Role Transitions
JoAnn Zerwekh, EdD, RN and Ashley Zerwekh Garneau, PhD, RN
When you’re finished changing, you’re finished.
Benjamin Franklin
After completing this chapter, you should be able to:
- • Discuss the concept of transitions.
- • Identify the characteristics of reality shock.
- • Compare and contrast the phases of reality shock.
- • Identify the stages of transition shock.
- • Identify times in your life when you have experienced a reality shock or role transition.
- • Describe methods to promote a successful transition.

Additional resources are available at http://evolve.elsevier.com/Zerwekh/nsgtoday/
Welcome to the profession of nursing! This book is written for nursing students who are in the midst of transitions in their lives. As a new student, you are beginning the transition to becoming indoctrinated into nursing, and sometimes it is not an easy transition. For those of you who are in the middle of nursing school, do you wonder if life even exists outside of nursing school? To students who will soon graduate, hang on; you are almost there! For whatever transition period you are encountering, our goal is to help make your life easier during this period of personal and professional adjustment into nursing. We have designed this book to help you keep your feet on the ground and your head out of the clouds, as well as to boost your spirits when the going gets rough.
As you thumb through this book, you will notice that there are cartoons and critical thinking questions that encourage your participation. Do not be alarmed; we know you have been overloaded with “critical thinking” during nursing school! These critical thinking questions are not meant to be graded; instead, their purpose is to encourage you to begin thinking about your transition, either into nursing school or into practice, and to guide you through the book in a practical, participative manner. Our intention is to add a little humor here and there while giving information on topics we believe will affect your transition into nursing practice. We want you to be informed about the controversial issues currently affecting nursing. After all, the future of nursing rests with you!
Are you ready to begin? Then let’s start with the real stuff. You are beginning to experience transitions—for some of you, just getting into nursing school has been a long struggle—and you are there! For others, you can see the light at the end of the tunnel as graduation becomes a reality. Nursing is one of the most rewarding professions you can pursue. However, it can also be one of the most frustrating. As with marriage, raising children, and the pursuit of happiness, there are ups and downs. We seldom find the world or our specific situation the exact way we thought it would or should be. Often your fantasy of what nursing should be is not what you will find nursing to be.
You will cry, but you will also laugh.
You will share with people their darkest hours of pain and suffering, but
You will also share with them their hope, healing, and recovery.
You will be there as life begins and ends.
You will experience great challenges that lead to success.
You will experience failure and disappointment.
You will never cease to be amazed at the resilience of the human body and spirit.
Transitions
What are Transitions?
Transitions are passages or changes from one situation, condition, or state to another that occur over time. They have been classified into the following four major types: developmental (e.g., becoming a parent, midlife crisis), situational (e.g., graduating from a nursing program, career change, divorce), health or illness (e.g., dealing with a chronic illness), and organizational (e.g., change in leadership, new staffing patterns) (Schumacher & Meleis, 1994).
What are Important Factors Influencing Transitions?
Understanding the transition experience from the perspective of the person who is experiencing it is important because the meaning of the experience may be positive, negative, or neutral, and the expectation may or may not be realistic. The transition may be desired (e.g., passing the NCLEX exam) or undesirable (e.g., the death of a family member, after which you have to assume a new role in your family).
Another factor in the transition process is the new level of knowledge and skill required, as well as the availability of needed resources within the environment. Dealing with new knowledge and skills can be challenging and stressful and can lead to a variety of different emotions related to the expectation of the new graduate to be competent (Box 1.1). This will resolve as your confidence grows and you have more understanding of the concept of how to “think like a nurse.”
Transitions are a part of life and certainly a part of nursing. Although the following discussions on role transition and reality shock focus on the graduate nurse experience, there are many applicable points for the new student as well. As you learn more about transitions, reality shock, and the graduate nurse experience, think about how this information may also apply to your transition experience into and through nursing school (Critical Thinking Box 1.1).
 Critical Thinking Box 1.1
Critical Thinking Box 1.1
Thoughts About Transition
What is your greatest concern about your transition? Is it personal or work transitions because you are a student nurse, or is it your transition from school to the practice setting?
Looking back, what transitions have you experienced? What transitions are occurring in your life now? Has your entry into, as well as progress through, nursing school caused transitions in your personal life? Has your anticipated job search caused transitions in your professional as well as personal life?
Transitions in Nursing
The paradox of nursing will become obvious to you early in your nursing career. This realization may occur during nursing school, but it frequently becomes most obvious during the first 6 months of your first job.
Health care organizations are very concerned about your transition experience and job satisfaction during that first 6 months of employment. Have you been hearing about “evidence-based practice?” Well, it is working for you now! During the first 6 months of employment, new graduates need a period of time to develop their skills in a supportive environment. Employee retention and job satisfaction are key issues with hospitals; confidence in performing skills and procedures, nurse residency programs, and dependence versus independence are key graduate nurse issues driving this research. The well-being of the graduate nurse and the ability to deliver quality nursing care during the transition period have sparked research to validate the need for special considerations of the graduate nurse experiencing transition (Casey et al., 2004; Duchscher, 2008, 2009; Godinez et al., 1999; Lavoie-Tremblay et al., 2002; Spector et al., 2015a; Steinmiller et al., 2003; Varner & Leeds, 2012). With identification of the basic problems encountered by new graduates during this first 6 months, there is a concerted effort to begin to meet the special needs of graduate nurses and assist them to “think like a nurse” (Research for Best Practice Box 1.1). Thinking like a nurse involves critical thinking, decision making, and clinical judgment. You may think these terms mean the same thing, but they do not. Just what exactly do these terms mean?
- ■ Critical thinking is active, purposeful, organized cognitive process used to carefully examine one’s thinking and the thinking of other individuals (Potter et al., 2021).
- ■ Decision making is the process involving critical appraisal of information that begins with recognizing a problem and ends with generating, testing, and evaluating a conclusion and comes at the end of the critical thinking process (Potter et al., 2021).
- ■ Clinical judgment is the observed outcome of critical thinking and decision making. It is an iterative process that uses nursing knowledge to observe and assess presenting situations, identify a prioritized client concern, and generate the best possible evidence-based solutions to deliver safe client care (NCSBN, 2019).
- ■ Throughout this text, you will find Critical Thinking Boxes to stimulate your thinking and Next Generation NCLEX (NGN) test items, which are a “call” for you to use clinical judgment.
The role transition process that occurs on entry into nursing school and the process from student to graduate nurse do not take place automatically. Having the optimal experience during role transition requires a great deal of attention, planning, and determination on your part. How you perceive and handle the transition will determine how well you progress through the process. It is important that you keep a positive attitude. The challenges and rewards of clinicals, tests, and work situations will cause your emotions to go up and down, but that is okay. It is expected, and you will be able to deal with it effectively. It is important that you keep a positive attitude. The wide range of emotions experienced during the transition process can often affect your emotional and physical well-being; check out the discussion of self-care strategies in Chapter 2.
So, let’s get started. Reality shock is often one of the first hurdles of transition to conquer in your new role as a graduate nurse or registered nurse (RN or Real Nurse). 
Reality Shock
What is Reality Shock?
Reality shock is a term often used to describe the reaction experienced when one moves into the workforce after several years of educational preparation. The recent graduate is caught in the situation of moving from a familiar, comfortable educational environment into a new role in the workforce in which the expectations are not clearly defined or may not even be realistic. For example, as a student, you were taught to consider the patient in a holistic framework, but in practice, you often do not have the time to consider the psychosocial or teaching needs of the patient even though they must be attended to and documented.
 Research for Best Practice Box 1.1
Research for Best Practice Box 1.1
Role Transition: Think Like a Nurse
Practice Issue
Students report that when they first entered their nursing courses, they were unaware of the complexity of thinking and problem solving that occurs in the clinical setting. They often are unable to “think on their feet” and change a planned way of doing something based on what is happening with a specific patient at any given moment. Research supports the finding that the beginning nursing graduate continues to have difficulty making clinical judgments (i.e., thinking like a nurse) (Etheridge, 2007; Ward & Morris, 2016). Graduates with baccalaureate degrees in nursing were interviewed three times in 9 months to determine their perceptions of how they learned to think like nurses (Tanner, 2006). In a later simulation study by Ashley and Stamp (2014), thinking like a nurse was one of the major themes that emerged when comparing sophomore and junior students. During simulation, the sophomore student approached the clinical scenario more as a layperson than as a professional with specialized knowledge, which was exhibited by little preplanning and the expectation that the clinical problem would be self-evident and would require nothing more than common sense to achieve an outcome.
Implications for Nursing Practice
Clinical Judgments—Thinking Like a Nurse
- • Nursing students and new graduates are often unaware of the level of responsibility required of nurses and lack confidence in their ability to make clinical judgments.
- • The process of learning to think like a nurse is characterized by building confidence, accepting responsibility, adapting to changing relations with others, and thinking more critically.
- • Multiple clinical experiences, support from faculty and experienced nurses, and sharing experiences with peers were critical in the transition from student nurse to beginning practitioner.
- • Nursing education must assist nursing students to engage with patients and act on a responsible vision for excellent care of their patients and with a deep concern for the patients’ and families’ well-being. Clinical reasoning and clinical judgment must arise from this engaged, concerned stance.
Considering This Information
What types of resources will you use as a nursing student to improve your clinical reasoning and clinical judgment skills? What characteristics have you observed in staff members who effectively “think like a nurse”? How can you begin to incorporate these aspects into your practice as a new graduate nurse?
The recent graduate in the workplace is expected to be a capable, competent nurse. That sounds fine. However, sometimes there is a hidden expectation that graduate nurses should function as though they have 5 years of nursing experience. Time management skills, along with the increasing acuity level of patients, are common problems for new graduates. This situation may leave you with feelings of powerlessness, depression, and insecurity because of an apparent lack of effectiveness in the work environment. There are positive ways to deal with the problems. You are not alone! Reality shock is not unique to nursing. It is present in many professions as graduates move from the world of academia to the world of work and begin to adjust to the expectations and values of the workforce.
What are the Phases of Reality Shock?
Kramer (1974) described the phases of reality shock as they apply to nursing (Table 1.1). Although she identified this process in 1974, these phases remain the basis for understanding the implications of reality shock and successfully progressing through the process. In our current world of nursing, we are still dealing with this same process. Adjustments begin to take place as the graduate nurse adapts to the reality of the practice of nursing. The first phase of adjustment is the honeymoon phase (Fig. 1.1). Recent graduates are thrilled with completing school and accepting a first job. Life is a “bed of roses” because everyone knows nursing school is much harder than nursing practice. There are no more concept care maps to create, no more nursing care plans to write, and no more burning the midnight oil for the next day’s examination. No one is watching over your shoulder while you insert a catheter or administer an intravenous medication. You are not a “student” anymore; now you are a nurse! During this exciting phase, your perception of the situation may feel unreal and distorted, and you may not be able to understand the overall picture.
Table 1.1
| Honeymoon | Shock and Rejection | Recovery |
|---|---|---|
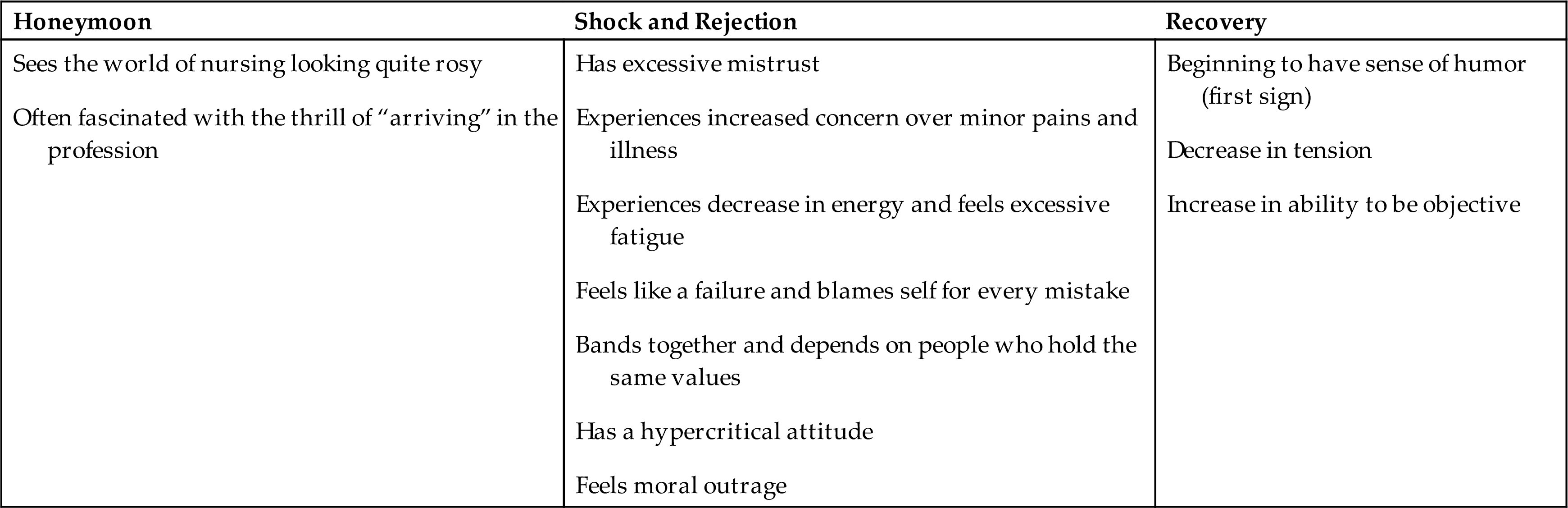
The honeymoon phase is frequently short lived as the graduate begins to identify the conflicts between the way she or he was taught and the reality of what is done. Every graduate nurse has a unique way of coping with the situations; however, some common responses have been identified. The graduate may cope with this conflict by withdrawing or rejecting the values learned during nursing school. This may mark the end of the honeymoon phase of transition. The phrase “going native” was used by Kramer and Schmalenberg (1977) to describe recent graduates as they begin to cope and identify with the reality of the situation by rejecting the values from nursing school and beginning to function as everyone else does.
With experiences such as this during transition, graduates may feel as though they have failed and begin to blame themselves for every mistake. They may also experience moral outrage at having been put in such a position. When the bad days begin to outnumber the good days, the graduate nurse may experience frustration, fatigue, and anger and may consequently develop a hypercritical attitude toward nursing. Some graduates become very disillusioned and drop out of nursing altogether. This is the period of shock and rejection.
A successfully managed transition period begins when the graduate nurse is able to evaluate the work situation objectively and predict the actions and reactions of the staff effectively. Prioritization, conflict management, time management, and support groups (peers, preceptors, and mentors) can make a significant difference in promoting a successfully managed transition period.
Nurturing the ability to see humor in a situation may be the first step. As the graduate begins to laugh at some of the situations encountered, the tension decreases, and the perception increases. It is during this critical period of recovery that conflict resolution occurs. If this resolution occurs in a positive manner, it enables the graduate nurse to grow more fully as a person. This growth also enables the graduate to meet the work expectations to a greater degree and to see that she or he has the capacity to change a situation. However, if the conflict is resolved in a less positive manner, the graduate’s potential to learn and grow is limited.
Kramer (1974) described four groups of graduate nurses and the steps they took to resolve reality shock. The graduates who were considered to be most successful at adaptation were those who “made a lot of waves” within both their job setting and their professional organizations. Accordingly, they were not content with the present state of nursing but worked to effect a better system. This group of graduates was able to take worthwhile values learned during school and integrate them into the work setting. Often, they returned to school—but not too quickly. Since Kramer’s original work, students are now encouraged to go back to school fairly quickly, especially with the emphasis from the Institute of Medicine (IOM) report of encouraging more advanced degrees in nursing.
Another group limited their involvement with nursing by just putting in the usual workday. Persons in this group seldom belonged to professional organizations and cited the following reasons for working: “to provide for my family,” “to buy extra things for the house,” and “to support myself.” Typically, this group’s negative approach to conflict resolution leads to burnout, during which time the conflict is turned inward, leading to constant griping and complaining about the work setting.
Another group of graduates seemed to have found their niche and were content within the hospital setting. However, their positive attitude toward the job did not extend to nursing as a profession; in fact, it was the opposite. Rather than leave the organization during conflict, these “organization nurses” would change units or shifts—anything to avoid increasing demands for professional performance.
The last group of graduates frequently changed jobs. After a short-lived career in hospital nursing, this group would pirouette off to graduate school, where they could “do something else in nursing” (meaning “I can’t nurse the way I’ve been taught, so I might as well teach others how to do things right”). Achieving a high profile in professional nursing organizations was common for these graduates, along with seeking a safer, more idealistically structured environment in which the values learned in school prevail.
The job expectations of the hospital administration or the employing community agency and the educational preparation of the graduate nurse are not always the same. This discrepancy is considered to be the basis of reality shock. Relationships among the staff, nursing professionalism, job satisfaction, and employee alienation were studied by Casey and colleagues (2004), Roche and colleagues (2004), and Varner and Leeds (2012). Interestingly, the issues of reality shock and role transition described by Kramer in the early 1970s are still around. We (nurses) have entered the 21st century with many of the same issues we had in the 20th century.
It might seem to you right now, after reading all of this information, that reality shock is a life-threatening situation. Be assured, it is not. However, you may experience some physical and psychological symptoms in varying degrees of intensity. For example, you may feel stressed out or have headaches, insomnia, gastrointestinal upset, or a bout of post-student blues. Just remember that it takes time to adjust to a new routine and that sometimes, even after you have gotten used to it, you still may feel overwhelmed, confused, or anxious. The good news is that there are various ways to get through this critical phase of your career while establishing a firm foundation for future professional growth and career mobility. Try the assessment exercise in Critical Thinking Box 1.2 and review the clinical judgment case scenario in the NGN Box 1.1.
Critical Thinking Box 1.2
Reality Shock Inventory
All students, as well as new graduates, experience reality shock to some extent or another. The purpose of this exercise is to make you aware of how you feel about yourself and your particular life situation.
Directions: To evaluate your views and determine your self-evaluation of your particular life situation, respond to the statements with the appropriate number.
| 1 Strongly agree | 4 Slightly disagree |
| 2 Agree | 5 Disagree |
| 3 Slightly agree | 6 Strongly disagree |
- 1. I am still finding new challenges and interests in my work.
- 2. I think often about what I want from life.
- 3. My own personal future seems promising.
- 4. Nursing school or my work has brought stresses for which I was unprepared.
- 5. I would like the opportunity to start anew knowing what I know now.
- 6. I drink more than I should.
- 7. I often feel that I still belong in the place where I grew up.
- 8. Much of the time, my mind is not as clear as it used to be.
- 9. I have no sense of regret concerning my major life decision of becoming a nurse.
- 10. My views on nursing are as positive as they ever were.
- 11. I have a strong sense of my own worth.
- 12. I am experiencing what would be called a crisis in my personal or work setting.
- 13. I cannot see myself as a nurse.
- 14. I must remain loyal to commitments even if they have not proven as rewarding as I had expected.
- 15. I wish I were different in many ways.
- 16. The way I present myself to the world is not the way I really am.
- 17. I often feel agitated or restless.
- 18. I have become more aware of my inadequacies and faults.
- 19. My sex life is as satisfactory as it has ever been.
- 20. I often think about students or friends who have dropped out of school or work.
To compute your score, reverse the number you assigned to statements 1, 3, 9, 10, 11, and 19. For example, 1 would become a 6, 2 would become a 5, 3 would become a 4, 4 would become a 3, 5 would become a 2, and 6 would become a 1. Total the number. The higher the score, the better your attitude. The range is 20 to 120.
Modified from White, E. (April 23, 1986). Doctoral dissertation. Chronicle of Higher Education (p. 28). Reprinted with permission.
 Call for Clinical Judgment Next-Generation Nclex® Examination–Style Case Study Box 1.1
Call for Clinical Judgment Next-Generation Nclex® Examination–Style Case Study Box 1.1
A 22-year-old newly licensed RN has completed a 4-week orientation at her place of employment. The nurse works with an assigned mentor over the next 6 months on the medical-surgical unit. Lately, the nurse believes that she cannot meet her assigned clients' needs because she feels overwhelmed by high client acuity, overtime, and a stressful environment with high staff turnover. Because of the pandemic crisis, the organization instituted mandatory overtime to help overcome the staffing shortage. The nurse often works a 12-hour shift and 5 or 6 days in row. The nurse reports feeling tired all the time and having difficulty focusing and prioritizing client care assignments, especially near the end of her shift when needing to give report to the oncoming shift. The nurse reports lack of time to spend with her friends and rarely has time to call or visit with her family because of working so many extra hours each week.
Which of the following would be signs of a successful role transformation for this new nurse? Select all that apply.
- 1. Having a couple glasses of wine each evening to unwind
- 2. Changing jobs and starting a new position at another agency
- 3. Nurturing the ability to see humor in various situations
- 4. Asking to schedule a vacation and requesting time off work
- 5. Learning to prioritize time better while caring for clients
- 6. Maintaining a healthy lifestyle of adequate sleep, diet, and exercise
- 7 . Avoiding mini-breaks throughout the workday
- 8. Seeking the help of other staff when her client workload becomes unmanageable
What is Transition Shock?
More recently, based on research by Duchscher (2008) building on Kramer’s seminal work, the process has been redefined as transition shock to describe the transition experience within a contemporary health care environment and according to Wakefield (2018), “penetrates beyond professional aspects of shock” (p. 47). Duchscher and Windey (2018) identify the stages of transition as a process of “becoming” that occur within the initial 12 months of nursing practice of the new graduate nurse and involves three stages: doing, being, and knowing. Box 1.2 summarizes the three stages.
 Critical Thinking Box 1.3
Critical Thinking Box 1.3Role Transformation
Remember when you first started nursing school? The war stories everybody told you? The changes that occurred in your family as a result of starting nursing school? Are you in the midst of that now, or does it seem like a long time ago? Can you really believe where you are now and where you were when you first began nursing school, those first nursing courses, and clinicals? It has taken a lot of work and sacrifice to get to where you are now. Believe it or not, you have already experienced a role transition—you successfully transitioned to being a student nurse. Now, as you draw nearer to the successful completion of that experience, you are ready to embark on a new one. Take a minute to read the thoughts of one of your peers about her transition into nursing. I’m sure you will smile at her satire (Critical Thinking Box 1.3).
Give yourself a well-deserved pat on the back for what you have accomplished thus far. It is important to learn early in your practice of nursing to take time to reflect on your accomplishments. Now, back to the present. Let’s look at the current role-transition process at hand, from student to graduate nurse RN.
Critical Thinking Box 1.4
Survival Techniques From One Who Has Survived
You finally did it; you have decided nursing is what you want to do for the rest of your life. After all, who would go through all this anguish if you only wanted to do this as a pastime? If you are taking this like everyone else, you are probably going to do this by trial and error, through “war” stories, or through helpful hints from the nursing staff.
You need to prioritize your time. This is a familiar and much-used term that you will hear often. It is also easier said than done. If you are single, you have an advantage—maybe. You can decide right now that single is “where it’s at” and stay that way for the duration. Of course, this means literally living the “single” life. There are no “dinners for two,” no telephone conversations, no movies at the cinema (rarely any TV)—in other words, no physical contact with anyone. I know you were not thinking about it anyway, but in case you are studying anatomy and physiology and hormonal thoughts pervade your consciousness, dismiss them.
If you are married, I am not suggesting divorce, just abstinence. Hopefully, you kissed your spouse good-bye when you came to school for your first day of class because your next chance will be on your breaks or when you graduate.
If you happen to be a parent, do as I did. I put pictures of myself in all rooms of my house when I started school so that the kids would not forget me. My children, in return, helped me by plastering their faces in my fridge (they know I’ll look there) or on my mirror (another sure spot). I have acquired a son-in-law, a daughter-in-law, and five grandchildren in the past 2½ years, and I usually do not recognize them if I run into them on the rare occasions when I go to the store for essentials (like food) or out to pay our utility bills. Christmas is fun, though, because each year I get to spend a few days getting to know the family again. But we all must wear name tags for the first day!
If your children are small, buy them the Fisher-Price kitchen and teach them how to “cook” nourishing “hot” cereal on the stove that does not heat up. For the infant, hang a TPN (hint: total parental nutrition) of Similac with iron at 40 mL/h that the baby can control by sound! Crying should do it! Instead of a needle, use a nipple….
Diapers—what would we do without those disposable diapers that stay dry for 2 weeks at a time? You can even buy the kind that you touch the waistband, and Mickey Mouse and his friends jump off to entertain your baby.
Some of you may feel guilty about not fixing those delicious meals your family once enjoyed. Do not! We get two “breaks” a year, and during that time, fix barrels of nourishing liquid (you can add a few veggies). When your family gets hungry, just take out enough to keep fluids and lytes balanced. Remind them that this is only going to last another year or two.
Have I covered everything? Oh, I forgot dust.… Dust used to bother me but not anymore. I use it to write notes to my 17-year-old, to let him know what time I am going to be in the house, so he will not mistake me for a burglar, and to say “I love you.”
On a serious note, each semester, you will get regrouped with new classmates. They will become your family, your support group. You will form a chain, and everyone is a strong link. This is a group effort. These are people who will laugh with you and cry with you. You will form friendships that will last a lifetime. Take advantage of these opportunities.
On a closing note, do not listen to all the “war stories” that go around—just to the credible ones like mine!
From Beagle, B. (May/June 1990). Survival techniques. AD Clinical Care (p. 17). Reprinted with permission.
When Does the Role Transition to Graduate Nurse Begin?
Does the transition begin at graduation? No. It started when you began to move into the novice role while in your first nursing course (Table 1.2). According to Benner (2001; 1984, p. 20):
Table 1.2
| Stage | Characteristics |
|---|---|
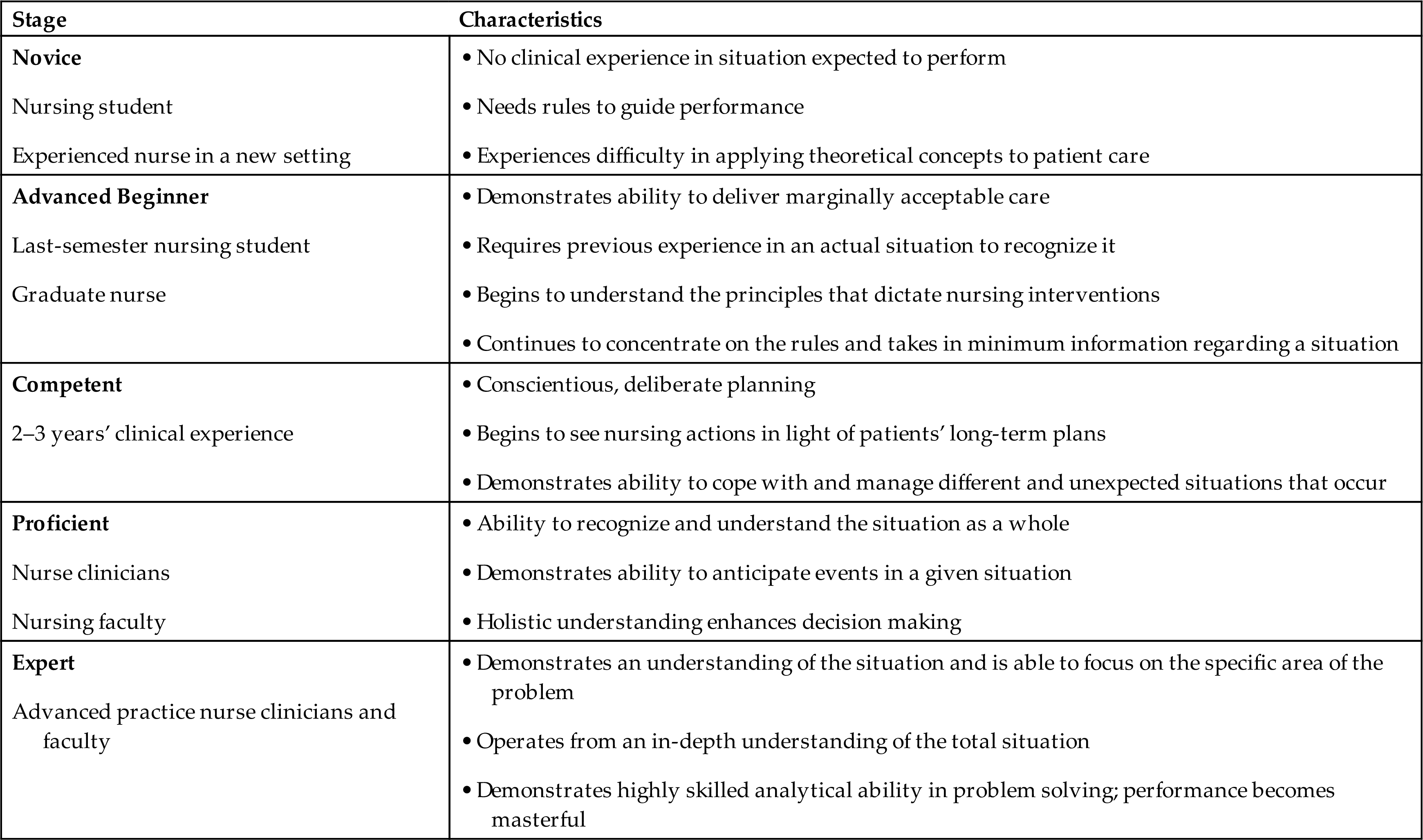
Modified from Benner, P. (2001). The Dreyfus model of skill acquisition applied to nursing. In From novice to expert (Commemorative Edition). Addison-Wesley.
Beginners have no experience of the situation in which they are expected to perform. To get them into these situations and allow them to gain experience also necessary for skill development, they are taught about the situation in terms of objective attributes, such as weight, intake/output, temperature, blood pressure, pulse, and other objective, measurable parameters of a patient’s conditions—features of the task world that can be recognized without situational experience.
For example, the instructor gives a novice or student nurse specific directions on how to listen for bowel sounds. There are specific rules on how to guide their actions—rules that are very limited and fairly inflexible. Remember your first clinical nursing experiences? Your nursing instructor was your shadow for patient care. As nursing students enter a clinical area as novices, they have little understanding of the meaning and application of recently learned textbook terms and concepts. Students are not the only novices; any nurse may assume the novice role on entering a clinical setting in which he or she is not comfortable functioning or has no practical experience. Consider an experienced medical-surgical nurse who floats to the postpartum unit; he or she would be a little uncomfortable in that clinical setting.
By graduation, most nursing students are at the level of advanced beginner. According to Benner (2001; 1984, p. 20):
Advanced beginners are ones who can demonstrate marginally accepted performance, ones who have coped with enough real situations to note (or to have pointed out to them by a mentor) the recurring meaningful situation components….
To be able to recognize characteristics that can be identified only through experience is the signifying trait of the advanced beginner. Thus, when directed to perform the procedure of checking bowel sounds, the students at this level are learning how to discriminate bowel sounds and understand their meaning. They do not need to be told specifically how to perform the procedure.
Let’s look at what you and your nursing instructors can do to promote your well-being and success during the role-transition experience. These activities reinforce your progress and movement along the continuum from advanced-beginner to competent nurse (see Table 1.2).
How Can I Prepare Myself for This Transition Process?
During the last semester of nursing school, it is very advantageous to have as much clinical experience as possible. The most productive area for experience is a general medical-surgical unit, which has a variety of patient cases. This helps you to ground your assessment and communication skills, as well as help you to apply principles that are most often tested on the NCLEX exam. This is also the area in which you will most likely be able to obtain some much-needed experience with basic nursing skills.
Begin Increasing Independence
It is time to have your nursing instructor cut the umbilical cord and allow you to function more independently, without frequent cueing and directing during the last semester of your clinical experience.
More Realistic Patient-Care Assignments
Start taking care of increasing numbers of patients to help you with time management, prioritization, and work organization. Evaluate the nursing staff’s assignments to determine what a realistic workload is for a recent graduate.
Clinical Hours that Represent Realistic Shift Hours
Obtain experience in receiving shift reports, closing charts, completing patient care, and communicating with the oncoming staff and other health care professionals involved in providing patient care.
Perform Nursing Procedures Instead of Observing
Take an inventory of your nursing skills and be sure to have this available for potential employers so they can see what skills you possess. If there are nursing skills you lack or procedures you are uncomfortable with, take this opportunity while you are still in school to gain the experience. Identify your clinical objectives to meet your personal needs. Request opportunities to practice from your instructor and staff nurses. Casey and colleagues (2004) identified skills that were challenging for graduate nurses in the first year of practice, which are currently still applicable. These skills included code blues, chest tubes, intravenous skills, central lines, blood administration, and patient-controlled analgesia. Although it is important for you to be proficient and safe in performing skills, Theisen and Sandau (2013) pointed out in their review that new graduate nurses lack competency in communicating with the health care team, delegating, resolving conflict during stressful situations (e.g., end-of-life care, deteriorating patient), prioritizing patient care, and making critical decisions. Make an effort to gain experience in these areas while you are still in school; you will be more comfortable in your nursing care as a graduate.
More Truth About the Real Work-Setting Experience
Identify people with whom you can objectively discuss the dilemmas of the workplace. Talk to graduates. Ask them what they know now that they wish they had known the last semester of school.
Look for Opportunities to Problem Solve and Practice Critical Thinking
Actively seek out learning opportunities in both the clinical and classroom setting to exercise your critical thinking skills and decision making. Now is the time to stand on your own two feet while there is still a backup—your instructor—available. Look for opportunities to communicate with the interprofessional team.
Request Constructive Feedback from Staff and Instructors
Stop avoiding evaluation and constructive criticism. Find out now how you can improve your nursing care. Ask questions and clarify anything that is not understood. Evaluate your progress on a periodic basis. The consequences may be less severe now than later with your new employer.
Request Clinical Experience in an Area or Hospital of Interest
If you have some idea of where you would like to work, it is very beneficial to have some clinical experiences in that facility the last semester of school. This gives you the opportunity to become involved with staff nurses, identify workload on the unit, and evaluate resources and support people. It also gives the employing institution an opportunity to evaluate you are you someone that institution would like to have work for them?
Think Positively
Be prepared for the reality of the workplace environment, including both its positives and negatives. You may have encountered by now the “ol’ battle ax” who has a grudge against new nursing graduates.
When you find these nurses, tune them out and steer out of their way! They have their own agenda, and it does not include providing supportive assistance to you. Eventually, you will learn how to work with this type of individual (see Chapter 13), but for now you should concentrate on identifying nurses who share your philosophy and are still smiling.
Another way to keep a positive perspective is to focus on the good things that have happened during the shift rather than on the frustrating events. When you feel yourself climbing onto the proverbial “pity pot,” ask yourself “Who’s driving this bus?” and turn it around!
Anticipate small irritations and disappointments and keep them in perspective. Do not let them mushroom into major problems. Turn disappointments and unpleasant situations into learning experiences. When you have encountered an unpleasant situation, the next time it occurs, you will recognize it sooner, anticipate the chain of events, and be better able to handle it.
Be Flexible
Procedures, policies, and nursing supervisors are not going to be the same as those you experienced in school. Be prepared to do things different from the way you learned them as a student. You do not have to give up all the values you learned in school, but you will need to reexamine them in light of the reality of the workplace setting. Flexibility is one of the most important qualities of a good nurse!
School-learned ideal.
Sit down with the patient before surgery and provide preoperative teaching.
Workplace reality.
One of your home care patients is receiving daily wound care for an extensive burn. You receive a message that the patient has been scheduled for grafting in the outpatient surgery department and is to be a direct admit at 6 AM the next morning. You have two more home visits to make: one to hang an intravenous preparation of vancomycin and the other a new hospice admission, which you know will take considerable time.
Compromise.
You delegate to one of the home care practical nurses to take the preoperative teaching and admission instructions to your patient. Later on, you make a telephone call to your preoperative patient and go over the preoperative care teaching information from the home care practical nurse. You make arrangements to meet this patient at home immediately after the grafting procedure is complete.
Get Organized
Does your personal life seem organized or chaotic, calm or frantic? Sit back and take a quick inventory of your personal life. How do you expect to get your professional life in order when your personal life is in turmoil? For some helpful tips on organizing your personal life, check out the personal management chapter (see Chapter 2).
Stay Healthy
Have you become a “couch potato” while in school? Are you too tired, or do you lack the time to exercise when you get home from work? Candy bars during breaks, pepperoni pizza at midnight, and Twinkies PRN? How have your eating habits changed during your time in school? Your routine should include exercise, relaxation, and good nutrition. Becoming aware of the negative habits that can have detrimental effects on your state of mind and overall physical health is important in developing a healthy lifestyle.
Find a Mentor
Negotiating this critical transition as you begin your nursing career should not be done in isolation. Evidence suggests that close support relationships, mentors, and preceptors are key, if not essential, ingredients in the career development of a successful, happy graduate (Duchscher & Windey, 2018). For additional tips on finding a mentor as you begin your professional practice, take a look at the mentoring chapter (see Chapter 3). In addition to your family and close nursing school friends, it is important to develop professional support relationships.
Find Other New Graduates
Frequently, several new graduates are hired at the same time. Some of them may even be your classmates. Find them and establish a peer support group. Sharing experiences and problems and knowing that someone else is experiencing the same feelings you are can be a great relief!
Have Some Fun
Do something that makes you feel good. This is life, not a funeral service! Nursing has opportunities for laughter and for sharing life’s humorous events with patients and coworkers. Surround yourself with people and friends who are lighthearted and merry and who bring out these feelings in you. Remember, the return of humor is one of the first signs of a healthy role transition. Loosen up a little bit. Go ahead, have some fun! Check out the information in Chapter 3 for more on selection of mentors and preceptors.
Know What to Expect
Plan ahead. Plan your employment interviews; ask to talk to nurses on the units and find out how nursing care is delivered in the institution. The length of orientation, staffing patterns, opportunity for internship, areas where positions are open, and resources for new graduates are all important to establish before employment. This helps you know what to expect when you go to work. Work satisfaction is a positive predictor of a successful role transition during the first year (Roche et al., 2004). Know what is expected of you on your work unit. How can you expect to do a job correctly if you do not know what the expectations are? Learn the “rules of the road” early. This may be in the hospital, doctor’s office, or community setting. While still in school, you may find it helpful to interview nurse managers to determine their perspectives on the role of the graduate nurse during the first 6 months of employment. This will give you a base of reference when you interview for your first job. How do you measure up to some of the common expectations nurse managers may be looking for in a graduate nurse?
- 1. Excited and sincere about nursing?
- 2. Open-minded and willing to learn new ideas and skills?
- 3. Comfortable with your basic nursing skills?
- 4. Able to keep a good sense of humor?
- 5. Receptive to constructive feedback?
- 6. Able to express your thoughts and feelings?
- 7. Able to evaluate your performance and request assistance?
- 8. Comfortable talking with your patients regarding their individual needs?
What is the Future of Role Transition?
In 2008, the Practice and Education Committee of the National Council of State Boards of Nursing (NCSBN) reported there was adequate evidence to support a regulatory model for transitioning new graduates to practice (NCSBN, 2008; NCSBN Learning Extension, 2021). The committee noted that the need for a transition regulatory model has grown from the changes occurring in health care over the past 20 years, not from deficiencies in nursing education or unrealistic expectations of the workplace. In the report from the committee to the NCSBN, the goal for the transition to practice regulatory model is “to promote public safety by supporting newly licensed nurses in their critical entry and progression into practice” (NCSBN, 2008, p. 2). In 2009, the NCSBN finalized the design of an evidence-based “transition to practice” regulatory model (Fig. 1.2) that includes modules on communication and teamwork, patient-centered care, evidence-based practice, quality improvement, informatics, and an additional module of preceptor training.
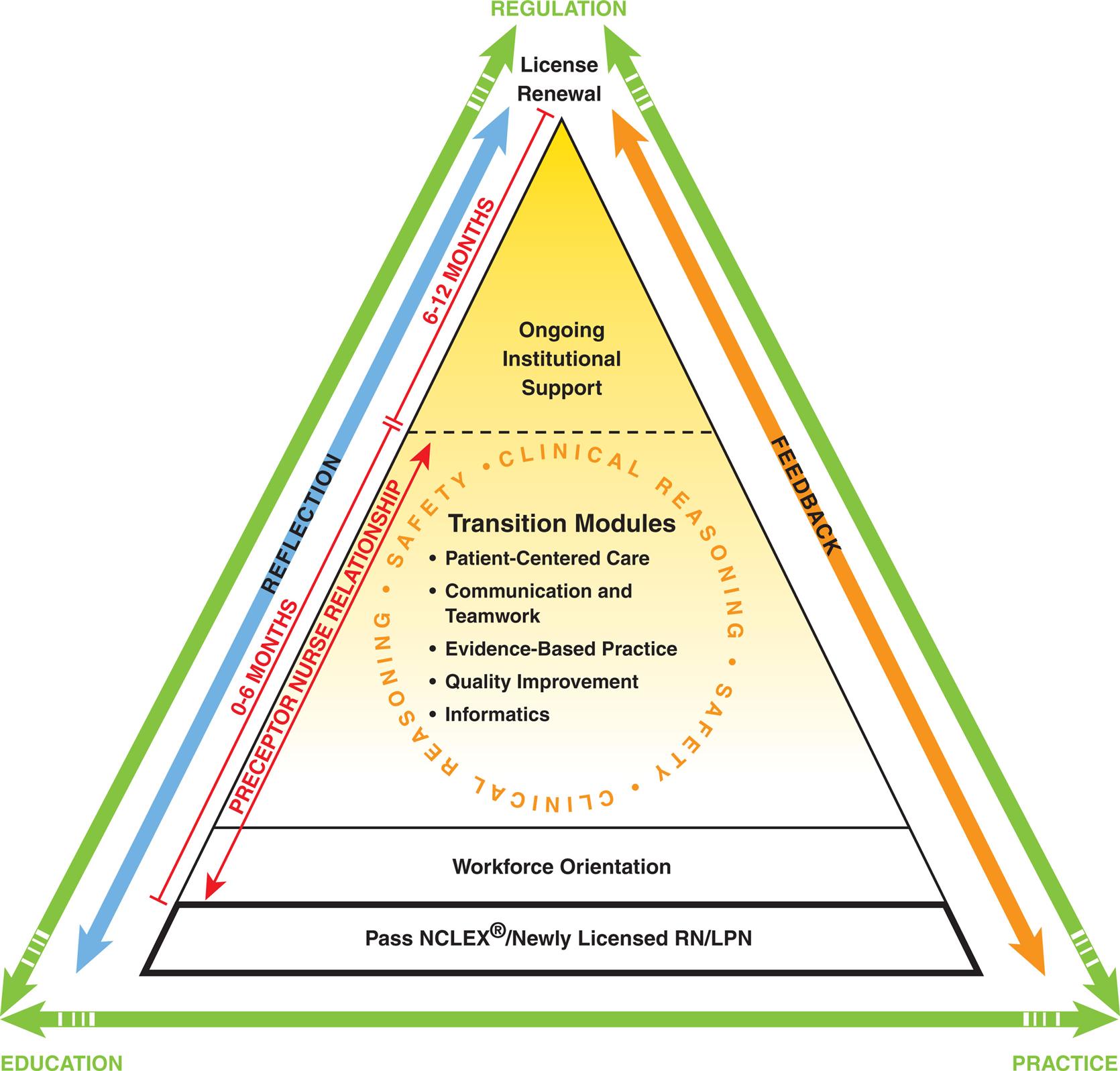
A pyramid shows Transition to Practice model as follows: • Level 1 include Pass N C L E X or Newly Licensed R N or L P N. • Level 2 includes workforce orientation. • Level 3 includes transition modules: Patient-centered care, communication and teamwork, evidence-based practice, quality improvement, and informatics. Clinical reasoning and safety form a circle around it. • Level 4 (6 to 12 months) includes ongoing institutional support with license renewal marked at the peak of the pyramid. • Level 2 and 3 (0 to 6 months) are preceptor nurse relationship. A double headed arrow marks reflection on left, feedback on right, regulation at top, and education and practice at left and right at the bottom respectively.
The results from the national Transition to Practice (TTP) study in hospital settings conducted by the NCSBN have been reported (NCSBN, 2021), which addressed questions about the effectiveness of the NCSBN’s TTP program and whether or not TTP programs make a difference in new graduate outcomes in terms of safety, competence, stress, job satisfaction, and retention (Research for Best Practice Box 1.2).
The TTP model recommends a 9- to 12-month internship so that new graduates receive continued support during the vulnerable period from 6 to 9 months. For the transition process to be effective, it should occur across all settings and at all education levels. This includes both RNs and LPNs and LVNs. To promote safer nursing practice through a regulatory transition period, practice, education, and regulation all must work together on the development of a model that will effectively support the new nurse in his or her transition to safe practice (Spector, 2015; Spector et al., 2015b).
The NCSBN Learning Extension (2021) offers an e-learning transition to practice course based on the NCSBN’s evidence-based comprehensive research study, TTP, that incorporates the recommendations from the QSEN project and the IOM. The program consists of five courses for new graduate nurses on the topics of communication and teamwork, patient- and family-centered care, evidence-based practice, quality improvement, and informatics, along with a preceptor course (NSCBN, 2013). It is a 6-month online program, which requires only 1 hour per week of coursework with continuing education credit provided upon completion.
Research for Best Practice Box 1.2
Role Transition
Practice Issue
With the increased complexity of the health care environment, new graduates struggle with the transition into clinical practice. This matter is related to several issues: sicker patients in an increasingly complex health care setting, the shortened gap between taking NCLEX and being licensed, variable transition experiences, increased patient workload because of the nursing shortage, high job stress and turnover rates in new graduate RNs (approximately 25% of new nurses leave their position within the first year of practice), and practice errors (NCSBN, 2021).
Implications for Nursing Practice
- • Transition experiences of new RNs vary across practice settings.
- • Building resilience, or the ability to overcome adversity and grow stronger from the experience, is an essential skill for the new graduate (Thomsas & Asselin, 2018).
- • Health care agencies with formalized transition programs have noted a marked drop in new graduate attrition, along with improved patient outcomes when a transition program has the following characteristics (NCSBN, 2018; Spector, 2015).
- • There includes a preceptorship with the preceptor receiving education for the preceptor role.
- • Program is 9–12 months in length.
- • Program content includes patient safety, clinical reasoning, communication and teamwork, patient-centered care, evidence-based practice, quality improvement, and informatics (Quality and Safety Education for Nurses [QSEN] competencies).
- • New graduates are given time to learn, apply content, obtain feedback, and share their reflections about the transition process.
- • Programs are customized so the new graduates learn specialty content in the areas where they are working.
- • At 6 months, when new graduates typically become more independent, there are an increase in errors, a decrease in job satisfaction, and an increase in work stress (Spector et al., 2015b).
- • At 12 months in practice, work stress and reported errors decrease, and job satisfaction increases; research findings support need for ongoing support during the first year of practice.
- • The 6- to 9-month period of practice is the most vulnerable time for new graduates.
Considering This Information
What can you do to ease your transition process?
In response to the 2010 IOM report, the Robert Wood Johnson Foundation has developed the Initiative on the Future of Nursing (Institute of Medicine of the National Academies, 2011) to address the IOM recommendations for the nursing profession. One recommendation is to implement nurse residency programs for new graduate nurses to acquire skills and develop competency in providing care to today’s complex and diverse health care population. Since the IOM report, state boards of nursing, nursing education programs, and health care institutions have joined together and developed nurse residency programs to prepare the future nurse—that’s you! For additional resources and research on nurse residency programs, check out the mentoring, preceptorship, and nurse residency program chapter (see Chapter 3).
Conclusion
What will be the direction for role transition of graduate nurses? Has your state adopted the TTP model? How will preceptors be selected, and will they be credentialed? As you progress through the chapters in this book, you will find references to the IOM, The Joint Commission, and other health care resources concerned with the safety of patients, the reduction of errors, the economic impact of errors, retention of nurses, and the cost of health care. These are key players and important considerations in the new nurse’s transition to safe nursing practice.
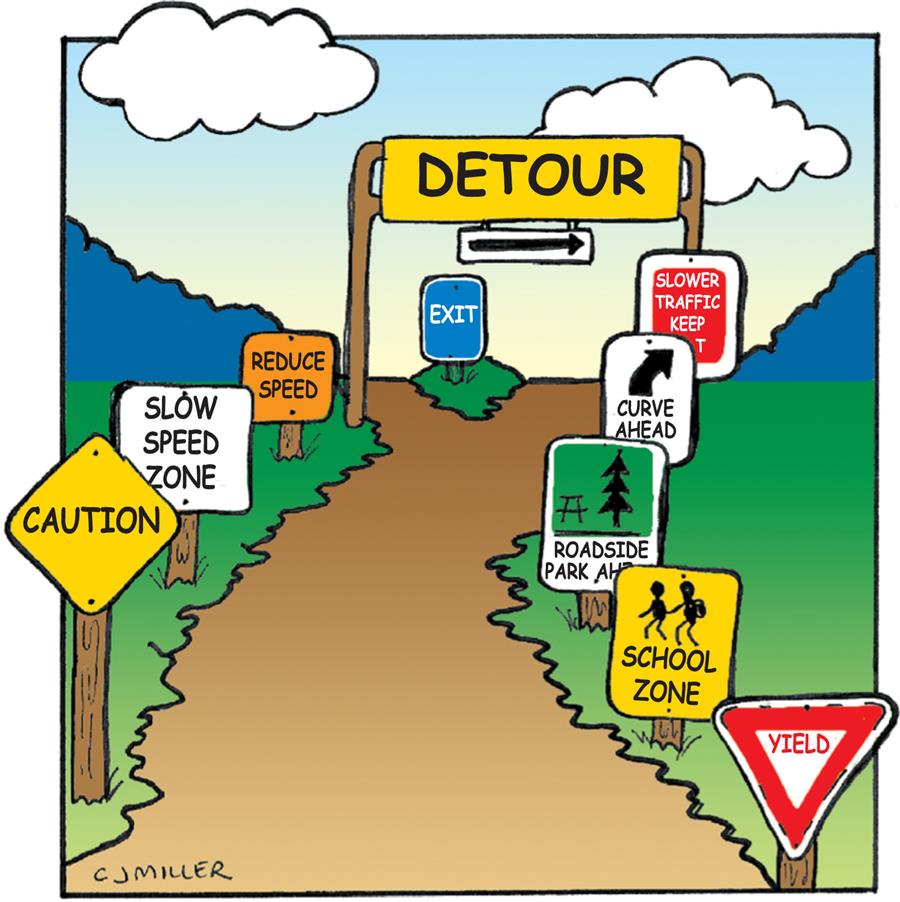
As you progress through your own personal transition into nursing practice, the “rules of the road” for transition can be likened to traffic signs (Fig. 1.3). Check out the following signs that will help you to direct your transition experience. Figure 1.4 gives additional advice from graduates who have successfully made the transition.
 Stop.
Stop.
Take care of yourself. Take time to plan your transition. Get involved with other recent graduates; they can help you. Do not be afraid to ask questions and do not be afraid to ask for help.
 Detour.
Detour.
You will make mistakes. Recognize them, learn from them, and put them in the past as you move forward. Regardless of how well you plan for change, there are always detours ahead. Detours take you on an alternate route. They can be scenic, swampy, or desolate, or they can bog you down in heavy traffic. Do not forget to look for the positive aspects—the detour may open your eyes to new horizons and new career directions.
 Curve Ahead.
Curve Ahead.
Get your personal life in order. Anticipate changes in your schedule. Be adaptable because the transition process is not predictable.
 Yield.
Yield.
You do not always have to be right. Consider alternatives and make compromises within your value system.
 Resume Speed.
Resume Speed.
Maintain a positive attitude. As you gain experience, you will become better organized and begin to really enjoy nursing. Be aware; sometimes as you resume speed, you may be experiencing another role transition as your career moves in a different direction.
 Exit.
Exit.
Pay attention to your road signs; do not take an exit you do not really want. Before you exit your job, critically evaluate the job situation. “Look before you leap” by making sure the change will improve your work situation.
 Slow Traffic; Keep Right.
Slow Traffic; Keep Right.
You may be more comfortable in the slower traffic lane with respect to your career direction. Take all the time you need; it is okay for each person to travel at a different speed. Do not get run over in the fast lane.
 School Zone.
School Zone.
Plan for continuing education, whether it is an advanced degree program or one to maintain your clinical skills or license. Allow yourself sufficient time in your new job before you jump back into the role of full-time student.
 Slow Speed Zone.
Slow Speed Zone.
Take time to get organized before you resume full speed! Have a daily organizational sheet that fits your needs and works for you both in your job and your personal life.
 Caution.
Caution.
Do not commit to anything with which you are not professionally or personally comfortable. Think before you act. Do not react. Do not panic. If in doubt, check with another nurse.
 Roadside Park Ahead.
Roadside Park Ahead.
Take a break, whether it is 15 minutes or 30 minutes a day to indulge yourself or a week to do something you really want to do.
 Relevant Websites and Online Resources
Relevant Websites and Online Resources
Commission on Collegiate Nursing Education (CCNE)
Accredited Nurse Residency Programs. http://www.aacnnursing.org/Portals/42/CCNE/PDF/CCNE-Accredited-Nurse-Residency-Programs.pdf
NCSBN
Transition to Practice. https://www.ncsbn.org/transition-to-practice.htm
NCSBN Learning Extension
Transition to Practice Online Program. https://ww2.learningext.com/newnurses.htm
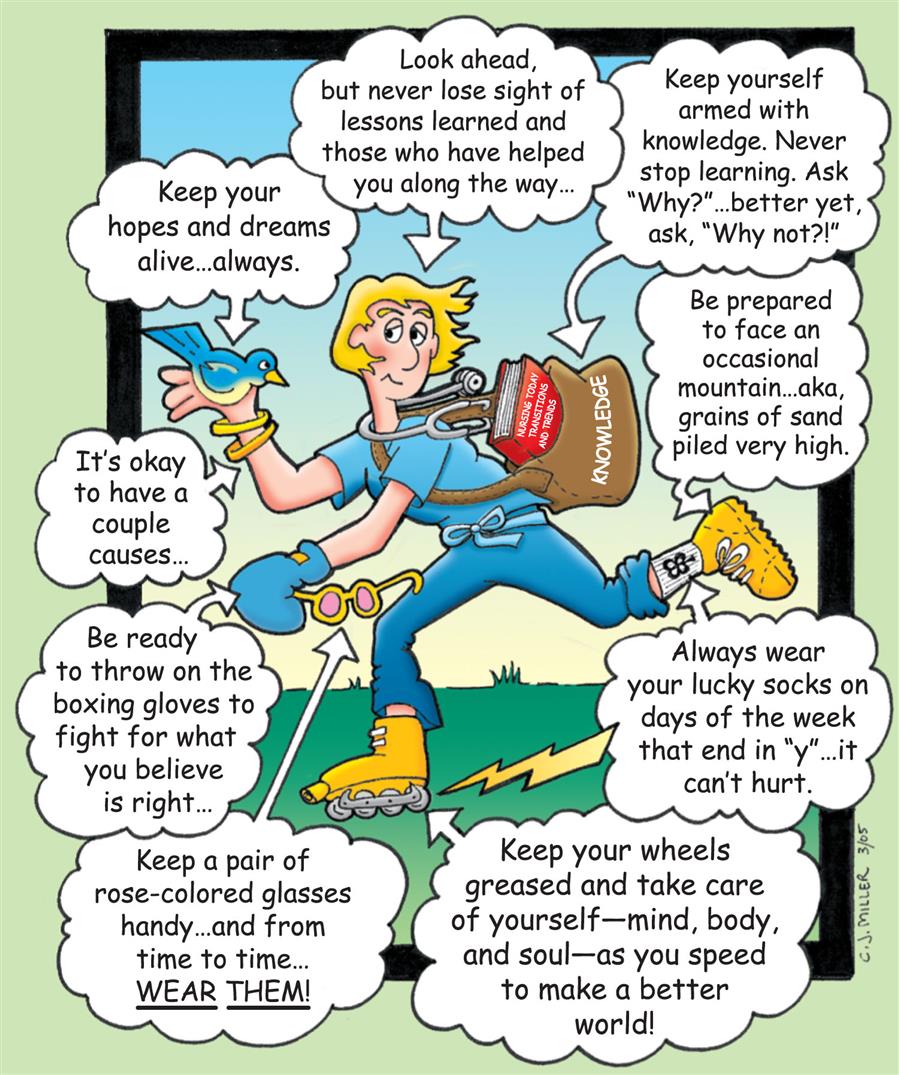
A cartoon shows a woman skating with a bag labeled knowledge and multiple text bubbles read: • Look ahead, but never lose sight of lessons learned and those who have helped you along the way. • Keep yourself armed with knowledge. Never stop learning. Ask why? better yet ask, why not? • Be prepared to face an occasional mountain aka, grains of sand piled very high. • always wear your lucky socks and the days of the week that end in y, it can't hurt. • Keep your wheels greased and take care of yourself including mind, body, and soul as you speed to make a better world. • Keep a pair of coloured glasses handy and from time to time wear them. • Be ready to throw on boxing gloves to fight for what you believe is right. • It’s okay to have a couple causes. • Keep your hopes and dreams alive always.