynamically assisted passive motion),
2
yoke splint,
8,9
border digit splint,
10
sagittal band bridge splint,
11,12
and most recently in conversation, the RM orthosis. Today, the preferred terms are relative motion extension (RME) and relative motion flexion (RMF) to highlight the relative position of the affected digit’s MCP joint and minimize confusion.
3,13
The RME and RMF orthoses are finger based; the RME orthosis positions the MCP joint of the affected finger(s) in 15 to 20 degrees more extension relative to that of the neighboring MCP joints, and the RMF orthosis positions the affected digit’s MCP joint(s) in greater flexion relative to that of the neighboring MCP joint(s), which are in 15 to 20 degrees less flexion. RME is widely used after extensor tendon zone IV to VII repair and for surgical and nonsurgical management after sagittal band injury
1,2,11,12,14
(Fig. 107.1). RMF has been advocated to restore balance to the extensor mechanism after acute and chronic boutonnière and after extensor tendon zone III repair
15–17
(Fig. 107.2). Most recently, a scoping review of worldwide experience using the RM concept was published by Hirth and coworkers,
3
who pointed out the versatility of this concept, which can apply to three orthotic purposes: “protective, adaptive and exercise.” This chapter reviews some established and some expanded uses of this concept. The RM concept is attractive because of its small size,
3
low-profile design that is simple and inexpensive to fabricate,
2,7,11,18
less morbidity because of decreased rehabilitation time,
1,2,18–20
early functional hand use,
2,21–23
earlier return to work,
1,2,18–24
improved patient compliance,
3,6
and less financial investment for care.19
The goal of this chapter is to establish the framework for understanding the RM concept. To do so, the authors have included relevant anatomy and biomechanics, clinical studies, illustrations, photos, and videos.
Relative Motion: the Metacarpophalangeal Joint and the “Quadriga Effect”
The Relative Motion concept is simple.
WH Merritt 25
Four types of finger orthoses are commonly described: static, dynamic, serial static, and static progressive.
26
The RM orthosis differs in that it takes advantage of the relationship between a single muscle shared by extrinsic extensor or flexor tendons to use what has been called the “quadriga effect” by positioning the affected digit’s MCP joint in relative extension or flexion to its neighbors for safe early active motion and functional hand use. The RM concept provides a simple management technique that safely permits active finger motion with decreased tension of the repaired or ruptured tendon, thus reducing repair adherence, reducing unfavorable joint capsule and collateral ligament remodeling, and likely increasing the strength of the repair. Understanding the quadriga effect and its application to RME and RMF is important in achieving effective results. Verdan
27
introduced this term for a complication that can occur after single-digit amputation, causing adjacent fingers to lose flexion. He named this the syndrome of the quadriga, resulting when the extensor tendon is sutured to the flexor digitorum profundus (FDP) tendon over an amputation stump. As a result, the performance of the FDP, a single muscle shared by multiple tendons, is hampered by the suture to create a relative length difference between the tendons, placing slack in the adjacent flexor profundi tendons and thus limiting active finger flexion.
Although Verdan’s description was only of profundi tendons to caution surgeons not to suture the extensors to the flexors over an amputated stump, the extensor digitorum communis (EDC) tendons also arise from a single muscle and have multiple juncturae tendinae and intramuscular connections between the four digits, allowing similar quadriga features, evidenced when one attempts to extend the ring finger while in a fisted position.
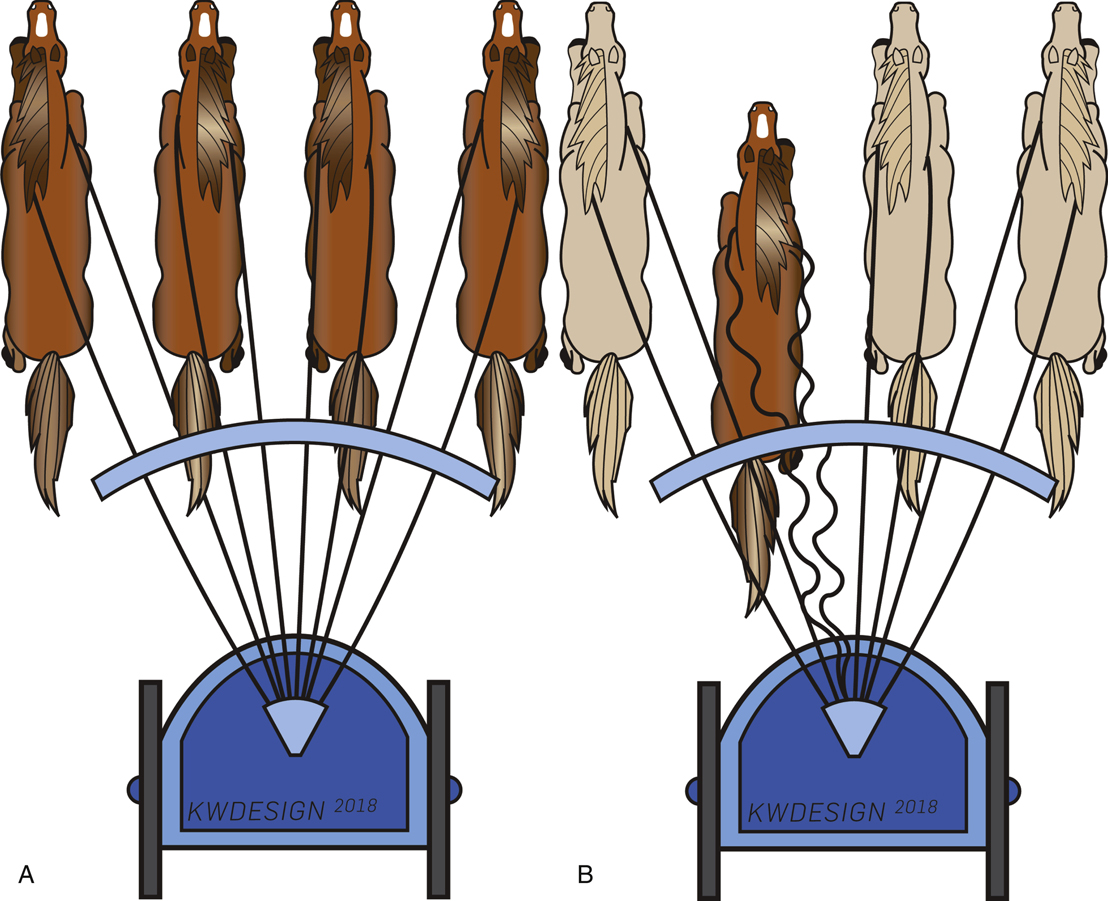
Quadriga is the name the Romans gave their two-wheeled chariot with equidistant reins used by the charioteer to control the four horses during the Roman and Greek Olympic races, explaining Verdan’s choice of terminology (Fig. 107.3A). In the human hand, the charioteer’s body is like the FDP or EDC muscle; the reins of the four horses are compared to the flexor or extensor tendons. To control the horses, the charioteer wraps the reins around his trunk so that with a twist of his body, the harnessed horses are pulled as one.
27
Although Verdan originally described the quadriga effect as an analogy for complications, this relationship can be advantageous. RME applies the principles Verdan described in the flexor profundi to the common extensor to produce a useful extensor “quadriga effect” designed specifically to protect extensor tendon repairs and sagittal band injuries. Although the extensor indicis proprius (EIP) and extensor digitorum minimi (EDM) are not single muscles shared by multiple tendons, management with RME works conceivably because the excursions of the independent extensor tendons match the excursions of the common extensor tendons with all sharing intramuscular and juncturae tendinae connections.
28,29
Sharma and coworkers
30
measured elongation of repaired tendons of cadavers with and without the RME orthosis, validating the protective benefit of the orthosis throughout the full range of motion (ROM) of the fingers, including making a fist. These authors’ results aligned with our clinical experience to confirm that tendon repairs are protected by the relative position of the MCP joints, demonstrating the least amount of elongation was measured in the experimental MCP joint position of RME neutral, and there were also no tendon ruptures in the RME orthosis–protected digits, even with full motion, but the repairs without the orthosis did gap.
30
This protective function of the RME orthosis was easily demonstrated by our 1978 cadaver study using only a “single weak” 6-0 nylon suture for tendon repair and repeated at the 2003 meeting of the American Society of Hand Therapists (ASHT) (Video 107.1). However, it is even more convincing in the emergency department, when under local anesthesia, a “single weak” 6-0 nylon suture is placed in an extensor tendon repair and a tongue depressor is positioned beneath the proximal phalanx to simulate an RME orthosis followed by active flexion and extension of the fingers without rupture.
In the 1978 cadaver study, composite finger and wrist flexion pulled on the single 6-0 nylon suture, although it did not rupture. Therefore, our original recommendation was to immobilize the wrist and interphalangeal (IP) joints, allowing active movement of only the MCP joints within the RME orthosis. Simply stated, the RM concept is all about the relative position of the MCP joints to one another. When the affected digit’s MCP joint is positioned in
relatively more extension, a length difference is created between the repair and its neighbor tendons, resulting in less tension on the repair. As the digits actively flex, the equidistant neighboring tendons, united by their interconnections, pull the shared EDC muscle distally to maintain the “quadriga effect” throughout the ROM. As demonstrated by the chariot analogy, when all reins are the same, equal reining results. If one rein is put on slack (as in a 15- to 20-degrees RME position in humans) when the charioteer pulls the reins, the relatively longer reins predominate, unloading the shorter rein so that the horse on the slack rein remains on lax tension (Fig. 107.3B).
© 2018 JW Howell, PT, MS, CHT.

© 2018 JW Howell, PT, MS, CHT.
© 2018 KW Design. Contact Katie Wright of KW Design; Wright.design.illustration@gmail.com.
Relative Motion Extension
Long Extensor Tendon Lacerations in Zones IV to VII
Before 1980, active finger motion after extensor tendon repair was a bold idea. Subsequent to cadaver observations, the RME orthosis was designed to verify that motion was safe for the repaired extensor tendons. The original edition of the RME orthosis was a finger-based orthosis that positioned the MCP joint of the affected digit in relatively more extension with the IP joints immobilized and was secured to the wrist orthosis with a strap.
3
In the second edition of the RME orthosis, the wrist remained immobilized at 25 to 30 degrees of extension, and all digits were allowed full motion, except the MCP joint of the affected digit, which was positioned in 20 to 25 degrees relatively more extension. In 1986, the RM concept and this second edition orthosis were published in a textbook reviewing advances in tendon management, as a “new approach to splinting extensor tendon zones V-VI.”
19
Robinson and coworkers
21
reported successful use of this new approach in 23 patients at the 1986 meeting of the ASHT. Concurrently, with additional experience and the successful management of many more patients, the third edition of the RME orthosis reduced the MCP joint relative position to 15 to 20 degrees.
1,2
At this same time, RME use was expanded to the management of extensor tendon zones IV and VII and sagittal band repairs.
1,2
The absence of reported secondary surgeries to release adhesions and stiff joints is a direct result of early active motion and early tendon excursion achieved by the RME orthosis.
2,6,7,20,21,33-36
Actual measurements of the amount of tendon excursion permitted by the RME orthosis have not been formally studied. Evans and Burkhalter
35
previously measured normal extensor tendon excursion intraoperatively,
concluding that 30 to 40 degrees of MCP joint flexion produced 5 mm of safe—and what they believed sufficient—extensor tendon excursion to obviate adhesions. Lalonde’s
32
excellent video demonstrates a patient under wide-awake local anesthesia, no tourniquet, technique (WALANT) moving actively through full finger motion except the 15 to 20 degrees limited by the RME orthosis with total excursion measured as 8 mm, exceeding the 5 mm suggested to limit adhesions (Video 107.2). Although much has been written about the strength of various extensor tendon repair techniques and suture material, these seem far less relevant than selecting an orthosis that permits safe early active motion. This notion aligns with the authors’ experiences in that some patients with infected extensor lacerations have been successfully managed with no repair whatsoever; they have been treated with only the RME orthosis.
2,25
The largest clinical series was published in 2005 under the acronym ICAM (immediate controlled active motion) by Howell and associates,
2
who reported on 20 years of experience with the RME and wrist orthoses in 140 patients with 190 extensor tendon zone IV to VII simple (n = 89) and complex (n = 51) injuries. Since that publication, Hirth and associates’
3
scoping review recognized the growing worldwide acceptance of the RM concept, citing six therapy programs that managed a total of 226 patients with both the RME and wrist orthoses and seven programs that used the RME-only orthosis for 145 patients with zone IV to VI repairs. Because usage of the RME-only orthosis without the wrist orthosis is relatively new and various authors have changed some of the original program details, review of these studies is worthwhile
6,7,20,23,24,33-36
(Table 107.1). In one study, the author reports better ROM and fewer extensor lags in the wearers of the RME-only orthosis than those wearing both orthoses.
6
Others instruct patients not to simultaneously fist and flex their wrists to avoid passive tension on the repair.
24
Another used the RME-only orthosis when repairs were distal to the juncturae tendinum in zones IV-V, otherwise these authors used both orthoses when the repair was proximal to the junctura and/or involved the EDM in zones IV to VI.
20
Two case reports confirmed that patients with multi-tissue injuries benefitted from a single orthosis fabricated to combine both the RME and RMF positions for adjacent finger usage, safely avoiding complex trauma complications.
14,16
Since 2005, a count of the global literature for extensor tendon repairs in zones IV to VI by author JWH shows approximately 203 patients with 212 repairs reported in 207 zones have been managed by the RME-only orthosis (see Table 107.1). However, since 2005, 246 patients with 266 tendon repairs reported in 252 zones have been managed with the combined wrist and RME finger orthoses (Table 107.2). Seemingly, the RME-only orthosis is being more extensively used, so these numbers will continue to change as therapists have greater experience using the finger-based orthosis to manage extensor tendon repairs. For now, it is important to keep in mind how the evidence for management of extensor tendon repairs with the RME-only orthosis varies by zone. To date, these reports suggest that zone IV repairs are well protected by the finger orthosis only. The 137 tendon repairs reported for zone V that have been successfully managed suggest that substantial evidence is accumulating. In zone VI, although the RME-only orthosis numbers are growing, program changes made by various authors have affected interpretation, and in zone VII, there is no evidence for use of the RME-only orthosis.
The original ICAM program described for management of zone IV to VII repairs has been altered by the various authors
6,10,20,23,24,33-36
(see Tables 107.1 and 2). A current update to the RME program for management of zone IV to VII extensor tendon repairs has been compiled by the authors in Box 107.1. The one rule, however, that has remained consistent is that at least one EDC or EIP or EDM tendon must remain intact to use the RME program. Most begin using the RME orthosis within 5 to 7 days of repair with inclusion of a wrist orthosis dependent on the zone of injury and therapist’s preference. Some require another orthosis for overnight, and some add a wrist orthosis if an extensor lag is present initially.
10,24,33
In the original ICAM study, workers safely returned to work in an average of 18 days wearing both the RME finger and wrist orthoses, Hirth and colleagues’
2,24
workers returned wearing the RME orthosis only by 3.3 weeks. These early return-to-work times have not been matched, which may be a result of restrictions appended by others to the original ICAM program, such as no driving or light use only. Collocott and coworkers
23
described the dilemma between the employer and the injured worker when the worker is advised to return to work under such provisions of no driving or no more than light duty use, for which the employer has no such work available or orthosis wear is not permitted on the worksite.
Of primary importance, no tendon ruptures have been reported by use of the RME-only orthosis or the combined wrist and finger RME orthoses. There have been only a few minor complications mentioned such as suture irritation, edema, and superficial skin infections, all of which resolved.
2,3,14,20,23,24
The number of therapy sessions has decreased from seven sessions reported in the 2005 ICAM report to four to six sessions.
2,3
Studies that have compared the RME-only orthosis with dynamic, early active motion, and immobilization programs found recovery of ROM substantially easier at 3 to 4 weeks for the RME group. However, by 3 months, all programs had comparable motion.
20,23,24
Measurement of ROM remains the most widely used method for reporting results of extensor tendon repair management. However, because there is no universal grading system or designated time to measure, comparison among studies is difficult.
3
Authors who report on grip strength make comparison with the opposite hand, which show an 85% recovery by week 8 and 100% by week 12.
3
Assessment of patient’s hand function with the Sollerman Hand Function Test has been compared between RME-only orthosis users and those assigned to another early active motion program wearing a wrist–hand–finger static orthosis with the IP joints free. At 1 month after surgery, those wearing the RME-only orthosis had significantly better Sollerman Test and QuickDASH (Disability of the Arm, Shoulder and Hand) scores of function and total active motion and less loss of flexion and at 8 weeks were found more satisfied with the RME-only orthosis.
23
Sagittal Band Injuries and Rupture: Acute and Chronic
The long extensor tendon in zones IV and V over the MCP joint level is maintained in a central position by deep and superficial fibers of the sagittal bands, which arise from the volar plate, flexor tendon sheath, proximal annular pulley, and intermetacarpal ligaments and form a retinacular tunnel that attaches to the extensor hood to stabilize the long extensor tendon during active motion. The MCP joint is extended through this sagittal band lasso noose, lifting up on the proximal phalanx. If this “ring” is broken by sagittal band disruption, the tendon may dislocate to a position between the metacarpal heads, and active extension will fail from the flexed MCP joint position.
Ryan and Murray
37
classified sagittal band injuries into three types, all of which can benefit from RME orthotic management. Type 1 is a contusion without tear or instability of the sagittal band. Type 2 involves tearing of the sagittal band tunnel, sometimes with painful snapping of the extensor tendon but without complete
dislocation. Type 3 consists of tendon dislocation into the groove between the metacarpal heads, most frequently to the ulnar side. Ishizuki
38
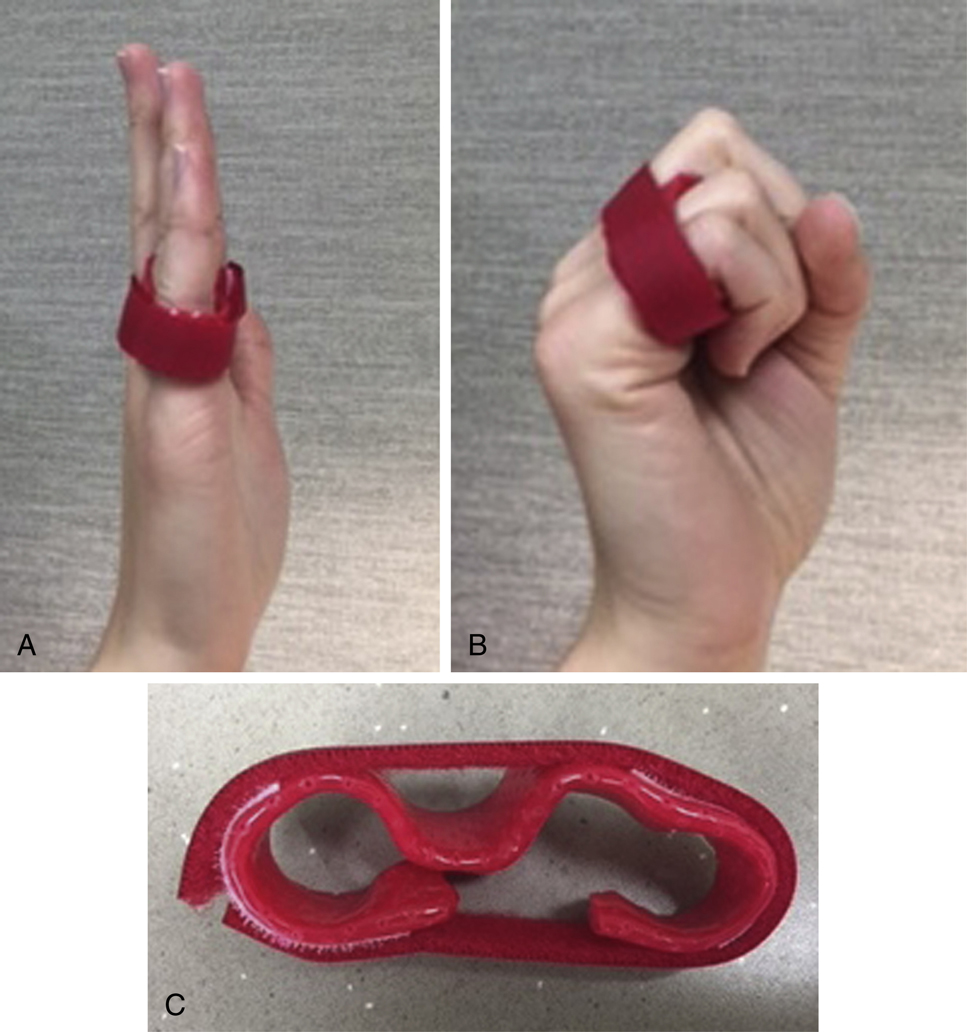
described superficial and deep sagittal band layers, suggesting that spontaneous sagittal band rupture observed in patients with connective tissue disorders might involve only the superficial layer, whereas traumatic dislocation most likely involves both layers. A healing sagittal band is well protected by the RME orthosis only because it prevents the fully flexed MCP joint position that leads to dislocation, maintaining the injured extensor tendon sagittal band complex in a more lax tension than its neighboring digits. The orthosis protectively places the injured or repaired extensor retinacular system as well as the proximal extensor hood on slack (Fig. 107.4). When the RME orthosis is used with the affected digits in relatively more MCP extension, tension from the pull of the EDC is reduced as a result of the “quadriga effect,” allowing for safe active ROM. Contouring the sides of the RME orthosis during fabrication to hug the finger keeps it protected and centralizes the tendon. Use of the RME orthosis during the healing phase allows for the early active motion necessary to limit adhesion formation and to guide remodeling.
1–3,14
TABLE 107.1
| Reference (Year) | Patients (n) | Zone IV | Zone V | Zone VI | Changes to Original ICAM Program, Including No Wrist Orthosis |
|---|---|---|---|---|---|
| Berry et al 6 (2008) | 14 | 1 | 11 | 2 | No further changes |
| Hirth et al 24 (2011) | 23 | — | 21 | 2 |
Added: night WHFO
Advice: no combined finger and wrist flexion
|
| Burns et al 7 (2013) | 2 | — | 2 | — |
Inclusion criteria: only simple injuries
Advice: no heavy lifting in RME orthosis
|
| Izadpanah et al 33 (2015) | 55 | 20 | 30 | 5 | Inclusion criteria: only simple injuries; zone IV proximally only and zone VI to distally only |
| Svens et al 20 (2015) a | 13 | 1 b | 12 b | — |
Orthotic use: 4 wk
|
| Turner 34 (2015) c | 31 | 4 d | 18 d | 9 d |
Added: WHO or WHFO when extensor lag initially present
Inclusion criteria: zone IV proximal only and zone VI to distally only
|
| Collocott 23 (2016) | 22 | — | 15 | 7 |
Added: night WHFO
Inclusion criteria: only simple injuries except 2 digits with multiple repairs in both zones V and VI
Advice: no combined fist and wrist flexion, driving, and specific activities
|
| Pilbeam (C. Pilbeam, written communication March 2018) | 8 | 1 | 7 | 0 |
Inclusion criteria: zones IV and V only
Added: WHO for all EDM and zone VI–VII repairs (see Table 107.2)
|
| Pilbeam (C. Pilbeam, written communication March 2018) | 35 | 11 e | 21 e | 7 e | Added: night splint not routine; added on occasion if extensor lag developed |
| Approximate RME orthosis only(203 patients with 212 tendon repairs reported in 207 zones) | 38 | 137 | 32 |

TABLE 107.2
| Reference (Year) | Patients (n) | Zone IV | Zone V | Zone VI | Author Changes to Original ICAM Program |
|---|---|---|---|---|---|
| Howell et al 2 (2005) | 135 | 4 | 112 | 9 | Not applicable; original ICAM program |
| Berry et al 6 (2008) | 7 | 2 | 3 | 2 | Orthotic use: worn an average of 45 days |
| Blakeway 36 (2013) | 1 | 1 | No changes to original ICAM program | ||
| Altobelli et al 35 (2013) a | 5 | 1 | 5 | Added: night WHFO | |
| Svens et al 20 (2015) b | 50 | 2 | 35 |
12
5
|
Orthotic use: work 6 wk by 45 patients in 49 zones and in 5 zone VI repairs worn 4 wk |
| Pilbeam 18 (2016) c | 25 | 5 | 18 | 2 | Added: prefabricated WHO substituted for custom WHO |
| Pilbeam (2018) d (written communication, March 2018) | 23 | 1 | 8 | 15 | Inclusion criteria: zones VI–VII and all EDM repairs (C) |
| Approximate RME + wrist orthosis(246 patients with 266 tendon repairs reported in 252 zones) | 25 | 182 | 45 |


© 2018 KW Design. Contact Katie Wright of KW Design; Wright.design.illustration@gmail.com.
Acute Sagittal Band Injury
For a patient with a typical acute sagittal band rupture, extension is possible when the EDC tendon is out of the intermetacarpal space and only redevelops when full flexion is attempted. Evidence is variable about how late conservative management can be effective for patients with complete tendon dislocation. Peelman and associates
12
used the RME orthosis after sagittal band rupture and found better success (95%) when patients were treated within 3 weeks of injury and a significant decrease (62%) in success after 6 weeks. The authors’ experience has been that if there is still inflammation present at 6 weeks, there is a better chance for success with this orthosis technique, and when wearing the orthosis, most patients soon reported pain relief. Pain is frequently relieved with use of an RME orthosis as opposed to buddy taping, which has been reported to remain painful even after 1 year of taping.
39
It should be noted that when extensor tendon subluxation is constant and occurs without pain, swelling, or other inflammatory manifestations, nonsurgical measures can be expected to fail.
1
Nonsurgical management of sagittal band injuries with the RME orthosis is relatively new for hand therapists, so a synopsis of the following studies is worth review. Several authors have successfully used a three- or four-finger RME orthosis design to position painful digits in 25 to 35 degrees of relative extension full time for 6 to 8 weeks.
11,12
In one large study of nonrheumatoid patients with sagittal band injury, traumatic or atraumatic onset did not affect the results in the acute (<3 weeks’ onset) and subacute (3–6 weeks’ onset) groups if treatment started within 6 weeks of onset of symptoms. The length of orthotic management ranged from 3 to 16 weeks, with pain resolved in most, although tendon subluxation was not always corrected. There were equal numbers of patients within the traumatic and atraumatic onset groups who eventually chose to have surgery.
12
The trend has been for most reports to exclude
rheumatoid patients from RME orthosis use after sagittal band rupture. However, our experience has been that rheumatoid patients with sagittal band injuries benefit from the RME orthosis when used as “protective” orthoses, provided the sagittal band rupture is the only problem and not accompanied by the presence of MCP joint volar subluxation and ulnar translocation of the flexor tendons. However, when RME orthoses are used as “adaptive” orthoses to improve hand function, even with these coexisting problems, patients with rheumatoid arthritis certainly do benefit.
1,3
In the authors’ experience, the RME program for nonsurgical management of acute sagittal band ruptures should be individualized to each patient, with the relative angle of extension of the affected digit MCP joint determined by observing the stability of the extensor tendon during active motion (Video 107.3). If more stability is needed, the orthosis can be modified by contouring the trough of the orthosis to hug the digit or by widening the volar aspect of the orthosis to reduce the arc of proximal interphalangeal (PIP) joint flexion or include the digit radial to the affected digit until pain and subluxation observed during movement is gone. If these adaptations do not provide the desired stability, a wrist orthosis can be tried to eliminate the destabilizing forces noted to occur during concurrent finger and wrist flexion with ulnar deviation.
39
The RME orthosis provides protective stability, so patients are encouraged to functionally use their hands, and wear should be full time for at least 6 weeks and for some as long as 3 months before surgery is considered. Although not common, some patients unknowingly remove their RME orthoses during sleep, interfering with sagittal band healing. To avoid this, fabrication of a less easily removed orthosis for nighttime wear may be required, or the RME orthosis may be taped to the hand overnight.
Chronic Sagittal Band Injury and Ruptures
Patients with chronic sagittal band ruptures and failed nonsurgical management require surgical reconstruction. The typically published conventional techniques have two common features: (1) to stabilize the ruptured side (usually ulnar) by reefing, grafting, or transferring tendon slips with the proper tension to centralize the tendon and (2) to immobilize the hand for 6 to 10 weeks followed by an intensive therapy program to recover motion. Merritt and coworkers
1
first described the use of the RME orthosis only for chronic sagittal band rupture in an older adult patient with rheumatoid arthritis, who, depending on which way her finger pointed, subluxed the tendon to either the radial or ulnar side, likely because of repeated steroid injections. This obviated the typical reconstruction techniques to stabilize the rupture side, so a juncturae tendinum graft pulley passed through the metacarpal head was used to centralize the EDC. Postoperatively, the dilemma to avoid adherence by means of early motion without rupture was solved by using the RME orthosis for 6 weeks, also permitting functional use of her hand and recovery of normal ROM without further subluxation.
1
Subsequently, 23 patients with similar sagittal band reconstructions have been reported, with equivalent results achieved using various centralized tendon grafts, including half of the flexor carpi ulnaris; half of the EIP; the juncturae tendinum; and most frequently, the palmaris longus, passing the centralized graft through a drill-hole tunnel in the metacarpal head followed by 6 weeks of RME orthosis management.
40
It is likely any of the published techniques for correcting chronic sagittal band rupture can be successfully managed with the RME-only orthosis (
Videos 107.4 and 104.5
).
Relative Motion Flexion
Relative Motion Flexion Orthosis for Boutonnière Deformity: “Winslow’s Diamond”
Boutonnière deformity has remained the most difficult of extensor tendon management problems, with acute injury intervention typically requiring 2 to 4 months out of work and the chronic fixed boutonnière deformity a conundrum that often defies any acceptable correction with current surgical or nonsurgical technique. Chronic deformity occurs largely because when first seen after injury, the deformity is frequently not present, and the diagnosis is not apparent without a careful, knowledgeable physical examination. The best treatment of boutonnière deformity is to avoid the deformity by early diagnosis and treatment. The authors believe that emergency department and immediate care physicians, primary care providers, hand surgeons, and hand therapists all need to be knowledgeable about the clinical tests that will reveal the occult boutonnière injury (Elson’s, modified Elson’s, and Boyes’ tests).
25
Any time the boutonnière injury diagnosis is in doubt, use of the RMF orthosis offers the ability to continue normal hand function during recovery and is a safe-protective alternative, worn full time until confirmation by clinical assessment, ultrasound, or magnetic resonance imaging (MRI).
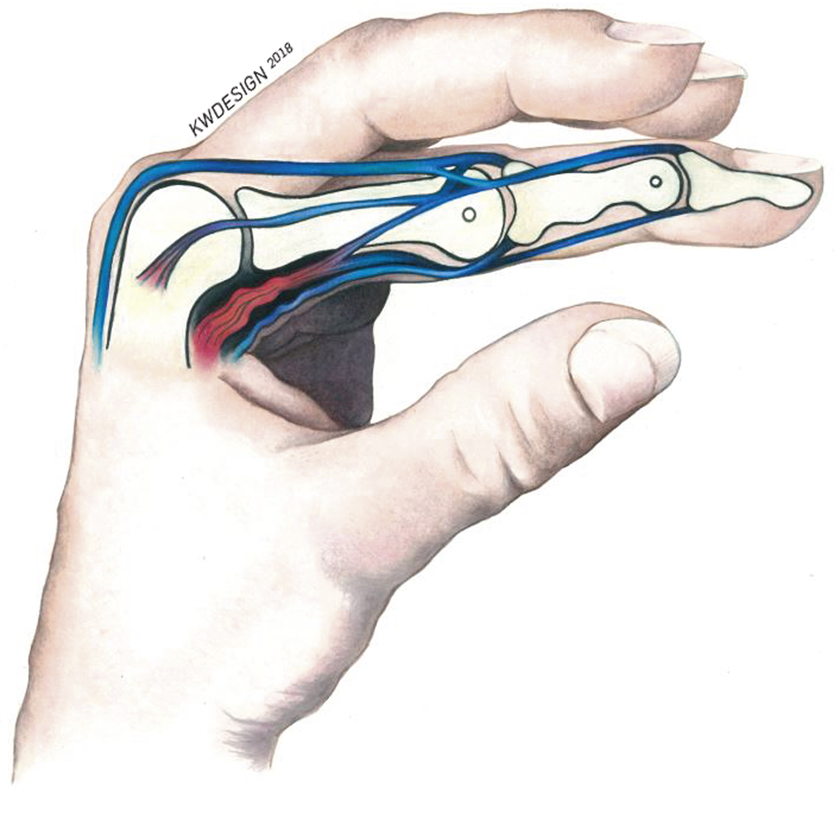
The 18th century Danish-born French anatomist Jacob B. Winslow (1669–1760) described the tendinous rhombus that later became known as “Winslow’s diamond,”
41
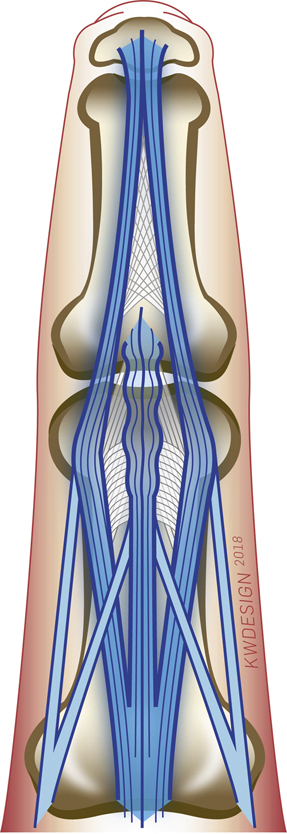
which represents the dynamic relationship between the extrinsic and intrinsic muscle contributors to the extensor mechanism. This tendinous diamond encircles the PIP joint, making it critical not only to balanced IP joint extension but also to potential use of the RMF orthosis to manage boutonnière injury (Fig. 107.5).
Biomechanical engineers have offered complex computerized mathematical studies of Winslow’s diamond relationships, citing the importance of the position of the MCP and PIP joints on tendon forces in the isolated digit. There has been little or no attention given to the significance of how changing the position of the MCP joints relative to each other alters the force relationship of the extrinsic flexor and extensor muscles and as a result causes an important IP joint response because of the dynamics of Winslow’s diamond.
41–45
Boutonnière deformity provides a unique opportunity for the RMF orthosis to provide simultaneous useful “quadriga effect” from both flexor and extensor extrinsic motor systems. The first opportunity to provide the “quadriga effect” comes from the flexor side in the profundi and the lumbrical muscles arising from the radial side of the profundi tendons. Although controversial, Kaplan
46
and Brand
47
both regarded the lumbrical as the principal extensor of the IP joints. Although not as powerful as the interossei, the lumbrical has four times greater excursion required for IP joint amplitude of motion and is more volarly positioned as it passes from beneath the deep transverse metacarpal ligament, giving it a greater angle for flexion leverage. Additionally, there is suggestion that it may provide sensory–motor feedback to position the IP system.
45
Zancolli’s
48
electromyographic studies confirm that the lumbrical remains active throughout digital extension, whereas the interossei is only intermittently active. He found that the powerful interossei are most active when there is need for forceful IP joint extension such as to stabilize the MCP joint in flexion against the powerful pull of the long extensors through its lateral slips and the lumbrical on the lateral bands.
47
This becomes apparent if one palpates the first dorsal interosseous muscle; then weakly extends the index finger IP joint; and then without changing the position of the MCP joint, more forcefully extends the IP joint to feel firm contractions of the
interosseous muscle. In the absence of interosseous function, one sees MCP joint hyperextension as in the fourth and fifth digits of an ulnar palsied hand. Because lumbricals arise from the profundi, placing an MCP joint in 15 to 20 degrees greater flexion relaxes that profundus tendon compared with its neighbors because of their common muscle, thereby also relaxing the lumbrical at its origin (Fig. 107.6). In boutonnière deformity, the lumbrical appears to be the principal deforming force to pull the lateral bands below the PIP joint axis of rotation, attenuating the residually weakened horizontal and oblique extensor hood fibers and injured triangular ligament of Winslow.

© 2018 KW Design. Contact Katie Wright of KW Design; Wright.design.illustration@gmail.com.
Under normal conditions, the extensor hood fibers and Winslow’s triangular ligament function to restrain the lateral band–conjoined tendon complex above the axis of PIP joint rotation as the complex shifts volar and lateral during flexion of the PIP joint, as described by Winslow.
41
In boutonnière deformity, the central slip attachment is absent, and the lateral bands are abnormally positioned below the joint axis of rotation, which allows the extrinsic extensor to pull the MCP joint into hyperextension and by way of the lateral slip attachments to the now relocated lateral band–conjoined tendon complex to cause PIP joint flexion and distal interphalangeal (DIP) joint hyperextension unless the RMF orthosis is used to alter the extrinsic extension force acting on the MCP and IP joints. Because the MCP joint of the affected digit is positioned in greater flexion, a simultaneously useful “quadriga effect” is created to relax pull of the long extensor–lateral slips and profundus–lumbrical muscle pull on the lateral bands. In fact, when the digit is placed in the RMF position, provided it is not a fixed boutonnière deformity, the lateral bands will dorsally reposition with active extension of the IP joints.
© 2018 KW Design. Contact Katie Wright of KW Design; Wright.design.illustration@gmail.com.
The second opportunity for the “quadriga effect” comes from the dorsal hand through the EDC tendons and their important trifurcation proximal to the PIP joint, the central slip inserting into the base of the middle phalanx and the lateral slips joining the combined interossei and lumbrical lateral bands to ultimately form the conjoined tendon that crosses the DIP joint to unite distally as the terminal tendon. Winslow
41
described the dynamics of this encircling “diamond” that normally separates and widens when the PIP joint is flexed and the EDC tendon is relaxed and then with PIP extension relocates centrally in a “cinching” fashion as the intrinsic and extrinsic tendons muscles actively contract (see Fig. 107.5). However, the lateral slips of the extrinsic long extensor tendon are quite capable of extending the IP joints alone without any intrinsic function. This is evidenced in complete ulnar nerve palsy when a dorsal blocking orthosis is used to position the palsied fourth and fifth digits in equal or greater MCP joint flexion relative to the radial digits and the lateral slips of the engaged long extensor produces IP joint extension in the affected digits. This same response can be created by the RMF orthosis when there is complete disruption of the central slip, extensor hood, and triangular ligament as long as the lateral band position remains correctable and the slack in Winslow’s loop is compensated by placing the affected MCP joint(s) in 15 to 20 degrees greater flexion.
The relative position of the MCP joints creates a simultaneously beneficial quadriga effect in the muscles of the extrinsic long extensor as well as the lumbrical via its origin from the profundus (see Fig. 107.6). Importantly, these beneficial differences in forces persist throughout the full range of active motion as permitted by the RMF orthosis because of the quadriga effect. The fact that the lumbrical origins of the fourth and fifth digits are bimodal does not seem to adversely influence the successful use of the RMF orthosis for these
digits. A possible reason could be the powerful counterforce dispersed from the EDC through the lateral slips into the lateral band–conjoined tendon by the RMF orthosis.
Isolated disruption of the EDC’s central slip insertion into the middle phalanx alone does not cause boutonnière deformity, as evidenced by the Fowler procedure, which carefully divides this central attachment from underneath the extensor hood to rebalance the extrinsic–intrinsic relationship for chronic mallet deformity.
49
A boutonnière deformity does not result from this procedure because the surrounding extensor hood and Winslow’s triangular ligament remain intact. Often after an acute boutonnière injury, the extent of extensor hood and triangular ligament of Winslow injury varies so that deformity may occur immediately or later. Provided enough of these structures remain intact to restrain the lateral bands dorsal to the PIP joint axis of rotation, the patient will be able to fully extend the PIP joint. However, if not protected after the PIP joint injury, the volar pull of the lumbrical will gradually attenuate these injured structures until the PIP joint “buttonholes” into the boutonnière deformity unless extrinsic and intrinsic muscle activity is counterbalanced by the RMF orthosis. This is why so many patients with boutonnière injury present initially with apparent normal ROM, only to progress to the deformity in subsequent weeks if undiagnosed and improperly managed.
The requirements for boutonnière deformity were defined by a recent innovative cadaver model.
50
In this model, Grau and colleagues
50
divided various combinations of Winslow’s ligament, extensor hood fibers, and the central slip. After dividing the central slip, a “modest” amount (2.4 degrees) of PIP joint extension was lost. However, missing from their model was lumbrical input, known as an important contributor to full PIP joint extension after a Fowler procedure. After further division of the extensor hood and Winslow’s ligament, a “marked” (29.2-degree) loss of PIP joint extension resulted; however, a boutonnière deformity was not created until all three structures were divided and the PIP joint was flexed to greater than 35 degrees.
50
It appears that if an RMF orthosis had been introduced into the study, the boutonnière deformity could have been avoided. A similar example was demonstrated at the 2003 ASHT meeting when all three structures were divided and the PIP joint flexed and extended with and without the RMF orthosis (see Video 107.1).
Acute Boutonnière Deformity
When patients present with an inability to extend the PIP joint or have painful full extension, it is important to determine whether the pain or loss of extension is attributable to disruption of the central slip, extensor hood, or Winslow’s triangular ligament (boutonnière deformity); a flexion contracture preceded by a pulley or volar plate injury (pseudo boutonnière); or a skin or Dupuytren’s cord contracture.
Elson’s test
51
and the modified Elson’s test
52
are used to examine for early central slip involvement after acute closed boutonnière injury. The Boyes test is often more useful for late deformity, although at times, it can identify boutonnière before deformity.
53
Elson’s test requires full flexion of the PIP joint over a table edge and assessment of the patient’s ability to extend the PIP joint and then observation for any extension force at the DIP joint. If the central slip is disrupted, PIP joint extension will be weakened, and the DIP joint may extend if the conjoined lateral bands have not slipped volarly. The modified Elson test offers visible evidence of volar displacement of the lateral bands by comparing the affected finger with the noninjured finger. This is done by placing the dorsal surface of the same digit of the opposite hand against the middle phalanx of the injured digit, keeping both PIP joints flexed to 90 degrees and requesting the patient to extend the DIP joints. If the lateral bands have shifted volarly, there will be greater extension seen in the DIP joint of the injured digit.
52
The Boyes test can be useful in acute injury, especially if there is some deformity. To perform this test, the PIP joint is first held in passive extension by the examiner while active and passive motion of the DIP joint is observed; second, the PIP joint is flexed, and DIP joint motion is compared. Volarly displaced lateral bands are verified if the DIP joint has less active and passive flexion when the PIP joint is extended compared with when the PIP joint is flexed.
53
In some acute patients, however, the result of the Boyes test might be negative if the lateral bands easily slide above and below the axis of rotation and full passive PIP extension is still possible.
25
However, in chronic boutonnière deformity, when lateral bands have become adherent, the Boyes test is usually the most useful provided the DIP joint remains supple. In the chronic stage, when the lateral bands become adherent, the DIP joint component of the test is restricted, so Elson’s test may not be of value. It is important that use of these tests is done to also separate PIP joints that have lack of extension because of flexor pulley or volar plate damage or stenosing tenosynovitis (pseudoboutonnière) from those with central slip, extensor hood, and Winslow’s triangular ligament involvement (boutonnière deformity). On examination, it is our experience that injuries to the volar PIP joint structures will test negative on the Elson and Boyes tests. Because of the flexor tendon restriction, only limited success will be achieved with use of the RMF orthosis because the relaxation of the flexor tendon is only temporary, with no correction of the primary problem. Unfortunately, late flexor tendon contracture or chronic extensor boutonnière deformity often has the same fixed ankylosed DIP joint that prohibits accurate clinical testing. MRI or ultrasound study can confirm whether the deformity originates from the dorsal or volar structures. In general, ultrasound seems preferable if extensor injury is likely,
54
and MRI may better determine the cause of flexor injury.
The authors find the “pencil test” is a simple way to simulate either the RMF or RME orthosis. This is done by placing a pencil, cotton-tipped applicator, or tongue depressor above (RMF) or below (RME) the proximal phalanx of the injured digit compared with the neighboring digits followed by active flexion and extension of the digit
17
(see the Critical Points box). This simulated RME–RMF pencil test is useful, for example, when examining an acutely injured PIP joint or the painful digit
55
or during intraoperative assessment using the simulated orthosis to determine how much active motion is safe.
Relative motion flexion is a fairly new orthotic management program with no established protocols. Various management techniques are used by different hand therapists and hand surgeons, although the anatomic rationale remains the same. Success requires the patient to understand the value of wearing the RMF orthosis full time after early diagnosis to avoid developing a boutonnière deformity or advancing an established deformity. If the early finger deformity is supple and easily correctable in the RMF position, the only requirement is to wear the RMF orthosis full time for 6 weeks, all the while moving the fingers through ROM and functionally using the hand. Therapy needs are minimal for a supple, orthosis-corrected deformity, needing only to be monitored to ensure compliance and recovery of motion and for orthosis adjustment.
25
Individualized therapy management is required in patients whose digits have developed DIP hyperextension or early volar PIP joint remodeling. Author WHM suggests that if the RMF orthosis is applied immediately after injury on fingers with supple PIP joints, DIP joint hyperextension will be corrected simply by wearing the RMF orthosis and using an orthosis to block
DIP joint hyperextension while allowing DIP joint flexion. In an acute boutonnière deformity, author JWH initially limits PIP joint flexion so as to not interfere with dorsal repositioning of the lateral bands. This is in contrast to author WHM, who encourages full active flexion any time full active extension has been achieved in the RMF orthosis.

Photo and orthosis design courtesy of © 2018 Gwendolyn van Strien, LPT, MSc.
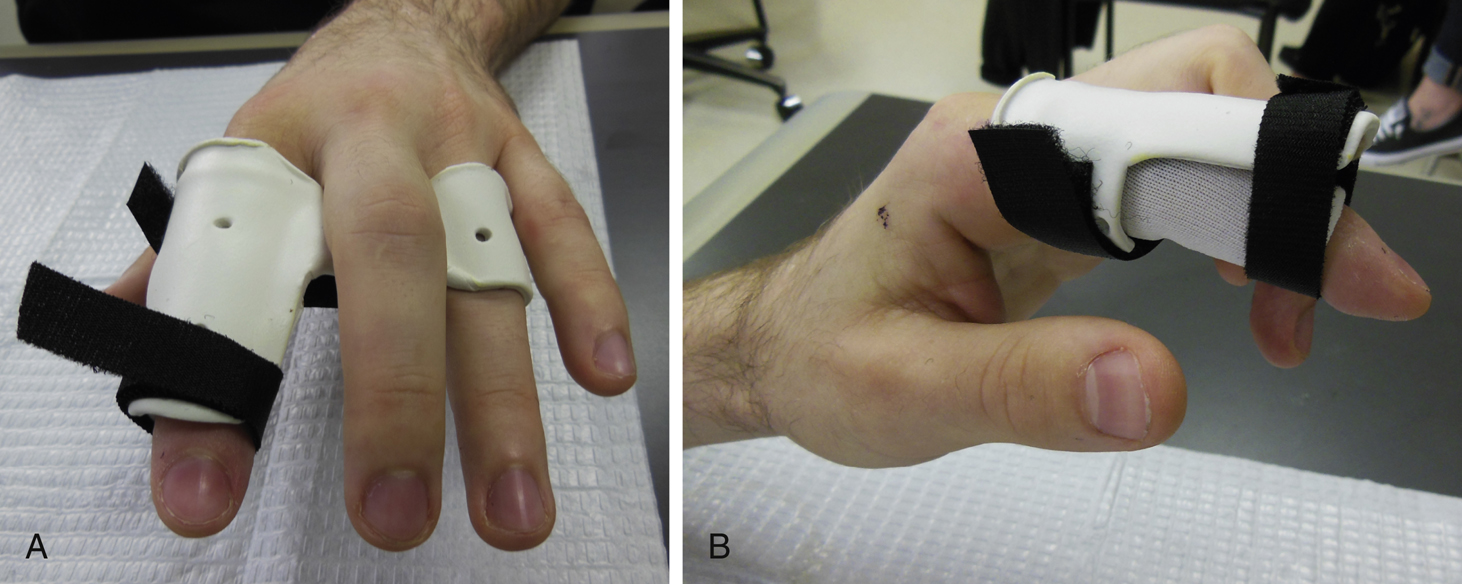
Fingers in which DIP joint hyperextension is accompanied by a PIP joint extension lag (although the joint is passively supple) may require both a DIP hyperextension block and RMF orthosis until extrinsic–intrinsic balance is restored. In the course of acute boutonnière assessment, author JWH applies the RMF orthosis–simulated “pencil test” to get a sneak preview before fabricating the RMF orthosis. For example, when “pencil tested,” the desired response in a supple PIP joint is that it actively extends to at least 20 degrees of neutral with minimal DIP joint hyperextension and has full passive extension. This indicates that the digit is a perfect candidate for the RMF orthosis worn full time for 6 weeks. However, if during the pencil test a similar supple digit achieves less than 20 to 30 degrees of active PIP joint extension (and there is no volar joint injury history), author JWH would add an RMF attachment to limit PIP joint flexion initially to 35 degrees, worn full time until active PIP extension improves to at least −20 degrees of neutral (Fig. 107.7). As active PIP joint extension continues to improve, the flexion block attachment can be either adjusted to allow more flexion or eliminated altogether with the RMF orthosis worn for at least another 6 weeks as determined by the therapist. It is common for some patients to not tolerate wearing the RMF orthosis at night, often removing it, so it may be necessary to use a static PIP joint extension orthosis for nighttime comfort and to better protect the finger. Patients with generalized joint hypermobility may require an additional orthosis to limit hyperextension of the DIP joint, worn together with the RMF orthosis to restore the extrinsic–intrinsic balance necessary for full PIP joint extension.
An acute open boutonnière surgical repair should be done under the Lalonde WALANT technique
32
using local anesthesia with epinephrine because the delicate intrinsic–extrinsic balance is difficult to restore without the patient’s active “awake” cooperation; this also provides the opportunity to apply the RMF position while in surgery to determine how much PIP joint flexion is safe for the repair (Video 107.6). After acute inflammation has subsided a few days after surgery, therapy to fabricate and fit the RMF orthosis, educate, and manage motion recovery with full-time orthosis wear is suggested for 6 to 8 weeks.
Chronic Boutonnière Deformity
Chronic boutonnière deformity has been an unresolved problem. In fact, any better active PIP joint extension than −20 degrees is considered an “excellent” result, and because of poor surgical results, no surgical effort is recommended if extension is no worse than −30 degrees.
56
The conundrum regarding inconsistent surgical outcomes was addressed in a recent literature review, with the authors concluding that “hand surgeons disagree not only on the best surgery, but even if surgery makes the finger better at all.”
57
Historically, nonsurgical management of patients with chronic boutonnière deformity has been restricted to intermittent serial casting with prolonged immobilization producing variable results with significant morbidity and frequent recurrent deformity. There is, however, wide agreement that before any other definitive treatment is considered, all digits with fixed PIP joint flexion contractures should be serial casted to gain as much passive PIP joint extension as possible, with at least −20 degrees recommended and as much recovery of DIP flexion as possible.
Jarrell and Merritt,
58
in their series of acute and chronic boutonnière deformities, serially casted all 15 chronic cases for an average of 2.5 weeks to achieve −20 degrees or less of passive PIP joint extension. Serial casting was followed by 3 months of full-time RMF orthosis wear, and therapy management required an average of 7.5 therapy sessions. In their series, the initial passive PIP joint extension in the chronic boutonnière deformities averaged −29 degrees (ranging from zero to −55), and final measures in these patients with chronic boutonnière deformities were rated as “excellent” by Steichen and Strickland
56
standards. In this group, an unforeseen average increase in combined IP joint ROM of 35.9 degrees was realized as a result of gains in both extension and flexion. Jarrell
58
stated that the most common reason for patients to return to therapy was to replace well-worn broken orthoses, which led her to routinely provide a second replacement orthosis. Although in this series, adequate PIP joint extension was achieved with serial casting, it is conceivable that if a PIP joint remains stiff and cannot be passively corrected to at least −20 degrees of PIP joint extension, a surgical release and reconstruction under WALANT followed by postoperative use of an RMF orthosis could offer greater success.
Chronic boutonnière deformity encompasses a wide spectrum of injury and chronicity for therapists to manage. Some patients are sent to therapy to prepare for surgical correction; for others, therapy is the final attempt to maximize digit function. To individualize management, an essential piece of the puzzle includes a “functional assessment” undertaken by a hand therapist regarding the patient’s functional and emotional needs. For example, if the PIP joint active extension lag can be passively improved to 30 to 35 degrees, some will be satisfied and willing to wear an RMF orthosis indefinitely as an “adaptive” orthosis, but others will be dissatisfied. Some may experience functional improvement from passive correction of the IP joint deformity contractures but find no value in wearing an RMF orthosis full time. Awareness through functional assessment of the patient’s goals will improve outcome acceptance. By definition, a chronic boutonnière deformity involves soft tissue changes of variable IP joint stiffness. Recovery of the 20/20 goal: 20 degrees of active DIP joint flexion and at least −20 degrees of passive PIP joint extension before RMF orthosis use is ideal and may be achieved with serial casting. Usually therapist preference determines the approach; choices include as a serial cast for both IP joints or a PIP joint cast worn with a progressive static DIP joint flexion orthosis. Often a piece of the boutonnière posture is MCP joint hyperextension; to counteract this, an RMF orthosis can be paired with the IP joint cast or orthosis. In the most challenging chronic boutonnière cases, author JWH prefers to reach the 20/20 goal and at least 30 degrees of active PIP joint extension before active PIP joint flexion in the RMF orthosis. When these guiding parameters are achieved, the transition from PIP joint casting into RMF orthosis wear should be therapist guided to individualize the program. For successful transition, the therapist and patient will need to determine how much PIP joint flexion is safe. One criterion is to use the patient’s sense of “tightness” during IP joint flexion, usually felt over the dorsal middle phalanx at about 30 to 40 degrees flexion of each IP joint. Author JWH limits PIP joint flexion by adding an attachment to the RMF orthosis to block flexion but allow extension (see Fig. 107.7). Subsequently over the next few weeks, the flexion block is pared down, guided by the feeling of tightness and goniometric measurement. Keeping realistic therapy goals in mind is important when managing patients with chronic deformities; few will have a perfect result. More realistically, the goal may be to recover “functional PIP joint motion.” Functional PIP joint motion has been observed to be −23 degrees of extension and 87 degrees of flexion,
59
which aligns with the Steichen-Strickland classification result of excellent as −20 degrees of extension and 80 degrees of flexion and good −30 degrees of extension and 70 degrees of flexion.
56
It has been the author’s (JWH) experience that management of the chronic boutonnière deformity accompanied by these stiffer soft tissue changes may require 3 to 6 months of limited therapy to maximize therapy results for the purpose of monitoring motion, education, and ensuring proper orthotic fit and function. For patients who chose to manage their chronic boutonnière long term, a custom-made commercially available jewelry-type orthosis and a static PIP extension orthosis for night wear might be needed.
Repaired Central Slip Extensor Tendon Zone III
Several therapy programs have been suggested for use after extensor tendon zone III central slip repair, including short-arc active motion,
60
a dynamic-assist orthosis,
61
a combination of a static PIP joint extension and an RMF orthoses,
62
and the RMF orthosis. The value and simplicity of the RMF program is that after repair, the patient wears the orthosis full time for 4 to 6 weeks while able to functionally use the hand and simultaneously exercise the finger. The RMF orthosis protects the repaired central slip in many ways. Early postoperative therapy management requires knowing how much PIP joint flexion is safe for the repair. If at the time of WALANT surgery author WHM determines that full flexion was easily achieved in the RMF position, postoperatively, he encourages full PIP joint ROM in the RMF orthosis. When no surgeon guidelines have been provided or motion has not been observed under WALANT, author JWH is guided by the important marker of 35 degrees of PIP joint flexion coupled with the patient’s feeling of “tightness.” RMF orthosis fabrication can include either the PIP joint flexion block attachment (see Fig. 107.7) or a dorsal static PIP joint extension addition (Fig. 107.8).
The suggested angle for PIP joint flexion postoperative progression is at least 75 degrees at week 4 and at least 100 degrees and discontinuation of the orthosis by week 6. Pairing active DIP joint flexion–extension as the PIP joint is held extended while wearing the RMF orthosis benefits tendon excursion and repair healing (Fig. 107.9). Through experience, author JWH has observed extensor lags of 15 to 20 degrees to resolve with full-time wear of the RMF orthosis; however, greater than 20-degree lags require detective work because a central slip is not a requirement for PIP joint extension, other critical dorsal structures may have been injured, or there is lateral band adherence, indicating a need for more PIP joint flexion and DIP joint flexion–extension exercises.
© 2018 KW Design. Contact Katie Wright of KW Design; Wright.design.illustration@gmail.com.
Summary
Our goal for this chapter was to review the rationale for the RM concept used as a “protective orthosis” in hand therapy management of extensor tendon zone III to VI repairs, sagittal band injuries, and acute and chronic boutonnière deformity. Although beyond the scope of this chapter, RM has other applications as a “protective” orthosis such as in tendon transfers after attrition ruptures in caput ulnae syndrome and Vaughn-Jackson syndrome,
25
flexor tendon
63
and digital nerve repair,
3
skin grafting,
3
intrinsic transfers,
3
intrinsic musculotendinous injury,
55
and finger joint arthroplasty.
3
As an examination tool, the simulated RMF–RME pencil test is used to evaluate undetermined finger joint pain
3
and to sneak preview the quadriga effect before orthosis fabrication.
3
When used as an “exercise” orthosis, it is most often used to improve ROM after such conditions as Dupuytren’s surgery or collagenase injection,
25
a mild flexion PIP joint contracture,
3,25
extensor hood adherence with PIP joint extension lag
3,25
(Fig. 107.10), MCP joint flexion that overpowers IP joint flexion,
64
or PIP joint hyperextension by stretching tight intrinsic muscles.
3
Finally, one of the most exciting RM orthotic applications is what Hirth and coworkers
3
described as the “adaptive” orthosis category, which has been used to manage rheumatoid arthritis finger deformities and the muscle imbalances of ulnar nerve palsy, cerebral palsy, Parkinson’s disease, and after C5 to C6 discectomy.
3,64
The authors look forward to further expansion that may provide deformity prevention such as for PIP joint strains, burned digits, adolescent hypermobile fingers, and early inflammatory arthritis. Many of these conditions require orthotic design originality and development of materials that are work or sport friendly, safe to be worn with open wounds, soft for
fragile skin, and aesthetically appealing for long-term wearers, all the while being compatible and focused on preserving useful hand function.
65,66
Refer to Video 107.7 for practical tips for fabrication of RM orthoses.

Photo and orthosis design courtesy of © 2018 Dr. Lynne Feehan, BScPT, MSc, PhD.
Acknowledgments
The authors thank Sandra Robinson and Melissa Hirth for their invaluable insights in strengthening the content of this chapter and to recognize their major contributions to the concept of RM.