14: Communication Strategies for Health Promotion and Disease Prevention
At the end of the chapter, the reader will be able to:
1. Define concepts related to health promotion and disease prevention.
2. Identify national agendas for health promotion and disease prevention.
3. Apply conceptual frameworks to health promotion actions.
4. Analyze evidence for health promotion and disease prevention strategies for individuals.
5. Evaluate health promotion and disease prevention strategies at the community level.
Health promotion can refer to international level policy issues or to policies within a community that raise awareness of healthy lifestyle behaviors (RHIhub, 2018). It can also be applied to individual nurse–patient interventions and communications, which will be the focus of this chapter.
An overarching goal of Healthy People 2030 is promotion of quality of life and healthy development and behaviors across all stages of life (U.S. Dept. of Health & Human Services, 2020). This chapter focuses on concepts affecting nursing roles in achieving specific health promotion and disease prevention. Underlying barriers are also explored. Underlying causes of health problems are increasingly recognized as a matter of concern. However, many nurses underutilize opportunities to provide our patients with health promotion concepts (Iriarte-Roteta et al., 2020).
Basic Concepts
Definitions
Health
is the ability to function and to experience well-being. Factors such as genetics, environment, economics, and societal conditions influence our health status, as do factors such as healthcare availability and our educational level. Health is considered by many to be a fundamental human right (United Nations, 2021).
Health promotion
is defined as the process in which a person takes control of their own health.
Well-being
is personal satisfaction in six dimensions: intellectual, physical, emotional, social, occupational, and health.
Health promotion activities are lifestyle activities that promote optimum health. Fig. 14.1 lists critical elements of health and well-being. Activities include the following:
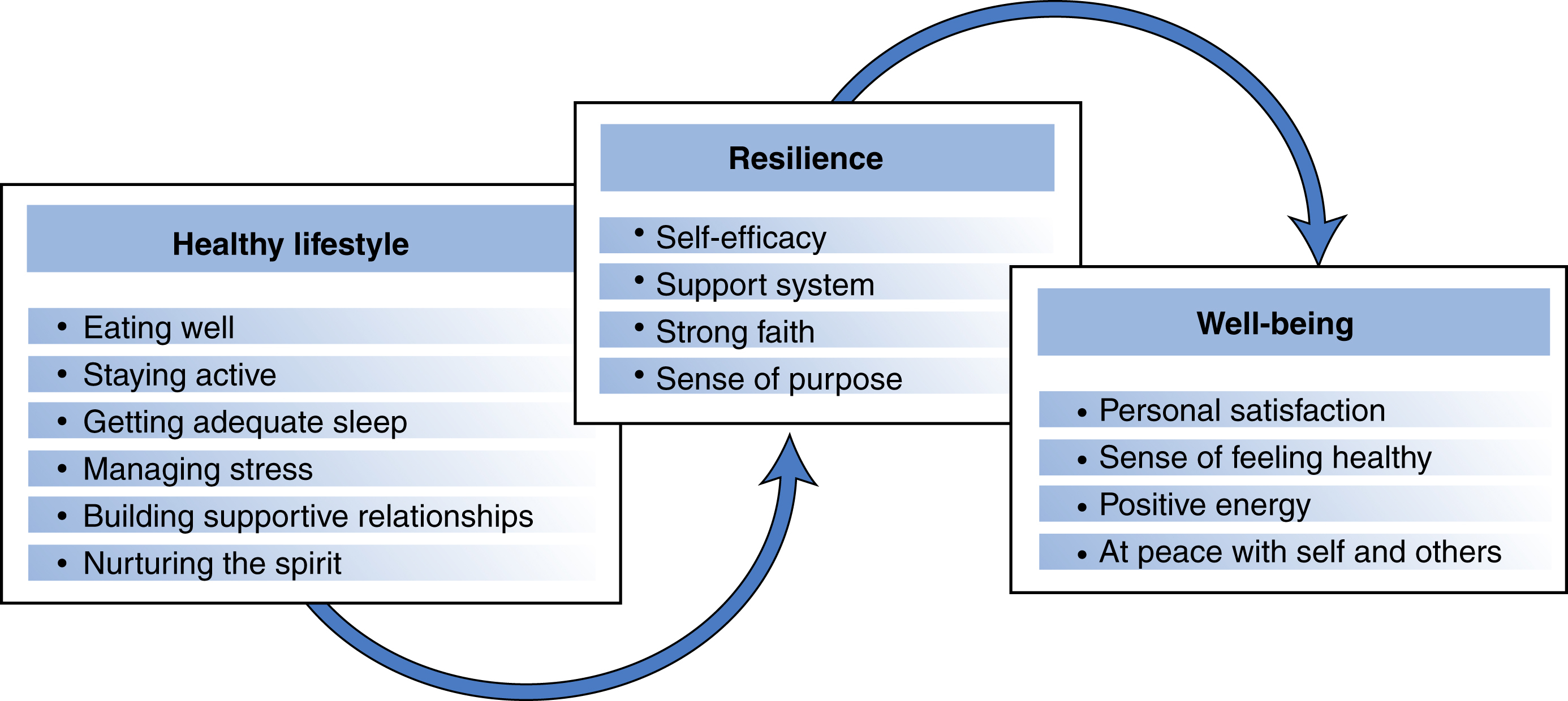
A flowchart shows Healthy lifestyle leads to resilience followed by well-being as follow:• Healthy lifestyle: Eating well, staying active, getting adequate sleep, managing stress, building supportive relationships, and nurturing the spirit.• Resilience: Self-efficacy, support system, strong faith, and sense of purpose.• Well-being: Personal satisfaction, sense of feeling healthy, positive energy, and at peace with self and others.
Case Study
Bele Chase Fears Vaccination

Mrs Chase, age 70, tells you she spent a year in lockdown during the recent pandemic and really wanted to be able to visit her grandchildren. However, she now fears flying and exposing herself to possible disease. Diane Gibb, FNP, is her longtime nurse practitioner with an established trusting relationship. She explains the efficacy of immunization and recommends the procedure, explaining dosage and possible mild side effects. Diane tells Ms Gibb that she herself has been immunized and would recommend it to her mother for her protection.
Theoretical Concepts in Health Promotion
While experts stress the need to look beyond individual patients to promote community and corporate policies, nurses primarily deal with helping patients change unhealthy behaviors. Pender’s health promotion model, Prochaska’s transtheoretical model, Bandura’s social learning theory, and the disease prevention epidemiological models are useful frameworks to guide health promotion strategies and help us understand the individual’s choices in health behavior.
Pender’s Health Promotion Model
Nurses use Nola Pender’s health promotion model to understand what motivates people to engage in specific health behaviors (Pender et al., 2011). As shown in Fig. 14.2, this focuses on three areas: characteristics and experiences of individuals; their behavior-specific cognition and affect; and behavioral outcomes. In Pender’s view, health is a dynamic process affected by personal factors, social support systems, and situational variables. The patient’s belief about the degree to which they believe their actions can affect health outcomes needs to be considered, a concept known as self-efficacy. Perceived barriers to action have an impact of the patient’s willingness to try to change their health-related behaviors.
Nurses can help patients modify unhealthy behaviors, but their capacity to change depends on what they believe about their illness, the seriousness if it, and their belief in the extent to which their own actions can produce positive outcomes. Nurses assess the degree of value patients place on their good health. Simulation Exercise 14.1 provides practice applying Pender’s model. Pender’s model identifies perceived benefits, barriers, and ability to take action related to health and well-being as important components of people’s health decision-making.
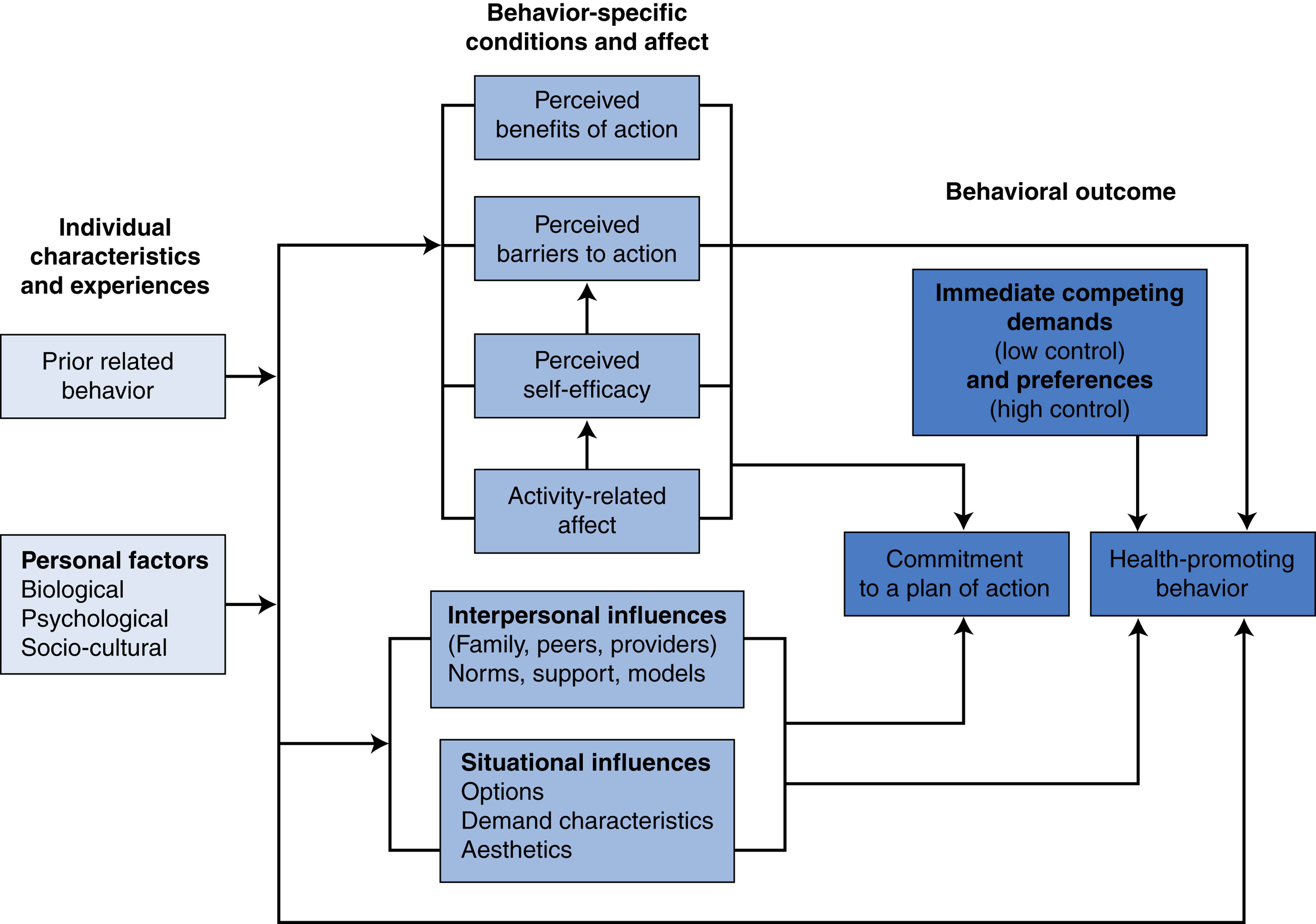
A flowchart shows Pender’s revised health promotion model as follows:• Individual characteristics and experiences: Prior related behavior and personal factors (biological, psychological, and socio-cultural).• Individual characteristics and experiences lead to behavior-specific conditions and affect.• Behavior-specific conditions and affect: Activity-related affect leads to perceived self-efficacy, perceived barriers to action, and perceived benefits of action; interpersonal influences (family, peers, providers) Norms, support, models; situational influences (options, demand characteristics, aesthetics). • Behavior-specific conditions and affect, interpersonal influences, and situational influences leads to commitment to a plan of action • Behavioral outcome: Interpersonal influences, situational influences, and immediate competing demands (low control) and preferences (high control) leads to health-promoting behavior.

Prochaska’s Transtheoretical Model for Change
This model is also called the Stages of Change Model. It is a decision-making model developed in the 1970s exploring the individual’s motivational readiness to intentionally change their behaviors and health habits (Prochaska & Norcross, 2013). Stages of readiness range from lack of acknowledgment of the problem to the taking of constructive actions to correct unhealthy behaviors. It employs cognitive and affective processes. By the last stage, the person has no desire to return to their former (unhealthy) behavior. Small changes are rewarded to reinforce the new behavior. Table 14.1 presents Prochaska’s model with suggested approaches for each stage and corresponding sample statements. Simulation Exercise 14.2 provides an opportunity to work with Prochaska’s transtheoretical model.
Bandura’s Social Learning Theory
Albert Bandura’s (1997) social learning theory proposes that humans observe and then copy a new behavior in a reciprocal interaction. According to Bandura, a person does not learn a new behavior by simply trying it out. Instead, they replicate the actions of others who serve as models. A big contribution to the study of health promotion is the concept of self-efficacy. Self-efficacy is defined as a personal belief in one’s ability to execute the actions required to achieve a goal. It represents a powerful mediator of behavior and behavioral change. Self-efficacy and motivation are reciprocal processes. Increased self-efficacy strengthens motivation, which, in turn, increases an individual’s capacity to complete the learning task.
Bandura considers learning to be a social process. He identified three sets of motivators: physical motivators,
social incentives, and cognitive motivators. Physical motivators can be internal, such as memory of previous discomfort or a symptom that the patient cannot ignore. Social incentives, such as praise and encouragement, increase self-esteem and give the patient reason to continue learning. Cognitive motivators are thought processes associated with change.
As a nurse, you might combine aspects of these theories, relating them to something your patient values to move the change process along toward achieving the desired outcome, such as in the Francis Cox case.
Disease Prevention Epidemiological Framework
There are several disease prevention frameworks concerned with risk and protective factors associated with specific diseases. Nurse can use case finding to identify risk factors in individuals, families, or communities. The goal is to prevent or delay the onset of disease or to manage progression to disability. Health promotion and disease prevention, with special attention to the underlying causes of a health problem, is increasingly recognized as a reimbursable, essential component of comprehensive healthcare. Regular health screenings can identify emerging treatable health problems such as osteoporosis, high blood pressure, or glaucoma.
- 1. Primary disease prevention—Intervention targets modifiable risk factors with suggestions for a healthier lifestyle. For example, promoting exercise and healthier diet to prevent onset of diseases such as diabetes. What other preventive advice have you heard? Were any communication strategies promoting this message any better than others? Fig. 14.3 depicts American National Prevention Strategies.
- 2. Secondary disease prevention—The focus is on early disease detection through regular screening. Early diagnosis allows implementation of treatment to hopefully prevent or modify the progression of a disease.
- 3. Tertiary disease prevention—These strategies minimize the damaging effects of a disease or injury once it occurs. The goal is to help patients achieve best quality of life possible. Simulation Exercise 14.3 provides an opportunity to develop your health profile and examine risk factors in your life.
Protective factors are defined as circumstances, resources, and personal characteristics that delay the emergence of chronic disease or lessen its impact. Although protective factors do not guarantee a life free of serious illness or early death, they play a significant role in helping patients improve their health and quality of life. Examples of protective factors include developing a healthy lifestyle, getting
daily exercise, eating a healthy diet, having annual medical checkups, increasing the number of available support systems, obtaining health insurance, and so on. Health education, social marketing, and screening services help people to become aware of health risk factors.
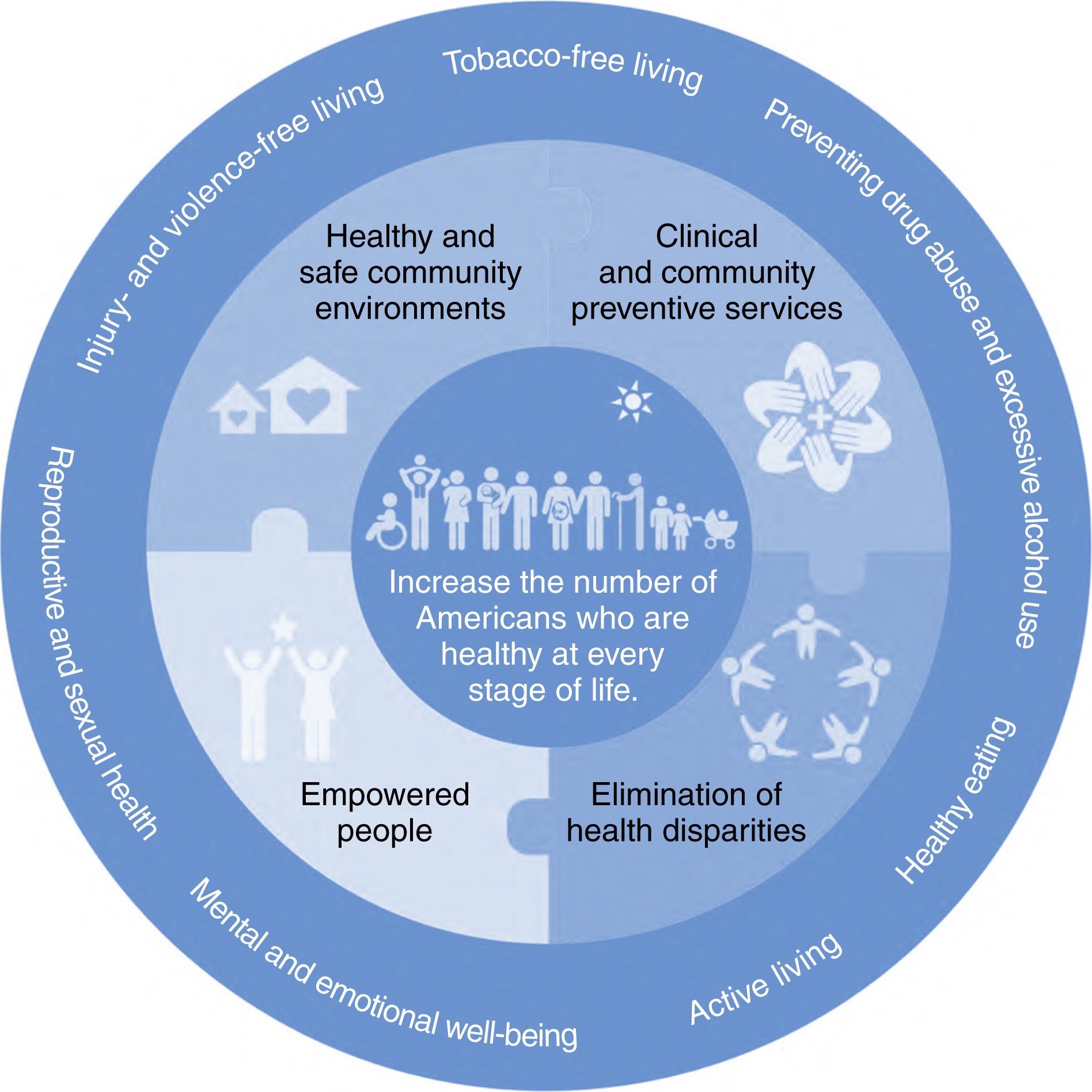
A wheel shows national prevention strategy as follows:• Outer circle is marked: Healthy eating, active living, mental and emotional well-being, reproductive and sexual health, preventing drug abuse and excessive alcohol use Injury- and violence-free living, and tobacco-free living.• Middle circle is divided into 4 parts as follows: Healthy and safe community environments, clinical and community preventive services, elimination of health disparities, and empowered people.• Core is marked: Increase the number of Americans who are healthy at every stage of life.
Global and National Health Promotion Agendas
The World Health Organization’s (WHO) global agenda is guided by a series of reports including The Ottawa Charter for Health Promotion (WHO, 1986), The Jakarta Declaration of the fourth International Conference on Health Promotion (WHO, 1997), and the Shanghai Declaration on Promoting Health in the “2030 Agenda for Sustainable Development” (WHO, 2018).
Social Determinants of Health
Societal and community systems interacting with personal factors impact health over time. Individuals incorporate norms and values from social networks often without conscious reflection. Economic factors and political policies affect the availability.
Social, economic, religious, and political factors affecting health promotion and disease prevention are embedded at the level of the community as well as the larger society. They have a significant effect on health and well-being. Although each person enters the world with a distinct set of constitutional factors (size, gender, intellect, and personality), each grows up within social and community networks and, over time, incorporates the social values of those networks. One’s environment interacts with personal factors to influence, enhance, or limit one’s health behaviors. Larger social community systems create roles and expectations that further shape and modify the individual’s health behaviors (Gray, 2017).
Health Disparities
Health disparities describes fundamental differences in adverse health outcomes and lost opportunities to achieve optimal health and well-being as it relates to demographics, income, education, and access. It is essential that nurses not just understand that health inequities exist, but also understand their causes (McFarland & MacDonald, 2019). Nationally, disparities account for significant variations in life expectancy, positive health outcomes, and the incidence of chronic disease and disability.
Causes
Social determinants associated with health disparities include lack of adequate health insurance, social isolation, cultural factors, access and availability of services, finances, lack of knowledge or education, food or job security, language barriers, health literacy, and poverty. Social determinants critically affect health, morbidity, and mortality. The elimination of health disparities is a primary objective of our nation’s public health agenda and a central focus of the National Center for Minority Health and Health Disparities within the National Institutes of Health.
Nurse Role
Except for our function educating patients, we nurses seem to have a lack of clarity about what constitutes our responsibility in social policies that underpin health disparities. Broadly our mission could include action to
Topic areas proposed to achieve these goals identify the population focus of attention. Objectives are organized in three categories—interventions, determinants, and outcomes. Healthy People 2030 reinforces the importance of social determinants as critical antecedents that influence health and well-being.
Disease Prevention
Disease prevention frameworks are concerned with identifying modifiable risk and protective factors associated with specific diseases and mental disorders. Nurses can use strategies in health counseling such as those suggested in Box 14.1. The goals of prevention emphasize managing and/or
preventing the risk of future disease, disability, and premature death. Three tiers of prevention—primary, secondary, and tertiary—offer a continuum of disease prevention focus.
Applications
Providing Health Education for Health Promotion
Health promotion strategies should be a part of everyday nursing care. Education and coaching can be introduced informally as you provide care. To succeed, nurses must become aware of the individual needs of each patient, take time to develop a personalized teaching plan, and access materials to supplement their teaching. Some suggest that this should be a priority (Bennett et al., 2020; Pueyo-Garrigues et al., 2019). Communication for patient education is discussed in Chapter 15.
Community-based interventions can be formally presented through patient education, screening programs, and social media. Choosing topics of interest to high-risk populations might include screening for disease common among certain population groups. Nurses can be influential in helping communities to create supportive health environments. For example, nurses can serve on health-related community advisory committees and provide relevant
discussions regarding care and funding. The provision of health fairs for area schools or community groups is another avenue nurses can use to support health promotion and disease prevention at the community level.
Common examples of general health promotion include developing a healthy lifestyle, good nutrition, regular physical activity, adequate sleep patterns, and stress reduction. But in addition to these desired outcomes, engaging in meaningful health promotion activities supports the development of patient autonomy, personal competence, and social relatedness.
Formal and informal instruction can focus on condition-specific topics. A wide variety of topics lend themselves to a health promotion focus. A sampling includes the following:
- • Alcohol, nicotine, and other types of drug abuse prevention, including the DARE anti–drug use program presented in elementary schools
- • Prevention, screening, and early detection of common chronic diseases such as human immunodeficiency virus (HIV), diabetes, cancer, heart disease, osteoporosis, and associated disorders
- • The fall prevention strategies, especially for older adults
- • Stress reduction for informal caregivers and organizational work sites
- • Healthy dietary practices
- • Regular exercise habits
- • Developing effective support systems
Motivational Interviewing
MI is “theoretically congruent” with the transtheoretical model of behavior change. A motivational intervention encompasses a patient’s values, beliefs, and preferences incorporated into relevant functional abilities and learned skills. Motivation is seen as a state of readiness rather than a personality trait. An overarching goal of individuals who need to improve their health is to develop a better health-related quality of life. To achieve this goal, people must want to change behaviors that compromise their health.
Treatment for many chronic diseases such as cancer, heart disease, asthma, diabetes, and arthritis often requires significant ongoing lifestyle changes. Patients are charged with taking a much more active role in designing and implementing the sometimes significant lifestyle changes that are required to live a purpose-filled life while coping with chronic illness. MI is a useful strategy in dealing with ambivalent patients who must make significant lifestyle changes.
The person must believe that success is “achievable” with his/her personal efforts and/or resources. The decision to change, the choice of goals, and the commitment to developing new behaviors is always under the patient’s control.
Readiness to change can be influenced. Nurses can better understand and influence a patient’s deeper perception of a problem through Socratic questioning. This type of questioning allows nurses to point to discrepancies between a patient’s goals or values and his or her current behaviors without argument or direct confrontation. MI helps patients address resistance and ambivalence about making health-related lifestyle changes in a nonjudgmental environment. Therapeutic strategies center on resolving problem behaviors, increasing committed collaboration, and joint decision-making.
MI is an intervention in which the nurse uses empathetic exploration to help a patient become aware of discrepancies in their behavior that are hurting their health and well-being. This exploration is coupled with teaching them new skills to achieve more healthy life goals.
Negotiating behavior change is conceptualized as a shared endeavor in which both patient and provider examine the patient’s potential and willingness to change destructive health behaviors. When motivational strategies match an individual’s readiness to change, this match increases the likelihood of positive intentional behavioral lifestyle changes.
There are two phases of MI. The first phase focuses on mutually exploring and resolving ambivalence to change as a collaborative endeavor. This is accomplished through weighing the pros and cons of the current situations and the actions one would have to take to make change possible. With the patient in charge of determining change activities, the second phase emphasizes strengthening and supporting the patient’s commitment to change based on the patient’s choice and capacity for change.
A good starting point is a simple introductory question, such as, “I wonder if you could tell me what you do to keep yourself healthy?” This type of question helps you to see what the patient values or even if he or she thinks about taking a personal role in achieving and maintaining healthy
behaviors. It also provides an opportunity to assess for possible issues that actually may be counterproductive, as in the Janet Chico case.
When a patient begins to tell you about his or her personal health habits, you can reflect on the relevant details and ask for clarification. The purpose of the dialog is to deepen the patient’s understanding. Use empathy in your responses. For example, “It sounds like you have been having a tough time and not getting a lot of support.”
Open-ended questions allow patients the greatest freedom to respond. Asking a patient if he regularly exercises may yield a one-sentence answer. Inviting the same patient to describe his activity and exercise during a typical day and what makes it easier or harder for him to exercise can provide stronger data. Potential concerns and inconsistency with values, preferences, or goals are more readily identified.
Patient and family perspectives on disease and treatment are not necessarily the same as those of their healthcare providers. For example, you may think that an emaciated or an obese woman would be worried about her weight and would want to modify it because she values the way she looks. On the other hand, her culture or family values and traditions may be in conflict with making significant behavioral changes. Until the patient can understand a health-related value for making a change, she will not put serious effort into doing so. This level of data allows nurses to tailor interventions based on the patient’s readiness to change and the availability of a support system.
As patients progress to the contemplative stage, nurses provide coaching guidance, information, and practical support to help them consider different choices and potential solutions. The pros and cons of each possible choice are explored. Empathy for the challenges faced by the patient and affirming the patient’s reflection process encourages patients to consider alternative options and to choose the most viable among them. A critical component of MI is acceptance of the patient’s right to make the final decision and the need for the clinician to honor the patient’s right to do so.
In the preparation stage, your role is to help patients establish realistic goals and develop a plan for achieving them. Goals should be realistic, patient-centered, and achievable. For example, the goal of losing 10 pounds in 3 months sounds more doable than a goal to simply losing weight (too vague) or losing 75 pounds (potentially overwhelming). Incremental goals build a sense of confidence, as the patient sequentially meets them.
Personalizing goals and treatment plans for your patients is critical. Each patient has a unique life situation, support system, and way of coping with problems. Unhealthy habits are cumulative and hard to break. Work with patients to monitor their progress, offering suggestions, revising goals or plans when needed, and reminding patients of progress made. It is useful to help patients proactively identify potential obstacles and to anticipate the next steps. You can offer additional suggestions, empathize or commend patient efforts, and revisit actions from the preparation stage if goals need revision. For example, you could say, “You have really worked hard to master your exercises” or “I’m really impressed that you were able to avoid eating sweets this week.” Availability to help patients solve problems or rethink plans, if needed, is also key.
Empowerment Strategies
We distinguish between empowerment as a goal in having control over the determinants of one’s quality of life and as a process in which one has control over problem formulation, decision-making, and the actions one takes to achieve relevant health goals. Patient empowerment takes place through clinician-initiated patient-centered care approaches and through actions patients take on their own initiative.
As a process strategy, empowering people to take the initiative with their own health and well-being supports a person’s ability to maintain his or her role as a functioning adult and facilitates the self-management of chronic disorders, as in the Yon case.
Empowerment Through Social Support
Empowerment implies a gathering of power. Social support from friends and family is an important empowerment
resource in health promotion activities. Social support describes a person’s “integration within a social network,” and “the perceived availability of support” when it is needed. The interested support of significant others can strengthen a person’s resolve, provide input for innovative solutions, and nurture the development of self-efficacy.
Health-related support groups in the community are available for a wide variety of diagnoses, providing relevant information, direct assistance, referral to appropriate resources, and the opportunity to simply interact with others experiencing similar challenges. For example, the Alzheimer’s Association (for Alzheimer disease and related disorders) holds regularly scheduled support groups in most major locations to assist family members. Community-based cancer support groups provide valuable information and support for many common cancer diagnoses. Educational and referral supports enable patients and families to learn the skills they need to effectively manage chronic conditions and to live healthy lives.
Health Promotion as a Population Concept
Community
is defined as a group of citizens that have either a geographic, population-based, or self-defined relationship and whose health may be improved by a health promotion approach. The community offers a natural social system with special significance for facilitating health promotion activities, particularly for people who are economically or socially disadvantaged. It is difficult to change attitudes and lifestyles to promote health when a patient’s social or economic environment does not support prevention efforts.
Successful community-based health promotion activities start with a community analysis of health issues identified by the community. Consciousness raising is critical, as engagement and buy-in of the community in which the activity is to take place is essential. The active participation of individuals, communities, and systems means a stronger and more authentic commitment to the establishment of the realistic regulatory, organizational, and sociopolitical supports that will be needed to achieve targeted health outcomes. Box 14.2 presents health promotion strategies useful at the community level as well as with our individual patients.
Community empowerment seeks to enhance a community’s ability to identify, mobilize, and address the issues that it faces to improve the overall health of the community.
This type of empowerment is fueled by both public policy and targeted education. Successful health promotion programs require individuals, groups, and organizations to act as active agents in shaping health practices and policies that have meaning to a target population. Specific interventions are designed to engage those people who are most involved as active participants in a common environmental concern related to health. Proactive social and political action to enhance health services can augment educational efforts to ensure program viability.
Health promotion activists recognize the community as their principal voice in promoting health and well-being. Health promotion represents a multidisciplinary approach, also inclusive of health education, public health, and environmental health. Health promotion strategies are relevant in clinics, schools, communities, and parishes; they can be introduced during many aspects of routine care in hospitals.
PRECEDE–PROCEED Model
The PRECEDE–PROCEED model is a community education structural framework for designing, implementing, and evaluating community-based health promotion. Developed by Green and Kreuter (2005), this model consists of two components. The PRECEDE dimension refers to the assessment and planning components of the program. The acronym PRECEDE stands for the predisposing, reinforcing, and enabling factors contributing to the educational/organizational diagnosis, which are directly addressed in the proceed component. Behavioral factors that can affect the success of the PRECEDE–PROCEED model are presented in Table 14.2.
Nurses also determine population needs and establish evaluation methods in the PRECEDE phase. Evaluation is a continuous process that begins when the program is implemented and is exercised throughout the educational experience. Sufficient resources, knowledge about target populations, and leadership training are part of an essential infrastructure needed to support health promotion approaches in the community.
A sustainable educational model needs political, managerial, and administrative supports for full implementation of a community-based approach to health promotion and disease prevention. Green later added the PROCEED component (policy, regulatory, organizational constructs in educational and environmental development). This component considers critical environmental and cost variables such as budget, personnel, and critical organizational relationships as part of the implementation phase. Having resources in place and assessing their sustainability is important in successful health promotion programs, although it is not always thought through in the planning phase. Components of the PRECEDE–PROCEED model are presented in Table 14.3.
As with all types of education and counseling, learners need to be actively engaged in goal setting and developing action plans that have meaning to them. The healthcare system is complex and requires a new level of patient decision-making.
Choosing the right strategies requires special attention to the learner’s readiness, capabilities, and skills. Box 14.1 presents strategies in health promotion counseling. Evaluation of health promotion activities is essential. In addition to evaluating immediate program effects, longitudinal evaluation of the impact of health promotion activities on morbidity, mortality, and quality of life is desirable. Keep in mind that what constitutes quality of life is a subjective reality for each patient and may differ from person to person.
Health Promotion Models for Community Empowerment
Community empowerment strategies are used to help identify and address environmental and social issues needed to improve the overall health of the community. This strategy is sometimes referred to as “capacity building.” Community-focused empowerment strategies build on the personal strengths, community resources, and problem-solving capabilities already existing among individuals
and within communities that can be used to address potential and actual health problems. Capacity building requires the inclusion of informal and formal community leaders as valued stakeholders. Networking, partnering, and creating joint ventures with indigenous and local religious organizations is a powerful consensus-building strategy that communities can use for effective health education planning and implementation. Box 14.2 outlines a process for engaging the community in health promotion activities.

Adapted from Green, L., & Kreuter, M. (2021). Health program planning: An educational and ecological approach (5th ed.). New York: McGraw-Hill.
Developmental Level
Developmental level affects both teaching strategies and the delivery of content. You will have patients at all levels of the learning spectrum with regard to their social, emotional, and cognitive development.
Developmental learning capability is not necessarily age-related; it is easily influenced by culture and stress. Social and emotional development does not always parallel cognitive maturity or literacy. Mirroring the patient’s communication style and framing messages to reflect cultural characteristics help improve comprehension and understanding. Parents and other family members can provide information about their child’s immediate life experiences and suggest commonly used words to be incorporated into the nurse’s health teaching.
Avoid information overload and giving vague or conflicting health information to older adults, particularly if
there is any evidence of cognitive processing issues. For example, it is better to say, “Take the white pill when you get up and before you eat your breakfast” than it is to say, “You need to take this medication on an empty stomach.” Written plus oral instructions reinforce messages. Another issue for older adults is that they often have multiple medications, some of which may look alike.
Incorporating Cultural Understandings
Cultural understandings add to the complexity of health promotion strategies in healthcare. Values, norms, and beliefs are an integral part of a person’s self; they influence individual and community lifestyles and health perceptions. Respecting a patient’s cultural values increases a patient’s trust of individual care providers. Eliciting and integrating explanatory information regarding health and illness into health teaching promotes better understanding and greater acceptance of health promotion and disease prevention recommendations. Cultural sensitivity includes knowledge of the preferred communication styles of different cultural groups.
Nurses participate routinely in community health promotion and disease prevention activities. They have an ethical and legal responsibility to maintain the expertise and interpersonal sensitivity required to promote effective patient learning.
Summary
This chapter focuses on communication strategies nurses can use to help people increase understanding of how they can increase health promotion activities. National and global agendas over the past decade reinforce the importance of developing public health policies to create supportive health environments. Specific attention to reducing health disparities, negative social determinants through strengthened community action for health, and increased access for all is advocated. Optimal health and well-being are considered the desired outcomes of health promotion activities.
Health promotion frameworks were presented. Pender’s health belief model identifies perceptions of benefits, barriers, and ability to take action related to health and well-being as components of the individual’s willingness to engage in health promotion activities.
Prochaska’s transtheoretical model is used to explore a person’s readiness to intentionally change his or her health habits.
Bandura’s social learning theory explores the role of self-efficacy in empowering patients to use health promotion and disease prevention recommendations to take better care of their health. The epidemiological model was used to demonstrate that health promotion can occur at any level of health status.
Community-based interventions are critical in addressing broader causal influences on health, referred to as social determinants.
Discussion Questions
- 1. In what ways are the concepts of health literacy and functional health literacy different and alike and why is this important?
- 2. Why are health promotion and disease prevention strategies receiving so much emphasis in contemporary healthcare?
- 3. How would you implement Pender’s model to enhance personal responsibility for health promotion and disease prevention practices?
- 4. Discuss how you could use MI as a tool for helping patients to learn self-management strategies.