3: Sinus mechanisms
Learning objectives
After reading this chapter, you should be able to:
- 1. Describe the electrocardiogram (ECG) characteristics of a sinus rhythm.
- 2. Describe the ECG characteristics, possible causes, signs and symptoms, and emergency management of sinus bradycardia.
- 3. Describe the ECG characteristics, possible causes, signs and symptoms, and emergency management of sinus tachycardia.
- 4. Describe the ECG characteristics, possible causes, signs and symptoms, and emergency management of sinus arrhythmia.
- 5. Describe the ECG characteristics, possible causes, signs and symptoms, and emergency management of sinoatrial (SA) block.
- 6. Describe the ECG characteristics, possible causes, signs and symptoms, and emergency management of sinus arrest.
Key terms
sinus arrhythmia: Dysrhythmia originating in the SA node that occurs when the SA node discharges irregularly; sinus arrhythmia is a normal phenomenon associated with the phases of breathing and changes in intrathoracic pressure.
sinus bradycardia: Dysrhythmia originating in the SA node with a ventricular response of less than 60 beats/min.
sinus rhythm: A normal heart rhythm; sometimes called a regular sinus rhythm (RSR) or normal sinus rhythm (NSR).
sinus tachycardia: Dysrhythmia originating in the SA node with a ventricular rate faster than 100 beats per minute (beats/min) with the maximum rate about 220 beats/min, minus the patient’s age in years.
Introduction
In this chapter, you will begin learning the characteristics of specific cardiac rhythms. Study these characteristics carefully and commit them to memory. Throughout this text, all ECG characteristics pertain to adult patients unless otherwise noted.
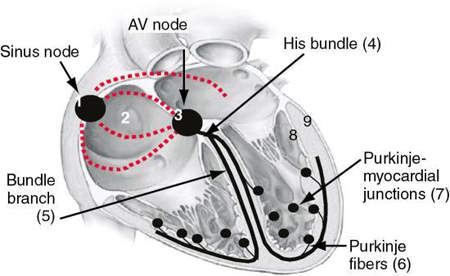
The normal heartbeat results from an electrical impulse that starts in the SA node (Fig. 3.1). Normally, pacemaker cells within the SA node spontaneously depolarize more rapidly than other cardiac cells. As a result, the SA node usually dominates other depolarizing areas at a slightly slower rate. The impulse is sent to transitional cells at the outside edge of the SA node and then to the myocardial cells of the surrounding atrium.
A rhythm that begins in the SA node has the following characteristics:
An electrical impulse that begins in the SA node may be affected by the following:
 ECG Pearl
ECG Pearl
Most, but not all, rhythms that begin in the SA node are regular.
Sinus rhythm
Sinus rhythm is the name given to a normal heart rhythm. Sinus rhythm is sometimes called a regular sinus rhythm (RSR) or normal sinus rhythm (NSR). Sinus rhythm reflects normal electrical activity—that is, the rhythm starts in the SA node and then heads down the normal conduction pathway through the atria, atrioventricular (AV) node and bundle, right and left bundle branches, and Purkinje fibers. In adults and adolescents, the SA node usually fires at a regular rate of 60 to 100 beats per minute (beats/min).
How do I recognize it?
ECG characteristics of a sinus rhythm include the following:
ECG Pearl
Be sure to commit the ECG characteristics of sinus rhythm to memory because the dysrhythmias discussed in this text relate to their similarities and differences compared with sinus rhythm.
Fig. 3.2 shows an example of a sinus rhythm recorded simultaneously in three leads: V1, II, and V5. As you look at this figure from left to right, note the 10-mm calibration marker that appears at the far left of each lead. Although we will focus on lead II as we examine this rhythm strip, you will find that it helps to view waveforms, segments, and intervals in more than one lead.

A sinus rhythm has a regular atrial and ventricular rhythm. Find the QRS complexes on the rhythm strip. Place one point of your calipers or make a mark on a piece of paper at the beginning of an R wave. Place the other point of the calipers or make a second mark on the paper at the beginning of the R wave of the next QRS complex. Without adjusting the calipers, evaluate each succeeding R-R interval. If you are using paper, lift the paper and move it across the rhythm strip. The R-R intervals in this example are regular. Because you have already identified the R waves, determine the ventricular rate. Because the rhythm is regular, calculate the rate using the small box method. There are 19 small boxes between R waves; therefore, the ventricular rate is about 79 beats/min. Remember, the built-in (i.e., intrinsic) rate for a rhythm that begins in the SA node is 60 to 100 beats/min; therefore, the rate of the rhythm in our example fits within the criteria for a sinus rhythm.
Now look to the left of the QRS complexes to find the P waves on the rhythm strip. A rhythm that begins in the SA node should have a positive (i.e., upright) P wave in lead II before each QRS complex (i.e., there should be a 1:1 relationship between P waves and QRS complexes). When you look at this rhythm strip, you can see one upright P wave before each QRS complex. Every P wave looks alike. Measure the P-P interval to see if the P waves occur regularly and then determine the atrial rate. You will find that the P waves occur regularly at a rate of 79 beats/min.
Now measure the PR interval and QRS duration. In a sinus rhythm, the PR interval measures 0.12 to 0.20 second and is constant from beat to beat. In this example, the PR interval is 0.16 second. The QRS complex usually measures 0.11 second or less. If there is a delay in conduction through the bundle branches, the QRS may be wide (i.e., greater than 0.11 second). In our example, the QRS measures between 0.04 and 0.08 second depending on the lead and complex selected for the measurement. Next, determine the QT interval by counting the number of small boxes between the beginning of the QRS complex and the end of the T wave and multiplying that number by 0.04 second. In our example, the QT interval measures about 8.5 boxes (0.34 second). This value is slightly less (shorter) than the normal value of 0.40 to 0.44 second.
Next, locate the TP segment and then the J point. Remember that deviation is measured as the number of millimeters of vertical ST-segment displacement from the J point (O’Gara et al., 2013). You will see that the ST segments in leads II and III of this rhythm strip are elevated. Now interpret the rhythm, specifying the origin (pacemaker site) of the rhythm and the ventricular rate. Because the rhythm shown in Fig. 3.2 fits the ECG criteria for a sinus rhythm, your interpretation should be sinus rhythm at 79 beats/min with ST-segment elevation (STE).
Sinus bradycardia
If the SA node fires at a rate slower than expected for the patient’s age, the rhythm is called sinus bradycardia. The rhythm starts in the SA node and then travels the normal conduction pathway, resulting in atrial and ventricular depolarization. In adults and adolescents, sinus bradycardia has a heart rate of less than 60 beats/min. When seen in heart transplant recipients, bradycardia is sometimes defined as a heart rate that is persistently slower than 70 or 80 beats/min (Kusumoto et al., 2018). The term severe sinus bradycardia is sometimes used to describe sinus bradycardia with a rate of less than 40 beats/min. There is no set rate at which sinus bradycardia can be labeled pathologic (Berger et al., 2016).
How do I recognize it?
ECG characteristics of sinus bradycardia include the following:
Fig. 3.3 is an example of sinus bradycardia. This rhythm’s characteristics are the same as those of a sinus rhythm with one exception—the rate. A sinus rhythm rate is 60 to 100 beats/min; the sinus bradycardia rate is less than 60 beats/min.

Let’s look at this rhythm strip using the same systematic format that you previously used. Begin by locating the QRS complexes on the rhythm strip. Evaluate each succeeding R-R interval. The R-R intervals in this example are regular. Now determine the ventricular rate. In this rhythm strip, the ventricular rate is 40 beats/min. Next, find the P waves on the rhythm strip. Remember that a rhythm that begins in the SA node should have a positive P wave (in lead II) before each QRS complex. In our example, you can see that there is a 1:1 relationship between P waves and QRS complexes, and every P wave looks alike. Now measure the P-to-P interval to see if the P waves occur regularly and determine the atrial rate. The P waves occur regularly at a rate of 40 beats/min. Next, measure the PR interval, QRS duration, and QT interval. In this example, the PR interval is 0.16 second, the QRS complex measures 0.08 second, and the QT interval is 0.40 second. ST-segment depression is present, and negative (i.e., inverted) T waves appear after each QRS complex. These findings must be noted in your final description of the rhythm. Therefore, the correct interpretation of this rhythm would be sinus bradycardia at 40 beats/min with ST-segment depression and inverted T waves.
ECG Pearl
In sinus bradycardia, the QT interval may be longer than expected because of the slower heart rate.
What causes it?
Sinus bradycardia is the most common bradydysrhythmia encountered during sleep (Kusumoto et al., 2018). It is also common in well-conditioned athletes. Prolonged standing and stimulation of the vagus nerve can also result in heart rate slowing. For example, coughing, vomiting, straining to have a bowel movement, or sudden exposure of the face to cold water can slow the heart rate. In people who have a sensitive carotid sinus, heart rate slowing can occur when a tight collar is worn or with the impact of the stream of water on the neck while in the shower. Sinus bradycardia can also occur because of one or more medications a patient is taking. For example, a patient prescribed a beta-blocker for their hypertension may experience bradycardia. Other causes of sinus bradycardia include the following:
What do I do about it?
Remember that cardiac output equals stroke volume × heart rate. Therefore, a decrease in either stroke volume or heart rate may decrease cardiac output. Many patients tolerate a heart rate of 50 to 60 beats/min but become symptomatic when the rate drops below 50 beats/min. A patient with an unusually slow heart rate may complain of dizziness or lightheadedness, fatigue, weakness, or confusion resulting from decreased cerebral blood flow (Sidhu & Marine, 2020). Decreasing cardiac output will eventually produce hemodynamic compromise (Box 3.1).
ECG Pearl
Interventions and treatments discussed in this text assume that an assessment has been performed, the patient’s clinical problem identified, and a physician order has been obtained when indicated. In the out-of-hospital setting, paramedics and nurses typically operate under standing physician orders, local protocols, or both. In the hospital setting, agency policy may permit standing orders to direct patient care when a patient’s condition changes rapidly and requires immediate intervention. When performed by a clinician with appropriate training per that institution’s policy, these orders may include routine therapies, monitoring guidelines, diagnostic procedures, and medication administration. Physician contact is necessary when standing orders or local protocols are unavailable.
If a patient presents with a bradycardia, assess how they are tolerating the rhythm. If the patient has no symptoms, no treatment is necessary. The term symptomatic bradycardia refers to signs and symptoms of hemodynamic compromise related to a slow heart rate. Treatment of symptomatic bradycardia should include assessing the patient’s oxygen saturation level and determining if signs of increased breathing effort are present (e.g., retractions, tachypnea). Give supplemental oxygen if oxygenation is inadequate and assist breathing if ventilation is inadequate. Establish intravenous (IV) access and obtain a 12-lead ECG. Atropine, administered intravenously, is the drug of choice for symptomatic bradycardia. Reassess the patient’s response and continue monitoring the patient.
Suppose symptomatic bradycardia develops because of one or more medications that a patient is taking. In that case, their provider may discontinue the drug and substitute another or reduce the dosage, reevaluate the patient’s symptoms and rhythm, and decide the next steps based on their response. In the setting of an MI, sinus bradycardia is often transient. If the patient has no symptoms, a slow heart rate can be beneficial in a patient who has had an MI because the heart’s demand for oxygen is less when the heart rate is slow.
ECG Pearl
Atropine is a drug used to increase the heart rate in a patient with symptomatic bradycardia. It works by blocking acetylcholine at the endings of the vagus nerves. The vagus nerves innervate the heart at the SA and AV nodes. Thus, atropine is most effective for narrow-QRS bradycardias. Atropine allows increased activity from the autonomic nervous system’s sympathetic division by blocking acetylcholine’s effects. As a result, the rate at which the SA node can fire is increased. Atropine also increases the rate at which an impulse is conducted through the AV node. Areas of the heart that are not innervated or minimally innervated by the vagus nerves (e.g., the ventricles) will not respond to atropine. Transplanted hearts do not usually respond to atropine because they lack vagal nerve innervation.
Sinus tachycardia
If the SA node fires at a rate faster than normal for the patient’s age, the rhythm is called sinus tachycardia. Sinus tachycardia begins and ends gradually. The rhythm starts in the SA node and travels the normal pathway of conduction through the heart, resulting in atrial and ventricular depolarization.
How do I recognize it?
ECG characteristics of sinus tachycardia include the following:
Sinus tachycardia looks much like a sinus rhythm, except that it is faster. It may be hard to tell the difference between a P wave and a T wave at very fast rates. In adults, the ventricular rate associated with sinus tachycardia is faster than 100 beats/min, with the maximum rate of about 220 beats/min, minus the patient’s age in years. The ventricular rate is usually less than 220 beats/min in infants or 180 beats/min in children.
Fig. 3.4 is an example of sinus tachycardia. Let’s look at this rhythm strip more closely. By glancing at the strip from left to right, you can see that the rate is faster than that of a sinus rhythm. Locate the QRS complexes, evaluate the R-R intervals, and then determine the ventricular rate. The R-R intervals in this example are regular, and the ventricular rate is 125 beats/min. The ventricular rate fits within the parameters of sinus tachycardia.

Look at the P waves on the rhythm strip, evaluate the P-P intervals for regularity, and determine the atrial rate. One upright P wave appears before each QRS complex, every P wave looks alike, and the P waves occur regularly at a rate of 125 beats/min. Now measure the PR interval, QRS duration, and QT interval. In this example, the PR interval is 0.16 second, the QRS complex measures 0.06 second, and the QT interval is 0.32 second. (Remember that it is normal for the QT interval to shorten as the heart rate increases). Now interpret the rhythm, noting the ST-segment depression that is present. The correct interpretation is sinus tachycardia at 125 beats/min with ST-segment depression.
What causes it?
Physiologic sinus tachycardia is a normal and transient response to the body’s demand for increased oxygen. The patient is often aware of an increase in heart rate. Some patients complain of palpitations, a racing heart, or a feeling of pounding in their chests. Examples of conditions that can cause sinus tachycardia include the following:
In a patient with coronary artery disease (CAD), sinus tachycardia can cause problems. The heart’s demand for oxygen increases as the heart rate increases. As the heart rate increases, there is less time for the ventricles to fill and less blood for the ventricles to pump out with each contraction, which can lead to decreased cardiac output. Recall that the coronary arteries fill when the ventricles are at rest. Therefore, rapid heart rates decrease the time available for coronary artery filling, decreasing the heart’s blood supply. Chest discomfort can result if the supplies of blood and oxygen to the heart are inadequate. In a patient experiencing an acute MI, sinus tachycardia may be an early warning signal for heart failure, cardiogenic shock, and more serious dysrhythmias.
Whereas sinus tachycardia is an expected physiologic response to increased oxygen demand, inappropriate sinus tachycardia (IST) describes a sinus tachycardia that occurs for no apparent physiologic cause. For example, a person’s heart rate may rapidly increase to more than 100 beats/min with minimal exertion, at rest, or both. Accompanying symptoms are usually nonspecific and include weakness, dizziness, fatigue, headache, shortness of breath, exercise intolerance, lightheadedness, chest discomfort, a racing heart, or palpitations. The mechanisms responsible for IST are not entirely understood, and a diagnosis is made only after other causes for the tachycardia have been ruled out (Yasin et al., 2018).
What do I do about it?
Treatment for physiologic sinus tachycardia is directed at correcting the underlying cause (i.e., fluid replacement, relief of pain, removal of offending medications or substances, reducing fever or anxiety). In a patient experiencing an acute MI, sinus tachycardia may be treated with medications to slow the heart rate and decrease myocardial oxygen demand (e.g., beta-blockers), provided there are no signs of heart failure or other contraindications.
Treatment of IST can be tricky. Lifestyle modifications are usually recommended, including decreasing caffeine and other stimulant intake, exercising regularly, and maintaining adequate hydration. Pharmacologic treatment with beta-blockers or calcium blockers, either alone or in combination, may be tried but are often ineffective, and symptoms can persist despite heart rate control. Ivabradine (Corlanor), a medication usually used to treat heart failure, has proved helpful in treating some IST patients. Surgical ablation may be performed in severe cases.
Some dysrhythmias with very rapid ventricular rates (i.e., above 150 beats/min) require the delivery of medications or a shock to stop the rhythm. However, it is essential to remember that shocking a sinus tachycardia is inappropriate; instead, treat the cause of the tachycardia.
Sinus arrhythmia
As you have seen so far, the SA node fires quite regularly most of the time. When it fires irregularly, the resulting rhythm is called sinus arrhythmia. Sinus arrhythmia begins in the SA node and follows the heart’s normal conduction pathway, resulting in atrial and ventricular depolarization. A sinus arrhythmia usually occurs at a rate of 60 to 100 beats/min. Sinus arrhythmia associated with the phases of breathing and changes in intrathoracic pressure is called respiratory sinus arrhythmia. Sinus arrhythmia unrelated to the ventilatory cycle is called nonrespiratory sinus arrhythmia.
How do I recognize it?
Characteristics of sinus arrhythmia include the following:
Let’s look at the rhythm strip in Fig. 3.5. How does this rhythm differ from the others we have discussed so far? Without using calipers or a piece of paper, you can see that it is irregular. Recognizing that, the rhythm cannot be a sinus rhythm because a sinus rhythm is regular. Because the rhythm is irregular, we will use the 6-second method to calculate the rate, which is 70 beats/min. Looking closely at the rest of the rhythm strip, you can see one upright P wave before each QRS complex. Upon measuring the PR interval, the QRS duration, and the QT interval, you will find that they are within normal limits.

This rhythm strip was obtained from a 39-year-old man who was complaining of “feeling faint.” If we were able to see the patient and watch his ventilatory rate and ECG at the same time, you would see a pattern. The patient’s heart rate increases gradually during inspiration (i.e., the R-R intervals shorten) and decreases with expiration (i.e., the R-R intervals lengthen). We will identify this rhythm as a sinus arrhythmia at 70 beats/min.
What causes it?
Respiratory sinus arrhythmia, which is the most common type of sinus arrhythmia, is a normal phenomenon that occurs with phases of breathing and changes in intrathoracic pressure. The heart rate increases with inspiration (i.e., the R-R intervals shorten) and decreases with expiration (i.e., the R-R intervals lengthen). The changes in rhythm disappear when patients hold their breath. Sinus arrhythmia is most commonly observed in children and young adults.
Nonrespiratory sinus arrhythmia can be seen in people with normal hearts, but it is more likely to be found in older individuals and those with heart disease. It is common after acute inferior wall MI, and it may be seen with increased intracranial pressure. Nonrespiratory sinus arrhythmia may result from the effects of medications (e.g., digitalis, morphine) or carotid sinus pressure.
What do I do about it?
Sinus arrhythmia usually does not require treatment unless accompanied by a slow heart rate that causes hemodynamic compromise. IV atropine may be indicated to treat the bradycardia if hemodynamic compromise is present because of the slow rate.
Sinoatrial block
With SA block, also called sinus exit block, the SA node’s pacemaker cells initiate an impulse, but it is blocked as it exits the SA node, resulting in periodically absent PQRST complexes. SA block is thought to occur because of the failure of the transitional cells in the SA node to conduct the impulse from the pacemaker cells to the surrounding atrium. Thus, SA block is a disorder of impulse conduction.
How do I recognize it?
When an impulse is blocked as it exits the SA node, the atria are not activated. The lack of atrial activation appears on the ECG as a single missed beat (i.e., a P wave, QRS complex, and T wave are missing). The pause caused by the missed beat is the same as, or an exact multiple of, the distance between two P-P intervals of the underlying rhythm. ECG characteristics of SA block include the following:
Let’s look at the example of SA block in Fig. 3.6. As you quickly scan the rhythm strip from left to right, the pause between the third and fourth beats is easily seen. The atrial and ventricular rhythm is irregular because of the pause. The rate is about 60 beats/min using the 6-second method of rate calculation. A positive P wave appears before each QRS complex, and the P waves look alike. The PR interval is 0.16 second and constant from beat to beat. The QRS complex measures 0.06 to 0.08 second, and the QT interval measures 0.32 to 0.36 second, which is within normal limits. Because the P waves are upright and each P wave is associated with a QRS complex, we know that the underlying rhythm came from the SA node. So far, we can identify this rhythm as a sinus rhythm with a ventricular rate of 60 beats/min.

Now we need to figure out what caused the pause between beats 3 and 4. First, look to the left of the pause and examine the waveforms of the beat that comes before the pause. Compare these waveforms with the others in the rhythm strip. It is essential to do this because sometimes waveforms hide on top of other waveforms, distorting their shape. In our example, nothing seems to be amiss. Now use your calipers or paper and plot P waves and R waves from left to right across the strip. When you do this, mark the rhythm strip where the next PQRST cycle should have occurred. You will find that precisely one PQRST cycle is missing. The P-P interval is an exact multiple of the distance between two P-P intervals of the underlying sinus rhythm. Although the SA node’s pace-making cells generated impulses regularly, the SA node’s transitional cells failed to transmit the impulse (as seen between beats 3 and 4). To complete our interpretation of this rhythm, we will explain the pause as an SA block. Putting it all together, we have a sinus rhythm at a rate of 60 beats/min with an episode of SA block.
What causes it?
SA block is rather uncommon. Possible causes of SA block include hypoxia, damage or disease to the SA node from CAD, myocarditis, or acute MI; carotid sinus sensitivity; increased vagal tone on the SA node; and medications (e.g., digitalis, quinidine, procainamide, salicylates). If episodes of SA block are frequent and accompanied by a slow heart rate, the patient may show signs of hemodynamic compromise.
What do I do about it?
Signs and symptoms associated with SA block depend on the number of sinus beats blocked. If the SA block episodes are transient and there are no significant signs or symptoms, the patient is observed. If signs of hemodynamic compromise are present and result from medication toxicity, the offending agents should be withheld. If the SA block episodes are frequent, IV atropine, temporary pacing, or insertion of a permanent pacemaker may be needed.
ECG Pearl
Sick sinus syndrome (SSS), also called sinus node dysfunction, is a dysrhythmia that most commonly affects adults over age 70 years and is usually related to degenerative SA node tissue changes. The effects of medications, inflammatory diseases of the heart, muscular dystrophy, and heart disease are possible causes. On the ECG, SSS can appear as alternating patterns of bradycardia and tachycardia (bradycardia-tachycardia syndrome) or skipped beats caused by episodes of SA block or sinus arrest. Patients may be asymptomatic, have subtle or nonspecific symptoms, or experience syncope, dizziness or lightheadedness, palpitations, or confusion. Chest discomfort, shortness of breath, or fatigue may occur during exercise. Diagnosis of SSS usually requires Holter monitoring or the use of an event recorder. Electrophysiologic testing may be performed if SSS is suspected, and monitoring devices do not capture ECG evidence of it.
Placement of a permanent dual-chamber pacemaker may be necessary to relieve symptoms and restore a regular cardiac rhythm.
Sinus arrest
Sinus arrest, also called sinus pause or SA arrest, is a disorder of impulse formation. With sinus arrest, the SA node’s pacemaker cells do not initiate an electrical impulse for one or more beats, resulting in absent PQRST complexes on the ECG.
When the SA node fails to initiate an impulse, an escape pacemaker site (i.e., the AV junction or the Purkinje fibers) should kick in and assume responsibility for pacing the heart. The term junctional denotes a beat or rhythm originating at the AV junction. Therefore, when the SA node does not fire and an escape pacemaker kicks in, the pause associated with a sinus arrest may be terminated by a junctional or ventricular escape beat. If an escape pacemaker site does not fire, you will see absent PQRST complexes on the ECG.
How do I recognize it?
ECG characteristics of sinus arrest include the following:
An example of sinus arrest is shown in Fig. 3.7. Looking at the rhythm strip from left to right, you can see a period of no electrical activity between the third and fourth beats. Begin analyzing the rhythm strip by determining the atrial and ventricular rhythmicity and rate. The rate is about 60 beats/min using the 6-second rate calculation method because the rhythm is irregular.

You can see a positive P wave in front of each QRS complex. The P waves look alike. The PR interval is 0.20 second and constant from beat to beat. The QRS complex is 0.10 second, and the QT interval is 0.36 second. Because the P waves are upright and each P wave is associated with a QRS complex, we know that the underlying rhythm came from the SA node.
Now let’s try to explain what caused the pause between beats 3 and 4. Look to the left of the pause and examine the waveforms of the beat that comes before the pause. Compare these waveforms with the others in the rhythm strip. There does not appear to be any distortion of the waveforms. Plot P waves and R waves from left to right across the strip using your calipers or paper. When you do this, mark the rhythm strip where the next PQRST cycles should have occurred. You will find that more than one PQRST cycle is missing. Because the SA node periodically failed to produce impulses, the P-P intervals are not exact multiples of other P-P intervals, characteristic of a sinus arrest. To complete our interpretation of this rhythm strip, we must add this explanation for the pause we saw; therefore, our final interpretation is a sinus rhythm at a rate of 60 beats/min with an episode of sinus arrest.
What causes it?
Causes of sinus arrest include damage to or disease of the SA node from CAD, acute MI, or rheumatic disease; carotid sinus pressure, a sudden increase in parasympathetic activity on the SA node, stimulation of the pharynx, obstructive sleep apnea, hypothermia, and effects of medications such as beta-blockers and calcium blockers. Studies have shown that 2-second periods of sinus arrest have been seen during 24-hour ambulatory ECG monitoring in healthy older adults and 3-second periods in long-distance runners (Kusumoto et al., 2018). In addition to sinus bradycardia, SA block and sinus arrest may occasionally occur during sleep (particularly in the young and in conditioned athletes), are usually asymptomatic events, and generally require no intervention (Kusumoto et al., 2018).
What do I do about it?
Signs and symptoms associated with sinus arrest depend on the number of absent sinus beats and the length of the sinus arrest because there is no cardiac output during the period of arrest. Symptoms may occur abruptly and include weakness, lightheadedness, dizziness, or syncope. If the episodes of sinus arrest are transient and there are no significant signs or symptoms, observe the patient. If signs and symptoms result from carotid sinus sensitivity and resultant vagal stimulation, remove tight clothing, if applicable. If hemodynamic compromise is present, IV atropine, temporary pacing, or both may be indicated. If the episodes of sinus arrest are frequent and prolonged (i.e., more than 3 seconds) or a result of SA node disease, permanent pacemaker insertion is generally warranted. A summary of the characteristics of sinus mechanisms can be found in Table 3.1.

| Dysrhythmia | Rhythm | Rate (beats/min) | P Waves (Lead II) | PR Interval | QRS Duration |
|---|---|---|---|---|---|
| Sinus rhythm | R-R and P-P intervals are regular | 60 to 100 | Positive; one precedes each QRS; P waves look alike | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Sinus bradycardia | R-R and P-P intervals are regular | Less than 60 | Positive; one precedes each QRS; P waves look alike | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Sinus tachycardia | R-R and P-P intervals are regular | Faster than 100; maximum rate about 220 minus the patient’s age in years | Positive; one precedes each QRS; P waves look alike | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Sinus arrhythmia | Irregular and often phasic with breathing | Usually 60 to 100 | Positive; one precedes each QRS; P waves look alike | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Sinoatrial (SA) block | Irregular; the pause is the same as, or an exact multiple of, the distance between two other P-P intervals | Usually normal but varies because of the pause | When present, positive in lead II; one precedes each QRS complex; P waves look alike | When present, 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Sinus arrest | Irregular; the pause is of undetermined length, more than one PQRST complex is missing, and it is not the same distance as other P-P intervals | Usually normal but varies because of the pause | When present, positive in lead II; one precedes each QRS complex; P waves look alike | When present, 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
Stop & review
Identify one or more choices that best complete the statement or answer the question.
- 1. Characteristics of rhythms that begin in the SA node include which of the following?
- 2. Which of the following are possible causes of sinus tachycardia?
- 3. A lead II rhythm strip obtained from a 38-year-old woman with difficulty breathing reveals a regular atrial and ventricular rhythm, a ventricular rate of 120 beats/min, an upright P wave before each QRS complex, and a normal PR interval and QRS duration. This rhythm is
- 4. Which of the following dysrhythmias is/are associated with one or more absent PQRST complexes?
- 5. Which of the following is true regarding respiratory sinus arrhythmia?
- a. Every other electrical impulse is blocked as it leaves the SA node.
- b. This rhythm is often associated with heart failure symptoms and dizziness.
- c. This rhythm is typically the result of degenerative changes in SA node tissue.
- d. The rhythm is irregular because the heart rate increases with inspiration and decreases with expiration.
- 6. A 35-year-old man has been experiencing nausea, vomiting, and diarrhea for the past 48 hours. His blood pressure is 112/70 mm Hg. The cardiac monitor reveals a sinus tachycardia at 124 beats/min. Management of this patient’s dysrhythmia should include
- 7. A lead II rhythm strip reveals a regular atrial and ventricular rhythm, a ventricular rate of 46 beats/min, an upright P wave before each QRS complex, a PR interval of 0.16 second, and a QRS duration of 0.08 second. This rhythm is
- 8. SA block is a disorder of ____, whereas sinus arrest is a disorder of ____.
- 9. Differentiating between a P wave and T wave is most likely to be difficult with which of the following rhythms?
Questions 10 through 17 pertain to the following scenario
A 75-year-old man presents with weakness and “feeling lightheaded.” His symptoms began about 30 minutes ago.
- 10. The patient’s blood pressure is 75/40 mm Hg, pulse 44 beats/min, and ventilations 16. A bradycardia is present when the heart rate is less than
- 11. You prepare to apply electrodes and lead wires to the patient for continuous ECG monitoring in lead II. Lead II views the
- 12. You are examining the waveforms on this patient’s ECG. What is the name given to the first negative deflection observed after the P wave?
- 13. As you measure the intervals on this patient’s rhythm strip, you recall that the PR interval’s normal duration is ______ second.
- 14. Analysis of the patient’s ECG reveals ST-segment depression in lead II. The presence of ST-segment depression suggests
- 15. For the ST-segment depression seen in lead II to be considered clinically significant, this finding would also need to be seen in which of the following anatomically contiguous leads?
- 16. Supplemental oxygen is being administered because the patient’s oxygen saturation level was 89% on room air. The patient reports that he continues to feel weak and lightheaded. The cardiac monitor continues to display sinus bradycardia and a second set of vital signs are essentially unchanged. Which of the following statements is true about this patient situation?
- 17. The patient’s symptoms persist, and his vital signs are essentially unchanged. The cardiac monitor shows a sinus bradycardia with ST-segment depression. You should prepare to administer
Short answer

| Dysrhythmia | Rhythm | Rate (beats/min) | P waves |
|---|---|---|---|
| Sinus bradycardia | Regular | Positive; one precedes each QRS; P waves look alike | |
| Sinus tachycardia | |||
| Sinus arrhythmia | Positive; one precedes each QRS; P waves look alike | ||
| SA block | |||
| Sinus arrest |
Sinus mechanisms—practice rhythm strips
- Use the five steps of rhythm interpretation discussed in Chapter 2 to interpret each of the following rhythm strips. All rhythms were recorded in lead II unless otherwise noted.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 20. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 21. Lead I.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 22. This rhythm strip is from a 90-year-old woman with difficulty breathing.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 23. This rhythm strip is from a 73-year-old man complaining of chest pain. He has a history of hypertension and lung disease.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 24. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 25. This rhythm strip is from a 57-year-old man with chest pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 26. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 27. This rhythm strip is from a 4-month-old infant who reportedly ingested an oral pain reliever.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 28. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 29. This rhythm strip is from a 40-year-old man complaining of back pain after jumping from a burning second-floor balcony.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 30. These rhythm strips are from a 44-year-old woman with chest pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 31. This rhythm strip is from a 6-year-old girl complaining of abdominal pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 32. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 33. This rhythm strip is from a 24-year-old woman complaining of weakness and fatigue.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 34. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 35. This rhythm strip is from a 29-year-old woman with a kidney stone.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 36. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 37. This rhythm strip is from a 53-year-old man with chest pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 38. This rhythm strip is from a 62-year-old man complaining of chest pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 39. This rhythm strip is from an 8-month-old infant after a seizure.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 40. This rhythm strip is from a 33-year-old woman complaining of abdominal pain.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 41. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 42. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 43. This rhythm strip is from a 37-year-old asymptomatic man.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 44. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 45. This rhythm strip is from a 44-year-old construction worker with a sudden onset of chest pressure.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 46. This rhythm strip is from an 85-year-old woman complaining of numbness in her legs.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
Stop & review answers
Multiple choice response
- 1. A, B, D, E. A rhythm that begins in the SA node has the following characteristics:
- 2. A, B, C. There are many causes of sinus tachycardia including pain, fever, and exercise. Medications such as calcium blockers, digitalis, beta-blockers, amiodarone, and sotalol, obstructive sleep apnea, and increased intracranial pressure are possible causes of sinus bradycardia.
- 3. C. A sinus tachycardia is differentiated from other rhythms that originate in the SA node by its rate (faster than 100 beats/min; maximum rate about 220 minus the patient’s age in years).
- 4. A, B. Sinus arrest and SA block are associated with one or more absent PQRST complexes.
- 5. D. Respiratory sinus arrhythmia, which is the most common type of sinus arrhythmia, is a normal phenomenon that occurs with phases of breathing and changes in intrathoracic pressure. The heart rate increases with inspiration (i.e., the R-R intervals shorten) and decreases with expiration (i.e., the R-R intervals lengthen). Sinus arrhythmia is most commonly observed in children and young adults.
- 6. C. Based on the information provided, the most likely cause of the patient’s sinus tachycardia is dehydration/hypovolemia, which is best managed by replacing fluids and electrolytes.
- 7. D. A sinus bradycardia’s characteristics are the same as those of a sinus rhythm with one exception—the rate. A sinus rhythm rate is 60 to 100 beats/min; the sinus bradycardia rate is less than 60 beats/min.
- 8. B. With SA block, the SA node’s pacemaker cells initiate an impulse, but it is blocked as it exits the SA node, resulting in periodically absent PQRST complexes. SA block is thought to occur because of the failure of the transitional cells in the SA node to conduct the impulse from the pacemaker cells to the surrounding atrium. Thus, SA block is a disorder of impulse conduction. With sinus arrest, the SA node’s pacemaker cells fail to initiate an electrical impulse for one or more beats, resulting in absent PQRST complexes on the ECG. Thus, sinus arrest is a disorder of impulse formation.
- 9. C. With sinus tachycardia, it may be hard to tell the difference between a P wave and a T wave at very fast rates.
- 10. A. In adults, a bradycardia exists if the rate is less than 60 beats/min.
- 11. B. Lead II views the inferior surface of the left ventricle.
- 12. A. A QRS complex normally follows each P wave. The QRS complex begins as a downward deflection, the Q wave, and represents depolarization of the interventricular septum.
- 13. C. The PR interval changes with heart rate but typically measures 0.12 to 0.20 second in adults. As the heart rate increases, the duration of the PR interval shortens. A PR interval is considered short if it is less than 0.12 second and long if it is more than 0.20 second.
- 14. B. ST-segment depression of 0.5 mm or more in a patient experiencing an acute coronary syndrome is suggestive of myocardial ischemia.
- 15. D. For the ST-segment depression seen in lead II to be considered clinically significant, this finding would also need to be seen in lead III or aVF. Leads II, III, and aVF view the inferior wall of the left ventricle.
- 16. B, C, D. The term symptomatic bradycardia is used to describe a patient who experiences signs and symptoms of hemodynamic compromise related to a slow heart rate. Because this patient is complaining of weakness and lightheadedness and is hypotensive, he is clearly symptomatic with his slow heart rate. Treatment of symptomatic bradycardia should include applying a pulse oximeter and administering supplemental oxygen if indicated, which have already been done. Next, establish IV access and obtain a 12-lead ECG.
- 17. A. Atropine, administered intravenously, is the drug of choice for symptomatic bradycardia. Reassess the patient’s response to the therapeutic interventions provided and continue monitoring the patient. Adenosine is used to slow the ventricular rate. Atenolol, a beta-blocker, would further slow the heart rate. Although amiodarone is an antiarrhythmic used to treat many atrial and ventricular dysrhythmias, it is not used to treat a sinus bradycardia.
Short answer

| Dysrhythmia | Rhythm | Rate (beats/min) | P Waves |
|---|---|---|---|
| Sinus bradycardia | Regular | Less than 60 | Positive; one precedes each QRS; P waves look alike |
| Sinus tachycardia | Regular | Faster than 100; maximum rate about 220 minus the patient’s age in years | Positive; one precedes each QRS; P waves look alike |
| Sinus arrhythmia | Irregular and often phasic with breathing | Usually 60 to 100 | Positive; one precedes each QRS; P waves look alike |
| SA block | Irregular; the pause is the same as, or an exact multiple of, the distance between two other P-P intervals | Usually normal but varies because of the pause | When present, positive in lead II; one precedes each QRS complex; P waves look alike |
| Sinus arrest | Irregular; the pause is of undetermined length, more than one PQRST complex is missing, and it is not the same distance as other P-P intervals | Usually normal but varies because of the pause | When present, positive in lead II; one precedes each QRS complex; P waves look alike |
Sinus mechanisms—practice rhythm strip answers
Note: The rate and interval measurements provided here were obtained using electronic calipers.
- 19. Fig. 3.8
- 20. Fig. 3.9
- 21. Fig. 3.10
- 22. Fig. 3.11
- 23. Fig. 3.12
- Rhythm: Regular
- Rate: 44 beats/min
- P waves: Positive; one precedes each QRS
- PR interval: 0.16 second
- QRS duration: 0.06 second
- QT interval: 0.38 to 0.40 second
- Interpretation: Sinus bradycardia at 44 beats/min, ST-segment depression, baseline artifact is present. Note the upright U waves after each T wave.
- 24. Fig. 3.13
- Rhythm: Irregular
- Rate: 68 to 76 beats/min
- P waves: When present, positive; one precedes each QRS
- PR interval: 0.16 second
- QRS duration: 0.08 second
- QT interval: 0.44 second
- Interpretation: Sinus rhythm at 76 beats/min with an episode of sinus arrest and return to sinus rhythm at 68 beats/min; tall T waves
- 25. Fig. 3.14
- 26. Fig. 3.15
- 27. Fig. 3.16
- 28. Fig. 3.17
- 29. Fig. 3.18
- 30. Fig. 3.19
- 31. Fig. 3.20
- 32. Fig. 3.21
- 33. Fig. 3.22
- 34. Fig. 3.23
- 35. Fig. 3.24
- 36. Fig. 3.25
- 37. Fig. 3.26
- 38. Fig. 3.27
- 39. Fig. 3.28
- 40. Fig. 3.29
- 41. Fig. 3.30
- Rhythm: Regular
- Rate: 68 beats/min
- P waves: Positive; one precedes each QRS
- PR interval: 0.28 to 0.30 second
- QRS duration: 0.06 to 0.08 second
- QT interval: 0.41 second
- Interpretation: Sinus rhythm at 68 beats/min with a prolonged PR interval and ST-segment depression; some baseline artifact is present
- 42. Fig. 3.31
- 43. Fig. 3.32
- 44. Fig. 3.33
- 45. Fig. 3.34
- 46. Fig. 3.35
References
Berger M.G, Rubenstein J.C. & Roth J.A. Cardiac arrhythmias Andreoli & Carpenter’s Cecil essentials of medicine 9th ed. 2016; Saunders Philadelphia, PA 110-135.
Kusumoto F.M, Schoenfeld M.H, Barrett C, Edgerton J.R, Ellenbogen K.A, Gold M.R. & Varosy P.D. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay Circulation 8, 2018;140: e382-e482.
O’Gara P.T, Kushner F.G, Ascheim D.D, Casey D.E, Jr.Chung M.K, de Lemos J.A. &. Zhao D.X. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction J Am Coll Cardiol 4, 2013;61: e78-e140.
Olshansky B. & Sullivan R.M. Inappropriate sinus tachycardia Europace 2, 2019;21: 194-207.
Sidhu S. & Marine J.E. Evaluating and managing bradycardia Trends Cardiovasc Med 5, 2020;30: 265-272.
Yasin O.Z, Vaidya V.R, Chacko S.R. & Asirvatham S.J. Inappropriate sinus tachycardia: current challenges and future directions J Innov Cardiac Rhythm Manage 7, 2018;9: 3239-3243.