5: Junctional rhythms
Learning objectives
After reading this chapter, you should be able to:
- 1. Describe the electrocardiogram (ECG) characteristics, possible causes, signs and symptoms, and initial emergency care for premature junctional complexes (PJCs).
- 2. Describe the ECG characteristics and possible causes for junctional escape beats.
- 3. Explain the difference between PJCs and junctional escape beats.
- 4. Describe the ECG characteristics, possible causes, signs and symptoms, and initial emergency care for a junctional escape rhythm.
- 5. Describe the ECG characteristics, possible causes, signs and symptoms, and initial emergency care for an accelerated junctional rhythm.
- 6. Describe the ECG characteristics, possible causes, signs and symptoms, and initial emergency care for junctional tachycardia.
Key terms
accelerated junctional rhythm: Dysrhythmia originating in the atrioventricular (AV) bundle with a rate between 61 and 100 beats per minute (beats/min).
junctional bradycardia: A rhythm that begins in the AV bundle with a rate of less than 40 beats/min.
junctional escape rhythm: A rhythm that begins in the AV bundle; characterized by a very regular ventricular rate of 40 to 60 beats/min.
junctional tachycardia: A rhythm that begins in the AV bundle with a ventricular rate of more than 100 beats/min.
retrograde: Moving backward; moving in the opposite direction to that which is considered normal.
Introduction
The atrioventricular (AV) node is a group of specialized cells located in the lower part of the right atrium above the base of the tricuspid valve (Fig. 5.1). The AV node’s main job is to delay an electrical impulse, allowing the atria to contract and complete filling of the ventricles with blood before the next ventricular contraction.
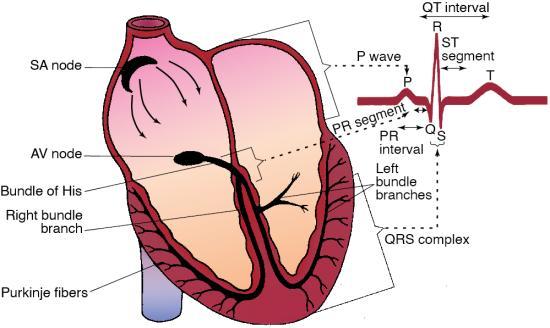
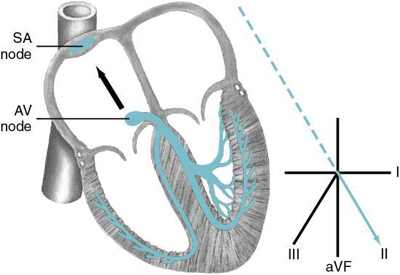
After passing through the AV node, the electrical impulse enters the bundle of His. The bundle of His, also called the common bundle or the AV bundle, is located in the upper part of the interventricular septum. It connects the AV node with the right and left bundle branches. The bundle of His has pacemaker cells capable of discharging at a rhythmic rate of 40 to 60 beats/min. The AV node and the nonbranching portion of the bundle of His are called the AV junction (Fig. 5.2). The bundle of His conducts the electrical impulse to the bundle branches.

Remember that the sinoatrial (SA) node is usually the heart’s pacemaker. The AV junction may assume responsibility for pacing the heart if:
- • The SA node fails to discharge (e.g., sinus arrest).
- • An SA node impulse is generated but blocked as it exits the SA node (e.g., SA block).
- • The rate of discharge of the SA node is slower than that of the AV junction (e.g., sinus bradycardia or the slower phase of a sinus arrhythmia).
- • An impulse from the SA node is generated and is conducted through the atria but is not conducted to the ventricles (e.g., an AV block).
Rhythms that begin in the AV junction used to be called nodal rhythms until electrophysiologic studies proved the AV node does not contain pacemaker cells. The cells nearest the bundle of His are actually responsible for secondary pacing function. Rhythms originating from the AV junction are now called junctional dysrhythmias.
If the AV junction paces the heart, the electrical impulse must travel backward (retrograde) to activate the atria. If a P wave is seen, it will be inverted in leads II, III, and aVF because the impulse is traveling away from the positive electrode (Fig. 5.3). If the atria depolarize before the ventricles, an inverted P wave will be seen before the QRS complex, and the PR interval will usually measure 0.12 second or less (Fig. 5.4). The PR interval is shorter than usual because an impulse that begins in the AV junction does not have to travel as far to stimulate the ventricles. If the atria and ventricles depolarize at the same time, a P wave will not be visible because it will be hidden in the QRS complex. When the atria are depolarized after the ventricles, the P wave typically distorts the end of the QRS complex, and an inverted P wave will appear after the QRS. The QRS duration associated with a rhythm that begins in the AV junction measures 0.11 second or less if conduction through the bundle branches, Purkinje fibers, and ventricles is normal.

 ECG Pearl
ECG Pearl
P waves are usually positive (i.e., upright) in lead I. Inverted P waves may be seen in some, all, or none of the chest leads.
Premature junctional complexes
How do I recognize them?
ECG characteristics of PJCs include the following:
| Rhythm: | Irregular because of the premature beats |
| Rate: | Usually within normal range but depends on underlying rhythm |
| P waves: | May occur before, during, or after the QRS; if visible, the P wave is inverted in leads II, III, and aVF |
| PR interval: | If a P wave occurs before the QRS, the PR interval will usually be 0.12 second or less; if no P wave occurs before the QRS, there will be no PR interval |
| QRS duration: | 0.11 second or less unless abnormally conducted |
A PJC occurs when an irritable site (i.e., focus) within the AV junction fires before the next SA node impulse is ready to fire, interrupting the underlying rhythm. Because the impulse is conducted through the ventricles in the usual manner, the QRS complex will usually measure 0.11 second or less. PJCs are sometimes called premature junctional extrasystoles. A noncompensatory (incomplete) pause often follows a PJC. This pause represents the delay during which the SA node resets its rhythm for the next beat. PJCs may occur in patterns—couplets, bigeminy, trigeminy, and quadrigeminy.
ECG Pearl
You can usually tell the difference between a PAC and a PJC by the P wave. A PAC typically has an upright P wave before the QRS complex in leads II, III, and aVF. A P wave may or may not be present with a PJC. If a P wave is present, it is inverted (retrograde) and may precede or follow the QRS. PJCs can be misdiagnosed when the P wave of a PAC is buried in the preceding T wave.
Junctional complexes may come early or late (i.e., before or after the next expected beat of the underlying rhythm). If the complex is early, it is called a premature junctional complex. If the complex is late, it is called a junctional escape beat. To determine if a complex is early or late, we need to see at least two beats in a row of the underlying rhythm to establish its regularity.
Let’s look at Fig. 5.5. Looking at the overall rhythm, it appears to be irregular. Because the rhythm is irregular, we estimate the rate using the 6-second method of rate calculation at 140 beats/min. All QRS complexes appear to be narrow, so we assume that all impulses started from above the ventricles. Using a pen or pencil, mark an “S” for SA node above each normal-looking P wave. Mark a “J” for junctional above those P waves that are inverted or absent. When you are finished, you should have a “J” marked over the P waves in beats 2, 5, 8, and 11. The rest of the P waves should be marked with an “S.” Now take your calipers or a piece of paper and mark the third and fourth complexes in Fig. 5.5. We already determined that these complexes came from the SA node. These beats reflect the underlying rhythm. We now know that the underlying rhythm is a sinus tachycardia at about 140 beats/min. Now move your calipers or paper to the right. If beat 5 occurred on time (i.e., when the next sinus beat was expected), it would line up with your calipers or paper. The fifth complex is early; it occurred before the next expected sinus beat; therefore, this complex is a PJC. The other beats that have an inverted P wave before the QRS are also PJCs.

A PJC is not an entire rhythm; rather, it is a single beat. When identifying a rhythm, be sure to specify the underlying rhythm and the origin of the ectopic beat(s). In this rhythm strip, we found that the underlying rhythm was a sinus tachycardia at about 140 beats/min. All of the ectopic beats were early and came from the AV junction; therefore, we interpret this rhythm strip as sinus tachycardia at 140 beats/min with frequent PJCs.
What causes them?
PJCs are less common than either PACs or PVCs. Causes of PJCs are shown in Box 5.1.
What do I do about them?
PJCs do not generally require treatment because most individuals who have PJCs are asymptomatic. However, PJCs may lead to symptoms of palpitations or the feeling of skipped beats. Lightheadedness, dizziness, and other signs of decreased cardiac output can occur if PJCs are frequent. If PJCs occur because of ingestion of stimulants or digitalis toxicity, these substances should be withheld.
ECG Pearl
Keep in mind that inverted P waves are normal in lead V1. To determine if a beat or rhythm came from the AV junction using this lead, look for a short PR interval. Use lead II, III, or aVF to confirm your findings.
Junctional escape beats or rhythm
How do I recognize it?
A junctional escape beat begins in the AV junction and appears late (i.e., after the next expected beat of the underlying rhythm). The ECG characteristics of junctional escape beats include the following:
| Rhythm: | Irregular because of late beats |
| Rate: | Usually within normal range but depends on underlying rhythm |
| P waves: | May occur before, during, or after the QRS; if visible, the P wave is inverted in leads II, III, and aVF |
| PR interval: | If a P wave occurs before the QRS, the PR interval will usually be 0.12 second or less; if no P wave occurs before the QRS, there will be no PR interval |
| QRS duration: | 0.11 second or less unless abnormally conducted |
Junctional escape beats frequently occur during episodes of sinus arrest or follow pauses of nonconducted PACs. Look at Fig. 5.6. Looking at the rhythm strip, you can see that the rhythm is irregular. There are three normal-looking beats on the left and two more on the far right. In the center of the strip is an odd-looking beat that appears in the middle of a long pause between beats 3 and 5. Looking more closely at beats 1, 2, 3, 5, and 6, you can see an upright P wave before each QRS complex. These beats came from the SA node. Based on this information, we know that the underlying rhythm is sinus in origin. Using your calipers or a piece of paper, mark the first and second complexes. When you move the calipers or paper to the right, you can see that beat 4 came late—that is, after the next expected sinus beat.

Now let’s try to figure out where beat 4 came from and why. If you put your finger over beat 4, can you explain what happened? The long pause between beats 3 and 5 is an episode of sinus arrest. Remember that if the SA node fails to initiate an impulse, an escape pacemaker site (i.e., the AV junction or ventricles) should assume responsibility for pacing the heart. Look closely at beat 4. The QRS complex is narrow, and there is no P wave before the QRS complex. The narrow QRS complex and absence of a positive P wave before the QRS complex tell us the beat came from the AV junction. Because the beat is late, it is a junctional escape beat. If beat 4 had been early, we would call it a PJC. What happened here? The SA node fired in beats 1, 2, and 3. When the sinus did not fire again when it should have, the AV junction kicked in and fired. Thus, a junctional escape beat is protective—preventing cardiac standstill. Two sinus beats follow this beat. Complete identification of the events in this rhythm strip would be as follows: Sinus rhythm at 60 beats/min with an episode of sinus arrest and a junctional escape beat.
ECG Pearl
Junctional escape beats and rhythms occur when the SA node fails to pace the heart or AV conduction fails.
A junctional rhythm is several sequential junctional escape beats. The terms junctional rhythm and junctional escape rhythm are used interchangeably. Remember that the intrinsic rate of the AV junction is 40 to 60 beats/min. Because a junctional rhythm starts from above the ventricles, the QRS complex is usually narrow, and its rhythm is very regular. The ECG characteristics of a junctional rhythm include the following:
| Rhythm: | Very regular |
| Rate: | 40 to 60 beats/min |
| P waves: | May occur before, during, or after the QRS; if visible, the P wave is inverted in leads II, III, and aVF |
| PR interval: | If a P wave occurs before the QRS, the PR interval will usually be 0.12 second or less; if no P wave occurs before the QRS, there will be no PR interval |
| QRS duration: | 0.11 second or less unless abnormally conducted |
If the AV junction paces the heart at a rate slower than 40 beats/min, the resulting rhythm is called junctional bradycardia. This terminology may seem confusing because the AV junction’s normal pacing rate of 40 to 60 beats/min is bradycardic. However, the term junctional bradycardia refers to a rate slower than expected for the AV junction. A junctional rhythm is shown in Fig. 5.7.

What causes it?
Junctional escape beats frequently occur during episodes of sinus arrest or after pauses of nonconducted PACs. Junctional escape beats may also be observed in healthy individuals during sinus bradycardia. Causes of a junctional rhythm appear in Box 5.2.
What do I do about it?
Patients may be asymptomatic with a junctional escape rhythm, or they may experience signs and symptoms associated with the slow heart rate and decreased cardiac output. Signs and symptoms may include lightheadedness, weakness, chest pain or pressure, syncope, altered mental status, effort intolerance, and hypotension. If the patient is experiencing symptoms, try to determine their frequency, timing, duration, severity, longevity, circumstances, triggers, and alleviating factors. Be sure to ask about any prescribed and over-the-counter medications (including herbal supplements) that the patient may be taking because these agents can cause or worsen a bradycardia.
Treatment depends on the cause of the dysrhythmia, the patient’s presenting signs and symptoms, and the frequency and severity of those symptoms. Patients who experience frequent symptoms may be asked to undergo continuous ambulatory ECG monitoring to determine if a dysrhythmia is a precipitating cause. Laboratory tests (e.g., electrolytes, thyroid function) may be ordered to help identify the cause of the dysrhythmia.
If a junctional rhythm results from the effects of a medication that slows the sinus rate, the medication should be withheld to allow the SA node to resume its pacing function. When a patient experiences serious signs and symptoms related to a slow heart rate, treatment should include applying a pulse oximeter, administering supplemental oxygen (if indicated), establishing intravenous (IV) access, and obtaining a 12-lead ECG. Atropine, given IV, is the first medication given for symptomatic bradycardia (Kusumoto et al., 2018). Reassess the patient’s response and continue monitoring. Implantation of a permanent pacemaker may be necessary if the patient is symptomatic and the junctional rhythm is the result of sinus node dysfunction.
Accelerated junctional rhythm
How do I recognize it?
If the AV junction speeds up and fires at 61 to 100 beats/min, the resulting rhythm is called an accelerated junctional rhythm. This rhythm is caused by altered automaticity of the bundle of His. The only ECG difference between a junctional rhythm and an accelerated junctional rhythm is the increase in the ventricular rate. An example of an accelerated junctional rhythm is shown in Fig. 5.8. The ECG characteristics of this rhythm include the following:
| Rhythm: | Very regular |
| Rate: | 61 to 100 beats/min |
| P waves: | May occur before, during, or after the QRS; if visible, the P wave is inverted in leads II, III, and aVF |
| PR interval: | If a P wave occurs before the QRS, the PR interval will usually be 0.12 second or less; if no P wave occurs before the QRS, there will be no PR interval |
| QRS duration: | 0.11 second or less unless abnormally conducted |

What causes it?
An accelerated junctional rhythm is associated with altered automaticity or triggered activity (Page et al., 2016). Causes of this dysrhythmia include acute MI, cardiac surgery, chronic obstructive pulmonary disease, digitalis toxicity, hypokalemia, and rheumatic fever. It may also be observed transiently after ablation for AV nodal reentrant tachycardia.
What do I do about it?
The patient is usually asymptomatic because the ventricular rate is 61 to 100 beats/min; however, the patient should be monitored closely. If the patient is symptomatic, treatment is focused on addressing the underlying cause of the dysrhythmia. For example, if the rhythm is caused by digitalis toxicity, this medication should be withheld.
Junctional tachycardia
How do I recognize it?
Junctional tachycardia is an ectopic rhythm that begins in the pacemaker cells found in the bundle of His. A junctional tachycardia exists when three or more sequential PJCs occur at a rate of more than 100 beats/min. ECG characteristics of junctional tachycardia include the following:
| Rhythm: | Ventricular rhythm usually regular, but may be irregular |
| Rate: | 101 to 220 beats/min |
| P waves: | May occur before, during, or after the QRS; if visible, the P wave is inverted in leads II, III, and aVF |
| PR interval: | If a P wave occurs before the QRS, the PR interval will usually be 0.12 second or less; if no P wave occurs before the QRS, there will be no PR interval |
| QRS duration: | 0.11 second or less unless abnormally conducted |
Junctional tachycardias are usually regular but may be irregular with variable conduction to the atria (Page et al., 2016). Nonparoxysmal (i.e., gradual onset) junctional tachycardia is a benign dysrhythmia that is usually associated with a gradual increase in rate (i.e., a warm-up pattern) to more than 100 beats/min; it rarely exceeds 120 beats/min (Zimetbaum, 2020). Paroxysmal junctional tachycardia, which is also known as focal or automatic junctional tachycardia, is an uncommon dysrhythmia that starts and ends suddenly and is often precipitated by a PJC. The ventricular rate for paroxysmal junctional tachycardia is generally faster, at a rate of 140 beats/min or more. When the ventricular rate is faster than 150 beats/min, it is challenging to distinguish junctional tachycardia from other supraventricular tachycardias. An example of junctional tachycardia is shown in Fig. 5.9.
What causes it?
Junctional tachycardia is caused by a disorder of impulse formation (i.e., automaticity) (Miller et al., 2019). It is uncommon in adults but may occur because of an acute coronary syndrome, digitalis toxicity, heart failure, or theophylline administration. Junctional tachycardia is more often seen in infants after cardiac surgery for congenital heart disease (Page et al., 2016).
What do I do about it?
Patients experiencing a junctional tachycardia may be asymptomatic. With sustained ventricular rates of 150 beats/min or more, the patient may complain of fatigue, palpitations, or chest discomfort or may experience syncope. Because of the fast ventricular rate, the ventricles may be unable to fill completely, resulting in decreased cardiac output. The more rapid the rate, the greater the incidence of symptoms because of increased myocardial oxygen demand. Junctional tachycardia associated with an acute coronary syndrome may do the following:
Treatment depends on the severity of the patient’s signs and symptoms, and expert consultation is advised. If the patient tolerates the rhythm, observation is often all that is needed. If the patient is symptomatic because of the rapid rate, initial treatment should include applying a pulse oximeter, administering supplemental oxygen (if indicated), establishing IV access, and obtaining a 12-lead ECG. Because it is often difficult to distinguish junctional tachycardia from other narrow-QRS tachycardias, vagal maneuvers and, if necessary, IV adenosine may be ordered to help determine the origin of the rhythm. If the rhythm is the result of digitalis toxicity, the medication should be withheld. If the rhythm is the result of theophylline administration, the infusion should be slowed or stopped. A beta-blocker (e.g., propranolol) or calcium blocker (e.g., diltiazem, verapamil) may be ordered (if no contraindications exist) to slow conduction through the AV node and thereby slow the ventricular rate. Synchronized cardioversion is not indicated for junctional tachycardia because it typically recurs within seconds after the shock, and a release of endogenous catecholamines following the shock can worsen the dysrhythmia (Miller et al., 2019). A summary of junctional rhythm characteristics appears in Table 5.1.
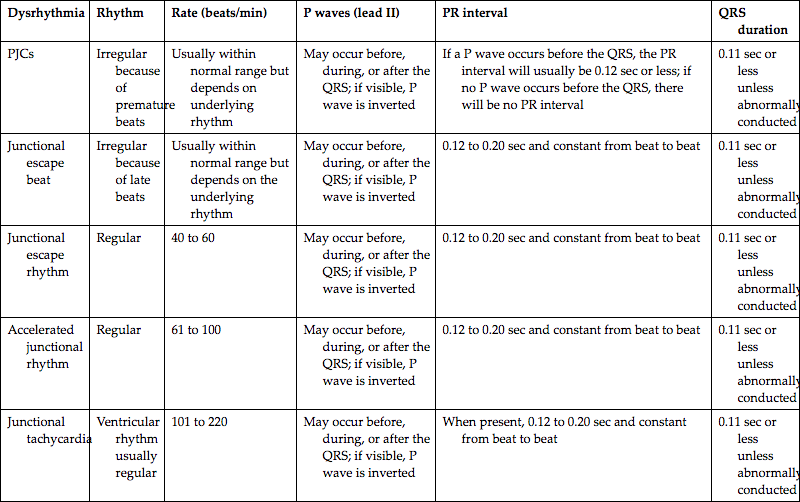
| Dysrhythmia | Rhythm | Rate (beats/min) | P waves (lead II) | PR interval | QRS duration |
| PJCs | Irregular because of premature beats | Usually within normal range but depends on underlying rhythm | May occur before, during, or after the QRS; if visible, P wave is inverted | If a P wave occurs before the QRS, the PR interval will usually be 0.12 sec or less; if no P wave occurs before the QRS, there will be no PR interval | 0.11 sec or less unless abnormally conducted |
| Junctional escape beat | Irregular because of late beats | Usually within normal range but depends on the underlying rhythm | May occur before, during, or after the QRS; if visible, P wave is inverted | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Junctional escape rhythm | Regular | 40 to 60 | May occur before, during, or after the QRS; if visible, P wave is inverted | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Accelerated junctional rhythm | Regular | 61 to 100 | May occur before, during, or after the QRS; if visible, P wave is inverted | 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
| Junctional tachycardia | Ventricular rhythm usually regular | 101 to 220 | May occur before, during, or after the QRS; if visible, P wave is inverted | When present, 0.12 to 0.20 sec and constant from beat to beat | 0.11 sec or less unless abnormally conducted |
Stop & review
Identify one or more choices that best complete the statement or answer the question.
- 1. Select the correct statements about PJCs.
- a. A noncompensatory (incomplete) pause often follows a PJC.
- b. Unlike premature atrial complexes, PJCs do not occur in patterns.
- c. If seen, the P wave of a PJC is negative and may appear before or after the QRS complex.
- d. A PJC begins within the AV junction and appears earlier than the next expected beat of the underlying rhythm.
- 2. An accelerated junctional rhythm is identified by a regular ventricular response occurring at a rate of
- 3. The term junctional bradycardia is used to describe a rhythm that is junctional in origin with
- 4. When viewing a junctional rhythm in lead II, where is the P wave location on the ECG if ventricular depolarization precedes atrial depolarization?
- 5. In rhythms originating from the AV junction, the QRS duration is typically _____ or less unless an intraventricular conduction delay exists.
- 6. Select the correct statements regarding junctional dysrhythmias.
- a. The intrinsic rate of the AV junction is 40 to 60 beats/min.
- b. Junctional dysrhythmias may be seen in acute coronary syndromes.
- c. An accelerated junctional rhythm is a potentially life-threatening dysrhythmia.
- d. The ventricular rhythm associated with junctional dysrhythmias is usually very regular.
- 7. The primary waveform used to differentiate PJCs from PACs is the
Questions 8—10 pertain to the following scenario
A 63-year-old man is complaining of dizziness that began about 45 minutes ago while cleaning his garage. Because the patient’s oxygen saturation level on room air was 88%, supplemental oxygen is being administered. The cardiac monitor has been applied, revealing the rhythm in Fig. 5.10. A coworker is attempting to establish intravenous access.
- 8. Which of the following statements are true about this patient’s cardiac rhythm?
- 9. The rhythm shown on the cardiac monitor is
- 10. The patient’s blood pressure is 82/50 mm Hg, ventilations 16. He states his normal blood pressure is about 130/80 mm Hg. The patient denies chest discomfort and states that he takes no prescription medications. His skin is cool, pink, and moist, and his breath sounds are clear. Intravenous access has been successfully established. Based on the information provided, which of the following statements is true regarding this patient situation?
- a. Because the patient is symptomatic with this rhythm, a vagal maneuver should be attempted.
- b. The patient is symptomatic with this rhythm. Obtain a 12-lead ECG and then administer atropine IV.
- c. Therapeutic interventions are not indicated because there is no evidence of ST-segment elevation on the cardiac monitor.
- d. Although the patient is complaining of dizziness, this symptom does not warrant any further intervention other than cardiac monitoring at this time.

Junctional rhythms—practice rhythm strips
Use the five steps of rhythm interpretation to interpret each of the following rhythm strips. All rhythms were recorded in lead II unless otherwise noted.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 12. Identify the rhythm (lead III).

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 13. This rhythm strip is from a 74-year-old woman with chest pain. She rates her pain 9/10.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 14. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 15. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 16. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 17. This rhythm strip is from an 80-year-old woman who states, “The room is spinning.”

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 18. This rhythm strip is from an 88-year-old woman who experienced a syncopal episode. Her medical history includes a myocardial infarction 9 years ago, a stroke 5 years ago, hypertension, and diabetes.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 19. This rhythm strip is from a 72-year-old man presenting with left-sided weakness. He has a history of a brain tumor.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 20. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 21. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 22. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 23. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 24. This rhythm strip is from a 43-year-old woman who was complaining of palpitations. The patient had a history of supraventricular tachycardia and stated that she could not tolerate adenosine.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 25. This rhythm strip is from a 43-year-old man after a seizure.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 26. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 27. This rhythm strip is from a 96-year-old man experiencing chest pain and palpitations.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 28. This rhythm strip is from a 79-year-old man complaining of palpitations. His initial blood pressure was 112/84 mm Hg. His second blood pressure, 8 minutes after the first, was 78/P mm Hg.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 29. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 30. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 31. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 32. This rhythm strip (lead I) is from a 51-year-old man found unresponsive. He has a history of esophageal varices and gastrointestinal bleeding.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 33. Identify the rhythm.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 34. This rhythm strip is from a 75-year-old man complaining of chest pain that has been present for 20 minutes. He rates his pain 8/10.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
- 35. This rhythm strip is from a 76-year-old woman complaining of weakness.

-
- Rhythm: __________________________ Rate: __________________________ P waves: _________________________
- PR interval: ______________________ QRS duration: _____________________ QT interval: _____________________
- Interpretation: _____________________________________________________________________________________
Stop & review answers
- 1. A, C, D. A PJC occurs when an irritable site within the AV junction fires before the next SA node impulse is ready to fire, interrupting the underlying rhythm. PJCs may occur as single beats or in patterns (e.g., couplets, bigeminy, trigeminy, quadrigeminy). A noncompensatory (incomplete) pause often follows a PJC. This pause represents the delay during which the SA node resets its rhythm for the next beat. When the P wave of a PJC is seen, it is negative and may appear before or after the QRS complex.
- 2. C. An accelerated junctional rhythm is a dysrhythmia originating in the AV bundle with a ventricular rate between 61 and 100 beats/min.
- 3. D. If the AV junction paces the heart at a rate slower than 40 beats/min, the resulting rhythm is called junctional bradycardia. This wording may seem confusing because the AV junction’s normal pacing rate (40 to 60 beats/min) is bradycardic. However, the term junctional bradycardia refers to a rate slower than normal for the AV junction.
- 4. C. If the AV junction paces the heart, the electrical impulse must travel in a backward (retrograde) direction to activate the atria. If a P wave is seen, it will be inverted in leads II, III, and aVF because the impulse is traveling away from the positive electrode. If the atria depolarize before the ventricles, an inverted P wave will be seen before the QRS complex, and the PR interval will usually measure 0.12 second or less. The PR interval is shorter than usual because an impulse that begins in the AV junction does not have to travel as far to stimulate the ventricles. If the atria and ventricles depolarize at the same time, a P wave will not be visible because it will be hidden in the QRS complex. When the atria are depolarized after the ventricles, the P wave typically distorts the end of the QRS complex, and an inverted P wave will appear after the QRS.
- 5. B. The QRS duration associated with a rhythm that begins in the AV junction measures 0.11 second or less if conduction through the bundle branches, Purkinje fibers, and ventricles is normal.
- 6. A, B, D. The patient with an accelerated junctional rhythm is usually asymptomatic because the ventricular rate is 61 to 100 beats/min, which is the same rate as a sinus rhythm.
- 7. A. You can usually tell the difference between a PAC and a PJC by the P wave. A PAC typically has an upright P wave before the QRS complex in leads II, III, and aVF. A P wave may or may not be present with a PJC. If a P wave is present, it is inverted (retrograde) and may precede or follow the QRS. PJCs can be misdiagnosed when the P wave of a PAC is buried in the preceding T wave.
- 8. B, D. In this rhythm strip, the atrial rate and rhythm cannot be determined because P waves are not visible. The ventricular rhythm is regular and the QRS is narrow, measuring 0.08 second.
- 9. B. The cardiac monitor shows junctional bradycardia at 32 beats/min with ST-segment depression and inverted T waves.
- 10. B. Although there is no evidence of ST-segment elevation on the cardiac monitor, this patient is symptomatic with his slow heart rate, evidenced by his dizziness and hypotension. Treatment of symptomatic bradycardia should include applying a pulse oximeter, administering supplemental oxygen (if indicated), and establishing IV access, which has already been done. Next, obtain a 12-lead ECG and then administer atropine IV. Reassess the patient’s response to your interventions and continue monitoring. Because vagal maneuvers are used to attempt to slow the heart rate of some tachycardias, and this patient is bradycardic, vagal maneuvers are contraindicated in this situation.
Practice rhythm strip answers
Note: The rate and interval measurements provided here were obtained using electronic calipers.
- 26. Fig. 5.11
- 27. Fig. 5.12
- Rhythm: Regular
- Rate: 100 beats/min
- P waves: One inverted P wave precedes each QRS
- PR interval: 0.14 second
- QRS duration: 0.10 second
- QT interval: 0.28 second (approximate, T-wave end is not clearly visible with all beats)
- Interpretation: Accelerated junctional rhythm at 100 beats/min with ST-segment elevation (STE)
- 28. Fig. 5.13
- Rhythm: Irregular
- Rate: 130 beats/min
- P waves: Positive; one precedes each QRS but the shape and amplitude of some differ; P wave of beat 10 is early and hidden in the T wave of the preceding beat
- PR interval: 0.14 second
- QRS duration: 0.07 second
- QT interval: 0.28 second
- Interpretation: Sinus tachycardia at 130 beats/min with a PAC
- 29. Fig. 5.14
- 30. Fig. 5.15
- 31. Fig. 5.16
- Rhythm: Irregular
- Rate: 70 beats/min
- P waves: Sinus P waves are positive before each QRS and some are notched; P wave of beat 3 is early, inverted, and appears after the QRS
- PR interval: 0.16 second
- QRS duration: 0.09 second
- QT interval: 0.36 second
- Interpretation: Sinus rhythm at 70 beats/min with a PJC (beat 3 is the PJC)
- 32. Fig. 5.17
- 33. Fig. 5.18
- 34. Fig. 5.19
- 35. Fig. 5.20
- 36. Fig. 5.21
- Rhythm: Irregular
- Rate: 33 beats/min (sinus beats); 32 beats/min (junctional beats)
- P waves: Sinus P waves positive before QRS; none visible for junctional beats
- PR interval: 0.16 second (sinus beats)
- QRS duration: 0.07 second
- QT interval: 0.37 second
- Interpretation: Sinus bradycardia at 33 beats/min to junctional bradycardia at 32 beats/min; artifact is present
- 37. Fig. 5.22
- Rhythm: Irregular
- Rate: 70 beats/min
- P waves: Sinus P waves are positive before each QRS; an early P wave appears after beat 5 and distorts the T wave; beat 6 has no P wave
- PR interval: 0.16 second
- QRS duration: 0.08 second
- QT interval: 0.38 second
- Interpretation: Sinus rhythm at 70 beats/min with a nonconducted PAC (note distortion of the T wave of the beat preceding the pause) and a junctional escape beat
- 38. Fig. 5.23
- 39. Fig. 5.24
- Rhythm: Irregular; regular during the tachycardia
- Rate: 160 beats/min; 188 beats/min during the tachycardia
- P waves: Inverted after QRS in beat 1; sinus P wave in beats 2 and 3; cannot differentiate with certainty between inverted P waves and inverted T waves in beats associated with the tachycardia
- PR interval: 0.16 second (sinus beats)
- QRS duration: 0.08 second
- QT interval: 0.24 second if the inverted waveforms during the tachycardia are T waves
- Interpretation: Junctional beat, two sinus beats, changing to a narrow QRS tachycardia that is probably junctional tachycardia at 188 beats/min; ST-segment depression
- 40. Fig. 5.25
- 41. Fig. 5.26
- Rhythm: Irregular
- Rate: 60 beats/min
- P waves: Positive before sinus beats, early and inverted before the QRS in beat 3, early and upright in beat 5
- PR interval: 0.18 second (sinus beats)
- QRS duration: 0.06 second
- QT interval: 0.43 second
- Interpretation: Sinus rhythm at 60 beats/min with a PJC (beat 3), a PAC (beat 5), and ST-segment depression; artifact is present
- 42. Fig. 5.27
- 43. Fig. 5.28
- Rhythm: Regular
- Rate: 143 beats/min
- P waves: None visible before each QRS; cannot differentiate with certainty between inverted P waves and inverted T waves after each QRS
- PR interval: None
- QRS duration: 0.07 second
- QT interval: 0.21 second if the inverted waveforms after each QRS are T waves
- Interpretation: Narrow-QRS tachycardia, probably junctional tachycardia, at 143 beats/min with ST-segment depression; artifact is present
- 44. Fig. 5.29
- 45. Fig. 5.30
- Rhythm: Irregular
- Rate: 80 beats/min
- P waves: Positive before sinus beats; early inverted P waves appear in beats 3 and 6
- PR interval: 0.17 second (sinus beats)
- QRS duration: 0.06 second (sinus beats)
- QT interval: 0.35 second (sinus beats)
- Interpretation: Sinus rhythm at 80 beats/min with PJCs (beats 3 and 6)
- 46. Fig. 5.31
- Rhythm: Irregular
- Rate: 77 beats/min (junctional beats)
- P waves: Positive for sinus beats; not visible for junctional beats
- PR interval: 0.12 second (sinus beats)
- QRS duration: 0.06 second
- QT interval: 0.33 second
- Interpretation: Sinus rhythm changing to an accelerated junctional rhythm at 77 beats/min, back to a sinus rhythm
- 47. Fig. 5.32
- 48. Fig. 5.33
- Rhythm: Irregular
- Rate: 40 beats/min
- P waves: Low amplitude but positive; one precedes each QRS; some are notched
- PR interval: 0.13 to 0.16 second
- QRS duration: 0.06 to 0.08 second
- QT interval: 0.41 second
- Interpretation: Sinus bradyarrhythmia at 40 beats/min with ST-segment depression; U waves are present
- 49. Fig. 5.34
- 50. Fig. 5.35
References
Kusumoto F.M, Schoenfeld M.H, Barrett C, Edgerton J.R, Ellenbogen K.A, Gold M.R. & Varosy P.D. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay Circulation 8, 2018;140: e382- e482.
Miller J.M, Tomaselli G.F. & Zipes D.P. Therapy for cardiac arrhythmias Braunwald’s heart disease: A textbook of cardiovascular medicine 11th ed. 2019; Elsevier Philadelphia, PA.
Page R.L, Joglar J.A, Caldwell M.A, Calkins H, Conti J.B, Deal B.J. & Al-Khatib S.M. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia Circulation 14, 2016;133: e506- e574.
Zimetbaum P. Supraventricular cardiac arrhythmias Goldman-Cecil medicine 26th ed. 2020; Elsevier Philadelphia, PA 331-343.