13: Labor and birth processes
Kitty Cashion
 http://evolve.elsevier.com/Perry/maternal
http://evolve.elsevier.com/Perry/maternal
During late pregnancy, the woman and fetus prepare for the labor process, a series of events by which the fetus is expelled from the uterus. The fetus has grown and developed in preparation for extrauterine life. The woman has undergone various physiologic adaptations during pregnancy that prepare her for giving birth and for motherhood. Labor and birth represent the end of pregnancy, the beginning of extrauterine life for the newborn, and a change in the lives of the family. This chapter discusses the factors affecting labor, the processes involved, the normal progression of events, and the adaptations made by both the woman and the fetus.
Factors affecting labor
At least five factors affect the process of labor and birth. These are easily remembered as the five Ps: passengers (fetus and placenta), passageway (birth canal), powers (contractions), position of the mother, and psychologic response. The first four factors are presented here as the basis for understanding the physiologic process of labor. The fifth factor is discussed in Chapter 16. Other factors can influence the woman’s labor and birth experience, including place of birth, preparation, type of provider (e.g., obstetrician or family medicine physician, nurse midwife), nursing care, presence of a support person, and procedures. These factors are discussed generally in Chapter 16 as they relate to nursing care during labor.
Passenger
The way the passenger—or fetus—moves through the birth canal is determined by several interacting factors: the size of the fetal head, fetal presentation, fetal lie, fetal attitude, and fetal position. Because the placenta also must pass through the birth canal, it can be considered a passenger along with the fetus; however, the placenta rarely interferes with the process of labor in a normal vaginal birth. An exception is the case of placenta previa (see Chapter 12).
Size of the fetal head
Because of its size and relative rigidity, the fetal head has a major effect on the birth process. The fetal skull is composed of two parietal bones, two temporal bones, the frontal bone, and the occipital bone (Fig. 13.1A). These bones are united by connective tissue sutures: sagittal, lambdoidal, coronal, and frontal (see Fig. 13.1B). The areas where more than two bones meet are called fontanels. During labor—after rupture of membranes—palpation of fontanels and sutures during vaginal examination reveals fetal presentation, position, and attitude.

Part A shows the lateral view of the skull with the front bone labelled as frontal bone and the next bone labelled as parietal bone, the bone below it labelled as temporal bone along with the bone behind it labelled as occipital bone. Part B shows a view above of the skull from above with a frontal suture present in between the frontal bone and coronal sutures between frontal bone and the presence of anterior fontanel present at the junction of the frontal and coronal suture. Sagittal suture present between parietal bone and lambdoid suture present between parietal bone and occipital bone with the presence of posterior fontanel.
The two most important fontanels are the anterior and posterior (see Fig. 13.1B). The larger of these, the anterior fontanel, is diamond shaped—approximately 3 cm by 2 cm—and lies at the junction of the sagittal, coronal, and frontal sutures. It closes by 18 months after birth. The posterior fontanel lies at the junction of the sutures of the two parietal bones and the occipital bone, is triangular, and is approximately 1 cm by 2 cm. It closes 6 to 8 weeks after birth.
Sutures and fontanels make the skull flexible to accommodate the infant brain, which continues to grow for some time after birth. However, because the bones are not firmly united, slight overlapping or molding of the shape of the head occurs during labor. This capacity of the bones to slide over one another also permits adaptation to the various diameters of the maternal pelvis. Molding can be extensive, but the heads of most newborns assume their normal shape within 3 days after birth (see Fig. 22.14).
Although the size of the fetal shoulders may affect passage, their position can be altered relatively easily during labor, so one shoulder may occupy a lower level than the other. This creates a shoulder diameter that is smaller than the skull, facilitating passage through the birth canal. After the birth of the head and shoulders, the rest of the body usually emerges quickly.
Fetal presentation
Presentation refers to the part of the fetus that enters the pelvic inlet first and leads through the birth canal during labor at term. The three main presentations are cephalic presentation (head first), occurring in approximately 97% of births (Fig. 13.2); breech presentation (buttocks, feet, or both first), occurring in approximately 3% of births (Fig. 13.3A–C); and shoulder presentation, seen in fewer than 1% of births (see Fig. 13.3D) (Cunningham, Leveno, Bloom, et al., 2018). The presenting part is that part of the fetus that lies closest to the internal os of the cervix. It is the part of the fetal body first felt by the examining finger during a vaginal examination. In a cephalic presentation, the presenting part is usually the occiput; in a breech presentation it is the sacrum; in the shoulder presentation it is the scapula. When the presenting part is the occiput, the presentation is noted as vertex (see Fig. 13.2). Factors that determine the presenting part include fetal lie, fetal attitude, and extension or flexion of the fetal head.

A graphic representation of fetal vertex, the image is divided into four quadrants where the right quadrants show the image where the baby's head is turned towards the right side, the top image represents the Right occipitoposterior position, the middle image represents the right occipitotransverse and the bottom image represents the Right occipitoanterior position. The left quadrants show the image where the baby's head is turned towards the left side, the top image represents the left occipitoposterior position, the middle image represents the left occipitotransverse and the bottom image represents the left occipitoanterior position.

A multi-part image labelled A through D. A: Frank breech: shows the sacrum of the fetus entering the pelvis. Lie: longitudinal or vertical, presentation: breech (incomplete), presenting part: Sacrum, attitude: Flexion, except for legs at knees.
B: Single footling breech: the sacrum at the pelvis with one of the legs already out of the pelvis. Lie: longitudinal or vertical, presentation: breech (incomplete), presenting part: sacrum, attitude: flexion, except for one leg extended at hip and knee.
C: Complete breech: the sacrum at the pelvis with legs folded together. Lie: longitudinal or vertical, presentation: breech (sacrum and feet presenting), presenting part: sacrum (with feet), attitude: general flexion.
D: Shoulder presentation: the shoulder of the fetus entering the pelvis. Lie: transverse or horizontal, presentation: shoulder, presenting part: scapula, attitude: flexion.
Fetal lie
Lie is the relation of the long axis (spine) of the fetus to the long axis (spine) of the mother. The two primary lies are longitudinal—or vertical—in which the long axis of the fetus is parallel with the long axis of the mother (see Fig. 13.2); and transverse, horizontal, or oblique, in which the long axis of the fetus is at a right angle diagonal to the long axis of the mother (see Fig. 13.3D). Longitudinal lies are either cephalic or breech presentations, depending on the fetal structure that first enters the mother’s pelvis. Vaginal birth cannot occur when the fetus stays in a transverse lie. An oblique lie, one in which the long axis of the fetus is lying at an angle to the long axis of the mother, is less common and usually converts to a longitudinal or transverse lie during labor (Cunningham et al., 2018).
Fetal attitude
Attitude is the relation of the fetal body parts to one another. The fetus assumes a characteristic posture (attitude) in utero partly because of the mode of fetal growth and partly because of the way the fetus conforms to the shape of the uterine cavity. Normally, the back of the fetus is rounded so the chin is flexed on the chest, the thighs are flexed on the abdomen, and the legs are flexed at the knees. The arms are crossed over the thorax, and the umbilical cord lies between the arms and the legs. This attitude is termed general flexion (see Fig. 13.2).
Deviations from the normal attitude may cause difficulties during birth. For example, in a cephalic presentation, the fetal head may be extended or flexed in a manner that presents a head diameter that exceeds the limits of the maternal pelvis, leading to prolonged labor, forceps- or vacuum-assisted birth, or cesarean birth.
Certain critical diameters of the fetal head can be measured by ultrasound. The biparietal diameter, which is about 9.25 cm at term, is the largest transverse diameter and an important indicator of fetal head size (Fig. 13.4B). In a well-flexed cephalic presentation, the biparietal diameter is the widest part of the head entering the pelvic inlet. Of the several anteroposterior diameters, the smallest and the most critical one is the suboccipitobregmatic diameter (about 9.5 cm at term) (see Fig. 13.4-A). When the head is in complete flexion, this diameter allows the fetal head to pass easily through the true pelvis (Fig. 13.5A). As the head is more extended, the anteroposterior diameter widens, and the head may not be able to enter the true pelvis (see Fig. 13.5).

A two-part image labelled A and B.
A: The diameters of the skull in the transverse section. Labels from left: mentum (chin), sinciput, vertex, occiput. Occipitofrontal diameter: 12 centimetre, occipitomental diameter: 13.5 centimetre, suboccipitobregmatic diameter: 9.5 centimetre.
B: The diameters of the skull from above in the transverse plane. Labels from top to bottom: Occiput, biparietal: 9.25 centimetre, vertex, sinciput.

Part A shows the chin touching the upper part of the chest and the smallest diameter of the head entering the pelvis. Part B shows the extension of the head and the part of the head with a larger diameter entering the pelvis. Part C shows the complete extension of the head and the part of the head with the largest diameter entering the pelvis.
Fetal position
The presentation, or presenting part, indicates that portion of the fetus that overlies the pelvic inlet. Position is the relationship of a reference point on the presenting part (occiput, sacrum, mentum [chin] or sinciput [deflexed vertex]) to the four quadrants of the mother’s pelvis (see Fig. 13.2). Position is denoted by a three-letter abbreviation. The first letter of the abbreviation denotes the location of the presenting part in the right (R) or left (L) side of the mother’s pelvis. The middle letter stands for the specific presenting part of the fetus (O for occiput, S for sacrum, M for mentum [chin], and Sc for scapula [shoulder]). The final letter stands for the location of the presenting part in relation to the anterior (A), posterior (P), or transverse (T) portion of the maternal pelvis. For example, ROA means that the occiput is the presenting part and is located in the right anterior quadrant of the maternal pelvis (see Fig. 13.2 ROA). LSP means that the sacrum is the presenting part and is located in the left posterior quadrant of the maternal pelvis (see Fig. 13.3A or C).
Station is the relationship of the presenting fetal part to an imaginary line drawn between the maternal ischial spines and is a measure of the degree of descent of the presenting part of the fetus through the birth canal. The placement of the presenting part is measured in centimeters above or below the ischial spines (Fig. 13.6). For example, when the lowermost portion of the presenting part is 1 cm above the spines, it is noted as being minus (−) 1. At the level of the spines, the station is referred to as 0 (zero). When the presenting part is 1 cm below the spines, the station is said to be plus (+) 1. Birth is imminent when the presenting part is at +4 to +5 cm. The station of the presenting part should be determined when labor begins so the rate of descent of the fetus during labor can be assessed accurately.

A figure shows a pelvis with a ten point scale. Points on the scale are marked at a distance of one centimetre each. The points above the ischial spine are marked with a negative sign and points below the ischial spine are marked with a positive sign. The points are numbered from the top starting from negative five, through positive five at the bottom. The scale represents the placement of the presenting part, measured in centimetres above or below the ischial spines.
Engagement is the term used to indicate that the largest transverse diameter of the presenting part (usually the biparietal diameter) has passed through the maternal pelvic brim or inlet into the true pelvis and usually corresponds to station 0. It often occurs in the weeks just before labor begins in nulliparas and may occur before or during labor in multiparas. Engagement can be determined by abdominal or vaginal examination.
Passageway
The passageway, or birth canal, is composed of the mother’s rigid bony pelvis and the soft tissues of the cervix, the pelvic floor, the vagina, and the introitus (the external opening to the vagina). Although the soft tissues, particularly the muscular layers of the pelvic floor, contribute to vaginal birth of the fetus, the maternal pelvis plays a far greater role in the labor process because the fetus must successfully accommodate itself to this relatively rigid passageway. The size and shape of the pelvis can be determined at the initial prenatal visit or on admission in labor. This information can then be used in the assessment of labor progress (Thorp & Grantz, 2019).
Bony pelvis
The anatomy of the bony pelvis is described in Chapter 3. The following discussion focuses on the importance of pelvic configurations as they relate to the labor process. (It may be helpful to refer to Figs. 3.4 and 3.5.)
The bony pelvis is formed by the fusion of the ilium, ischium, pubis, and sacral bones. The four pelvic joints are the symphysis pubis, the right and left sacroiliac joints (Fig. 13.7A), and the sacrococcygeal joint (see Fig. 13.7B). The bony pelvis is separated by the brim, or inlet, into two parts: the false and the true pelves. The false pelvis is the part above the brim and plays no part in childbearing. The true pelvis, the part involved in birth, is divided into three planes: the inlet, or brim; the midpelvis, or cavity; and the outlet.

Part A shows a pelvis from above with the labels for transverse diameter marked for the vertical line, anteroposterior diameter marked for the vertical line, pubic bone, and symphysis pubis marked in the anterior region. Part B shows the parts of the pelvic bone when viewed from below which shows pubic arch ischial tuberosity in the anterior region and sacrococcygeal joint and coccyx in the posterior region.
The pelvic inlet, which is the upper border of the true pelvis, is formed anteriorly by the upper margins of the pubic bone, laterally by the iliopectineal lines along the innominate bones, and posteriorly by the anterior upper margin of the sacrum and the sacral promontory.
The pelvic cavity, or midpelvis, is a curved passage with a short anterior wall and a much longer concave posterior wall. It is bounded by the posterior aspect of the symphysis pubis, the ischium, a portion of the ilium, the sacrum, and the coccyx.
The pelvic outlet is the lower border of the true pelvis. Viewed from below it is ovoid; somewhat diamond shaped, and bounded by the pubic arch anteriorly, the ischial tuberosities laterally, and the tip of the coccyx posteriorly (see Fig. 13.7B). In the latter part of pregnancy, the coccyx is movable (unless it has been previously fractured and has fused to the sacrum during healing).
The pelvic canal varies in size and shape at various levels. The diameters at the plane of the pelvic inlet, midpelvis, and outlet, plus the axis of the birth canal (Fig. 13.8), determine whether vaginal birth is possible and the manner by which the fetus may pass down the birth canal.

A: The frontal view of the pelvic cavity with the diameters at the plane of the pelvic inlet highlighted. The plane of inlet is the midplane, plane below it has the greatest dimension and the plane near the coccyx has the least dimension. The ischial spine and ischial tuberosity are also labelled. B: The side view of the pelvis with the labels for inlet, midplane, and outlet. C: The side view of the pelvis showing the axis of the birth canal with a plummet and the curve of sacrum represented by a curved arrow. Ischial spine and ischial tuberosity are labelled.
The subpubic angle, which determines the type of pubic arch, together with the length of the pubic rami and the intertuberous diameter, is of great importance. Because the fetus must first pass beneath the pubic arch, a narrow subpubic angle is less accommodating than a rounded wide arch. The method of measurement of the subpubic arch is shown in Fig. 13.9. A summary of obstetric measurements is given in Table 13.1.

An illustration of perineal view of a female shows gloved hands stretching the upper lips of vulva apart with each thumb while the hands are placed on each inner thigh.
Source: (From Barkauskas, V. H., Baumann, L. C., & Darling-Fisher, C. S. [2002]. Health and physical assessment [3rd. ed.]. St. Louis: Mosby.)| Plane | Diameter | Measurements |
|---|---|---|
| Inlet (Superior Strait) |

An illustration of midsagittal view of a woman with a fetus in her womb shows middle and index fingers of one hand inserted straight inside the vaginal canal while the index finger of the other hand is placed below the index finger on the lateral side. Length of diagonal conjugate (solid colored line), obstetric conjugate (broken colored line), and true conjugate (blue line)a |
|
|
Obstetric: measurement that determines whether presenting part can engage or enter superior strait |
||
| Midplane | 10.5 cm |
|
|
Transverse diameter (interspinous diameter) The midplane of the pelvis normally is its largest plane and the one of greatest diameter |

An illustration shows index finger inserted in the pelvic girdle and touching the right side of the coccyx and an arrow shows its movement from left to right. Measurement of interspinous diametera |
|
| Outlet | ≥8 cm |
|

An illustration of perineal view of a female shows gloved hands of an examiner supporting the Thom’s pelvimeter over each ischial tuberosity with each thumb. Use of Thom’s pelvimeter to measure intertuberous diametera |
aFrom Seidel, H. M., Ball, J. W., Dains, J. E., et al. (2011). Mosby’s guide to physical examination (7th ed.). St. Louis: Mosby.
The four basic types of pelves are classified as follows:
The gynecoid pelvis is the most common, with major gynecoid pelvic features present in approximately 50% of all women. Anthropoid and android features are less common, and platypelloid pelvic features are the least common. Mixed types of pelves are more common than are pure types (Cunningham et al., 2018). Examples of pelvic variations and their effects on mode of birth are given in Table 13.2.
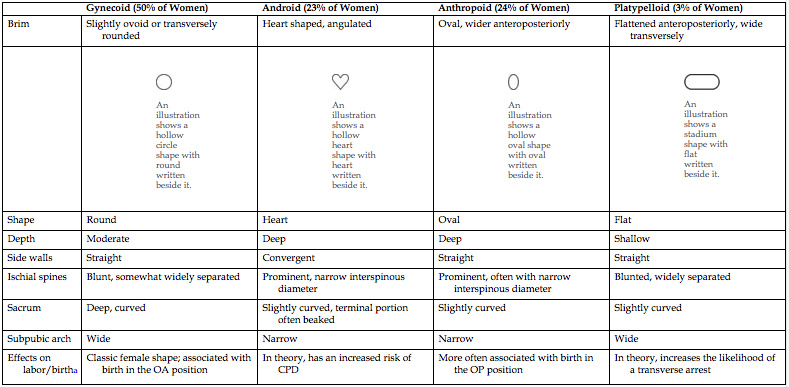
| Gynecoid (50% of Women) | Android (23% of Women) | Anthropoid (24% of Women) | Platypelloid (3% of Women) | |
|---|---|---|---|---|
| Brim | Slightly ovoid or transversely rounded | Heart shaped, angulated | Oval, wider anteroposteriorly | Flattened anteroposteriorly, wide transversely |

An illustration shows a hollow circle shape with round written beside it. |

An illustration shows a hollow heart shape with heart written beside it. |

An illustration shows a hollow oval shape with oval written beside it. |

An illustration shows a stadium shape with flat written beside it. |
|
| Shape | Round | Heart | Oval | Flat |
| Depth | Moderate | Deep | Deep | Shallow |
| Side walls | Straight | Convergent | Straight | Straight |
| Ischial spines | Blunt, somewhat widely separated | Prominent, narrow interspinous diameter | Prominent, often with narrow interspinous diameter | Blunted, widely separated |
| Sacrum | Deep, curved | Slightly curved, terminal portion often beaked | Slightly curved | Slightly curved |
| Subpubic arch | Wide | Narrow | Narrow | Wide |
| Effects on labor/birtha | Classic female shape; associated with birth in the OA position | In theory, has an increased risk of CPD | More often associated with birth in the OP position | In theory, increases the likelihood of a transverse arrest |
aData from Kilpatrick, S., Garrison, E., & Fairbrother, E. (2021). Normal labor and delivery. In M. B. Landon, H. L Galan, E. R. M. Jauniaux, et al. (Eds.), Gabbe’s obstetrics: Normal and problem pregnancies (8th ed.). Philadelphia: Elsevier.
CPD, Cephalopelvic disproportion; OA, occipitoanterior; OP, occipitoposterior.
Assessment of the bony pelvis can be performed during the first prenatal evaluation and need not be repeated if the pelvis is of adequate size and suitable shape. In the third trimester of pregnancy, the examination of the bony pelvis may be more thorough, and the results more accurate because there is relaxation and increased mobility of the pelvic joints and ligaments as a result of hormonal influences. Widening of the joint of the symphysis pubis and the resulting instability may cause pain in any or all of the pelvic joints.
Because the examiner does not have direct access to the bony structures and because the bones are covered with varying amounts of soft tissue, estimates of size and shape are approximate. Precise bony pelvis measurements can be determined by use of radiographic computed tomography (CT) or magnetic resonance imaging (MRI). However, these procedures are rarely performed for this purpose because evidence is lacking that they are beneficial. Indeed, some data show possible harm associated with their use because of an increase in cesarean birth rates (Kilpatrick, Garrison, & Fairbrother, 2021). Even precise measurements do not always predict a woman’s ability to give birth vaginally because of the many ways the fetus can negotiate the pelvis and the accommodation of maternal soft tissues. Therefore, pelvimetry results rarely contraindicate a trial of labor.
Soft tissues
The soft tissues of the passageway include the distensible lower uterine segment, the cervix, the pelvic floor muscles, the vagina, and the introitus. Before labor begins, the uterus is composed of the uterine body (corpus) and the cervix (neck). After labor has begun, uterine contractions cause the uterine body to have a thick and muscular upper segment and a thin-walled, passive, muscular lower segment. A physiologic retraction ring separates the two segments (Fig. 13.10). The lower uterine segment gradually distends to accommodate the intrauterine contents as the wall of the upper segment thickens and its accommodating capacity is reduced. The contractions of the uterine body thus exert downward pressure on the fetus, pushing it against the cervix.

Part A shows the uterus of a non-pregnant individual with the labels for body, isthmus, and cervix. Part B shows the uterus in the early stage with closed internal os and external os. Part C shows the uterus in the second stage with the active segment marked above the physiological retraction ring and the passive segment marked below the physiological retraction ring till the external os. Part D shows completed opened internal and external orifice and the presence of the pathological ring.
The cervix effaces (thins) and dilates (opens) sufficiently to allow the first fetal portion to descend into the vagina. As the fetus descends, the cervix is actually drawn upward and over this first portion.
The pelvic floor is a muscular layer that separates the pelvic cavity above from the perineal space below. This structure helps the fetus rotate anteriorly as it passes through the birth canal. Chapter 7 describes changes in the vagina that occur during pregnancy. At term, the vagina can dilate to accommodate the fetus and permit its passage to the external world.
Powers
Involuntary and voluntary powers combine to expel the fetus and placenta from the uterus. Involuntary uterine contractions, called the primary powers, signal the beginning of labor. Once the cervix has dilated, voluntary bearing-down efforts by the woman, called the secondary powers, augment the force of the involuntary contractions.
Primary powers
The involuntary contractions originate at certain pacemaker points in the thickened muscle layers of the upper uterine segment. From the pacemaker points, contractions move downward over the uterus in waves, separated by short rest periods. Terms used to describe these involuntary contractions include frequency (the time from the beginning of one contraction to the beginning of the next), duration (length of contraction), and intensity (strength of contraction at its peak).
The primary powers are responsible for the effacement and dilation of the cervix and descent of the fetus. Effacement of the cervix means the shortening and thinning of the cervix during the first stage of labor. The cervix, normally 2 to 3 cm long and approximately 1 cm thick, is obliterated or “taken up” by a shortening of the uterine muscle bundles during the thinning of the lower uterine segment that occurs in advancing labor. Only a thin edge of the cervix can be palpated by an examiner when effacement is complete. Effacement generally progresses significantly in first-time term pregnancy before more than slight dilation occurs. In subsequent pregnancies, effacement and dilation of the cervix tend to progress together. Degree of effacement is expressed in percentages, from 0% to 100% (e.g., a cervix is 50% effaced) (Fig. 13.11A–C).
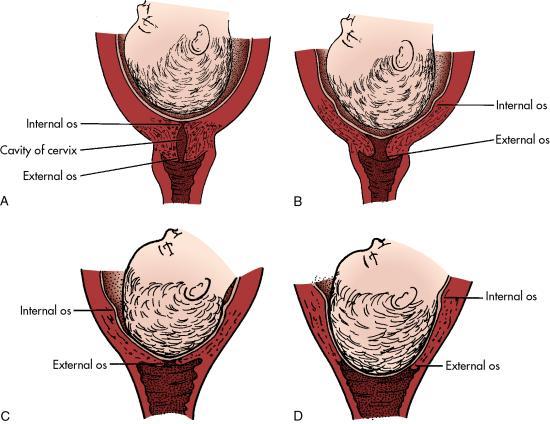
Part A shows the closed internal os of the cervix along with the head of the fetus present in the uterus towards the cervix. Part B shows the opening of the internal os with the head moved towards the cervix. Part C shows the head of the fetus well placed in the fetus. Part D shows the complete dilation of the cervix and the opening of the external orifice.
Dilation of the cervix is the enlargement or widening of the cervical opening and the cervical canal that normally occurs once labor has begun. The diameter of the cervix increases from less than 1 cm to full dilation (approximately 10 cm) to allow birth of a term fetus. When the cervix is fully dilated (and completely retracted), it can no longer be palpated by an examiner (see Fig. 13.11D). Full cervical dilation marks the end of the first stage of labor.
Dilation of the cervix occurs by the drawing upward of the musculofibrous components of the cervix, caused by strong uterine contractions. Pressure exerted by the amniotic fluid while the membranes are intact or by the force applied by the presenting part can promote cervical dilation. Scarring of the cervix as a result of prior infection or surgery may slow cervical dilation.
In the first and second stages of labor, increased intrauterine pressure caused by contractions exerts pressure on the descending fetus and the cervix. When the presenting part of the fetus reaches the perineal floor, mechanical stretching of the cervix occurs. Stretch receptors in the posterior vagina cause release of endogenous oxytocin that triggers the maternal urge to bear down, or the Ferguson reflex.
Uterine contractions are usually independent of external forces. For example, laboring women who are paralyzed because of spinal cord lesions above the twelfth thoracic vertebra have normal but painless uterine contractions. In addition, use of epidural analgesia during labor does not decrease the frequency or intensity of contractions (Cunningham et al. 2018).
Secondary powers
As soon as the presenting part reaches the pelvic floor, the contractions change in character and become expulsive. The laboring woman experiences an involuntary urge to push. She uses secondary powers (bearing-down efforts) to aid in expulsion of the fetus as she contracts her diaphragm and abdominal muscles and pushes. These bearing-down efforts result in increased intraabdominal pressure that compresses the uterus on all sides and adds to the power of the expulsive forces.
The secondary powers have no effect on cervical dilation, but they are of considerable importance in the expulsion of the infant from the uterus and vagina after the cervix is fully dilated. When and how a woman pushes in the second stage of labor are much-debated topics. Continued study is needed to determine the effectiveness and appropriateness of strategies used by nurses to teach pushing techniques, the suitability and effectiveness of various pushing techniques related to abnormal fetal heart patterns, and the standards for length of pushing in terms of maternal and fetal outcomes. See Chapter 16 for further discussion regarding pushing during the second stage of labor.
Position of the laboring woman
Position affects the woman’s anatomic and physiologic adaptations to labor. Frequent changes in position reduce fatigue, increase comfort, and improve circulation. Therefore, a laboring woman should be encouraged to find positions that are most comfortable to her.
Positioning for second-stage labor may be determined by the woman’s preference, but choices are limited by her condition or that of the fetus, the environment, and the health care provider’s confidence in assisting in a birth in a specific position. See Chapter 16 for further discussion of positioning during labor and birth.
Process of labor
The term labor refers to the process of moving the fetus, placenta, and membranes out of the uterus and through the birth canal. Various changes take place in the woman’s reproductive system in the days and weeks before labor begins. Labor itself can be discussed in terms of the mechanisms involved in the process and the stages through which the woman moves.
Signs preceding labor
In first-time pregnancies, the uterus sinks downward and forward about 2 weeks before term, when the presenting part of the fetus (usually the fetal head) descends into the true pelvis. This settling is called lightening, or dropping, and usually happens gradually. After lightening, women feel less pressure below the ribcage and breathe more easily, but usually more bladder pressure results from this shift. Consequently, a return of urinary frequency occurs. In a multiparous woman, lightening may not take place until after uterine contractions are established and true labor is in progress.
The woman may complain of persistent low backache and sacroiliac distress as a result of relaxation of the pelvic joints. She may identify strong, frequent, but irregular uterine (Braxton Hicks) contractions.
The vaginal mucus becomes more profuse in response to the extreme congestion of the vaginal mucous membranes. Brownish or blood-tinged cervical mucus may be passed (bloody show). The cervix becomes soft (ripens) and partially effaced and may begin to dilate. The membranes may rupture spontaneously.
Other phenomena are common in the days preceding labor: (1) weight loss of 0.5 to 1.5 kg (approximately 1 to 3.5 lb) caused by water loss resulting from electrolyte shifts that in turn are produced by changes in estrogen and progesterone levels; and (2) a surge of energy. The woman may have a burst of energy that allows her to do whatever activities she feels will help her to prepare for labor. Less commonly, some women have diarrhea, nausea, vomiting, and indigestion. Box 13.1 lists signs that may precede labor.
Onset of labor
The onset of true labor cannot be ascribed to a single cause. Many factors, including changes in the maternal uterus, cervix, and pituitary gland, are involved. Hormones produced by the normal fetal hypothalamus, pituitary gland, and adrenal cortex probably contribute to the onset of labor. Progressive uterine distention and increasing intrauterine pressure seem to be associated with increasing myometrial irritability. This is a result of increased concentrations of estrogen, oxytocin, and prostaglandins and decreasing progesterone levels. The mutually coordinated effects of these factors result in the occurrence of strong, regular, rhythmic uterine contractions (Blackburn, 2018). The outcomes of these factors working together are normally the birth of the fetus and the expulsion of the placenta.
Stages of labor
The course of labor at or near term gestation in a woman without complications and a fetus in vertex presentation consists of: (1) regular progression of uterine contractions, (2) progressive effacement and dilation of the cervix, and (3) progressive descent of the presenting part. Four stages of labor are recognized. (These stages are discussed in greater detail, along with nursing care for the laboring woman and family, in Chapter 16.)
The first stage of labor is considered to last from the onset of regular uterine contractions to full dilation of the cervix. Commonly, the onset of labor is difficult to establish because the woman may be admitted to the labor unit just before birth and the beginning of labor may be only an estimate. The first stage is much longer than the second and third combined. However, great variability is the rule, depending on the factors discussed previously in this chapter. The first stage of labor is divided into two phases: a latent (early) phase and an active phase (Simpson & O’Brien-Abel, 2021). During the latent phase, there is more progress in effacement of the cervix and little increase in descent. During the active phase, there is more rapid dilation of the cervix and increased rate of descent of the presenting part (see the Next-Generation NCLEX® Examination-Style Case Study).
The second stage of labor lasts from the time the cervix is fully dilated to the birth of the infant. It is composed of two phases: the latent (passive fetal descent) phase and the active pushing phase. During the latent phase, the fetus continues to descend passively through the birth canal and rotate to an anterior position as a result of ongoing uterine contractions. The urge to bear down during this phase is not strong, and some women do not experience it at all. During the active pushing phase, the woman has strong urges to bear down as the presenting part of the fetus descends and presses on the stretch receptors of the pelvic floor.
The third stage of labor lasts from the birth of the infant until the placenta is delivered. The placenta normally separates from the uterine wall with the third or fourth strong uterine contraction after the infant has been born. After it has separated, the placenta can be expelled with the next uterine contraction.
The fourth stage of labor begins with the delivery of the placenta and lasts until the woman’s condition is considered stable in the immediate postpartum period, usually within 1 hour after giving birth (Simpson & O’Brien-Abel, 2021). During this stage, the woman begins to recover physically from birth, so it is an important time to observe for complications, such as abnormal bleeding (see Chapter 21).
Mechanism of labor
As already discussed, the female pelvis has varied contours and diameters at different levels, and the presenting part of the passenger is large in proportion to the passage. Therefore, for vaginal birth to occur, the fetus must adapt to the birth canal during the descent. The turns and other adjustments necessary in the human birth process are termed the mechanism of labor (Fig. 13.12). The seven cardinal movements of the mechanism of labor that occur in a vertex presentation are engagement, descent, flexion, internal rotation, extension, external rotation (restitution), and birth by expulsion. Although these movements are discussed separately, in actuality, a combination of movements occurs simultaneously. For example, engagement involves both descent and flexion.

A silhouette of a pregnant female with different positions of the fetus during labour. Part A shows the head of the fetus in the pelvic inlet along with the second image showing the pelvic bone and the relation of the posterior fontanel of the fetus with the pubic symphysis. Part B shows the chin of the fetus closer to the chest and the second image of the pelvis shows the posterior fontanel away from the lateral surface of the pelvis. Part C shows the rotation of the head at the pelvic floor and the second image posterior fontanel parallel to the pubic symphysis. Part D shows the extension of the neck of the fetus causing its appearance outside the pelvic floor and the second image shows the head outside the pelvic bone. Part E shows the rotation of the head after appears outside the pelvic floor and the second image shows the rotation of the head leading to the posterior fontanel away from the pubic symphysis. Part F shows the rotation of the shoulders along with the rotation of the head and the second image shows the posterior fontanel further away from the pubic symphysis.
Engagement
When the biparietal diameter of the head passes the pelvic inlet, the head is said to be engaged in the pelvic inlet (see Fig. 13.12A). In most nulliparous pregnancies, this occurs before the onset of active labor because the firmer abdominal muscles direct the presenting part into the pelvis. In multiparous pregnancies in which the abdominal musculature is more relaxed, the head often remains freely movable above the pelvic brim until labor is established.
Asynclitism
The head usually engages in the pelvis in a synclitic position (i.e., one that is parallel to the anteroposterior plane of the pelvis). Frequently, asynclitism occurs (the head is deflected anteriorly or posteriorly in the pelvis), which can facilitate descent because the head is being positioned to accommodate to the pelvic cavity (Fig. 13.13). Extreme asynclitism can cause cephalopelvic disproportion, even in a normal-size pelvis, because the head is positioned so it cannot descend through the maternal pelvis (see Chapter 17).

A silhouette of a pregnant female with different positions of the head of the fetus. Part A shows the head is deflected in the anterior direction. Part B shows the head of the fetus that is parallel to the anteroposterior plane of the pelvis. Part C shows the head is deflected in the posterior direction in relation to the pelvis.
Descent
Descent refers to the progress of the presenting part through the pelvis. It depends on at least four forces: (1) pressure exerted by the amniotic fluid, (2) direct pressure exerted by the contracting fundus on the fetus, (3) force of the contraction of the maternal diaphragm and abdominal muscles in the second stage of labor, and (4) extension and straightening of the fetal body. The effects of these forces are modified by the size and shape of the maternal pelvic planes and the size of the fetal head and its capacity to mold.
The degree of descent is measured by the station of the presenting part (see Fig. 13.6). As mentioned, little descent occurs during the latent phase of the first stage of labor. Descent accelerates in the active phase when the cervix has dilated to 6 cm. It is especially apparent when the membranes have ruptured.
During first-time labor and birth, descent is usually slow but steady; in subsequent pregnancies, descent may be rapid. Progress in descent of the presenting part is assessed by abdominal palpation and vaginal examination until the presenting part can be seen at the introitus (see Chapter 16).
Flexion
As soon as the descending head meets resistance from the cervix, pelvic wall, or pelvic floor, it normally flexes so the chin is brought into closer contact with the fetal chest (see Fig. 13.12B). Flexion permits the smaller suboccipitobregmatic diameter (9.5 cm) rather than the larger diameters to present to the outlet.
Internal rotation
The maternal pelvic inlet is widest in the transverse diameter; therefore, the fetal head passes the inlet into the true pelvis in the occipitotransverse position. The outlet is widest in the anteroposterior diameter; for the fetus to exit, the head must rotate. Internal rotation begins at the level of the ischial spines but is not completed until the presenting part reaches the lower pelvis. As the occiput rotates anteriorly, the face rotates posteriorly. With each contraction the fetal head is guided by the bony pelvis and the muscles of the pelvic floor. Eventually, the occiput will be in the midline beneath the pubic arch. The head is almost always rotated by the time it reaches the pelvic floor (see Fig. 13.12C). Both the levator ani muscles and the bony pelvis are important for achieving anterior rotation. A previous birth injury or regional anesthesia may compromise the function of the levator sling.
Extension
When the fetal head reaches the perineum for birth, it is deflected anteriorly by the perineum. The occiput passes under the lower border of the symphysis pubis first, and then the head emerges by extension: first the occiput, then the face, and finally the chin (see Fig. 13.12D).
Restitution and external rotation
After the head is born, it rotates briefly to the position it occupied when it was engaged in the inlet. This movement is referred to as restitution (see Fig. 13.12E). The 45-degree turn realigns the infant’s head with the back and shoulders. The head can then be seen to rotate further. This external rotation occurs as the shoulders engage and descend in maneuvers similar to those of the head (see Fig. 13.12F). As noted, the anterior shoulder descends first. When it reaches the outlet, it rotates to the midline and is delivered from under the pubic arch. The posterior shoulder is guided over the perineum until it is free of the vaginal introitus.
Expulsion
After birth of the shoulders, the head and shoulders are lifted up toward the mother’s pubic bone, and the trunk of the baby is born by flexing it laterally in the direction of the symphysis pubis. When the baby has emerged completely, birth is complete, and the second stage of labor ends.
Physiologic adaptation to labor
In addition to the maternal and fetal anatomic adaptations that occur during birth, physiologic adaptations must occur. Accurate assessment of the laboring woman and fetus requires knowledge of these expected adaptations.
Fetal adaptation
Several important physiologic adaptations occur in the fetus. These changes occur in fetal heart rate (FHR), fetal circulation, respiratory movements, and other behaviors.
Fetal heart rate
FHR monitoring provides reliable and predictive information about the condition of the fetus related to oxygenation. The average FHR at term is 140 beats/min; the normal range is 110 to 160 beats/min. Earlier in gestation the FHR is higher, with an average of approximately 160 beats/min at 20 weeks of gestation. The rate decreases progressively as the maturing fetus reaches term. However, temporary accelerations and slight early decelerations of the FHR can be expected in response to spontaneous fetal movement, vaginal examination, fundal pressure, uterine contractions, abdominal palpation, and fetal head compression. Stresses to the uterofetoplacental unit result in characteristic FHR patterns (see Chapter 15 for further discussion).
Fetal circulation
Fetal circulation can be affected by many factors, including maternal position, uterine contractions, blood pressure, and umbilical cord blood flow. Uterine contractions during labor tend to decrease circulation through the spiral arterioles and subsequent perfusion through the intervillous space. Most healthy fetuses are well able to compensate for this stress and exposure to increased pressure while moving passively through the birth canal during labor. Usually, the umbilical cord moves freely in the amniotic fluid. However, it can be compressed during uterine contractions (Blackburn, 2018; Miller, Miller, & Cypher, 2022).
Fetal respiration
Certain changes stimulate chemoreceptors in the aorta and carotid bodies to prepare the fetus for initiating respirations immediately after birth (Blackburn, 2018; Fraser, 2021). These changes include the following:
- • Fetal lung fluid is cleared from the air passages as the infant passes through the birth canal during labor and (vaginal) birth. The process of labor itself also contributes to the absorption of some of the lung fluid before birth.
- • Fetal oxygen concentration decreases.
- • Arterial carbon dioxide pressure concentration increases.
- • Arterial pH decreases.
- • Bicarbonate level decreases.
- • Fetal respiratory movements decrease during labor.
Maternal adaptation
As the woman progresses through the stages of labor, various body system adaptations cause her to exhibit both objective signs and subjective symptoms (Box 13.2).
Cardiovascular changes
During the first stage of labor, maternal cardiac output increases by 12% to 31%, primarily because of an increase in stroke volume as an average of 300 to 500 mL of blood is shunted from the uterus into the maternal vascular system with contractions. An even greater increase in cardiac output occurs during the second stage of labor. Cardiac output peaks within 10 to 15 minutes after birth and returns to its pre-labor baseline within the first postpartum hour (Mastrobattista & Monga, 2019).
Changes in blood pressure also occur. In general, both systolic and diastolic pressures increase during contractions and return to baseline levels between contractions. Systolic values increase more than diastolic values (Blackburn, 2018).
Supine hypotension (see Fig. 16.5) occurs when the ascending vena cava and descending aorta are compressed. The laboring woman is at greater risk for supine hypotension if the uterus is particularly large because of a larger than usual fetus, multifetal pregnancy, or polyhydramnios or if she is obese, dehydrated, or hypovolemic. In addition, some medications can cause hypotension.
 SAFETY ALERT
SAFETY ALERT
The woman should be discouraged from using the Valsalva maneuver (holding one’s breath and tightening abdominal muscles) for pushing during the second stage. This activity increases intrathoracic pressure, reduces venous return, and increases venous pressure. Cardiac output and blood pressure increase, and the pulse slows temporarily. During the Valsalva maneuver, fetal hypoxia may occur. The process is reversed when the woman takes a breath.
The white blood cell (WBC) count increases during labor (Blackburn, 2018). Although the mechanism leading to this increase in WBCs is unknown, it may be secondary to physical or emotional stress or to tissue trauma. Labor is strenuous, and physical exercise alone can increase the WBC count.
Some peripheral vascular changes occur, perhaps in response to cervical dilation or compression of maternal vessels by the fetus passing through the birth canal. Flushed cheeks, hot or cold feet, and eversion of hemorrhoids may result.
Respiratory changes
Increased physical activity with greater oxygen consumption is reflected in an increase in the respiratory rate. Hyperventilation may cause respiratory alkalosis (an increase in pH), hypoxia, and hypocapnia (decrease in carbon dioxide). In the unmedicated woman in the second stage of labor, oxygen consumption almost doubles. Anxiety also increases oxygen consumption.
Renal changes
During labor, spontaneous voiding may be difficult for various reasons such as tissue edema caused by pressure from the presenting part, discomfort, analgesia, and embarrassment. Proteinuria of 1+ is a normal finding because it can occur in response to the breakdown of muscle tissue from the physical work of labor.
Integumentary changes
The integumentary system changes are evident, especially in the great distensibility (stretching) in the area of the vaginal introitus. The degree of distensibility varies with the individual. Despite this ability to stretch, even in the absence of episiotomy or lacerations, minute tears in the skin around the vaginal introitus do occur.
Musculoskeletal changes
The musculoskeletal system is stressed during labor. Diaphoresis, fatigue, proteinuria (1+), and possibly an increased temperature accompany the marked increase in muscle activity. Backache and joint aches (unrelated to fetal position) occur as a result of increased joint laxity at term. The labor process itself and the woman’s pointing her toes can cause leg cramps.
Neurologic changes
Sensorial changes occur as the woman moves through the phases of the first stage of labor and from one stage to the next. Initially, she may be euphoric. Euphoria gives way to increased seriousness, then to amnesia between contractions during the second stage, and finally to elation or fatigue after giving birth. Endogenous endorphins (morphine-like chemicals produced naturally by the body) raise the pain threshold and produce sedation. In addition, physiologic anesthesia of perineal tissues caused by pressure of the presenting part decreases the perception of pain.
Gastrointestinal changes
During labor, gastrointestinal motility and absorption of solid foods are decreased, and stomach-emptying time is slowed. Nausea and vomiting of undigested food eaten after the onset of labor are common. Nausea and belching also occur as a reflex response to full cervical dilation. The woman may state that diarrhea accompanied the onset of labor, or the nurse may palpate the presence of hard or impacted stool in the rectum.
Endocrine changes
The role played by the endocrine system in the initiation of labor is not completely understood. However, changes in maternal hormone levels are involved in the process. The onset of labor may be triggered by decreasing levels of progesterone and increasing levels of estrogen, prostaglandins, and oxytocin (Simpson & O’Brien-Abel, 2021). Metabolism increases, and blood glucose levels may decrease with the work of labor.
References
Blackburn S.T. Maternal, fetal, and neonatal physiology: A clinical perspective 5th ed. 2018; Elsevier St. Louis.
Cunningham F, Leveno K, Bloom S., et al. Williams obstetrics 25th ed. 2018; McGraw-Hill Education New York.
Fraser D. Newborn adaptation to extrauterine life K.R, Simpson P, Creehan N. & O’Brien-Abel et al. AWHONN’s perinatal nursing 5th ed. 2021; Wolters Kluwer Philadelphia.
Kilpatrick S, Garrison E. & Fairbrother E. Normal labor and delivery M.B, Landon H.L, Galan E.R. M. & Jauniaux et al. Gabbe’s obstetrics: Normal and problem pregnancies 8th ed. 2021; Elsevier Philadelphia.
Mastrobattista J.M. & Monga M. Maternal cardiovascular, respiratory, and renal adaptation to pregnancy R, Resnik C.J, Lockwood T.R. & Moore et al. Creasy & Resnik’s maternal-fetal medicine: Principles and practice 8th ed. 2019; Elsevier Philadelphia.
Miller L, Miller D. & Cypher R. Mosby’s pocket guide to fetal monitoring: A multidisciplinary approach 9th ed. 2022; Elsevier St. Louis.
Simpson K. & O’Brien-Abel N. Labor and birth K.R, Simpson P, Creehan N. & O’Brien-Abel et al. AWHONN’s perinatal nursing 5th ed. 2021; Wolters Kluwer Philadelphia.
Thorp J.M. & Grantz K.L. Clinical aspects of normal and abnormal labor R, Resnik C.J, Lockwood T.R. & Moore et al. Creasy & Resnik’s maternal-fetal medicine: Principles and practice 8th ed. 2019; Elsevier Philadelphia.