Therapeutic Use of Self: Applying the Intentional Relationship Model in Group Therapy
Renée R. Taylor, Laura Van Puymbrouck
OBJECTIVES
- 1. Define therapeutic use of self in occupational therapy.
- 2. Identify the central components of the intentional relationship model.
- 3. Apply the six therapist interpersonal modes within the interpersonal reasoning process.
- 4. Differentiate therapeutic responding from suboptimal responding.
- 5. Understand the application of the intentional relationship model in group therapy approaches.
- 6. Understand the difference between activity focusing and interpersonal focusing according to the intentional relationship model.
- 7. Understand the role of group dynamics (adaptive and maladaptive) in therapy outcomes.
- 8. Apply the intentional relationship model to a group therapy case example.
AN INTRODUCTION TO THERAPEUTIC USE OF SELF IN OCCUPATIONAL THERAPY
According to the Intentional Relationship Model (IRM; Taylor, 2020). Therapeutic use of self is defined as the application of empathy and intentionality to an interpersonal knowledge base and corresponding skill set that is applied thoughtfully to resolve challenging or poignant interpersonal events in practice. Therapeutic use of self requires the therapist to strive toward a fundamental understanding of each client at an interpersonal level, focusing on the client's communication preferences and needs. This process of understanding involves a personal and subjective investment in the client during which the therapist makes moment-to-moment decisions about how to initiate and respond to the client's reactions to therapy and/or the therapist (Taylor, 2020).
Throughout its history, occupational therapy (OT) has emphasized the importance of understanding the interpersonal characteristics of a client, in addition to his, her, or their physical, sensory, or cognitive impairments. In individual and group therapy applications, terms such as client-centered care, empathy, and narrative reasoning frequently appear in the literature. These concepts and values have been upheld in academic research as well as in clinical settings. For example, a growing number of studies indicate that the client-therapist relationship is a key determinant of whether OT has been successful (AOTA, 2020; Ayres-Rosa & Hasselkus, 1996; Cole & McLean, 2003). However, there has been a lack of cohesion between evidence and discussion about the importance of these values and literature describing the concrete skills and competencies that are necessary to enact them within a clinical setting.
The Occupational Therapy Practice Framework (AOTA, 2020) describes the therapeutic use of self as “integral to the practice of OT [and] used in all interactions with clients.” Many believe that the ability to communicate with one's client develops intuitively. The communication necessary to introduce a therapeutic activity, conduct an assessment, or respond to a client's concerns somehow becomes second nature over time. In many OT situations, this may appear to be the case. Although some believe that use of self is intuitive, a survey study of OT practitioners in the United States found that most agreed that the field lacks sufficient knowledge about therapeutic use of self (Taylor, Lee, Kielhofner, & Ketkar, 2009). For example, only 4.3% of respondents reported taking a class that focused only and specifically on this topic in OT school (Taylor, Lee, Kielhofner, & Ketkar, 2009). This chapter provides a rationale for the use of the IRM (Taylor, 2020), describes the model, and describe its application in group therapy. A case example is presented that illustrates a clinician's use of this model in a group therapy situation.
THE INTENTIONAL RELATIONSHIP MODEL IN OCCUPATIONAL THERAPY
Contemporary OT practice requires a therapist to understand how to manage the relationship with a client to optimize occupational engagement (Kielhofner, 2009). A conceptual practice model that provides a set of concrete tools and suggestions for development of interpersonal skills is a necessary guide in assisting occupational therapists in developing an understanding of use of self. The IRM explains therapeutic use of self and its relationship with occupational engagement. It defines the most critical components of the client-therapist relationship as they are enacted in practice. The Intentional Relationship Model (IRM; Taylor, 2020) places the client's communication needs and preferences at the center of all therapeutic interactions and holds the therapist responsible for working to develop a trusting and open relationship with the client (Taylor, 2020).
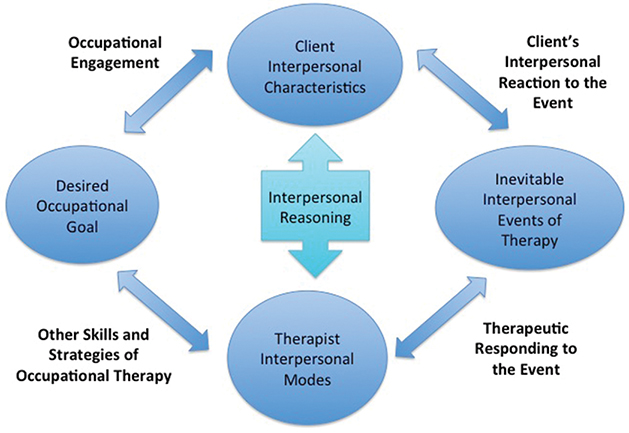
The IRM guides therapists to navigate four aspects of the therapist-client relationship. These are: (1) the client's interpersonal characteristics, (2) the interpersonal events that inevitably occur during therapy, (3) the therapist's use of modes and other interpersonal skills, and (4) the client's engagement in occupation. According to the IRM, therapeutic use of self is defined as a product of the extent to which one applies empathy and intentionality to understand the client on an interpersonal level and to direct the interchangeable use of six therapist communication modes to resolve evocative interpersonal events in practice. Therapeutic use of self requires the therapist to strive toward a fundamental understanding of the client and involves a personal and subjective investment in the client during which the therapist makes moment-to-moment decisions about how to initiate and respond to the client using one of the six therapist communication modes. The IRM asks therapists to observe and understand their clients from an interpersonal perspective, to be prepared to respond therapeutically to rifts and other significant interpersonal events that occur during therapy, and to communicate within a mode that matches the client's interpersonal needs of the moment (Taylor, 2020). This model, which is illustrated in Fig. 4.1, provides a theoretical framework for understanding the significance that all interactions have and guidance in how to therapeutically respond in a manner that best serves the client. Each of the central components of the model is described in the following pages, and more extensive information is presented in Taylor (2020).
Client Interpersonal Characteristics
At first appraisal, the relevant aspects that the client brings into a therapeutic relationship may appear to be obvious. For example, a client's heightened need for control becomes salient the moment he or she asks what seems to be an unnecessary question for the third time. A client's reluctance to engage in an activity may become apparent when he or she appears not to have heard a given instruction. One quickly learns of a client's limited capacity to assert his or her needs when the client is found lying on a mat without a means to right himself or herself, not having asked anyone for help.
Although these are common characteristics of clients in everyday practice, they are not traditionally discussed as fundamental aspects of OT care plans or documented in a client's chart notes. Understanding the more challenging aspects of a client's interpersonal characteristics from an objective but empathic perspective assists a therapist to act in a way that is intentional and facilitating of occupational engagement (Fig. 4.2).
IRM defines the essential interpersonal characteristics of a client in terms of the following 14 categories:
- • Communication style
- • Tone of voice
- • Body language
- • Facial expression (affect)
- • Response to change or challenge
- • Level of trust
- • Need for control
- • Approach to asserting needs
- • Predisposition to giving feedback
- • Response to feedback
- • Response to human diversity
- • Orientation toward relating
- • Preference for touch
- • Interpersonal reciprocity
Communication style refers to a client's ability to communicate in a clear, well-paced, and detailed yet succinct manner that is appropriate to his or her developmental level and cognitive ability. Reticence to communicate or, by contrast, excessive loquaciousness will undoubtedly affect the therapeutic dynamic and the quality of occupational engagement that might otherwise be possible to achieve. Therefore the IRM calls for therapists to consider communication difficulties, such as these in building the therapeutic alliance, selecting an approach to communication, and ultimately in establishing the OT care plan. The same approach applies to the remaining categories of client characteristics. Tone of voice may be notably low, high, tense, strained, or breathy, for example. Tone of voice may reveal whether an individual might be sad, angry, or nervous, for example. Body language is expressed in a slouched posture, an overly erect posture, crossed arms, crossed legs, fidgeting, restlessness, pacing, moving slowly, or moving rapidly, for example. Body language may point to the way an individual feels toward others that are present, or it may be a function of the way a person feels within, independently of the social environment. Facial expression (affect) is defined as a client's general emotional expression during therapy, ranging from appropriately buoyant for the situation (flexible) to flat (absence of expression) to heightened (intensely emotional) to labile (fluctuating anywhere between elation, anger, angst, and despair).
Response to change or challenge refers to a client's ability to adapt to changes in the therapy plan or environment and his or her approach to OT tasks and situations that are new or challenging. Level of trust refers to a client's ability to trust that the therapist has his or her best interests in mind and that every effort will be made to ensure his or her physical safety and emotional wellbeing. Need for control is defined as the degree to which a client takes an active versus passive role within the relationship and in determining the course of therapy. Approach to asserting needs defines a client's approach to expressing his or her wishes and needs for support, information, resources, or other requests within the therapeutic relationship, if they are expressed at all.
Predisposition to giving feedback describes a client's tendency toward providing the therapist with corrective feedback or praise, or both. In some cases, this feedback may be appropriately matched to the therapist's behavior or performance, and in other cases, the therapist may struggle to see the relevance of the feedback or may find the feedback to be excessive. In yet other cases, a therapist may struggle to obtain any feedback from a client, who may be reluctant to provide feedback.
Response to feedback involves a client's ability to provide the therapist with appropriate negative or positive comments about his or her reactions to the therapist and experience of therapy as either helpful or unhelpful. Response to feedback describes a client's ability to maintain perspective when receiving praise from the therapist or when receiving correction during performance, limits on behavior, or information about his or her strengths and weaknesses. Response to human diversity is defined by a client's reaction to ways in which he or she may be the same or different from the therapist in terms of observable sociodemographic characteristics (i.e., race, ethnicity, gender, age) and other interpretations of outward appearance or perceived worldview. Some clients have more difficulty than others relating to a therapist whom they perceive as differing from them in fundamental ways.
Orientation toward relating defines a client's need for interpersonal closeness versus professional distance within the therapeutic relationship. Difficulties may occur when the client's expectations about the relationship differ from those of the therapist. Preference for touch involves a client's observed comfort with or expressed reaction to any type of physical touch, whether it be a necessary part of treatment or an expression of caring.
Interpersonal reciprocity refers to a client's ability to engage fully in the therapy process or show appreciation toward the therapist as a separate but connected partner within the therapy process. Some clients may be so focused on their own situations that they may lack this capacity, whereas others may function in an active and mutual way within the relationship. Regardless of the outcome, a client's capacity for reciprocity is always felt by the therapist and must be managed accordingly.
In summary, understanding client interpersonal characteristics is fundamental to planning how to respond during therapeutic interactions. Familiarizing oneself with the interpersonal characteristics of each of one's clients becomes particularly important in group therapy situations, in which it is important to consider the effects of one client's behavior on another, in addition to the effects of the therapist's behavior on each and every one of the clients and on the group as a whole. Example of client characteristics as they may be observed in a group therapy situation are presented in Table 4.1. An extensive discussion of client characteristics may be found in Taylor (2020).
TABLE 4.1
| Interpersonal Characteristic | Group Therapy Example |
|---|---|
| Communication style | Elizabeth's group communication style appears to be a reluctance caused by a lack of confidence when asked her opinion on what activities the group should work on in a session. In one-on-one environments she is quick to provide her opinion. |
| Tone of voice | Alex's tone of voice shifts noticeably from soft spoken and halting when asked to provide her own idea during story making to a louder, higher pitch when offering story ideas to Elizabeth during the group session. While her speech processing is impacted by her diagnosis, the tone of her voice can be used to understand how Alex is feeling during group tasks. |
| Body language | When it is her turn in group turn-taking activities, Elizabeth tilts her head down and avoids eye contact with the therapist, as well as other group members. This closed body language corresponds to her decreased self-confidence for asserting herself or her ideas in group activities. |
| Level of trust | During a session in which the therapist incorporated an overhead swing, all of the girls demonstrated hesitancy in attempting the activity despite encouragement. Alex has had multiple interactions both one on one and in the group with the therapist and displayed increased trust for this activity. Observing Alex enjoy the task encouraged the two other girls to engage in it. |
| Need for control | Iris' high need for control is evident during a parallel play activity of coloring because she frequently chooses and distributes crayon colors for the other girls to use, hoarding the most popular colors for herself. |
| Approach to asserting needs | In the coloring scenario, Elizabeth is unable to ask for a crayon color to be returned that has been taken from her despite her desire for it. Despite the therapist offering support for Iris to return the crayon, Elizabeth instead quickly picks up a crayon offered to her as a replacement by Iris. |
| Response to change and challenge | Unable to locate a commonly used CD for music during the group, Alex is quick to look for alternatives; however, Iris appears distraught by this inconsistency and withdraws from the group activity. |
| Affect | Because of Iris' high need to control the group and her dynamic affect, the therapist is careful to be sensitive to how her emotional vacillations affect the entire group and minimizes how these behaviors could be used by Iris as a tool for control. |
| Predisposition to giving feedback | During decision making for activity choice, Elizabeth infrequently provides input. When encouraged to provide a very basic choice, she displays prolonged hesitation; ultimately, she is dominated by others in the group and is unable to verbalize her opinion. Later, when alone with the therapist, she acknowledges that she knew what she wanted to choose but was afraid the other girls would not like it. |
| Capacity to receive feedback | When Iris is encouraged to be more sensitive to turn taking when making choices, she is unable to receive this feedback without obvious disengagement and irritability for a brief time in response to the therapist. |
| Response to human diversity | In this particular playgroup, the girls all have historical difficulties with a male in their immediate family dynamic. Because of this, when attempts have been made for a male therapist to lead the group, each girl displays increased withdrawal behaviors and disengagement from activity. |
| Orientation toward relating | Each of the girls displays varying levels of relating to one another. Alex and Elizabeth have a nurturing and mutually helping relationship (e.g., they frequently hold hands together while walking); however, Iris has the need to remain safely distant with limited displays of intimacy to the other girls. |
| Preference for touch | Each child in the playgroup has different preferences for touch, most notable during times of distress. Iris prefers limited physical touch, withdrawing when it is attempted, whereas Alex prefers prolonged hugs to comfort her. |
| Interpersonal reciprocity | During one session, the therapist gets a paper cut. Differences are noted with each child in her reciprocity toward the therapist's pain. Elizabeth is quick to ask her if the therapist is okay; Alex appears distressed by this occurrence, with decreased eye contact and verbalizations; and Iris begins telling a story about how many times she has had paper cuts and the effect they had on her. |
The Inevitable Interpersonal Events of Therapy
Similar to client characteristics, difficult or positive but emotionally poignant circumstances that occur during therapy are a normal part of everyday practice for every therapist. However, knowing how to anticipate and respond to them in a deliberate and planned therapeutic way is not necessarily an assumed, universal skill. According to the IRM (Taylor, 2020), an interpersonal event is a naturally occurring communication, reaction, process, task, or general circumstance that occurs during therapy and that has the potential to detract from or strengthen the therapeutic relationship. In therapy, these events may be precipitated by the following kinds of circumstances:
- • Client resistance (e.g., a client refuses, either actively or passively, to communicate or participate in some activity)
- • Therapist behavior (e.g., the therapist provides feedback that a client finds difficult to hear)
- • Client display of strong emotions in therapy (e.g., a client becomes tearful when reflecting on the extent of his or her impairment before beginning therapy, as compared with the progress made recently)
- • A difficult circumstance of therapy (e.g., a client is uncomfortable practicing toileting hygiene with the therapist)
- • A rift or conflict between the client and therapist (e.g., a client disagrees with a treatment recommendation and confronts the therapist in a way that the therapist perceives is personal)
- • Differences concerning the aim of therapy (e.g., a client insists on a goal that the therapist believes is not attainable, or the therapist recommends a goal that the client rejects)
- • Client requests that test the boundaries or limits of the therapeutic relationship (e.g., the client invites the therapist to attend his or her wedding)
These are only a few of the myriad possible interpersonal events that occur during the course of OT. The full list of the 12 categories of interpersonal events includes the following (Fig. 4.3):
- • Expression of strong emotion
- • Intimate self-disclosures
- • Power dilemmas
- • Nonverbal cues
- • Verbal innuendos
- • Crisis points
- • Resistance and reluctance
- • Boundary testing
- • Empathic breaks
- • Emotionally charged therapy tasks and situations
- • Limitations of therapy
- • Contextual inconsistencies

Definitions and examples of group therapy situations for each of these are presented in Table 4.2 and are described in more detail in Taylor (2020). When interpersonal events occur, their interpretation by the client is a product of the client's unique set of interpersonal characteristics. Sometimes the event may have a significant effect on the client and other times a client will be unaffected or minimally affected. When such events occur, it is important that the therapist be aware that the event has occurred and take responsibility for responding appropriately.
TABLE 4.2
| Interpersonal Event | Definition | Group Therapy Example |
|---|---|---|
| Expression of strong emotion | External displays of internal feelings are shown with a high level of intensity beyond usual cultural norms for interaction. Can be positive or negative expressions. | During the end of playgroup and immediately following a power dilemma that was resolved with successful use of Empathizing Mode, Iris gives a hug to the therapist and exclaims she loves the therapist more than anybody else in the world. |
| Intimate self-disclosures | Statements or stories reveal something unobservable, private, or sensitive about the person making a disclosure. These can be stories about oneself or about close others. | Alex discloses during imagination time and story development that her mother and father are getting divorced. While casually brought up during the group conversation, this disclosure reveals an area of stress for Alex. |
| Power dilemmas | Tensions arise in the therapeutic relationship because of clients' innate feelings about issues of power, the inherent situation of therapy, the therapist's behavior, or other circumstances that underscore clients' lack or loss of power over aspects of their lives. | During cleanup time at the conclusion of playgroup, Iris' refusal to put her toys away is coupled with her sitting in the middle of the floor with her arms folded. It is important that the therapist does not attempt to force her to participate here, because a power dilemma is a common end result. |
| Nonverbal cues | Communications do not involve the use of formal language. Some examples of these are facial expressions, movement patterns, body posture, and eye contact. | Elizabeth has a tendency to limit eye contact and engage in idle fiddling with a toy during discussion of client choices for activities at the beginning of playtime. |
| Verbal innuendos | Communications in which the client says something elusive or oblique that is meant to serve as a hint about a more direct communication. | Iris' quick actions to reach out and assist Elizabeth in activities, especially those requiring fine motor skills, are often accompanied by statements reflecting that Iris assumes Elizabeth is unable to perform the task. An example of this is: “Let me help you, I'll make it pretty.” |
| Crisis points | Unanticipated, stressful events cause clients to become distracted or temporarily interfere with clients' ability for occupational engagement. | During an outing to a playground, Alex becomes frightened by a passing dog, causing tearfulness and requiring the therapist to decrease attention to the group as a whole to console Alex. Careful attention had to be given to return to the group's needs as soon as Alex was consoled to avoid escalation of the crisis to others in the group. |
| Resistance and reluctance | Resistance is a client's passive or active refusal to participate in some or all aspects of therapy for reasons linked to the therapeutic relationship. Reluctance is disinclination toward some aspect of therapy for reasons outside the therapeutic relationship. | Elizabeth's refusal to follow the other children in rolling somersaults in the grass is reluctance based on her long-standing sensory processing difficulties. |
| Boundary testing | A client behavior violates, or asks the therapist to act in ways outside, the defined therapeutic relationship. | When asked to participate in an activity, Iris states she will only participate if the therapist will take her to the candy store after therapy. |
| Empathic breaks | The therapist fails to notice or understand a communication from a client, or communication or behavior initiated by the therapist is perceived by the client as hurtful or insensitive. | During the group's parallel play time Alex proudly displays her completed coloring project, which is below her age appropriateness. The therapist congratulates her but states that it must have been easy because it was from a baby's coloring book. Alex immediately responds with a deflated affect. |
| Emotionally charged therapy tasks or situations | Activities or circumstances can lead clients to become overwhelmed or experience uncomfortable emotional reactions, such as embarrassment, humiliation, or shame. | During a physically challenging activity, Elizabeth suffers from increased oral secretions that she is unable to perceive. Iris points this out to the other group members, which embarrasses Elizabeth and makes her withdraw from the activity. |
| Limitations of therapy | There are restrictions on the available or possible services, time, resources, or therapist actions. | During playtime decision making, a promise was made that, at the conclusion of the hour, the group would be allowed to play with a favorite toy. At the appropriate time for this reward to occur, the toy has been misplaced and is unable to be found for follow-through of the promised reward. |
| Contextual inconsistencies | Any aspect of a client's interpersonal or physical environment changes during the course of therapy. | This playgroup has three therapists who typically treat them; however, when a new therapist must assume the group session, the group requires some time to adjust to this new individual. |
Interpersonal events are:
Interpersonal events are part of the constant give and take that occurs in a therapy process. They are distinguished from other events or processes in that they are charged with the potential for an emotional response either when they occur or later after reflection. Consequently, if they are ignored or responded to less than optimally, these events can threaten both the therapeutic relationship and the client's occupational engagement. When optimally responded to, these events can provide opportunities for positive client learning or change and for solidifying the therapeutic relationship. Because they are unavoidable in any therapeutic interaction, one of the primary tasks of a therapist practicing according to the IRM is to respond to these inevitable events in a way that leads to repair and strengthening of the therapeutic relationship (Taylor, 2020).
The Six Interpersonal Modes
According to the IRM, effective use of self requires therapists to know and responsibly accept interpersonal blind spots, recognize and cultivate strengths within their therapeutic personas, and develop less-used communication approaches through a reflective and ongoing self-appraisal of the effects of their behavior on clients (Taylor, 2020). The first step in accomplishing this is through an understanding of the six therapist interpersonal modes. A therapeutic mode is a specific way of relating to a client. The IRM identifies six therapeutic modes:
A brief definition of each mode and an example of its use in a group therapy situation are provided in Table 4.3. More detailed information about how to communicate using the six modes is presented in Taylor (2020).
TABLE 4.3
| Mode | Definition | Group Therapy Example |
|---|---|---|
| Advocating | The therapist ensures that the client's rights are enforced and resources are secured. May require the therapist to serve as a mediator, facilitator, negotiator, enforcer, or other type of advocate with external persons and agencies. | Speech therapy services will soon be discontinued for the client. However, following several playgroup sessions in which oral secretion management difficulties occurred, the occupational therapist discusses with the family the possibilities of working on this goal area and advocates for pushing back discontinuation of speech to allow for treatment focusing on this issue. |
| Collaborating | The therapist expects the client to be an active and equal participant in therapy, and ensures choice, freedom, and autonomy to the greatest extent possible. | A goal area for this playgroup is to facilitate equal decision making and turn taking by all members of the group. During activity selection, the therapist structures a routine that requires each child to be responsible for different choices of the day. This routine is a constant, and the therapist uses collaboration mode to ensure all voices are heard during activity decision making. |
| Empathizing | The therapist continually strives to understand the client's thoughts, feelings, and behaviors while suspending any judgment. The therapist ensures that the client verifies and experiences the therapist's understanding as truthful and validating. | Following a failed attempt to manipulate the group, the client withdraws and becomes passive-aggressive during attempts to engage her. The therapist uses empathizing mode to allow the client to discuss her feelings. The use of empathizing mode demonstrates to the client that the therapist understands her behavior and is not critical of it. |
| Encouraging | The therapist seizes the opportunity to instill hope in a client and celebrate a client's thinking or behavior through positive reinforcement. The therapist conveys an attitude of joyfulness, playfulness, and confidence. | During a 10-minute span in which the three girls participated in a task that required a group effort from all to succeed, the therapist used appropriate reinforcement through the encouraging mode to identify positive behaviors from each child as they worked together successfully. At the successful conclusion of the task, encouraging mode was again used to celebrate their achievement. |
| Instructing | The therapist carefully structures therapy activities and is explicit with clients about the plan, sequence, and events of therapy. The therapist provides clear instruction and feedback about performance and sets limits on a client's requests or behavior. | At the onset of each playgroup session, the therapist initiates the activity with clearly established rules and goals of the group. Using instructing mode and a consistent approach with each session reminds the girls (and assists the client with her recall of the group's agenda) of what their tasks and expectations are. |
| Problem solving | The therapist facilitates pragmatic thinking and solving dilemmas by outlining choices, posing strategic questions, and providing opportunities for comparative or analytic thinking. | One activity that occurs during each playgroup is imagination play or story telling that will be acted out. In one session, the group is asked to create a journey through an imaginative land that has many physical challenges. The group works together with assistance from the therapist using problem-solving mode, facilitating input from each girl, to create a story of three princesses walking along a path with various challenges to save three puppies that must be carried home to safety. |
Therapists naturally use therapeutic modes that are consistent with their fundamental interpersonal characteristics. For example, a therapist who tends to be more of a listener than a talker and believes in the importance of understanding another person's perspective before suggesting would likely use empathizing as a primary therapeutic mode in therapy. Therapists vary widely in terms of the range and flexibility with which they use modes in relating to clients. Some therapists relate to clients in one or two primary ways, whereas others draw on multiple therapeutic modes, depending on the interpersonal characteristics of the client and the situation, or inevitable interpersonal events, at hand. One of the goals in using IRM is to become increasingly comfortable using any of the six modes flexibly and interchangeably, depending on the client's needs. A therapeutic mode or set of modes define therapist's general interpersonal style when interacting with a client. Therapists able to use all six of the modes flexibly and comfortably and to match those modes to the client and the situation are described as having a multimodal interpersonal style.
According to the IRM, a therapist's choice and application of a particular therapeutic mode or set of modes should depend largely on the interpersonal characteristics of the client and his or her reaction to any interpersonal events that may be occurring. Although a client may prefer that the therapist use one or two central modes, certain interpersonal events in therapy may call for a mode shift. A mode shift is a conscious change in one's way of relating to a client. For example, if a client perceives a therapist's attempts at problem solving to be insensitive or off the mark, an intentional therapist would notice this in the client's tone of voice, affect, and body language, and would accordingly switch from the problem-solving mode to a different mode, such as the empathizing mode. This would allow the therapist to obtain a better understanding of the client's perspective and current experience.
The IRM interpersonal reasoning process, described in the following paragraph, is used to guide the therapist in deciding when a mode shift might be required and determining which alternative mode to select. Because the interpersonal aspects of OT practice are complex and require a therapist to possess a highly adaptive therapeutic persona, the IRM recommends that therapists learn to draw on all six of the therapeutic modes in a flexible manner according to the different interpersonal needs of each client and the unique demands of each clinical situation.
The Interpersonal Reasoning Process
The third therapist interpersonal competency involves the capacity to engage in an interpersonal reasoning process when an interpersonal dilemma presents itself in therapy. Interpersonal reasoning is a stepwise process by which a therapist decides what to say, do, or express in reaction to the occurrence of an interpersonal dilemma in therapy. It includes developing one's capacity for empathic understanding of each client's unique interpersonal characteristics, developing a mental vigilance toward the interpersonal aspects of therapy in anticipation that a dilemma might occur, and selecting one or more of the six therapist communication modes as a means of responding to the event. The process then requires the therapist to reflect upon his, her, or their mode use and its effects upon the client. The six steps of interpersonal reasoning and their definitions are presented in Table 4.4. An extensive description and discussion of these steps can be found in Taylor (2020).
TABLE 4.4
| Step of Interpersonal Reasoning | Definition |
|---|---|
| Anticipate | Use observational skills, information from others who have interacted with the client, and your direct experience interacting with the client to anticipate the likely interpersonal events that may occur during therapy, given your knowledge of the client's interpersonal characteristics. |
| Identify and cope | Use IRM language to label a difficult client characteristic or interpersonal event when it occurs. Do what it takes to collect yourself and get emotional perspective on the situation. Remind yourself not to take it personally. |
| Determine if a mode shift is required | Ask yourself the following questions to determine whether a mode shift is required: What mode am I currently using with this client, if any? What are the effects of the mode on the client? Would another mode better serve the interpersonal needs of this client at this moment? |
| Choose a response mode or mode sequence | Interact within the mode or modes that you think the client prefers or needs at this moment. Think about a sequence of modes that you might use to accommodate changes in what the client might need from moment to moment. |
| Draw on any relevant interpersonal skills associated with the modes | Think about other communication, rapport-building, and conflict resolution skills that you might draw on in association with your mode use. |
| Gather feedback | Gather nonverbal or verbal feedback from the client as to whether he or she feels comfortable with the way you approached the event or difficulty. |
IRM, The intentional relationship model.
APPLYING THE INTENTIONAL RELATIONSHIP MODEL IN GROUP THERAPY SITUATIONS
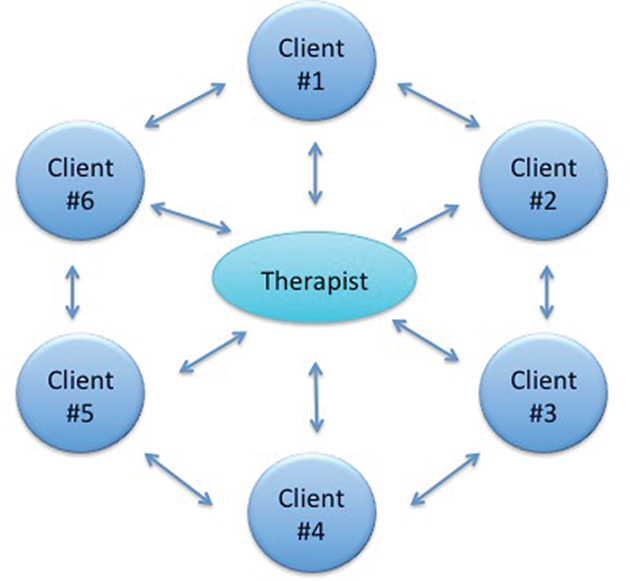
With the exception of educational and planning groups, most OT groups involve engaging clients in some level of activity. The demands associated with selecting, grading, and engaging all members in the activity can sometimes be so great that they may cloud a therapist's vision of important interpersonal dynamics within the group. The IRM principle that activity focusing must be balanced with interpersonal focusing (Cole & McLean, 2003) is particularly relevant in group therapy situations. This principle holds that therapists should not overrely on aspects of an activity to replace or compensate for the need to attend to the interpersonal aspects of the therapy practice. Dimming the lights or downgrading an activity in response to a toddler's emotionally laden refusal to participate in therapy is an example of activity focusing. By contrast, changing one's mode from instructing to collaborating (allowing the client to take the lead in therapy) or empathizing (observing and listening for a client's needs) is an example of interpersonal focusing. When focusing on the interpersonal aspects of a group therapy situation, therapists must consider a number of questions that will help them understand the group and decide how to interact with it in a way that serves the best interests of as many members as possible (if not all members). According to IRM, a social systems perspective calls for therapists to understand the interpersonal aspects of their interactions with each client in the group, as well as the interpersonal aspects of the mutual interactions between members (Fig. 4.4) (Taylor, 2020). Questions that characterize a social systems perspective include:
- • What are the most salient interpersonal characteristics of each member of the group? How are they similar and how are they different? What modes work best for group members individually and collectively (Fig. 4.5)?
- • Is there a member of the group that appears to present a greater number of difficult interpersonal characteristics as compared with others? How does this member's behavior affect others in the group? What modes are most effective in managing this person's behavior?
- • Who are the most engaged members of the group? Who are the most disengaged? What modes work best to increase occupational engagement within the group?
- • Who are the most prominent or influential members? How do they exert their power? Do they affect the group in a positive, negative, or mixed way? What modes work best to increase the likelihood of a positive outcome?
- • What topics, general themes, or content of conversation dominate the group?
- • What is the general emotional tone or mood of the group?
- • Is communication within the group shared, open, and direct or are there certain alliances and indirect routes of communication?
- • What productive dynamics exist that support the group's best interests?
- • What maladaptive dynamics exist? What modes are most successful in managing the maladaptive dynamics?
- • How are disagreements or conflicts of interest managed?
- • What other interpersonal events are likely to occur within the group or are emerging as potential patterns? What modes are most effective when responding to these events?

One of the most effective ways to begin to understand interactions from a social systems perspective is to observe a group of people interacting while keeping these questions in mind.
Adaptive Versus Maladaptive Group Dynamics
When one attempts to interact with a social system, such as a group, the entire system becomes a kind of client in itself. As the therapist, you may take on one or more roles within the system and use modes to move into and out of the system in an intentional way to serve an individual client's or the group's best interests. To do this, one must be able to objectively identify and work within any number of dynamics that may emerge.
A dynamic defines the distinctive quality, emotional tone, and specific interpersonal events that compose an interaction between individuals. For example, a dynamic involving competition for approval from the group leader may be observed between latency age girls participating in a dance group. Although it may not always be a productive dynamic, it is observed frequently in practice. If a dynamic serves a specific purpose within the system, it may become repetitive or entrenched over time. For example, a competitive dynamic between the girls may increase the likelihood that at least one of the girls will receive approval from a therapist who is otherwise weak in the encouraging mode (i.e., less likely to give open praise).
Dynamics can be productive or maladaptive. One example of a productive dynamic is a trusting dynamic. A trusting dynamic is characterized by evidence of trust between a client and therapist. For example, if a client feels confident about a therapist's ability to teach and demonstrate a sewing skill, his or her trust in the therapist will manifest in his or her earnest attempts to learn the skill. When a therapist returns the trust by showing a genuine investment in teaching, it constitutes further evidence that the therapist trusts that the client has a sincere desire to learn. If a client seeks input to check if the skill is being performed correctly, it constitutes behavioral evidence of this trusting dynamic. Similarly, if a therapist shows pleasure with the client's accomplishment, it is evidence of increased investment and emotional involvement in the trusting dynamic. Another example of a productive dynamic includes a collaborative dynamic in which members of the group work together to achieve a desired outcome (Fig. 4.6).

Similarly, a problem-solving dynamic in which different members brainstorm solutions and consider potential consequences of different actions typically leads to a productive outcome, and the end result is that important decisions are made and clients feel an increased sense of ownership and control.
If leaders are interpersonally self-disciplined about their mode use and strive to restrain their personal desires for control, approval, and success from influencing their behaviors, it is likely that most groups will be characterized by dynamics that are predominantly productive. However, even when therapists make all the best efforts to sustain productive dynamics, no one is invulnerable to being invited or drawn into a maladaptive dynamic. This is particularly likely in long-standing social systems in which maladaptive ways of relating can become entrenched over time. For this reason, it is critical that you be able to recognize maladaptive dynamics and differentiate them from dynamics that are productive.
All dynamics serve a specific interpersonal need or purpose. Maladaptive dynamics are similar to productive dynamics in that they serve the needs of at least one individual within the system. Distinct from productive dynamics, however, maladaptive dynamics are usually inefficient and involve negative feelings or outcomes for at least one of the involved individuals. An example of a maladaptive dynamic is one that commonly faces parents of adolescents who are struggling to differentiate themselves as individuals and take responsibility for the consequences of their actions. In this dynamic, the adolescent continually seeks guidance from the parents only to protest and explain why the guidance offered is unhelpful or would not work. This is commonly referred to as a help-seeking and help-rejecting dynamic. As a result, all individuals in the system end up feeling frustrated and ungratified. Some examples of maladaptive dynamics that have the potential to affect the process or outcomes of therapy are presented in Table 4.5.
TABLE 4.5
| Dynamic | Description |
|---|---|
| Help seeking–help rejecting | When an individual establishes a pattern of asking for assistance, guidance, or advice and then explaining why it would not work, a help-seeking-help-rejecting dynamic has been established. Potential negative outcomes include frustration or decreased performance in the help seeker. This dynamic is most frequently observed in parent-child relationships or in other relationships involving a power differential. If it is entrenched, it may be replicated within the therapeutic relationship. |
| Competitive | Individuals often compete to obtain an interpersonal need or a valued resource, particularly if it is perceived to be in short supply. If this competition is sustained, potential negative outcomes include conflict between the competitors or feelings of decreased self-esteem in the loser. Although they may occur in any system, competitive dynamics are often observed between siblings, friends, or client peers within a given milieu. |
| Enabling negative behavior | When individuals permit, facilitate, or support the behavior of another individual even though it is negative or potentially harmful, they further enable the negative behavior. The outcome is a continuation or worsening of the behavior. This behavior is frequently observed in couple's relationships or in families in which people are not able to show disapproval or take steps to limit the behavior for fear of disappointing the other individual, making the individual angry, or losing the relationship altogether. |
| Dominance-submission | A dominance-submission relationship is a nondemocratic system that is characterized by a clear power differential that involves the consistent oppression of some individuals by others. Individuals may attempt to dominate others to increase their perceived control over their life circumstances or to compensate for feelings of insecurity or inferiority. Individuals may assume a submissive role because they have limited resources or options for independence; they are accustomed to being mistreated; they have low self-esteem; they perceive themselves as less powerful; they perceive themselves as physically, emotionally, or intellectually inferior; or they wish to avoid confrontation. Potential outcomes include passivity, vulnerability, learned helplessness, or feelings of low self-worth in the submissive individuals. In worst cases, this dynamic evolves into a pattern of emotional, sexual, or physical abuse. These dynamics are most likely to occur in relationships that involve one individual assuming a caregiving role for a more vulnerable individual. Dominant or abusive behaviors suggest that the caregiver is not emotionally capable of functioning in that role and should either seek mental health services immediately or discontinue his or her relationship with the vulnerable individual entirely. |
| Enmeshment | In an enmeshment dynamic, individuals have close ongoing contact. It is expected that individuals share information readily, even if it is highly intimate or personal. There is an expectation that all individuals conform to and share similar worldviews and other behaviors and attitudes. Decision making is shared and the concept of individuality is downplayed. Members of enmeshed systems are fiercely loyal to each other despite conflicts or major transgressions. Caregivers in this dynamic often become overinvolved or controlling in reference to a client's treatment. The potential negative outcomes of an enmeshment dynamic include a closed or secretive system that is difficult for healthcare professionals to enter; psychological dependency between members; a lack of individuality between members; and occasionally feelings of angst or resentment related to the perception that one's efforts are being controlled, stifled, or smothered by the system. Enmeshment dynamics are most often observed in families and couples. |
| Disengagement | Disengagement dynamic occurs when individuals have little contact and do not share personal information readily. Individuals in the system view themselves as independent of one another in terms of worldview, attitudes, behavior, and decision making. The potential negative outcome is a lack of closeness, loyalty, communication, and connection between members. Caregivers in this dynamic are typically underinvolved in the client's care. Potential negative consequences of this dynamic include feelings of isolation and disappointment in others' lack of presence and investment. In worst cases, disengagement within systems can result in the physical or medical neglect of a client. Although they may occur in any system, disengagement dynamics are most often observed in families and couples. |
| Approach-avoidance | When an individual enters a relationship with an expectation that the other will fulfill certain (often unrealistic) needs, there is often a period of intense contact and, in some cases, feelings of closeness. When people are ambivalent about this closeness or when their intentions for the relationships are limited to seeking need fulfillment, they promptly retreat into avoidance. This avoidance may be explained by the fact that they perceived that their needs were not met or by the fact that the relationship became so intense in their minds that it evoked uncomfortable or contradictory feelings (e.g., feeling smothered, fears of abandonment or rejection, feelings of rage, an intense and unfulfilled desire to be admired or unconditionally accepted). When approach-avoidance dynamics occur in couples' relationships, they often involve the same partner repeatedly approaching the other partner to obtain need fulfillment and the other partner repeatedly finding ways to withdraw. Because the approaching partner's needs are not gratified, the approach behaviors become increasingly intense (and sometimes demanding) over time. In return, the avoiding partner continues to find ways to increase withdrawal (e.g., falls asleep, leaves the environment, becomes emotionally unresponsive, is at a loss for words, remains at work later, spends more time with others, focuses more on the children, or turns to substances or other addictions) to counterbalance the approach behavior. The outcome is a relationship characterized by unpredictability, a lack of trust, feeling smothered or abandoned, and a lack of mutuality. Clients who suddenly appear intensely connected and divulge a tremendous amount of personal details during one session only to appear distant or fail to show up for the next session may be enacting this dynamic in therapy. |
| Idealizing-devaluing | Individuals can be consistently idealizing of one another, consistently devaluing, or they can change between the two states. An idealizing dynamic is one in which individuals filter their perceptions of others in such a way that the positive characteristics of the others are exaggerated and any negative characteristics are downplayed or denied entirely. A devaluing dynamic is the opposite in which the negative characteristics are exaggerated. Some individuals have a tendency to relate to and know others only in terms of these two categories. Either state is characterized by an unrealistic and superficial knowledge of others. When others unwittingly allow themselves to become a part of this dynamic, they eventually find it uncomfortable, terrifying, or infuriating. At one moment they may be placed unrealistically on a pedestal only to find that they will be rejected or even vilified in a subsequent interaction. This dynamic is often observed in relationships with healthcare providers (including occupational therapists), particularly when clients, parents, or partners have unrealistic expectations of the provider and do not want to assume sufficient responsibility for the problem or for the solution. |
| Reluctance-reassurance | When an individual (couple, family, or group) is consistently anxious, skeptical, or self-doubting about engaging in occupation and others reliably attempt to bolster, entice, and reassure them, a dynamic of reluctance and reassurance is occurring. Potential negative outcomes of this dynamic include psychological dependency, low intrinsic motivation, and limited opportunities for independence and progress. |
| Demonstrative-voyeuristic | When individuals become involved in elaborating on, embellishing, or dramatizing their reactions or hardships, they often have a need for their hardship to be recognized and validated. When others are entertained by this behavior or do nothing but watch or listen, a demonstrative-voyeuristic dynamic is occurring. Negative outcomes include lack of progress and the eventual realization that the voyeuristic party is taking pleasure in the behavior. Although this realization may only serve to increase the demonstrative behavior, it is neither a therapeutic nor a humane way of relating. If committed by the therapist, this kind of voyeuristic behavior is unethical because it does not represent an attempt to provide best practice. |
| Helpless-rescuing | A helpless-rescuing dynamic occurs when individuals fall into a pattern of recruiting assistance when it is not necessary. Often the helpless behavior is a maladaptive expression of an entrenched need to be loved, attended to, or cared for. For some individuals, this need is strong and exists no matter how much love, care, and attention is provided. The other part of the system enables the helpless behavior by rushing in to assist without recognizing that the behavior is maladaptive. The outcomes include increased dependency on the part of the helpless individual and eventual anxiety or resentment on the part of the rescuers. This dynamic can be culturally contexted and may not always result in maladaptive outcomes for the client. Although it may occur in any system, it is most often observed in parents of disabled children who feel guilty or responsible for the impairment and are unaware of the consequences of enabling the child's helpless behavior. |
| Chaotic-organizing | A chaotic-organizing dynamic is one in which one aspect of a system is irresponsible, disorganized, slovenly, undisciplined, or lacking in emotional self-control. The other part of the system continually seeks to compensate by replacing lost items, reminding the individual of scheduled appointments or necessary tasks, cleaning up and organizing the person's physical environment, or providing required emotional and logistic support so that the person can function. One maladaptive outcome of this dynamic is an ongoing power struggle between the chaotic and organizing aspects of the system. Another consequence is the intensification of the chaotic behavior. Although it may occur in any system, this dynamic is most frequently witnessed in systems in which one member has an impairment that affects cognition, such as attention deficit hyperactivity disorder, bipolar disorder, a psychotic disorder, or another neurological condition. |
| Manipulating-conceding | Some individuals may be accustomed to getting their needs met through manipulation, particularly when they perceive that there may be an obstacle to getting what they want. This involves a pattern of knowing what the other likes or needs, and then giving it out in small doses with the expectation that the other will reciprocate by gratifying the manipulator's needs. When the other party concedes out of feelings of obligation or guilt, the conceding party is fueling the dynamic. Negative outcomes include eventual feelings of resentment and anger in the person enabling the dynamic and a failure to learn to ask for needs in a more direct manner and a failure to accept limits imposed by others in the manipulator. In occupational therapy, this dynamic is often observed when working with parents who struggle to feel confident about disciplinary approaches and often feel guilty about setting limits consistently. It may also be witnessed in couples, friendships, or in student-teacher relationships. If it exists, it is also likely to play out in the therapeutic relationship. |
| Scapegoating | When two or more individuals collude to influence, criticize, reprimand, subjugate, shame, punish, or otherwise control another individual, a scapegoating dynamic has emerged. These dynamics may involve entire families or groups that decide to ally against a single individual. Individuals are most likely to engage in this dynamic when they are allied around a common ideology or when they perceive the scapegoated individual has threatened the status quo or equilibrium of the system or if they feel that the individual is otherwise problematic. Often triangulation reflects a need to displace anger within the system and the most vulnerable, powerless, or emotionally safe individual is usually selected as the convenient target. Although this dynamic is most likely to occur within families or groups, it may also occur when a therapist forms an alliance with one of two parents against the other, with one or more clients against another, or with one partner of a couple against the other. |
In complex and long-standing relationships, multiple dynamics may emerge, some of which may be productive and others of which may be maladaptive. At times, it may be unclear whether a dynamic is ultimately productive or maladaptive. It is common for families, couples, or other social systems to assume that a maladaptive dynamic is productive because it feels familiar and defines the way people have always interacted within the system. Although it may be uncomfortable or painful at times, members participating in the dynamic may be unaware of any need for change. Also possible is that dynamics that were once thought to be positive may become negative over time (and vice versa). The nature and number of potential dynamics that can occur within a given social system are endless.
If a dynamic is prominent within a system, whether one is aware of it or not, it is inevitable that one will be invited or drawn into it when interacting with the system. The difference between being invited to join a maladaptive dynamic or simply drawn into it involves the issue of intentionality. An intentional therapist will recognize the dynamic before becoming involved with it. After identifying the dynamic, the therapist would then use interpersonal reasoning to decide how to interact within the dynamic. An unintentional therapist may not realize that he or she has become involved in the dynamic until his or her involvement has resulted in an interruption or disruption of the client-therapist relationship.
Managing Maladaptive Dynamics of Systems
At one time or another and to varying degrees of intensity, certain maladaptive dynamics are bound to emerge within almost any social system one encounters. The goal of learning about these dynamics is to:
- • Understand their implications for the group and for occupational engagement
- • Anticipate their effects on relationships within the group
- • Remain an objective observer of the dynamic
- • Make an intentional decision about whether and how to manage the dynamic
Even though maladaptive dynamics inevitably involve negative feelings for one or more members, they are very difficult to change. No matter how uncomfortable or unhappy they are, members of the system will habitually act together to sustain the dynamic because this is how they are most accustomed to interacting with one another. This is often the case even if members of the system recognize that sustaining the dynamic results in negative outcomes for the client or group. Because systems are, by nature, highly resistant to change, it is important to continually strive toward an empathic understanding of any social system with which you are working. In striving to understand maladaptive dynamics within a social system, you should:
- • Look to the system for the problem (e.g., all persons involved in the interaction), rather than to the client alone
- • Try to understand why members are invested in sustaining the maladaptive dynamic
What makes sense about the dynamic? What interpersonal needs are served by the members of the system who are enacting the dynamic? How does the dynamic serve the client's needs? What might each of the members lose if they were to stop interacting in this way?
- • Try to assume a historic or multigenerational understanding of the dynamic. When did it begin? Do members of the system have a history of interacting in this way? What is known about the childhood family relationships of those most invested in sustaining the maladaptive dynamic? How do their unique histories make them prime candidates to function in their current roles within the system?
After you have achieved an empathic understanding of the system, the next step is to decide whether to remain an objective observer of the maladaptive dynamics or whether to try to manage or eradicate them. The decision whether to intervene in the dynamic is best made by asking yourself the following questions:
- • Is the dynamic interfering with the course of therapy?
- • Does the group perceive that this dynamic is negatively affecting outcomes?
- • Are certain members of the group attempting to replicate the dynamic within the therapeutic relationship? If so, what are the potential long-term outcomes of this behavior?
If the answer to any of these initial questions is yes, then the IRM recommends that therapists use their interpersonal reasoning to select and change modes while working to attenuate or eradicate a rigid way of interacting. If, through the use of modes, therapists are interpersonally in tune with all of the members of the system, the system will be more amenable to additional systems-focused interventions that might be attempted in the future. The empathizing mode is reliable and effective regardless of the dynamic being addressed. In many cases, it is considered a prerequisite for the use of any other mode because of its powerful ability to allow therapists to create an alliance with any member of the system that is problematic or otherwise in need of empathy. Maladaptive dynamics create an emotional environment that is often characterized by tension and feelings of vulnerability in various members of the system. The empathizing mode is often effective in reducing tension and bolstering peoples' self-confidence. If therapists explain the importance of hearing all voices upfront and then take the time and effort to hear and validate the perspectives of each member, a precedent for such behavior will be set within the system. The end result of beginning with an empathic approach toward the system is that members are ultimately primed to accept other modes and work to more receptively toward systems change (Fig. 4.7).

Applying Intentional Relationship Model to Coleadership Situations
The interpersonal dynamics within a group become more complex when there is more than one leader present. When coleading a group with another occupational therapist (or other professional), each therapist should be aware of the primary modes he or she is using and the effect of these modes on group dynamics. According to IRM, therapists should know what their strong and weak modes are so that they may use each other's strengths to compensate for their own limitations while leading the group. The use of different modes and their effects on the different members and on the group dynamic as a whole should be discussed openly between coleaders before and after each session. Adjustments in mode use should be made if it is determined that a certain mode or dynamic between the coleaders is enabling counterproductive dynamics to occur within the group. Intentional use of modes by each coleader will increase the likelihood of occupational engagement for all group members and improve the overall dynamics and mood of exchange between members.
CASE EXAMPLE: APPLYING IRM TO A CHILD'S PLAYGROUP
Three young girls, Alex, 11 years old; Iris, 9 years old; and Elizabeth, 11 years old, have routinely been placed into a group dynamic to focus on individual goals that address the ability to successfully function within group settings for return to a school environment. The group goals are for interactive imaginative play, rule following, and turn taking. In addition to group goals, each child has goals addressing deficits found that limit her ability for successful participation in school-based groups.
Alex is recovering from a head injury with deficits most significantly observed in short-term memory, initiation, abstraction, and other executive functions. Although her processing of speech is slow, she is open and social in her communication style and demonstrates a high level of comfort and trust with all therapists in the clinic. She presents with a mothering personality toward the younger children in the clinic; however, at times she is overly controlling within a group setting, offering uninvited assistance that overwhelms others in the group. She frequently looks for approval from the therapist when she is assisting the other children. When confronted with challenges or change, she opts for tasks that are easy for her to perform and below her capacity cognitively and socially. Her affect is bright and positive in conditions she is familiar with, but she has difficulty receiving feedback in her areas of deficits. She is open to touch and responds well to all levels of diversity, although she is withdrawn when in a room with an unfamiliar man. She frequently seeks out the therapist for affirmation of a job well done. An area of significant difficulty is her limited ability to provide feedback during group planning and decision making. She also has endurance and mild standing balance deficits. Individually and within the group setting encouraging mode and empathizing mode work best with Alex.
Iris is a 9-year-old girl recovering from removal of a malignant brain tumor followed by chemotherapy. She is in remission at this point. Her rehabilitation goals focus specifically on behavioral issues, emotional regulation, and cognitive deficits of attention to detail, divided attention, and impulsivity. Her interpersonal characteristics are representative of her behavioral and cognitive deficits. She is verbose and intrusive in her communication. She frequently interrupts the other children in the group and is tangential in her thoughts. Her need for control is very high. She frequently attempts to dominate the sessions and others and is manipulative in interactions with the other girls and therapists. She displays decreased capacity for trust, requesting frequent feedback from the therapist or others confirming their intentions. In conjunction with this, her intrusiveness occurs during group and individual tasks, frequently attempting to control the activity, conversation, or less outgoing group participants. She is overly assertive of her needs; however, her impulsivity predisposes her to spontaneously report her internal feelings on every subject. She is resistant to participate in tasks and activities that she has not identified as her own and attempts to bargain with the therapist to “get her way.” She also frequently refuses to perform tasks that may challenge her cognitively or physically. Her emotional regulation displays itself most frequently when she is challenged or feels she has not been allowed to do what she wants. Tantrums and physical threats toward the therapist occur when she senses she has lost control. She also appears to have a decreased capacity for touch because this frequently results in an aggressive response. This also occurs when limits are set or feedback is provided to her regarding her behavior or performance. Her verbosity includes providing unsolicited feedback to others in a group. The interpersonal characteristics of relating toward others, response to diversity, and capacity for reciprocity are immaturely developed in her at this time. Physical deficits include mild visual neglect and advanced balance deficits. Mode selection is much different with Iris in an individual setting than in a group setting. Individually, she at times works well in instructing and problem-solving mode; however, use of these modes in a group setting consistently creates power dilemmas (Fig. 4.8). Within a group setting, empathizing mode is most effective at this time.

Elizabeth is an 11-year-old child with cerebral palsy from birth. She has no cognitive deficits; however, she is socially withdrawn and tactile defensive. Her communication style is much better in one-on-one sessions than in group settings. She appears reluctant to offer her opinion or choices for activities and withdraws when encouraged. Her initial decreased capacity for trust of other children and therapists is evident in nonverbal cues, such as standing in the background, making limited eye contact, and responses during group discussions or activity selection. Elizabeth has a problematically low need for control. She appears passive during most tasks and is dominated by the others in the group. She is indirect in her assertion of her needs and appears to lack confidence in her abilities through statements, such as “I'm not good at that” or “I'm slow at everything I do.” Because of this decreased self-confidence she is reluctant during tasks or activities that are new to her or perceived to be beyond her capacity. She does well with encouragement when in one-on-one sessions, often surprising herself when she achieves something new; however, this has not transitioned to behavior noted in group settings. Despite appearing anxious and shy, her affect and emotional regulation are good. She receives feedback and incorporates it; however, she rarely provides feedback, and when solicited, she is hesitant. Her sensitivity to others is significant. She demonstrates a high level of empathy toward other children, and when given an opportunity to assist another, her affect brightens and her engagement increases. She responds well to diversity and relates well with her therapists. She prefers limited touch and does best with deep pressure, and this has created difficulty in group settings. Her capacity for reciprocity between herself and other children is high. She demonstrates the ability for increased tolerance and patience in all scenarios and often expresses gratitude to others when she has received outside help. She presents physically with decreased functional use of her right upper extremity for fine motor and gross motor tasks, decreased standing balance, and ability for transitional movements into and out of positions. During one-on-one sessions, Elizabeth functions very well when the therapist uses collaborating and problem-solving modes. In a group setting, she also functions well with these; however, encouraging mode and empathizing mode are used more successfully.
The group sessions with these three clients at times will focus on engaging in a form of parallel play; however, the majority of the time, the main goal is for the clients to work together to create or achieve some end result as a unified group. The various interpersonal characteristics of the clients have created both productive and maladaptive dynamics. Because of her interpersonal characteristics, Iris presents both as the most prominent influence in the group and the most engaged. This creates difficulties for the therapist, because Iris exerts her power at times to the extent that it affects the group in a negative way. When Iris is allowed to manipulate and control the group activities and individuals, the emotional tone of the group becomes less goal focused as a team, and often the end result is failure to successfully complete the group project. The other negative result is continuation of interpersonal characteristics that are reinforcing the inability of each of the girls to be a successful participant in group environments. Another dynamic that exists within the group is the dynamic between Alex and Elizabeth. This dynamic has mixed results in that it can be productive in facilitating a helping emotion within the group environment, but, when allowed to dominate, it is maladaptive for Elizabeth's independence and creates a conflict in Iris, because she feels left out of the group dynamic.
The intentional choice made by the occupational therapist is to use empathizing mode with advancement to collaboration mode during group activities. Other mode use is observed; however, these two facilitate the most productive dynamic scenarios during group play. The following is an example of the group in a recent treatment session:
The three girls quickly engage with each other in the kid's playroom. Alex and Elizabeth hold hands as they are walking into the room, and Iris runs in front of them. Once the group has settled, discussion on the activity selection for the day begins. Alex and Elizabeth agree that they should do coloring, and Iris shouts out that coloring is boring and they should do puzzles. Using empathizing mode, the therapist agrees that each of those activities sounds like a good idea but reminds the group that the goal is to do a big project together. The therapist suggests that the girls work together on a big activity and at the end of the session they can have 10 minutes of free-choice time. All the group members agree to this with positive affect. Sitting together in a circle on the floor, the group begins to think and imagine what fun story they can make up. The therapist asks each girl to provide input, taking turns creating a narrative of an imaginary journey of three girls traveling to a far-off land. Iris begins to dominate the story; however, the therapist, using empathizing mode, suggests that, although all her ideas are good, they will start with only one of the good ideas. Iris does not feel deflated by this and instead chooses one aspect of her story to incorporate. The therapist then asks either Alex or Elizabeth to go next. Both girls hesitate, but, using empathizing mode again, the therapist, hoping to work on some memory areas, suggests to Alex that she might have good ideas from a story she has read or heard recently. She struggles to come up with an idea, but with some cueing is able to. The therapist used encouraging mode to reinforce to the group what good turn-taking they are doing and how good the story is sounding. Next it is Elizabeth's turn to add to the narrative. Despite having the strongest cognitive skills and ability to abstract, her withdrawn behavior makes this activity challenging. Alex appears to sense this and begins to provide suggestions, which is most interesting because she was unable to come up with ideas while it was her turn. Iris also begins to verbalize her ideas, which creates a dynamic furthering Elizabeth's decreased ability to provide feedback. Using empathizing mode, the therapist reinforces that each girl's ideas are good ones; however, the goal of the story making is that everyone has a chance to add an original idea. The therapist, using empathizing mode, moves very slightly in front of Elizabeth between her and the other girls to give her a sense of separation while she thinks. Elizabeth suggests two ideas and, using collaboration mode, the therapist asks the group to decide which of the two good ideas Elizabeth came up with they should put into their story. Elizabeth's affect is obviously more engaged by this. The group discusses how the story would sound with each idea and together make a decision. The group goal is to act out the narrative to a successful completion. Using IRM, this therapist's intentional incorporation of mode use allowed the group to successfully complete the creation of a narrative with each individual participating as an equal component of a productive dynamic.
SUMMARY
As noted in the beginning of this chapter, OT is rich in literature supporting the effectiveness of a successful client-therapist relationship. Despite this, there has been an absence of a model for therapists to use as a source for developing concrete skills and competencies that are necessary to enact them within a clinical setting. This chapter introduced the IRM, and offers it as that source for skill development and competencies in group and individual OT settings. IRM provides a theoretical framework for understanding the significance that all interactions have and guidance in how to therapeutically respond in a manner that best serves the client. The defined suggestions for therapeutically responding to client interpersonal characteristics and inevitable interpersonal events are invaluable tools for any therapist. Introduction and instruction in six therapist interpersonal modes for relating to clients were provided both for individual treatment and group dynamics. The case example allowed the reader the opportunity to evaluate the significant effect of understanding clients' interpersonal characteristics and planned therapeutic mode use has on successful therapist-client interactions and productive versus maladaptive dynamics within the group. The combined elements of the IRM are established guides for better understanding the client, the interpersonal events that occur in therapy, and what the therapist brings to the situation and the occupation. IRM offers a tool for occupational therapists to learn how to understand the theoretical framework of therapeutic use of self and guidance in effectively positioning the client as the focal point of each therapy session, individual or group, for successful engagement in occupational tasks.
REVIEW QUESTIONS
- 1. What are the four main components of the therapist-client relationship that are the focus of IRM?
- 2. When a therapist is planning a treatment session with a given client, the choice and application of a particular therapeutic mode or set of modes depend on two major qualities that the client brings to the therapy session. Describe these.
- 3. A dynamic defines the distinctive quality, emotional tone, and specific interpersonal events that compose an interaction between individuals. Dynamics can be defined as productive or maladaptive. Provide one example for each.
- 4. In the case example that was provided, identified modes were empathizing, encouraging, and collaborative. As you read through the descriptions of the events of the group, another mode was used but not identified in the description. Based on reviews of the events, what other mode may have been used?
- 5. In the group case example, describe how the dynamic between Alex and Elizabeth is a productive dynamic for the group.
- 6. In the group case example, describe how the dynamic between Alex and Elizabeth is maladaptive.
- 7. Failure of a therapist to notice or understand a communication from a client or communication or behavior initiated by the therapist that is perceived by the client as hurtful or insensitive is what form of inevitable interpersonal event?
References
American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process. American Journal of Occupational Therapy, 74(Suppl. 2), 7412420010. https://doi.org/10.5014/ajot.2020.74S2001
Ayres-Rosa, S., & Hasselkus, B. R. (1996). Connecting with patients: the personal experience of professional helping, Occup Ther J Res, 16, 245–260.
Cole, B., & McLean, V. (2003). Therapeutic relationships re-defined, Occup Ther Mental Health, 19(2), 33–56.
Kielhofner, G. (2009). Conceptual foundations of occupational therapy (4 ed.). FA Davis.
Taylor, R. (2020). The intentional relationship: Occupational therapy and use of self. (2nd ed.). FA Davis.
Taylor, R., Lee, S., Kielhofner, G., & Ketkar, M. (2009). Therapeutic use of self: a nationwide survey of practitioners' attitudes and experience. American Journal of Occupational Therapy, 63, 182–207