83: Neurological evaluation of the ICU patient
Marguerite F. Knipe, BA, DVM, DACVIM (Neurology)
Key points
- • Determining whether neurological abnormalities in the ICU patient are primary or secondary to underlying systemic disease is a frequent clinical dilemma.
- • Many critical illnesses have sequelae that can result in structural neurological lesions.
- • Prognosis for neurological recovery is based on the neurological examination, making comfort and confidence in interpretation of a neurological examination paramount for the ICU clinician.
- • Focal or asymmetrical neurological deficits are more consistent with a structural lesion than diffuse or symmetrical signs.
- • Since many advanced neurodiagnostics require general anesthesia, judicious assessment of potential diagnostic gain vs. risks of anesthesia in the critical patient is essential.
Assessment of the critical patient’s neurological status and function is often very challenging. Sometimes determining whether the patient is truly neurologically normal or abnormal is close to impossible because the neurological examination is frequently altered by medication, trauma, or the polypathology of the critically ill animal.
The mission of the critical care specialist or neurologist is to interpret despite many of these confounding factors and determine the presence and significance of neurological dysfunction in their patients.
This chapter briefly describes the mechanics of the neurological examination, since complete descriptions are best delineated in other texts,1-3 and focuses primarily on challenges and how to troubleshoot interpretation and localization in the ICU patient.
The complete neurological examination comprises the following sections:
Ideally, all aspects are evaluated in every patient; however, clinical judgement may necessitate a limited examination based on the patient’s clinical status and concerns. Fortunately, for the observant and experienced clinician, much of the neurological examination can be done with minimal manipulation of the patient.
Mentation
Mentation is categorized as one of the following:
Localization
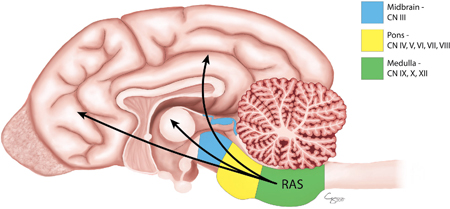
Normal mentation requires a normal cerebrum (conscious reactions/interpretation of environment, personality) and a normal brainstem (contains the reticular activating system, which projects to activate cerebrum) (Fig. 83.1). Thus, abnormal mentation implies either cerebrum or brainstem dysfunction; if there is brainstem involvement, then often cranial nerve deficits are present as well (see Cranial Nerve section). If there are no evident cranial nerve deficits, then the abnormal mentation is more likely the result of a lesion in the cerebrum or thalamus (rostral to the brainstem cranial nerve nuclei).
Level of mentation/consciousness is one of the primary assessments in the modified Glasgow Coma Scale (MGCS),4 which is an objective score (3–18) shown to correlate with survival in veterinary patients with head trauma (Box 83.1).5,6
Troubleshooting mentation abnormalities
Abnormal mentation is probably the most frequent clinical complaint in ICU patients. Level of arousal and the ability to interact appropriately with surroundings are almost always altered in patients experiencing pain, receiving medications for pain management, or in patients with severe metabolic derangements. Any medication can affect individual patients adversely, although there are some more likely than others (for example, anticonvulsants, opioids, benzodiazepines). Mentation is one of the easiest aspects for clinicians to appreciate improvement or decline; however, determining whether abnormalities result from primary brain disease or secondary to metabolic derangements or pharmacological intervention is very challenging. A common dilemma is determining whether a patient is sick enough to have the observed degree of altered mentation or if primary brain disease is a likely component.
The MGCS can be used as a monitoring tool; however, the correlation with survival has only been shown in patients with traumatic injury (see also Chapter 128).5,6 The principles of neurological improvement or decline in the MGCS are similar for any patient with brain disease, but caution should be used if trying to directly correlate outcome in patients with nontraumatic brain disease. Management and evaluation of the ICU patient with abnormal mentation should include:
Gait and posture
Evaluation of gait and posture should include the following:
- • Ambulatory or nonambulatory: Must be able to take at least a few unassisted steps with all limbs to be considered ambulatory
- • If nonambulatory, is voluntary movement present or absent (plegia)?
- • Limbs: Which limbs are affected? All four limbs? Just pelvic limbs? Limbs on one side (hemiparesis/plegia)
- • Circling (direction): Even if nonambulatory, some patients may turn their head and body as if they would circle (Fig. 83.2B).
- • Posture (position of the head and body): head tilt (Fig. 83.2A), head turn (Fig. 83.2B), torticollis, and opisthotonus (Fig. 83.3)

Localization
- • Head tilt: vestibular disease (see Box 83.2 and Fig. 83.2A)
- • Head turn: most consistent with cerebral/thalamic or forebrain lesion, ipsilateral (Fig. 83.2B)
- • Circling: seen with cerebral disease (towards the side of the lesion; see Box 83.3) or vestibular disease (either towards or away from the lesion; see Box 83.2)
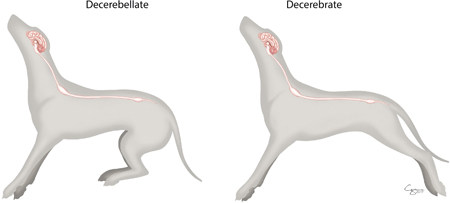
- • Decerebrate posture (Fig. 83.3 and
 Video 83.1): severe midbrain lesion, poor to grave prognosis
Video 83.1): severe midbrain lesion, poor to grave prognosis - • Decerebellate posture (Fig. 83.3 and Video 83.1): cerebellar lesion
- • Shiff–Sherrington posture (Video 83.1): T3–L7 lesion
Troubleshooting gait
Determining whether or not the thoracic limbs or just the pelvic limbs are affected creates a delineation in localization:
Paresis vs. Weakness
Weakness, or loss of strength, implies pathology involving the motor unit in the lower motor neuron (LMN) cell body in the spinal cord, peripheral nerve axon and/or myelin, neuromuscular junction, or muscle, while paresis describes decreased voluntary movement, from either the upper motor neuron (UMN) or LMN lesion.
Depending on the disease process, or if a traumatic injury is likely, it may not be practical or safe for the clinician to attempt extensive gait analysis.
Can’t walk vs. Won’t walk
Determining a patient’s ability to ambulate, or certainly the presence or absence of voluntary movement, is one of the more telling findings of a neurological exam. Many factors may make patients unwilling to walk or move: pain, fear/behavior, or severe illness/malaise. Several tricks can be used to evaluate for voluntary movement or ambulation, but most importantly, assume that your patient can and will run away from you and ensure there is some form of restraint (leash) or other means of controlling egress (enclosed room).
- • Supported walking: Lift and support patient by hand or with a sling device and encourage walking. This works well for most animals; however, in nervous, fearful, or compliant animals, the proximity and handling by a human may cause them to freeze and not move, and escape motivation or abandonment motivation (below) might be more effective. Supported walking to assess movement is very effective in patients with weakness and neuromuscular disease when voluntary movement is often very good, but their strength to support their full body weight is limited.
- • Owner motivation: Have the owner distant from the animal and call to them. May help to support the patient, if appropriate.
- • Escape motivation: Provide an escape route (open room door, open cage to return to) to motivate ambulation trying to get away from the examiner.
- • Abandonment motivation: Walk away from the patient or exit the room to motivate the animal to follow.
Cranial nerves
See Box 83.4 and Video 83.2.
- Menace response: response because it involves recognition and processing in the cerebral cortex vs. reflexes that do not.
- Pupillary light reflexes (PLRs): midbrain
- Trigeminofacial reflexes: (palpebral, vibrissae, lip pinch): pons
- Corneal reflex: pons
- Physiologic nystagmus: pons, midbrain
- Gag reflex: medulla
Localization
Cranial nerve deficits usually support an ipsilateral lesion in the brainstem or the peripheral cranial nerve. The menace response is frequently affected by lesions elsewhere in the brain (cerebral dysfunction, see Box 83.3) and requires evaluation of other cranial nerve tests to determine whether the afferent or efferent nerve are involved.
Troubleshooting cranial nerves
Other than the menace response and reaction to nasal stimulation, most of the tests of cranial nerves are reflexes and require no cerebral or conscious execution, so the loss of a reflex is abnormal and usually indicative of a lesion, particularly if asymmetrical (Fig. 83.1).
- • Animals with heavy sedation or recovering from anesthesia may not have CN reflexes. As a result, similar to the rest of the neuro examination, cranial nerve function is most reliably assessed in patients when they are the least affected by medications.
- • Animals without an eye or with ocular trauma are challenging because many CN reflexes involve the eyes (PLRs, physiologic nystagmus, among others), so look for other reflexes to assess brainstem function.
- • Systemic anticholinergic medications such as atropine or glycopyrrolate can alter resting pupil size (mydriatic) and amount of constriction when assessing PLRs. Similarly, other drugs often result in miotic pupils (benzodiazepines). See Chapter 85 for more on pupillary assessment in the patient with increased intracranial pressure.
Proprioceptive positioning
Assessment of proprioceptive placing can include the following:
Localization
Normal placing reactions require intact peripheral nerves and the spinal cord, brainstem, and cerebrum, so they are probably the least specific tests for neurological disease since they are frequently abnormal in patients with any kind of neurological dysfunction. Clinicians must use the rest of the neurological examination to help localize a lesion.
Troubleshooting proprioceptive placing
Because these evaluations involve more manipulation of the patient, they are often not assessed in patients with concerns for spinal trauma.
Placing reactions are often more interesting if the placing is normal in the patient being evaluated. Because the pathways involve so many aspects of both the peripheral and central nervous system, if placing reactions are normal, the clinician should seriously consider a nonneurologic cause for the patient’s problem.
False normals: struggling patients, feeling off-balance and constantly shifting weight and moving.
Potential false absents
- • Sedation/anticonvulsants/pain medications/severe metabolic derangement. These are conscious, voluntary reactions, so any pharmacological or physiological impairment of mentation or awareness may result in abnormal or absent reactions, usually symmetrical.
- • Limb trauma/fracture/luxation: Again, these are voluntary placing reactions, so if a limb is severely injured and painful, the animal may not want to move it to an appropriate position. *This is very challenging, since neurological function of a limb in a trauma patient plays an important role in prognosis and decisions for any possible surgical intervention. A limb with both a humeral fracture and a brachial plexus avulsion has a poor prognosis for return to function and is not a good candidate for fracture repair. In these cases, careful evaluation of limb reflexes and sensation/nociception is essential.
Segmental reflexes
Localization
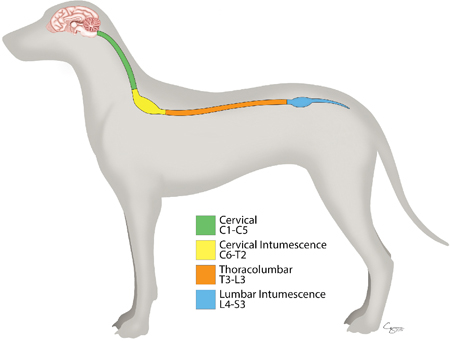
Evaluation of segmental reflexes is essential to localizing spinal cord lesions (Fig. 83.4) and determining whether the UMN system is affected (UMN signs) or the LMNs are affected (LMN signs) (Box 83.5). The UMN system originates in the cerebrum and brainstem and synapses on the LMNs in the brainstem (cranial nerves) and spinal cord to effect voluntary movement (Box 83.6).
UMNs and LMNs are required for normal voluntary movement, so a lesion in either system can affect the ability to move the limb resulting in paresis or paralysis and/or ability to replace the limb.
Troubleshooting segmental reflexes
Trauma
If the humerus or femur is fractured, then the lever arm for the reflex mechanism is lost, so even if all neural structures are intact, the reflex may not be present. Similarly, the voluntary movement of a limb may also be affected, certainly the ability to bear weight with a proximal limb fracture. This is particularly challenging to evaluate in the polytrauma patient, where whether a limb has neurological function often determines whether to repair a fracture. Utilize cutaneous testing and sensation to determine the presence and extent of any possible neurological lesion.
Spinal shock
Spinal shock is the transient loss of muscle tone and segmental reflexes caudal to an acute spinal cord injury. This is appreciated on clinical examination by noting LMN signs (decreased/absent reflexes) in a patient with an otherwise UMN spinal cord localization.7,8 Spinal shock results from physiologic dysfunction of the LMN versus a true structural injury to the LMNs. Various theories for transient disruption of spinal cord synaptic and interneuronal conduction are proposed, but excessive inhibitory neurotransmitters secondary to the injury have a prominent role in the pathophysiology.8,9 Awareness of spinal shock phenomenon is essential for accurate neuroanatomical localization and understanding that the loss of reflexes may not reflect a multifocal disease process.
- • Clinically, loss of the flexion/withdrawal reflex seems most common,7,8 but loss of tendon reflexes is also possible.
- • Rate of recovery of reflexes is variable, ranging from hours to weeks,7,8,10 but improvement is noted in most patients.
- • Recheck reflexes over time, especially if localization seems multifocal; if spinal shock, reflexes will improve with time.
Spinal shock vs. Myelomalacia
In thoracolumbar spinal cord injury, LMN signs to the pelvic limbs are highly concerning for descending myelomalacia, with a grave to poor prognosis for any return to function.11
- • Spinal shock reflex deficits are often partial (i.e., absent flexion/withdrawal but present tendon reflexes) and may be asymmetric, while loss of reflexes with myelomalacia tends to be complete in both limbs.
- • Patients with myelomalacia will not have deep pain perception (see below). This reflects the severe and irreversible pathology of myelomalacia.
- • Patients with spinal shock may also not have deep pain perception, depending on the severity of the lesion, but will have improvement of reflexes and tone to be more consistent with an UMN lesion, even if the spinal cord is functionally transected.10
Sensation/nociception
- • Superficial pain perception (nociception): noxious stimulus to interdigital skin; look for evidence of conscious reaction (whining/crying, attempting to bite or escape, looking at stimulus, may be as subtle as pupillary dilation or pausing in panting).
- • Deep pain perception (nociception): noxious stimulus applied over the digit; goal to stimulate the periosteum; look for conscious reaction.
Localization
Important for assessment of spinal cord injury, peripheral nerve injury, and brain disease (i.e., coma). Loss of pain perception, particularly deep pain, is strongly associated with a poor prognosis for recovery of function.12 Confidence in distinguishing the flexion/withdrawal reflex from a conscious reaction to a noxious stimulus is essential for accurate assessment of patient prognosis.
Troubleshooting nociceptive assessment
Potential false negatives (seems like pain sensation is absent)
- • Behavior: stoic or frozen-fearful animal
- • Because we are evaluating a conscious reaction, patients with stoic temperaments or are frozen with fear may not react as we might expect.
- • If there is no reaction in the limb(s) you are evaluating, try pinching a normal limb to gauge the animal’s level of reactivity. If there is minimal reaction in an apparently normal limb, then interpretation of pain perception may not be reliable.
- • Opioids and other pain or sedation medications
- • Animal does not flex the limb
- • Look for the conscious reaction to the stimulus, not the flexion of the limb. The action of flexing or moving the limb can be just a reflex (see Reflexes previously) and does not equate to conscious sensation. There are many reasons the animal may not move the limb, fracture and pain or mechanical inability to flex the limb, LMN disease (e.g., polyradiculoneuritis, botulism) where the motor capabilities are affected, but the sensory pathways are intact.
Potential false positives (seems like pain sensation is present when it may not be)
- • Exaggerated flexion of the limb, where the animal may react to the general movement of the body, not the noxious stimulus
- • UMN reflexes can be extremely exaggerated, with the brisk flexion movement causing the body to move. The animal may react to the movement, and that could be interpreted as a reaction to the noxious stimulus applied to the digit.
- • Eliminate the vigorous flexion movement from the equation by holding the limb in flexion before pinching.
- • Behavior: very reactive or anxious patient
Neurologically abnormal
If abnormal, localize first to the following:
Then localize better within the division (see Box 83.2, Box 83.3, Box 83.5, Box 83.6, Box 83.7), and finally lateralization, if present.
Clinical challenges in the critical patient with neurological disease
Determining brain death
There are currently no standards to determine brain death in veterinary medicine, although the critical care clinician will likely be faced with this clinical challenge. In human adults, the American Academy of Neurology lists three mandatory clinical findings necessary to indicate irreversible cessation of brain function: coma, absence of brainstem reflexes, and apnea.13 These are straightforward clinical evaluations in the veterinary ICU patient, and in the absence of anesthetic drugs and an appropriate withdrawal time from these medications indicate a poor prognosis.
Additional functional assessment of the cerebrum (electroencephalogram [EEG]) and brainstem (brainstem auditory evoked response [BAER]) may assist in the clinical decision for euthanasia. These are functional modalities utilized at our institution to confirm severe cerebrocortical and brainstem dysfunction, in addition to the clinical status of comatose, absent brainstem reflexes, and apneic.
BAER
More than just a hearing test, the BAER evaluates brainstem function and may provide additional diagnostic support for severe brainstem injury.
- • Use caution in the interpretation of no waveforms/flatline BAER. These may be secondary to deafness, middle or external ear disease, or even technical problems.
- • It is most helpful clinically if early waveforms, but not later, waveforms are noted. This indicates that peripheral portions of the auditory pathway are intact, but not the central (brainstem) portions.
Electroencephalogram
For humans, the American Clinical Neurophysiology Society states 11 guidelines for EEG recording in suspected cerebral death,14 many of which would be possible to meet in veterinary facilities with EEG capabilities, but other guidelines are specific to the larger size of the human skull (e.g., 8–20 electrodes 10 cm apart). Even in veterinary patients, documenting electrocerebral inactivity or burst-suppression patterns in the prolonged absence of anesthetic drugs supports the clinical diagnosis of brain death.
Distinguishing if neurological deficits are primary or secondary to systemic disease
Even if the deficits are primary, are they sequelae of a systemic disease (e.g., embolism or hemorrhage secondary to hypercoagulability; seizures secondary to hypoglycemia) or a new separate problem (see also Box 83.8)?
If magnetic resonance imaging (MRI) was a simple and inexpensive diagnostic test, it would be easy to screen the central nervous system (CNS) in our patients; however, in the critically ill animal, general anesthesia can put the patient at risk for more problems and may not be necessary for adequate management of the case.
Is imaging indicated?
It would be easy, of course, if advanced imaging did not require anesthesia.
What about sedated computed tomography?
- • It is fast and can be done without general anesthesia.
- • Unless you are screening for skull or vertebral column fractures or are trying to rule out a large extraparenchymal compressive lesion or mass, computed tomography (CT) will not provide the amount of detail for parenchymal disease that MRI does, and in the critically ill patient, parenchymal inflammatory or vascular lesions are very high on the list of most likely causes, and would not likely be visible on CT.
Doesn’t imaging help determine prognosis?
- • No. Prognosis should always be based on the neurological examination, regardless of findings on radiographs, CT, or MRI. Imaging can only evaluate the location and extent of the lesion and contributes more information about the most likely cause. A patient can have a T3–L3 myelopathy with absent deep pain perception and a normal appearance of the spinal cord on MRI. The prognosis is still poor.
Will imaging findings change the treatment plan?
It is important to weigh the personal curiosity desire to know against the clinical need-to-know for best patient management.
Situations where considering imaging may be worth the risk/expense include the following:
- • Patient’s systemic problems are improved, but the neurological deficits are not
- • This is a common dilemma. How long is “long enough” to wait for neurological improvement? Depending on the underlying etiology (infarct, hemorrhage, necrosis), a neurological deficit resulting from sequelae of a primary systemic disease could be permanent, even if the underlying disease improves. A patient’s hypercoagulable state may resolve, but if the patient is paraplegic secondary to thromboembolism, the myelopathy may take weeks to months to improve, if at all.
- • Keep in mind that your neurological examination is the basis for prognosis (see above). Imaging can only localize and further characterize any lesions.
- • Neurological deficits progress despite apparent adequate management of the systemic disease
- • Deterioration of neurological status warrants strong consideration to discover if there are other specific interventions possible for the patient.
- • Again, prognosis is still based on neurological examination, so a patient that has progressed from obtunded to stupor to coma has a poor prognosis, regardless of etiology.
- • Deficits are unlikely to be secondary to the primary systemic disease process
- • For example: A patient with hypoglycemia may be expected to have seizures secondary to that metabolic dysfunction; however, if that patient develops new central vestibular signs, that is a lesion unlikely to be a direct consequence of the hypoglycemia. It may still be a CNS lesion secondary to another systemic problem (perhaps the patient is hypercoagulable and prone to thromboembolic events) but unlikely to be a sequela to the original problem of hypoglycemia, so it is worth considering imaging.
- • Owners are unlikely to proceed with continued care if a second problem is found. Findings will change case management.
Next steps
Fluctuations in patients’ well-being in the ICU are closely monitored, and this includes the neurological examination. The ICU clinician’s vigilance of the patient’s neurological status and valuation of advanced neurodiagnostics guides best recommendations to both clients and other primary clinicians with critically ill patients.
Keep in mind:
- • Prognosis is based on the neurological examination
- • Appreciate that the nervous system is often secondarily affected in the ICU patient and may not need specific diagnostics/treatment, but neurological lesions will change the management of the patient (bladder management, recumbent care, ventilatory support, etc.)
- • Recognize what deficits fall into the realm of likely secondary to underlying disease and what deficits are likely separate
- • Asymmetrical signs should increase the suspicion of a structural lesion
Video 83.1 This video illustrates and explains differences between some acute postures seen in patients with neurological injury.
Video 83.2 This video demonstrates the cranial nerve exam and illustrates related anatomy for interpretation.
References
1. Dewey CW & da Costa RC. Practical guide to canine and feline neurology ed 3 2016; Wiley Ames, IA.
2. Platt S & Olby NJ. BSAVA manual of canine and feline neurology ed 4 2013; BSAVA Gloucester.
3. Lorenz MD, Coates JR & Kent M. Handbook of veterinary neurology ed 5 2011; Elsevier Saunders St Louis.
4. Shores A. Craniocerebral trauma Kirk & RW. Current veterinary therapy X 1983; WB Saunders Philadelphia 847-885.
5. Platt SR, Radaelli ST & McDonnell JJ. The prognostic value of the modified Glasgow Coma Scale in head trauma in dogs J Vet Intern Med 6, 2001;15: 581-584.
6. Sharma D & Holowaychuk MD. Retrospective evaluation of prognostic indicators in dogs with head trauma: 72 cases (January-March 2011) J Vet Emerg Crit Care 5, 2015;25: 631-639.
7. Full AM, Heller HL & Mercier M. Prevalence, clinical presentation, prognosis, and outcome of 17 dogs with spinal shock and acute thoracolumbar spinal cord disease J Vet Emerg Crit Care 3, 2016;26: 412-418.
8. Smith PM & Jeffery ND. Spinal shock – comparative aspects and clinical relevance J Vet Intern Med 2005;19: 788-793.
9. Ko HY. Revisit spinal shock: pattern of reflex evolution during spinal shock Korean J Neurotrauma 2, 2018;14: 47-54.
10. Handa Y, Naito A, Watanabe S, et al: Functional recovery of locomotive behavior in the adult spinal dog Tohoku J Exp Med 1986;148: 373-384.
11. Castel A, Olby NJ, Ru H, et al: Risk factors associated with progressive myelomalacia in dogs with complete sensorimotor loss following intervertebral disc extrusion: a retrospective case-control study BMC Vet Res 2019;15: 433.
12. Langerhuus L & Miles J. Proportion recovery and times to ambulation for non-ambulatory dogs with thoracolumbar disc extrusion treated with hemilaminectomy or conservative treatment: a systematic review and meta-analysis of case-series studies Vet J 2017;220: 7-16.
13. Wijdicks EFM, Varelas PN, Gronseth GS, et al: Evidence-based guideline update: determining brain death in adults - report of the Quality Standards Subcommittee of the American Academy of Neurology Neurology 2010;74: 1911-1918.
14. Stecker MM, Sabau D, Sullivan LR, et al: American Clinical Neurophysiology Society Guideline 6: minimum technical standards for EEG recording in suspected cerebral death Neurodiagn J 4, 2016;56: 276-284 https://doi.org/10.1080/21646821.2016.1245575.